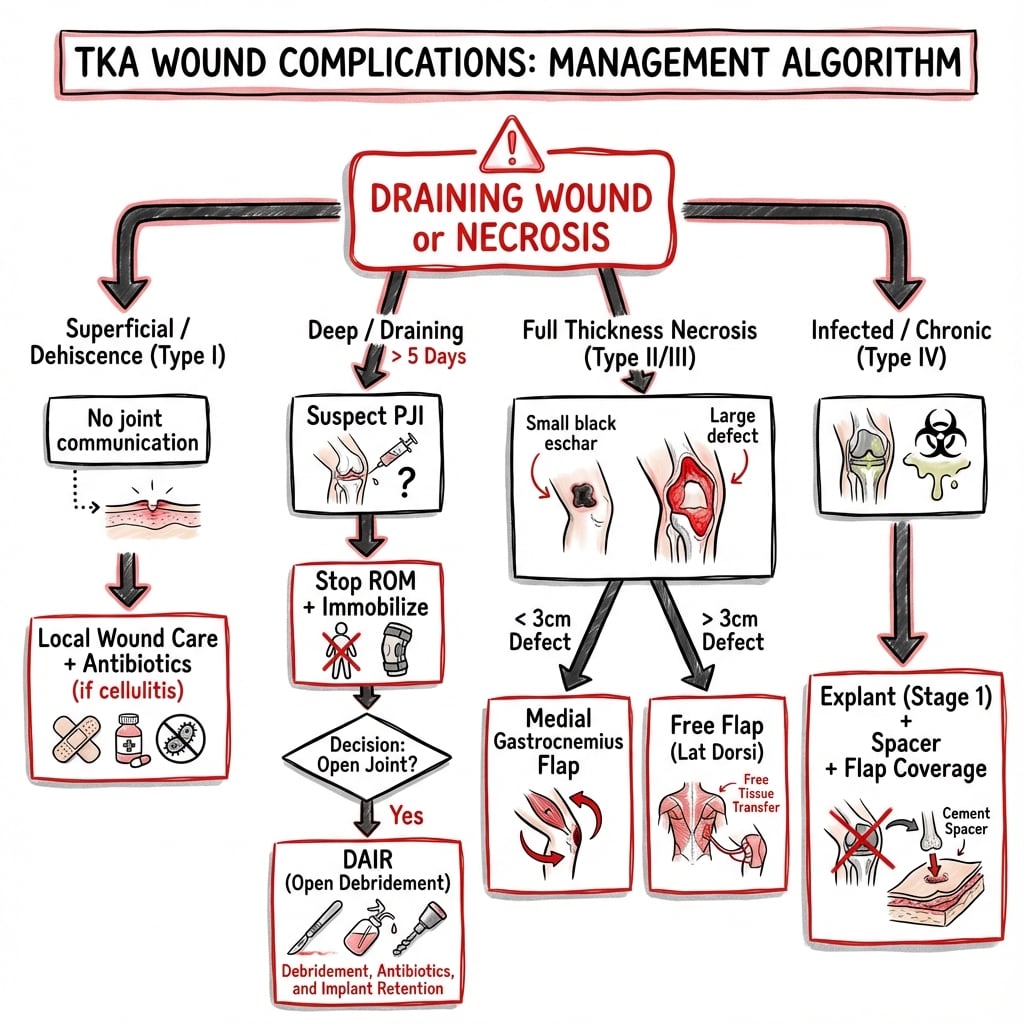
TKA Wound Complications
A spectrum from prolonged drainage to full-thickness necrosis with exposed prosthesis — the final common pathway to periprosthetic joint infection if mismanaged.
- Persistent wound drainage beyond 5-7 days is the single most important early warning sign and a strong independent predictor of PJI
- The anterior knee has thin, watershed-perfused soft tissue with no muscle padding — minor problems escalate to exposed prosthesis quickly
- Exposed prosthesis or extensor mechanism mandates urgent debridement plus soft-tissue coverage (gastrocnemius flap is the workhorse), not continued dressings
- “Each additional day of drainage raises infection risk ~29% (Patel JBJS 2007) — quote this to justify early intervention
- “Local wound care alone resolves roughly two-thirds of persistent drainage; the decision is when to stop waiting and operate
- “Closed-incision NPWT lowers SSI in revision arthroplasty but causes blistering in primary TKA — know where it helps
TKARisk Factors for TKA Wound Complications
Hook:The first four (Weight, steroids/immunosuppression, uncontrolled diabetes, poor Nutrition) are the highest-yield modifiable targets to optimise before elective TKA.
