Occult Spiral Tibia | Clinical Diagnosis | 9 Months to 3 Years
- Age 9 months to 3 years - child must be ambulatory (walking age)
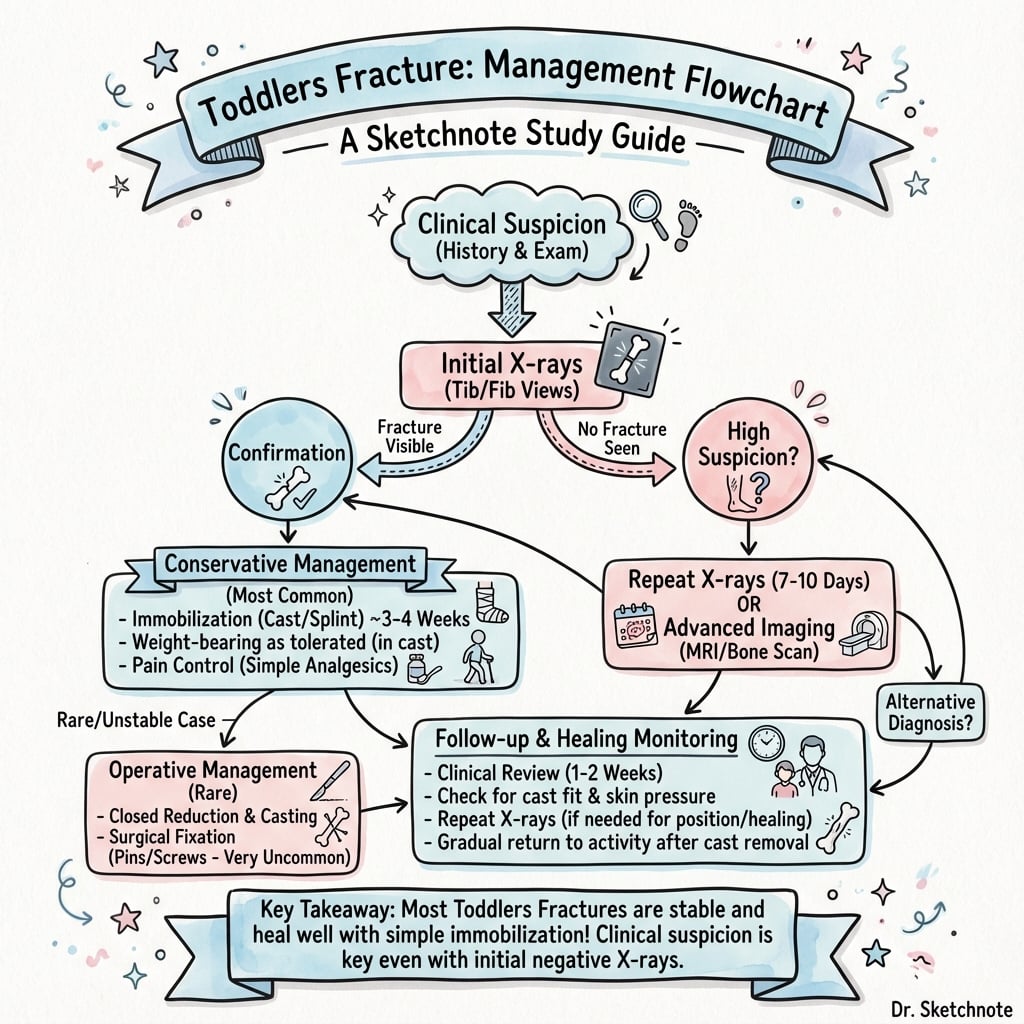
- X-ray is OFTEN NEGATIVE initially - treat clinically if suspected
- Spiral fracture pattern on distal to mid tibial shaft
- Repeat X-ray at 2 weeks shows periosteal reaction confirming fracture
- Consider NAI if pattern inconsistent with developmental stage
- “Negative X-ray does NOT rule out toddler's fracture
- “Bone scan or MRI only if diagnosis uncertain and not improving
- “3-4 weeks in below-knee or above-knee cast
- “Look for spiral line on oblique view if AP/lateral negative
X-ray negative in 50%. If clinical suspicion high (limping walking-age toddler, point tenderness tibia, no other cause), treat with cast even if X-ray negative. Repeat X-ray at 2 weeks shows healing.
