Hemimelic epiphyseal osteochondromas | Children, lower limb | Usually one side of one limb
- Definition: a rare, non-hereditary developmental disorder of childhood with osteocartilaginous overgrowth (osteochondroma-like masses) arising from one or more epiphyses, almost always confined to one side of one limb
- Hemimelic = one half: the medial or lateral half of the epiphysis is affected (medial more often than lateral), and the lesion respects the midline of the limb
- Not an osteochondroma: it shares histology with osteochondroma but is not linked to the EXT genes and is not part of hereditary multiple exostoses; it is intra-articular/epiphyseal rather than metaphyseal
- MRI is the key investigation: it shows the cartilage cap continuous with epiphyseal cartilage, defines the lesion before the bony nidus ossifies, and plans surgery
- Main risks if untreated: progressive deformity, joint incongruity, mechanical block, limb-length discrepancy and early secondary osteoarthritis - marginal excision of symptomatic lesions is the mainstay of treatment
- “Hemimelic = affects medial OR lateral half of an epiphysis, one limb only
- “Most common around the ankle (talus) and knee (distal femur)
- “NOT EXT-related, NOT hereditary multiple exostoses
- “MRI defines the unossified cartilage cap and guides excision
- “Recurrence and secondary OA are the principal long-term concerns
Trevor disease looks like an osteochondroma on histology but is epiphyseal/intra-articular, unilateral within one limb, not EXT-related and not hereditary. Do not call it "multiple hereditary exostoses".
The differential includes synovial chondromatosis, intra-articular chondroma, and rarely a chondral/parosteal lesion. MRI plus the typical age and hemimelic epiphyseal pattern usually settle it; biopsy only if doubt.
State the hemimelic, one-limb pattern, name the Azouz (localised/classical/generalised) types, and stress MRI to show the cartilage cap before deciding on marginal excision.
Overview and Epidemiology
Dysplasia epiphysealis hemimelica (DEH), eponymously Trevor disease (or Trevor-Fairbank disease), is a rare developmental skeletal disorder defined by asymmetric osteocartilaginous overgrowth of one or more epiphyses in a growing child. The masses behave like osteochondromas but arise from the epiphysis (or an epiphyseal equivalent such as a carpal/tarsal bone) rather than the metaphysis.
The defining word is hemimelic - "half a limb". Two features follow from it:
- The lesion affects the medial or lateral half of an epiphysis (medial side more often than lateral).
- Involvement is almost always limited to one side of one limb, respecting the midline; the lower limb is far more often affected than the upper limb.
It was described by Mouchet and Belot in 1926 ("tarsomegalie") and characterised in the English literature by Trevor in 1950 and by Fairbank in 1956, who coined "dysplasia epiphysealis hemimelica".
According to PubMed, the imaging review by Tyler and colleagues emphasises that DEH is an asymmetric overgrowth of the cartilage of a medial or lateral epiphysis or epiphyseal equivalent, and that imaging is central to diagnosis and to distinguishing it from more sinister lesions (DOI).
NOTNOT-OC - How DEH Differs From Osteochondroma
Hook:DEH is NOT an OC: think NOT-OC to recall the five ways it differs from a metaphyseal osteochondroma.
Pathophysiology and Anatomy
DEH is best understood as a disorder of localised epiphyseal cartilage proliferation. A focus of chondrocytes within the epiphysis loses normal growth restraint and proliferates, producing a cartilage-capped mass that undergoes enchondral ossification from within - exactly the mechanism of an osteochondroma, but originating in the epiphysis.
Histology: the lesion is histologically indistinguishable from an osteochondroma. There is a cartilage cap of disorganised but cytologically benign chondrocytes overlying a bony stalk/nidus, with a zone of enchondral ossification at the base. Because the histology is benign and non-specific, the diagnosis is clinical and radiological, not histological - biopsy is reserved for atypical cases.
Behaviour:
- The lesion grows with the child and tends to stop enlarging at skeletal maturity (like an osteochondroma).