DRYWOUNDSurgical Steps to Achieve a Healing Wound
Hook:Technique is the only wholly intraoperative lever: a tension-free, well-perfused, layered closure is the single best preventive measure.
TKAApproach to the Draining TKA Wound
Hook:If the wound is still DAMP beyond 5-7 days and not improving, stop dressing and start operating - deep tissue cultures, not superficial swabs.
Epidemiology & Burden
Overall Incidence
Wound complications after TKA represent a significant clinical challenge: the anterior knee soft-tissue envelope is thin, mobile, and supplied by a watershed of perforators with no muscle padding over the implant, so apparently minor problems can progress rapidly to an exposed prosthesis. Persistent wound drainage (PWD) is the most studied marker — large arthroplasty cohorts report a PWD prevalence of roughly 3-6%, and PWD carries a markedly elevated risk of progressing to periprosthetic joint infection (PJI).
Persistent drainage as a dose-dependent risk factor
- Retrospective study of 1226 primary TKAs and 1211 THAs
- Each day of prolonged wound drainage increased the risk of wound infection by 29% after TKA and 42% after THA
- Morbid obesity was the only independent risk factor for infection after primary TKA
- Higher drain output and LMWH prophylaxis were associated with longer time to a dry wound
Temporal Patterns
| Time Period | Wound Complication Type | Frequency |
|---|---|---|
| 0-7 days | Wound drainage, haematoma | Most common period |
| 1-2 weeks | Superficial infection, early dehiscence | Critical intervention window |
| 2-4 weeks | Delayed healing, skin necrosis | Decision point for flap coverage |
| 1-3 months | Chronic wound, sinus formation | Indicates deep infection |
Aetiology, Patient & Surgical Factors
Why the Anterior Knee Is Vulnerable
The anterior knee soft-tissue envelope is thin and mobile, with a tenuous, predominantly medial blood supply from the descending genicular and superior/inferior medial geniculate vessels. Most TKA incisions are midline, so the lateral skin flap is perfused across a watershed by medial perforators — explaining why marginal necrosis tends to occur at the lateral wound edge and why prior lateral scars or wide undermining are dangerous. There is no muscle padding over the implant, so any full-thickness loss exposes capsule, extensor mechanism or prosthesis directly. Wound failure is therefore the interaction of impaired host biology (the modifiable factors below) with mechanical and vascular insults from surgical technique.
Host Factors
Understanding and optimizing modifiable risk factors is essential for prevention. The literature consistently identifies patient-related factors as the primary determinants of wound healing.
Obesity (BMI greater than 35)
- Most significant modifiable risk factor
- BMI greater than 40 increases risk 6-fold
- Weight loss of 5-10% significantly reduces risk
- Consider bariatric referral for BMI greater than 45
Diabetes Mellitus
- HbA1c greater than 8% associated with 2-3x increased risk
- Perioperative glucose control critical (target less than 10 mmol/L)
- Preoperative optimization period 3-6 months ideal
- Continuous glucose monitoring perioperatively recommended
Smoking
- Current smoking doubles wound complication risk
- Minimum 4 weeks cessation recommended preoperatively
- 8 weeks cessation optimal for microvascular recovery
- Quitline referral (13 7848) as standard practice
Nutrition
- Albumin less than 3.5 g/dL associated with poor healing
- Prealbumin more sensitive marker of acute nutrition status
- Total lymphocyte count less than 1500 indicates immunocompromise
- Dietitian referral for optimization
Medications
- Corticosteroids: prednisolone greater than 10mg daily increases risk
- Methotrexate: continue through surgery (current evidence)
- Biologics: hold 1-2 dosing cycles preoperatively
- Anticoagulation: increases haematoma risk
Surgical Factors
Risk Stratification
| Risk Category | Characteristics | Management Strategy |
|---|---|---|
| Low Risk | BMI less than 30, non-smoker, HbA1c less than 7%, no previous surgery | Standard precautions |