9 months to 3 years. Child must be ambulatory (walking). Before walking = suspicious for NAI. After 3 years = other diagnoses more likely. The classic patient just started walking.
Look for subtle spiral. Often best seen on internal oblique view. Non-displaced, minimal periosteal reaction initially. May only see soft tissue swelling or subtle cortical irregularity.
Consider abuse if atypical. Spiral tibial fracture in non-ambulatory child (not yet walking) raises suspicion for NAI. Document developmental milestones carefully.
| Feature | Typical Finding | Red Flag |
|---|---|---|
| Age | 9 months to 3 years (walking) | Non-ambulatory = NAI concern |
| Mechanism | Low-energy twisting fall | High-energy = atypical |
| X-ray | Often negative initially | Multiple fractures = NAI |
| Location | Distal to mid tibial shaft | Metaphyseal = bucket handle (NAI) |
| Pattern | Spiral/oblique, non-displaced | Transverse = higher energy |
SPIRALToddler's Fracture Features
Hook:SPIRAL fracture that's SUBTLE - treat clinically!
RED FLAGSWhen to Suspect NAI
Hook:RED FLAGS in pediatric fractures must be documented!
CASTToddler's Fracture Management
Hook:CAST the limping toddler - don't wait for positive X-ray!
Overview and Epidemiology
Walking age but immature gait. Toddlers just learning to walk have an unsteady gait and are prone to twisting falls. The tibia is relatively weak compared to the forces generated. After age 3-4, gait matures and coordination improves.
- Peak age 9 months to 3 years
- Must be ambulatory (started walking)
- Boys slightly more common
- Common pediatric fracture
- Often presents to ED or GP
- Low-energy twisting injury
- Running and stumbling
- Playground falls
- Often unwitnessed
- Child cannot describe mechanism
Anatomy and Biomechanics
Pediatric Tibial Shaft
Location: Fracture typically occurs in the distal third to middle third of the tibial diaphysis.
Why spiral? Rotational force with fixed foot creates spiral pattern. The periosteum is thick in children and often remains intact, limiting displacement.
Blood supply: Pediatric tibia has excellent blood supply. Union is rapid (3-4 weeks) compared to adults.
Classification and Variants
Classic Toddler's Fracture
Location: Distal to mid tibial diaphysis.
Pattern: Spiral or oblique, non-displaced or minimally displaced.
Key feature: The fracture is often subtle or invisible on initial X-ray. Look carefully for a faint spiral line or cortical discontinuity.
Clinical Assessment
- Child limping or refusing to walk
- Often no witnessed injury
- Low-energy mechanism if observed
- No significant trauma
- Developmental milestones (is child walking?)
- Point tenderness along tibial shaft
- Minimal or no swelling
- Refuses to bear weight
- No obvious deformity
- Normal neurovascular status
Trust your clinical exam. A walking-age toddler who refuses to bear weight, has point tenderness over the tibia, and has no other explanation (hip, knee, foot pathology ruled out) likely has a toddler's fracture even if X-ray is negative. TREAT CLINICALLY.
Before diagnosing toddler's fracture, ensure you have assessed: hip (septic joint, Perthes, transient synovitis), knee (injury, infection), foot (foreign body, injury), soft tissue (bruising, infection). A limping child workup may include inflammatory markers if infection suspected.
Investigations
X-ray Protocol
Standard views: AP and lateral tibia/fibula (full length including ankle and knee).
Internal oblique view: May reveal the spiral fracture line when AP/lateral are negative.