- As it grows it can distort the joint surface, create a mechanical block, stretch the capsule and ligaments, and cause angular deformity or limb-length discrepancy.
- Long-standing joint incongruity predisposes to secondary osteoarthritis in adult life.

Classification
The most widely cited classification is by Azouz et al (1985), which grades DEH by the extent of skeletal involvement and correlates loosely with prognosis:
- Localised form: a single epiphysis or one ossification centre is affected (for example, one tarsal bone or one femoral condyle). Best prognosis.
- Classical form: more than one epiphysis within a single lower limb is involved (for example, distal femur plus talus on the same side). This is the typical, most common pattern.
- Generalised form: the entire lower limb from the pelvis to the foot is affected, sometimes with megaepiphyses (enlargement of a whole epiphyseal centre). Worst prognosis, with the greatest deformity and functional burden.
According to PubMed, Azouz and colleagues studied 24 patients (adding 15 new cases) and subdivided DEH into localised, classical and generalised forms, also describing advanced bone age and metaphyseal/growth-plate involvement in some cases (DOI).
LCGLCG - Azouz Forms (Localised, Classical, Generalised)
Hook:LCG = Localised, Classical, Generalised - increasing extent, decreasing prognosis. The Classical (multi-epiphysis, one limb) form is the one you will see most.
Clinical Presentation
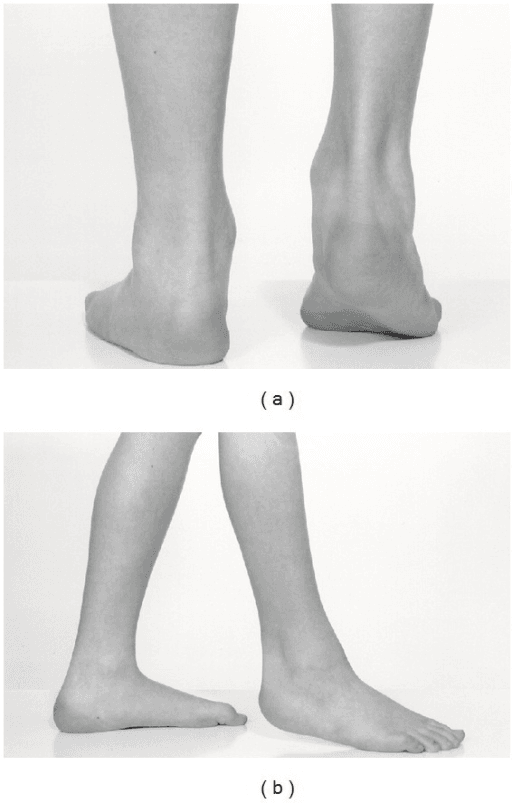
The classic presentation is a young child with a painless or mildly painful hard lump near a joint of one limb, usually noticed by a parent.
Typical features in the history:
- A firm swelling around the ankle or knee, often present for months to years
- Pain in roughly half of patients, often mechanical (worse with activity)
- Limping, deformity (angular or rotational), or a leg-length difference noticed over time
- Restricted or catching joint movement, or a feeling of the joint "locking" when the mass blocks motion
- Strictly one limb - bilateral or crossing-midline involvement should make you doubt the diagnosis
According to PubMed, the foot-and-ankle systematic review found that a mass and pain were the presenting features in 54% of cases, reinforcing the picture of a juxta-articular swelling that may or may not hurt (DOI).
Investigations
Plain radiographs are the first-line investigation and are often diagnostic once the lesion ossifies:
- An irregular, lobulated ossified mass arising from the epiphysis on one side of the joint (medial or lateral half)
- The mass is continuous with the epiphysis and may contain multiple ossific foci that coalesce with time
- Joint surface distortion, angular deformity and sometimes an advanced bone age in the affected epiphysis
- Early in the disease the cartilaginous lesion may be radiographically occult until the ossific nidus appears, which is why a normal radiograph does not exclude DEH in a young child
MAPMAP-IT - Imaging the Lesion
Hook:MAP-IT the lesion: MRI, AP/lateral films, Plan with CT, Identify other sites, Tissue only if atypical.