| Moderate Risk | BMI 30-40, controlled diabetes, previous surgery | Enhanced optimization, consider drain |
| High Risk | BMI greater than 40, HbA1c greater than 8%, immunosuppression, PVD | Multidisciplinary optimization, extended antibiotics, plastic surgery consultation |
| Very High Risk | Prior radiation, scleroderma, multiple risk factors | Consider primary flap coverage, staged approach |
Evidence: Modifiable Risk Factors
Glycaemic markers and SSI in diabetic TKA
- 462 diabetic patients (714 TKAs)
- Preoperative HbA1c at or above 8% was associated with superficial SSI (OR 6.1, 95% CI 1.6-23.4)
- Fasting blood glucose at or above 200 mg/dL was also associated with superficial SSI (OR 9.2)
- Glycaemic markers correlated; HbA1c and 2-hour postprandial glucose correlated most strongly
Preoperative smoking cessation halves wound complications
- Landmark multicentre RCT of 120 patients undergoing hip/knee replacement
- A 6-8 week preoperative cessation programme (counselling plus nicotine replacement) reduced wound-related complications from 31% to 5% (p=0.001)
- Overall complication rate fell from 52% to 18% (p=0.0003)
- Secondary surgery and cardiovascular complications also trended lower
Classification of Wound Complications
Anatomical Classification
Definition: Involvement of skin and subcutaneous tissue only, without extension to deep fascia or joint.
Types:
- Prolonged drainage: Serous or serosanguinous discharge beyond 5-7 days
- Superficial dehiscence: Partial separation without fascial involvement
- Skin necrosis: Full-thickness skin death, variable extent
- Superficial infection: Cellulitis, suture abscess, superficial SSI
Key Features:
- Intact deep fascia on probing
- No communication with joint space
- Culture typically skin flora
- Systemic symptoms absent or mild
Temporal Classification
| Timing | Classification | Aetiology | Implications |
|---|---|---|---|
| Less than 2 weeks | Acute | Technical factors, haematoma, early infection | Best prognosis if addressed promptly |
| 2-4 weeks | Subacute | Healing failure, skin necrosis evolving | Window for salvage with soft tissue procedures |
| Greater than 4 weeks | Delayed/Chronic | Established necrosis, chronic wound, biofilm | Higher risk of deep infection, more complex reconstruction |
| Greater than 3 months | Late | Sinus tract, chronic infection | Usually indicates PJI requiring staged revision |
Severity Grading
Grade I - Minor
- Prolonged drainage less than 10 days
- Responds to local measures
- No skin necrosis
- Normal inflammatory markers
Grade II - Moderate
- Drainage 10-14 days OR superficial dehiscence
- Requires theatre for washout/closure
- Limited skin necrosis (less than 2cm)
- Elevated but improving inflammatory markers
Grade III - Major
- Drainage greater than 14 days OR deep dehiscence
- Skin necrosis greater than 2cm
- Exposed capsule or extensor mechanism
- Persistently elevated inflammatory markers
Grade IV - Severe
- Exposed prosthesis
- Full-thickness necrosis
- Failed previous intervention
- Deep infection confirmed
Clinical Presentation and Assessment
History
Key Questions:
- Timing of symptom onset relative to surgery
- Character of drainage (serous, serosanguinous, purulent, haemoserous)
- Volume of drainage (saturating dressings, frequency of changes)
- Associated symptoms (fever, increasing pain, swelling)
- Compliance with postoperative instructions
- Any trauma or falls
Red Flags:
- Fever greater than 38.5 degrees C
- Increasing pain after initial improvement
- Purulent drainage at any time
- Systemic symptoms (malaise, rigors)
- Failure of wound to progress after 5-7 days
Examination
Wound Assessment:
- Extent of erythema (mark and date margins)
- Character of drainage on dressing
- Presence of necrosis (eschar, purple discoloration)
- Wound edge approximation
- Tension on closure
- Evidence of haematoma
Surrounding Skin:
- Tissue turgor and quality
- Previous scars
- Skin grafts or flaps
- Evidence of venous insufficiency
Investigations
The aim is to distinguish a settling superficial problem from established or impending deep infection. No single test is definitive — the trend matters more than any one value, and deep sampling beats superficial swabs.