What to look for: Subtle spiral line, cortical irregularity, soft tissue swelling. The fracture is often NON-DISPLACED.
| View | Finding | Sensitivity |
|---|---|---|
| AP tibia | May show spiral line | Variable |
| Lateral tibia | Often negative | Low |
| Internal oblique | Best for spiral | Higher |
| 2-week follow-up | Periosteal reaction | High |
Management
Do not wait for positive X-ray to treat. If clinical suspicion is high (limping walking-age toddler, tibial tenderness, low-energy mechanism), apply a cast. The child will improve, and follow-up X-ray confirms the diagnosis.
Cast Treatment
Options: Above-knee cast (AKC) or below-knee cast (BKC). Both are acceptable.
AKC advantages: Controls rotation better. Tolerated well by toddlers (they adapt quickly).
BKC advantages: Lighter, allows knee motion.
Duration: 3-4 weeks. Healing is rapid in this age group.
Follow-up: X-ray at 2-3 weeks to confirm healing. Remove cast when callus visible.
Explain to parents: "We suspect a minor fracture that may not show on today's X-ray. We will treat with a cast for 3-4 weeks. A repeat X-ray will confirm healing. Your child will be walking normally again soon."
Surgical Considerations
Surgery NOT Required
Toddler's fractures are almost universally treated non-operatively. Surgical intervention is not indicated for typical toddler's fracture. Cast immobilization for 3-4 weeks achieves 100% union.
Why no surgery? Non-displaced fracture, excellent pediatric healing, thick periosteum maintains alignment, no instability.
Complications
Complications of Toddler's Fracture
| Complication | Incidence | Management |
|---|---|---|
| Delayed diagnosis | Common | Repeat X-ray at 2 weeks |
| Cast-related issues | Occasional | Skin checks, cast modification |
| Nonunion | Extremely rare | Almost never occurs in children |
| Growth disturbance | None | Fracture is diaphyseal, not physeal |
| Long-term disability | None | Excellent prognosis |
Toddler's fracture has an excellent prognosis. Union is virtually 100%. There are no long-term sequelae. The child returns to normal function within weeks.
Follow-Up Protocol
Toddler's Fracture Follow-Up
Clinical assessment, X-ray (may be negative), apply cast if suspected. Document developmental milestones.
Optional - check cast fit if any concerns. Phone follow-up acceptable.
X-ray through cast or after cast removal. Look for periosteal reaction / callus confirming fracture healing.
Remove cast once callus visible and child comfortable. Allow gradual return to walking.
Child should be walking normally. No further follow-up needed unless concerns.
Outcomes and Prognosis
Key Prognostic Points
Union: Virtually 100% - nonunion essentially does not occur.
Remodeling: Not needed - fracture is usually non-displaced.
Growth: No growth disturbance - fracture is diaphyseal, not physeal.
Function: Complete return to normal gait and activity.
Special Considerations
When to Consider Non-Accidental Injury
Red flags:
- Child is non-ambulatory (not yet walking)
- Spiral fracture in infant
- Inconsistent or changing history
- Delayed presentation
- Other injuries in different healing stages
Action: If NAI suspected, full skeletal survey, child protection referral, thorough documentation.
Controversies and Areas of Uncertainty
The longstanding teaching is to cast every clinically-suspected toddler's fracture. Newer data (Coveney 2024) show selected presumptive cases do as well without immobilisation. There is no consensus and practice varies widely.
A randomised trial (Bradman 2021) found a removable CAM boot gave easier care and faster weight-bearing with equal healing. Many still default to an above-knee cast for the unreliable toddler. The "best" device remains debated.
Some pathways discharge with safety-netting only; others mandate a 2-week clinic film to "confirm" a clinically obvious diagnosis. Repeat imaging mainly adds reassurance and exposure, not management change, in the typical case.
Mellick's CAST work argues the rigid "9 months to 3 years" definition is artificial - accidental spiral tibial fractures occur across early childhood. The classic age band is a teaching aid, not a strict diagnostic gate.