Differential Diagnosis
The Exam Warning names the mimics ("synovial chondromatosis, intra-articular chondroma, a chondral/parosteal lesion") but the topic never sets out how to tell them apart - and "what else could this be?" is a standard CIM/viva follow-up. Each entity has its own dedicated topic; the point here is the distinction from DEH.
- Key differences from DEH
- Key differences from DEH: Arises from the **metaphysis** with cortex and medulla continuous with the parent bone; EXT1/EXT2-related; multiple form is hereditary
- Clue that settles it
- Clue that settles it: DEH is **epiphyseal/intra-articular, hemimelic, one limb, non-EXT, non-hereditary**
- Key differences from DEH
- Key differences from DEH: **Multiple similarly-sized cartilaginous bodies within the synovium/joint**, not arising from the epiphyseal bone; typically older patients
- Clue that settles it
- Clue that settles it: DEH is a **mass continuous with the epiphysis**; a child with one hemimelic epiphyseal mass, not scattered loose bodies
- Key differences from DEH
- Key differences from DEH: A surface/juxtacortical **cartilage** tumour without the hemimelic epiphyseal pattern
- Clue that settles it
- Clue that settles it: DEH's cartilage cap is **continuous with epiphyseal cartilage** on MRI and respects a limb half
- Key differences from DEH
- Key differences from DEH: **Parosteal, surface-based** osteocartilaginous mass of hands/feet with **no cortico-medullary continuity** and 'blue bone' histology
- Clue that settles it
- Clue that settles it: DEH is **epiphyseal**, one-limb, and continuous with the epiphysis, not a surface lesion of a tubular bone
- Key differences from DEH
- Key differences from DEH: Older patients, cortical destruction, an ill-defined soft-tissue mass or rapid growth
- Clue that settles it
- Clue that settles it: **Atypical features prompt MRI ± biopsy**; DEH is benign, slow-growing and histologically bland
Q: How do you separate Trevor disease from synovial chondromatosis and osteochondroma on the imaging?
A: DEH's cartilage-capped mass is continuous with the epiphyseal cartilage and confined to the medial or lateral half of one limb - unlike an osteochondroma (metaphyseal, cortico-medullary continuity with the parent bone, EXT-related) and unlike synovial chondromatosis (multiple similar-sized cartilaginous bodies lying within the synovium, not arising from the epiphysis, usually older patients). Atypical features (cortical destruction, soft-tissue mass, rapid growth) prompt MRI ± biopsy to exclude a chondral/parosteal malignancy.
Uncommon Sites: Upper Limb, Carpal/Tarsal and Spine
The classification tabs introduce Arealis types 3-6 (upper limb and spine) and the definition notes DEH can arise from an "epiphyseal equivalent such as a carpal or tarsal bone", but these presentations are never developed - and they are exactly where the diagnosis is missed. (The original description by Mouchet and Belot was in fact of the tarsus - "tarsomegalie".)
- Epiphyseal equivalents (carpus and tarsus). The carpal and tarsal bones ossify from a single centre, so a carpal or tarsal bone behaves as an epiphyseal equivalent and can host a DEH lesion. This is why the talus and tarsals are such classic sites, and why a tarsomegaly (enlarged, deformed tarsal bone) is a recognised presentation.
- Upper-limb DEH (Arealis types 3-4). Rare but recognised: lesions of the distal radius/ulna epiphysis or the carpus produce a hard juxta-articular wrist mass, radial or ulnar deviation deformity, reduced forearm/wrist motion and, at the elbow/shoulder, restricted movement. It is easily mistaken for an osteochondroma - the hemimelic, one-limb, epiphyseal pattern and MRI settle it.
- Spinal DEH (Arealis type 6). Exceptionally rare; epiphyseal-equivalent overgrowth from a vertebral element can encroach on the canal or a neural foramen (cord or root compression) or drive a deformity/scoliosis. MRI is essential to map the cartilage and any neural compromise, and treatment is excision/decompression of the symptomatic lesion.