Differential Diagnosis
| Condition | Features | Distinguishing Factors |
|---|---|---|
| Haematoma | Early, fluctuant, ecchymosis | Usually presents day 0-3; decreasing with time |
| Seroma | Non-tender, fluctuant, clear fluid | May be late; aspirate is straw-coloured |
| Superficial Infection | Erythema, warmth, tenderness | Responds to antibiotics; markers mildly elevated |
| Deep Infection | Systemic symptoms, joint involvement | Elevated markers, positive aspirate |
| Wound Tension/Necrosis | Progressive skin changes | May have minimal drainage initially |
| Fat Necrosis | Firm, tender nodules | Obese patients; may drain oily fluid |
Prevention Strategies
Preoperative Optimization
Diabetes Control
- Target HbA1c less than 8% (ideally less than 7%)
- Endocrinology referral for poor control
- Perioperative glucose monitoring protocol
- Insulin sliding scale in hospital
Nutrition
- Albumin target greater than 3.5 g/dL
- Preoperative oral supplements (e.g., Ensure, Resource)
- Consider parenteral nutrition if severely malnourished
- Vitamin C and zinc supplementation
Smoking Cessation
- Minimum 4 weeks preoperative cessation
- Nicotine replacement therapy acceptable
- Quitline referral (13 7848)
- Consider varenicline/bupropion
Weight Optimization
- Target BMI less than 40 for elective surgery
- Dietitian and exercise physiologist referral
- Consider bariatric surgery referral for BMI greater than 50
- 5-10% weight loss reduces risk significantly
Surgical Technique
Incision Planning
- Use previous incision if adequate
- Most lateral incision preferred if multiple
- Minimum 7cm skin bridge between incisions
- Full-thickness skin flaps
- Avoid undermining
Tissue Handling
- No-touch technique for skin edges
- Avoid Army-Navy retractors on skin edges
- Self-retaining retractors with care
- Minimal cautery to dermis
- Preserve subcutaneous fat layer
Haemostasis
- Tourniquet use controversial; if used, release before closure
- Tranexamic acid (topical or IV) reduces haematoma
- Meticulous point haemostasis
- Consider drain in high-risk patients (controversial)
Closure Principles
- Layered closure essential
- Capsular closure: absorbable braided suture
- Deep dermal: absorbable monofilament (critical layer)
- Skin: staples or running subcuticular
- Minimal tension on skin edges
- Consider barbed suture for capsule
Postoperative Care
Management Algorithm
Decision Framework
When to operate on persistent drainage
- 300 of 11,785 arthroplasties (2.9%) developed persistent drainage beyond 48 hours
- Drainage stopped spontaneously with local wound care and oral antibiotics in 217 (72%)
- Of the 83 needing surgery, a single debridement succeeded in 76%
- Delayed timing of surgery and malnutrition predicted failure of the first debridement
Persistent drainage and the risk of PJI
- Review of 4873 TJAs; persistent wound drainage prevalence 6.2%
- PWD was associated with markedly higher odds of PJI (OR 16.9, 95% CI 9.1-31.6)
- Risk factors included diabetes, morbid obesity and rheumatoid arthritis
- Around 65% of PWD resolved with local wound care alone, mirroring Jaberi
Over-anticoagulation predisposes to wound problems and PJI
- Case-control study of 78 septic revisions with matched controls
- Postoperative haematoma and wound drainage were significant risk factors for periprosthetic infection
- A mean INR over 1.5 was more common in patients who developed wound complications and subsequent PJI
- Suggests excess anticoagulation is a modifiable contributor to wound-related infection
Indications:
- Drainage less than 5 days, decreasing trend
- Superficial erythema responding to elevation
- Normal or minimally elevated inflammatory markers
- No systemic symptoms
- Stable wound appearance
Management:
- Bed rest with leg elevated
- Dressing changes as needed (sterile technique)
- Cease anticoagulation if safe
- Consider compression
- Daily wound review
- Oral antibiotics if superficial infection
Endpoint Criteria:
- Wound dry for 48 hours
- Erythema resolved
- Inflammatory markers normalizing
- Patient afebrile
Failure Criteria (Proceed to Theatre):
- No improvement at 48-72 hours
- Progression of drainage or erythema
- Rising inflammatory markers
- New systemic symptoms
Specific Scenarios
| Scenario | Initial Management | Escalation Trigger | Definitive Treatment |
|---|---|---|---|
| Drainage day 3-5, stable | Observation, bed rest, elevation | No improvement 48hr | I&D, direct closure |