The controversy is a trap and an opportunity. State that the fracture is benign and that the live debates are about how much immobilisation and follow-up, not whether to exclude sepsis and NAI. Anchoring on the safe principles (rule out septic arthritis, consider NAI in the non-ambulant child) scores marks regardless of which immobilisation philosophy you favour.
Evidence Base and Key Studies
Dunbar et al. - Original Description (1964)
- Coined the term 'toddler's fracture' / obscure tibial fracture of infants
- Subtle spiral or hairline fracture of the tibial shaft in ambulant young children
- Often occult on the initial radiograph; soft-tissue swelling may be the only clue
- Excellent prognosis with simple immobilisation
Mellick et al. - CAST Fractures Series
- Retrospective review of 55 children with isolated spiral tibial fractures (two US tertiary centres)
- Age range 12 to 94 months (mean 50.7 months); no child was under 1 year of age
- Lower two-thirds of the tibia involved in 95%; displacement usually none or minimal
- No fracture was confirmed to be non-accidental - the pattern is overwhelmingly accidental
Bradman et al. - RCT: CAM Boot vs Above-Knee Cast
- Randomised controlled trial, 87 children aged 1 to 5 years with proven or suspected toddler's fracture
- Controlled-ankle-motion (CAM) boot vs above-knee plaster-of-Paris cast
- CAM boot gave significantly better caregiver care-and-comfort scores at every time-point (all p under 0.001)
- Faster return to weight-bearing at day 7-10 (77.5% vs 53.8%) with NO difference in fracture healing or pressure injuries
John et al. - Expanding the Concept
- Pictorial review broadening 'toddler's fracture' beyond the classic spiral tibia
- Includes occult fibular buckle/plastic-bowing, tibial stress/compression and tarsal/metatarsal fractures
- Some fractures so subtle that bone scintigraphy or follow-up radiographs are needed to detect them
- All share an identical clinical picture - the limping or non-weight-bearing toddler
Starshak et al. - Occult Calcaneal 'Toddler's' Fracture
- Ten occult calcaneal fractures in children aged 19 to 41 months presenting with acute limp
- All had non-contributory initial radiographs and were detected by bone scintigraphy
- Follow-up films later showed the fracture in 4 of 10 and confirmed healing
- Described as 'another toddler's fracture' - the foot can be the hidden source
Coveney & Barrett - Immobilisation vs None
- Retrospective review of 166 children (96 radiologically confirmed, 70 presumptive) in Ireland
- 13% were managed with NO immobilisation; presumptive cases were less likely to be immobilised
- Six-month ED re-attendance was similar: 17% (immobilised) vs 13% (not immobilised), p = 0.66
- Fall from standing height was the commonest mechanism (33%)
Alqarni & Goldman - Practical Management Review
- Practice review of confirmed and presumed toddler's fracture
- Diagnosis is clinical, frequently (but not always) documented on radiographs
- Recommends a CAM boot or short-leg back-slab over rigid casting where possible
- For most children no paediatric orthopaedic follow-up is required
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An 18-month-old boy presents with acute onset limping. Mum reports he was playing in the backyard and then started crying and refusing to walk. He is afebrile. X-rays of the tibia are normal. How would you manage this?”
“A 7-month-old infant presents with a spiral tibial fracture. The parents report she rolled off the couch and hasn't been moving her leg since. She is not yet walking. What are your concerns?”
“A 22-month-old was treated for suspected toddler's fracture in a cast 2 weeks ago after presenting with a limp and negative X-ray. On review today, the parents report she is still not walking. Repeat X-ray is also normal. What are your next steps?”
MCQ Practice Points
Q: What is the typical age range for toddler's fracture? A: 9 months to 3 years. The child must be ambulatory (walking age). Before walking age, consider NAI.