- Why it matters for staging. Because additional sites change the Azouz/Arealis type and prognosis, Arealis recommended a whole-body bone scan to detect clinically silent upper-limb or axial lesions when DEH is confirmed.
Q: Trevor disease is 'lower-limb', so why look elsewhere?
A: Although the lower limb dominates, DEH is recognised in the upper limb (Arealis types 3-4) and rarely the spine (type 6), and it arises from epiphyseal equivalents - the carpal and tarsal bones (the original "tarsomegalie"). Carpal/distal-radius lesions cause a wrist mass with deviation deformity; spinal lesions can compress the cord or a root. Confirming DEH warrants a whole-body bone scan to find silent additional sites, which sets the type and prognosis.
Management Algorithm
There is no high-level evidence and no standardised protocol because the condition is so rare; management is symptom-driven and individualised.
Two broad routes:
- Observation for small, asymptomatic lesions that are not causing deformity or mechanical block. The lesion typically stops growing at skeletal maturity. Monitor clinically and radiologically because unchecked growth makes later surgery harder.
- Surgery (marginal excision) for lesions causing pain, deformity, mechanical block, joint incongruity, instability or limb-length problems, or where progressive growth threatens the joint.
According to PubMed, the foot-and-ankle systematic review reported that surgery was chosen in 92% of patients, of whom 95% underwent mass excision, with recurrence the most frequent complication (about 9%) - reflecting that most reported cases are symptomatic enough to operate on (DOI).
Surgical Technique
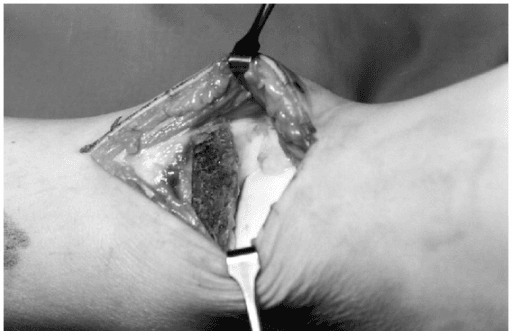
Marginal (intralesional-to-marginal) excision is the workhorse procedure.
Principles:
- Use a direct approach centred on the lesion (for example, a medial approach for a medial talar/distal tibial lesion), protecting nearby tendons, ligaments and the neurovascular bundle
- Expose the mass at its base and excise it flush with the parent epiphysis, removing the cartilage cap as completely as is safely possible - residual cap is the main source of recurrence
- Protect the articular cartilage and physis: do not violate the growth plate; preserve as much joint surface as possible
- Smooth the remaining contour to restore joint congruity; intra-articular loose fragments should be removed
- Complete excision is not always achievable when the lesion is intimately related to the joint surface or physis; the systematic review and Arealis et al both note that even partial excision can be a successful, symptom-relieving treatment (DOI)
EXCISEEXCISE - Operative Checklist
Hook:EXCISE the lesion the right way: expose safely, excise the cap, congruity, injure nothing vital, stabilise/align, evaluate length.
Complications
If the lesion is left untreated or grows unchecked, the natural-history complications are:
- Progressive angular deformity (valgus/varus) and rotational deformity
- Joint incongruity and mechanical block, with stiffness and locking
- Limb-length discrepancy from asymmetric epiphyseal growth
- Joint instability as the mass deforms or stretches the collateral ligaments
- Secondary (early) osteoarthritis of the affected joint in adolescence or adult life - the most important long-term consequence
According to PubMed, Degnan and Ho-Fung emphasise that DEH may result in pain, growth disturbance and early development of osteoarthritis, which is why timely treatment of symptomatic lesions matters (DOI).
RAGIDRAGID - Things That Go Wrong
Hook:Trouble in DEH is RAGID: Recurrence, Arthritis, Growth disturbance, Instability, Damage at surgery.