| Drainage greater than 7 days | Theatre within 24-48hr | Deep tissue involvement | I&D +/- NPWT |
| Skin necrosis 2-4cm | Debridement, assess depth | Exposed capsule | Local flap coverage |
| Exposed prosthesis | Urgent plastic surgery consult | Unable to cover locally | Free flap or staged revision |
| Proven deep infection | DAIR protocol | Virulent organism, loose implant | Staged revision |
NPWT (Negative Pressure Wound Therapy)
Role in TKA Wound Complications:
- Bridge to definitive closure
- Promotes granulation tissue
- Reduces oedema and drainage
- Allows serial debridement
- NOT a definitive treatment for exposed prosthesis
Technique:
- White foam over exposed tissue (less adherent)
- Black foam for granulation (more aggressive)
- Continuous pressure 75-125 mmHg
- Changes every 48-72 hours
- Not through joint capsule if exposed
Contraindications:
- Active bleeding
- Malignancy in wound
- Untreated osteomyelitis
- Exposed vessels without coverage
Closed-incision NPWT: helps in revision, not primary TKA
- Meta-analysis of RCTs of closed-incision NPWT after elective hip and knee arthroplasty
- ciNPWT reduced SSI overall (3.4% vs 7%, RR 0.48) and specifically in revision THA/TKA (RR 0.41)
- In primary TKA it increased non-infectious wound complications (RR 4.71)
- Wound blistering rose greater than 12-fold after primary TKA with ciNPWT
Soft Tissue Coverage Options
Local Flaps
Anatomy:
- Two heads: medial and lateral
- Medial head larger, more commonly used
- Vascular pedicle: sural arteries (branches of popliteal)
- Pivot point at musculotendinous junction
Indications:
- Proximal and middle third TKA wounds
- Exposed proximal prosthesis
- Soft tissue defects up to 10x15cm
Technique:
- Medial approach for medial head
- Identify and protect saphenous nerve
- Divide tendon at musculotendinous junction
- Rotate into defect
- Split-thickness skin graft over muscle
Advantages:
- Reliable blood supply
- Good tissue bulk
- Well-established technique
- Can be performed under tourniquet
Limitations:
- Cannot reach distal third of wound
- Cosmetic deficit of calf
- Minor functional impact (minimal weakness)
Coverage Algorithm by Location
| Wound Location | First-Line Coverage | Second-Line Coverage |
|---|---|---|
| Proximal third (above patella) | Medial gastrocnemius flap | Lateral gastrocnemius, free flap |
| Middle third (patella level) | Gastrocnemius flap | Propeller flap, free flap |
| Distal third (below patella) | Hemisoleus flap | Propeller flap, free flap |
| Extensive (full incision) | Combined gastrocnemius-soleus | Free latissimus dorsi |
Complications, Outcomes & Prognosis
Success Rates
Medial gastrocnemius flap for exposed or infected TKA
- 47 patients reconstructed with a medial gastrocnemius flap for an exposed or infected TKA
- Flap failure was rare (3 of 47, 6.4%)
- Implant survivorship was only 59.6% at mean 6.7-year follow-up
- Functional outcome was often compromised, reflecting unfavourable underlying conditions
Factors Affecting Outcome
| Factor | Favourable | Unfavourable |
|---|---|---|
| Timing of Intervention | Less than 2 weeks from symptom onset | Greater than 4 weeks |
| Inflammatory Markers | Normalizing trend pre-flap | Persistently elevated |
| Cultures | Negative at time of coverage | Positive, especially MRSA/resistant organisms |
| Patient Factors | Non-smoker, controlled diabetes | Uncontrolled diabetes, active smoking |
| Wound Aetiology | Mechanical (wound tension, haematoma) | Established deep infection |
Complications of Flap Coverage
Early (less than 2 weeks):
- Flap necrosis (partial or complete): 5-10%
- Haematoma: 5%
- Seroma: 10-15%
- Skin graft failure: 10-20%
Late (greater than 2 weeks):
- Chronic wound/sinus: 10-15%
- Deep infection requiring revision: 10-20%
- Stiffness (loss of ROM): 20-30%
- Cosmetic concerns: common
Long-Term Outcomes
Prosthesis Survival:
- At 2 years: 75-85% with early treatment
- At 5 years: 65-75%
- Revision rates higher than uncomplicated TKA
Functional Outcomes:
- ROM typically reduced (average loss 10-20 degrees flexion)
- Oxford Knee Score reduced by 5-10 points versus uncomplicated
- Patient satisfaction variable (70-80% satisfied)
- Return to activities possible but delayed
Evidence Base & Landmark Literature
The evidence base for TKA wound complications is dominated by large retrospective cohorts and a small number of Level I trials on prevention (smoking cessation) and adjuncts (closed-incision NPWT). The verified key papers below are cross-referenced in their relevant sections above.