Q: What percentage of toddler's fractures have a negative initial X-ray? A: Approximately 50%. Repeat X-ray at 2 weeks shows periosteal reaction, confirming the diagnosis.
Q: How should you manage a suspected toddler's fracture with negative X-ray? A: Apply a cast and treat clinically. A negative X-ray does not rule out the diagnosis. Treat based on clinical suspicion.
Q: What is the typical fracture pattern in toddler's fracture? A: Spiral or oblique, non-displaced, distal to mid tibial shaft. The spiral pattern results from rotational force.
Q: How long should a toddler's fracture be casted? A: 3-4 weeks. Healing is rapid in this age group.
Q: In what circumstance is a spiral tibial fracture concerning for NAI? A: In a non-ambulatory child (not yet walking). Toddler's fracture requires the child to be walking. Spiral fracture in a non-walker raises abuse concern.
Guidelines, Registries & Global Practice
- Spiral tibial fracture is among the most common fractures of the ambulant toddler worldwide
- Mellick's series: mean age ~51 months, none under 1 year, slight male predominance, left side marginally more common
- Lower two-thirds of the tibia in ~95% of cases; the fibula is characteristically intact
- Incidence is hard to quantify because radiograph-negative cases are inconsistently recorded
- No implant registry applies (non-operative injury), so evidence comes from ED/paediatric cohorts and one RCT
- Bradman RCT (Australia) and Coveney cohort (Ireland) both point toward lighter, removable immobilisation
- Re-attendance, not union, is the practical outcome - union is effectively universal
- Bone scintigraphy (historical) has largely given way to follow-up radiographs or MRI for true diagnostic doubt
| Body / source | Diagnosis emphasis | Immobilisation stance |
|---|---|---|
| RCEM / NICE-aligned UK pathways | Clinical diagnosis; radiograph-negative limp can still be a fracture; safeguarding screen | Below-knee cast or removable boot; many discharge with safety-netting |
| AAOS / US paediatric ED practice | Tibia films, treat presumptively if classic; broaden search if atypical | Long or short leg cast traditional; CAM boot increasingly accepted |
| AO Foundation (paediatric) | Stable, low-energy diaphyseal pattern; intact periosteal sleeve | Conservative immobilisation; surgery essentially never indicated |
| RACGP / family-physician reviews | Clinical diagnosis, frequently documented on X-ray | Prefer CAM boot or short-leg back-slab; usually no orthopaedic referral |
- Ready access to repeat radiographs, ultrasound and MRI to exclude sepsis and occult fracture
- Formal safeguarding teams and skeletal-survey protocols for suspected NAI
- Growing use of removable boots and nurse-led / virtual fracture-clinic follow-up
- Heavier reliance on clinical diagnosis and a single radiograph; advanced imaging may be unavailable
- Plaster cast remains the default - cheap, robust and reliable for the unsupervised toddler
- Safeguarding pathways may be informal; clinicians must still document mechanism and milestones carefully
Whatever the resource setting, a spiral long-bone fracture in a non-ambulant infant, a mechanism that does not fit, delayed presentation, or injuries of differing ages mandates consideration of inflicted injury, documentation of developmental milestones, and referral through the local safeguarding process. Mandatory-reporting law exists in most jurisdictions but the clinical duty to protect the child is global.
Key Features
- Age 9 months to 3 years (walking)
- Spiral/oblique tibial shaft fracture
- Low-energy twisting mechanism
- X-ray often negative initially
Clinical Diagnosis
- Point tenderness over tibia
- Refuses to bear weight
- No visible deformity
- Treat even if X-ray negative
Treatment
- Above or below knee cast
- 3-4 weeks duration
- Repeat X-ray at 2 weeks
- 100% union rate
NAI Concerns
- Non-ambulatory child = red flag
- Spiral fracture in infant suspicious
- Inconsistent mechanism
- Document developmental stage
Prognosis
- Excellent - complete recovery
- No growth disturbance
- No long-term sequelae
- Normal gait by 4-6 weeks