Postoperative Care and Rehabilitation
Immediate postoperative care:
- Protect the joint: a period of splint/cast immobilisation or protected weight-bearing depending on the site, the extent of excision and any osteotomy performed
- Neurovascular checks after ankle and knee procedures
- Wound care and standard infection surveillance
Rehabilitation:
- Progressive range-of-motion work once the soft tissues have settled, to prevent stiffness around a joint that was often already stiff pre-operatively
- Strengthening and gait re-education, particularly after deformity correction or osteotomy
- For osteotomy/guided-growth cases, follow standard bony-healing and alignment protocols before unrestricted activity
Long-term surveillance (the most important point):
- Continue follow-up until skeletal maturity because the lesion can recur while the child is still growing and new deformity can develop
- Periodic clinical and radiographic review; image any new pain, swelling or deformity promptly
- Counsel the family that recurrence and the late risk of osteoarthritis mean this is a long-term, not a one-off, relationship
WATCHWATCH - Follow-up After Treatment
Hook:WATCH the child after surgery: wound/weight-bear, alignment, till maturity, catch recurrence early, hips-to-toes function.
Outcomes and Prognosis
General prognosis is good for localised, single-limb disease treated appropriately, but it worsens with greater extent of involvement.
- Localised / Azouz localised (Arealis type 1): best outcome; lowest risk of osteoarthritis even without resection
- Classical / multi-epiphysis disease: more deformity and a higher likelihood of needing surgery and developing secondary OA
- Generalised disease: greatest functional burden, more staged procedures, and the highest osteoarthritis risk
Key prognostic messages:
- Resection - even partial - is usually successful in relieving symptoms; complete excision is ideal but not always possible near the joint surface or physis
- Recurrence is common during growth (about 9% in foot-and-ankle disease) and falls after skeletal maturity
- The dominant long-term concern is secondary osteoarthritis from joint incongruity, which is why restoring a congruent, well-aligned joint matters more than simply removing a lump
According to PubMed, Arealis et al concluded that type 1 (single lower-limb) lesions carry the best prognosis with the least chance of developing osteoarthritis, and that resection - even when only partial - can be a successful treatment (DOI).
Guidelines, Registries & Global Practice
Global epidemiology:
- A very rare developmental disorder (about 1 per 1,000,000), with a male predominance (~3:1) and presentation in childhood
- Lower-limb predominance, with the talus and knee epiphyses most often affected; upper limb and spine are uncommon
- No strong racial or geographic predilection has been established given the rarity
Side-by-side principles (consistent across the literature):
- There is no formal national guideline for Trevor disease because of its rarity; practice is driven by case series and systematic reviews (Azouz; Arealis; Artioli; imaging reviews by Tyler and by Degnan/Ho-Fung)
- Diagnosis: clinical pattern plus radiographs and MRI; MRI is universally favoured for the cartilage cap and unossified disease, and to avoid radiation in children
- Classification: the Azouz localised/classical/generalised scheme is the standard reference, with the Arealis six-type system offered as a prognostic refinement
- Treatment: observation for small asymptomatic lesions and marginal excision for symptomatic disease are the globally accepted approaches, with deformity correction (osteotomy or guided growth) as needed
Registry note: Trevor disease is a rare paediatric developmental dysplasia and is not captured by arthroplasty/implant registries (NJR, AJRR, AOANJRR, SHAR, NZJR). The evidence base is single-centre series and pooled literature reviews, not registry data.
High- vs limited-resource variation:
- In well-resourced settings, MRI and CT-based planning, guided-growth implants and intra-articular techniques allow earlier, joint-preserving treatment
- In limited-resource or remote settings, late presentation with larger lesions and established deformity is more common, and treatment relies on excision with simpler imaging and fixation
- Because the condition is rare, referral to a paediatric orthopaedic centre improves diagnosis and outcomes everywhere
MCQ Practice Points
The following points are frequently tested in Orthopaedic exams on Trevor disease.
Q: What does the term "hemimelic" describe in dysplasia epiphysealis hemimelica?