| Theme | Landmark Evidence | Take-Home |
|---|---|---|
| Drainage is dose-dependent | Patel, JBJS Am 2007 (Level III) | Each extra day of drainage raises TKA infection risk ~29% |
| Drainage predicts PJI | Shahi, Arthroplast Today 2019 (Level III) | PWD prevalence 6.2%; PWD to PJI OR ~16.9 |
| When to operate | Jaberi, CORR 2008 (Level III) | ~65-72% settle with local care; single debridement ~76% success if early |
| Glycaemic control | Hwang, CORR 2014 (Level III) | HbA1c at or above 8% raises superficial SSI odds ~6-fold |
| Smoking cessation | Møller, Lancet 2002 (Level I RCT) | 6-8 week programme cut wound complications 31% to 5% |
| ciNPWT | Ailaney, J Arthroplasty 2020 (Level I MA) | Helps in revision; increases blistering in primary TKA |
| Flap salvage | Wiberg, Scand J Surg 2023 (Level IV) | Gastrocnemius flap heals soft tissue but implant survival only ~60% |
Controversies & Areas of Uncertainty
The evidence base for managing TKA wound complications is largely retrospective; several core decisions remain genuinely contested and make excellent viva discussion points.
Guidelines, Registries & Global Practice
Global Epidemiology
Knee arthroplasty volume is rising worldwide, so the absolute burden of wound complications is growing even as rates stay broadly stable (1-4% primary, higher in revision). Registries consistently identify infection — for which a wound complication is often the gateway — as a leading cause of early revision within the first 1-2 years. Persistent wound drainage prevalence clusters around 3-6% across large cohorts irrespective of country, and the same modifiable risks (obesity, diabetes, smoking, malnutrition, inflammatory arthropathy) dominate globally.
Side-by-Side Guidance
| Body | Emphasis Relevant to TKA Wounds |
|---|---|
| WHO (Global SSI prevention) | Strong: preoperative bathing, appropriate skin antisepsis (alcohol-based chlorhexidine), weight-based timely prophylactic antibiotics, glycaemic control, normothermia; against prolonged postoperative antibiotics |
| AAOS / ICM (US, international consensus) | Optimise modifiable risks (HbA1c, BMI, nutrition, Staph decolonisation); treat persistent drainage promptly; deep tissue cultures; early debridement over prolonged dressings |
| NICE / BOA (UK) | SSI-prevention bundle, MSSA/MRSA screening and decolonisation, chlorhexidine prep; early senior review and intervention for problem wounds |
| AO Foundation / EFORT (Europe) | Tension-free soft-tissue handling, watershed-aware incision planning, multidisciplinary (plastics) involvement for compromised envelopes |
Where guidance genuinely converges: optimise the host, prepare and handle skin meticulously, do not let a draining wound persist, sample deep tissue, and involve plastic surgery early. Where it diverges is mainly in the detail of decolonisation protocols and the role of adjuncts such as closed-incision NPWT.
Registry Notes
Major arthroplasty registries (NJR for England/Wales, AJRR in the US, AOANJRR in Australia, the Nordic registries) do not capture wound complications as a discrete endpoint, but they track the downstream signal — early revision for infection. Across these registries, infection is a dominant cause of revision in the first 2 years, underlining wound integrity as a modifiable lever on revision rates.
High- vs Limited-Resource Practice
| Domain | Well-Resourced Setting | Limited-Resource Setting |
|---|---|---|
| Plastic surgery access | On-site microsurgery and flap expertise | Often absent; reliance on local muscle flaps, earlier transfer, or general/orthopaedic-led coverage |
| Adjuncts | Closed-incision NPWT, advanced dressings readily available | Limited; emphasis on technique, elevation and timely debridement |
| Host optimisation | Multidisciplinary pre-habilitation (endocrine, dietetics) | Variable; cessation counselling and glycaemic basics still high-yield and low-cost |
| Timing of escalation | Rapid theatre access for early I&D | Delays common; threshold to refer/transfer should be lower |
The principles are universal; the resource-dependent variable is how quickly soft-tissue coverage and theatre can be mobilised — which is precisely the determinant of implant salvage.
Key Takeaways
Prevention is Better Than Cure
- Optimize modifiable risk factors preoperatively (obesity, diabetes, smoking, nutrition)
- Meticulous surgical technique with emphasis on tissue handling
- Layered closure with attention to deep dermal layer
- Appropriate postoperative wound care
Early Recognition and Intervention
- Persistent drainage beyond 5-7 days is a red flag
- 48-72 hour rule: if conservative measures fail, proceed to theatre
- Trend of inflammatory markers more important than absolute values
- Low threshold for surgical exploration in high-risk patients
Definitive Management
- Aggressive debridement and lavage in theatre
- Direct closure if possible; NPWT as bridge if not
- Early plastic surgery involvement for complex wounds
- Gastrocnemius flap is the workhorse for soft tissue coverage
Outcomes
- Early treatment (less than 2 weeks) preserves 75-85% of prostheses
- Delayed treatment (greater than 4 weeks) drops to 50-60%
- Gastrocnemius flap has 90-95% success rate
- Functional outcomes reduced but acceptable with successful salvage
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman is 8 days post primary TKA. The wound is still leaking serosanguinous fluid and soaking the dressing. She is afebrile and the knee is not red. How do you assess and manage her?”
“A patient referred from a peripheral hospital has a 4 cm area of full-thickness skin necrosis over the anterior knee 3 weeks after TKA, with the extensor mechanism visible at the base. Walk me through your management.”
“How would you reduce the risk of wound complications before and during an elective TKA in a high-risk patient — a smoker with a BMI of 42 and HbA1c of 9%?”
Key Numbers
- Wound complication rate: 1-4% primary TKA, 4-12% revision
- Persistent drainage greater than 5-7 days requires intervention
- BMI greater than 40 = 6-fold increased risk
- HbA1c target: less than 8% (ideally less than 7%)
- Albumin target: greater than 3.5 g/dL
- Smoking cessation: minimum 4 weeks, optimal 8 weeks
- Skin bridge minimum: 7cm between incisions
- Flap coverage success: 90-95% gastrocnemius
- Prosthesis retention early treatment: 75-85%
- Prosthesis retention late treatment: 50-60%
Classification
- Superficial: skin and subcutaneous only, intact fascia
- Deep: through fascia, potential joint communication
- Acute: less than 2 weeks (best prognosis)
- Subacute: 2-4 weeks (window for salvage)
- Delayed: greater than 4 weeks (higher infection risk)
Management Triggers
- 48-72 hour rule: if no improvement, proceed to theatre
- Any exposed prosthesis = urgent flap consultation
- Necrosis greater than 2cm = likely needs flap
- Positive cultures at coverage = worse prognosis
- NPWT is bridge to closure, not definitive treatment
Flap Coverage
- Gastrocnemius: workhorse, proximal and middle third
- Medial head most commonly used (larger)
- Soleus: middle to distal third
- Free flap: failed local options, large defects
- Early plastic surgery involvement improves outcomes
Risk Factors (WOUND RISK)
- Weight (BMI greater than 35)
- Oral steroids and immunosuppression
- Uncontrolled diabetes (HbA1c greater than 8%)
- Nutrition poor (albumin less than 3.5)
- Dermatologic conditions
- Revision surgery or previous incisions
- Inflammatory arthropathy
- Smoking (current or recent)
- Knee previous radiation or surgery
Prevention Pearls
- Chlorhexidine washes x5 days preoperatively
- MRSA decolonization if carrier (mupirocin)
- No-touch technique for skin edges
- Layered closure with deep dermal sutures (critical)
- Tranexamic acid reduces haematoma
- Undisturbed dressing 48-72 hours postoperatively