A: It means half a limb - the lesion affects the medial or lateral half of an epiphysis (medial more often than lateral) and is essentially confined to one side of one limb, respecting the midline. Bilateral or midline-crossing disease should prompt you to question the diagnosis.
Q: How does Trevor disease differ from a solitary osteochondroma?
A: The histology is identical (a cartilage-capped bony mass), but DEH is epiphyseal/intra-articular (osteochondroma is metaphyseal), is unilateral within one limb, is sporadic and non-hereditary, and is not associated with EXT1/EXT2 mutations or hereditary multiple exostoses.
Q: Which sites are most commonly affected?
A: The lower limb dominates - the talus (most common single site, especially in foot-and-ankle series) and the distal femur / proximal tibia around the knee. Tarsals, distal tibia and the patella are also reported; upper limb and spine are rare.
Q: What is the single most useful investigation and why?
A: MRI. It shows the cartilage cap continuous with epiphyseal cartilage (the diagnostic feature), detects the lesion before the bony nidus ossifies when radiographs are normal, and maps the lesion to the joint surface, physis and neurovascular structures for surgery.
Q: What is the Azouz classification?
A: Localised (one epiphysis), classical (more than one epiphysis in a single lower limb - the typical pattern), and generalised (whole limb pelvis-to-foot, sometimes with megaepiphyses). Prognosis worsens from localised to generalised.
Q: What is the mainstay of treatment for a symptomatic lesion?
A: Marginal excision of the osteocartilaginous mass, including the cartilage cap, while protecting the physis and articular cartilage. Small asymptomatic lesions can be observed. Deformity is corrected with osteotomy or guided growth, and limb-length discrepancy managed along standard lines.
Q: What is the most common complication after surgery, and what is the key long-term concern?
A: Recurrence (about 9% in foot-and-ankle disease, from incomplete removal of the cartilage cap during growth) is the most common surgical complication. The key long-term concern is secondary (early) osteoarthritis from joint incongruity.
At a Glance
The OnePagerSummary above gives the headline facts. Trevor disease is a rare developmental dysplasia in which cartilage-capped osteochondral masses grow from the epiphyses on one side of one limb in a child. The exam wants you to recognise the pattern, separate it from osteochondroma, use MRI, and manage symptomatic lesions with marginal excision while watching for deformity and recurrence.
TREVORTREVOR - Core Features
Hook:Spell TREVOR to recall the disease named after Trevor: tarsus/knee, rare, epiphyseal, very young boys, one limb, resect if symptomatic.
Summary
Trevor disease (dysplasia epiphysealis hemimelica) is a rare, sporadic developmental disorder in which osteochondroma-like cartilage-capped masses grow from one or more epiphyses on one side of one limb in a child. It is hemimelic (medial or lateral half), epiphyseal/intra-articular, and crucially not EXT-related and not hereditary - this is how it differs from osteochondroma and hereditary multiple exostoses.
Key diagnostic points:
- Young child (male predominance) with a hard, fixed juxta-articular mass on one limb, most often the talus or knee
- MRI is the key investigation, showing the cartilage cap continuous with epiphyseal cartilage and detecting unossified disease
Classification:
- Azouz: localised, classical, generalised (prognosis worsens with extent)
- Arealis: a six-type, prognosis-correlated scheme (type 1 single lower-limb lesion does best)
Management:
- Observe small, asymptomatic lesions with surveillance
- Marginal excision (including the cartilage cap, protecting physis and joint surface) for symptomatic disease, with osteotomy or guided growth for deformity; even partial excision can succeed
Critical exam points: name the hemimelic, one-limb, epiphyseal pattern; distinguish it firmly from osteochondroma/EXT disease; use MRI; treat symptomatic lesions by marginal excision; and counsel about recurrence during growth (~9%) and the long-term risk of secondary osteoarthritis, following the child until skeletal maturity.
Exam Day Cheat Sheet
Must-Know Definition
- **Dysplasia epiphysealis hemimelica (Trevor disease)**: rare, sporadic developmental disorder with osteochondroma-like masses arising from one or more **epiphyses**
- **Hemimelic** = medial OR lateral half of an epiphysis, essentially **one side of one limb**
- **Not EXT-related, not hereditary, not metaphyseal** - this is how it differs from osteochondroma
- Childhood onset, **male predominance ~3:1**, lower-limb dominant
Sites & Classification
- **Most common sites**: talus (ankle) and distal femur/proximal tibia (knee)
- **Azouz**: localised (one epiphysis) - classical (more than one epiphysis, one limb) - generalised (whole limb, megaepiphyses)
- Prognosis worsens from localised to generalised
- **Arealis** six-type scheme: type 1 (single lower limb) has the best prognosis
Investigations
- **Radiographs**: lobulated ossified epiphyseal mass, one side of the joint, with deformity
- **MRI = key test**: cartilage cap continuous with epiphyseal cartilage; detects unossified disease; plans surgery
- **CT** for complex bony/tarsal planning; **bone scan/skeletal survey** to find silent sites
- **Biopsy not routine** - histology mirrors osteochondroma; reserve for atypical cases
Management Principles
- **Observe** small, asymptomatic lesions (with vigilant surveillance)
- **Marginal excision** for pain, deformity, mechanical block, instability or progressive growth
- Remove the **cartilage cap** while protecting the **physis and articular cartilage**
- Correct deformity (**osteotomy or guided growth**) and address limb-length discrepancy
- **Even partial excision can succeed** when complete removal is unsafe near the joint
Complications (High Yield)
- **Recurrence** (~9% in foot-and-ankle disease) - from residual cartilage cap during growth
- **Secondary (early) osteoarthritis** - the key long-term concern, from joint incongruity
- **Angular deformity and limb-length discrepancy** from asymmetric epiphyseal growth
- **Iatrogenic physeal injury / arrest** if the growth plate is violated
- **Neurovascular, tendon or articular cartilage injury** at surgery
Viva Scenario Approach
- State the **hemimelic, one-limb, epiphyseal** pattern up front
- Separate it from **osteochondroma / hereditary multiple exostoses** (not EXT-related)
- Order **MRI** to show the cartilage cap and plan surgery
- Choose **observe vs marginal excision** based on symptoms and deformity
- Counsel about **recurrence during growth** and the **long-term osteoarthritis** risk
- Commit to **follow-up until skeletal maturity**
Quick Exam Tips
- Hemimelic = one half of an epiphysis, one limb only
- Talus and knee epiphyses are the commonest sites
- MRI shows the cartilage cap continuous with epiphyseal cartilage
- Azouz = localised / classical / generalised
- Marginal excision for symptomatic lesions; observe the quiet ones
- Recurrence ~9%; early OA is the main long-term risk
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 6-year-old boy is brought in with a hard lump on the inner side of his right ankle, present for over a year and now mildly painful with sport. The left ankle is normal. On examination there is a firm, non-mobile, bony mass over the medial distal tibia/talus with slightly reduced ankle dorsiflexion. How would you approach this?”
“An 8-year-old girl has confirmed Trevor disease of the distal femoral epiphysis. Over 12 months she has developed a 10-degree valgus deformity at the knee, increasing pain, and catching on deep flexion. What factors guide your decision, and what would you do?”
“A 5-year-old boy had marginal excision of a medial talar Trevor lesion 18 months ago. He now returns with a recurrent medial ankle swelling and early valgus. Radiographs confirm a recurrent ossified epiphyseal mass. How do you manage this?”
Evidence Base
- 25 publications, 70 patients (53 male, 16 female), mean age 9.6 years
- Talus was the most common location; mass and pain were the presentation in 54%
- Surgery in 92% of patients, mass excision in 95% of those operated
- Recurrence was the most frequent complication, about 9% of cases
- Series of 24 patients with 15 new cases added to the literature
- Proposed the localised, classical and generalised subdivision still used today
- Generalised disease may show megaepiphyses (enlargement of a whole epiphyseal centre)
- Described advanced bone age and metaphyseal/growth-plate involvement in some cases