Transphyseal Distal Humerus Fracture
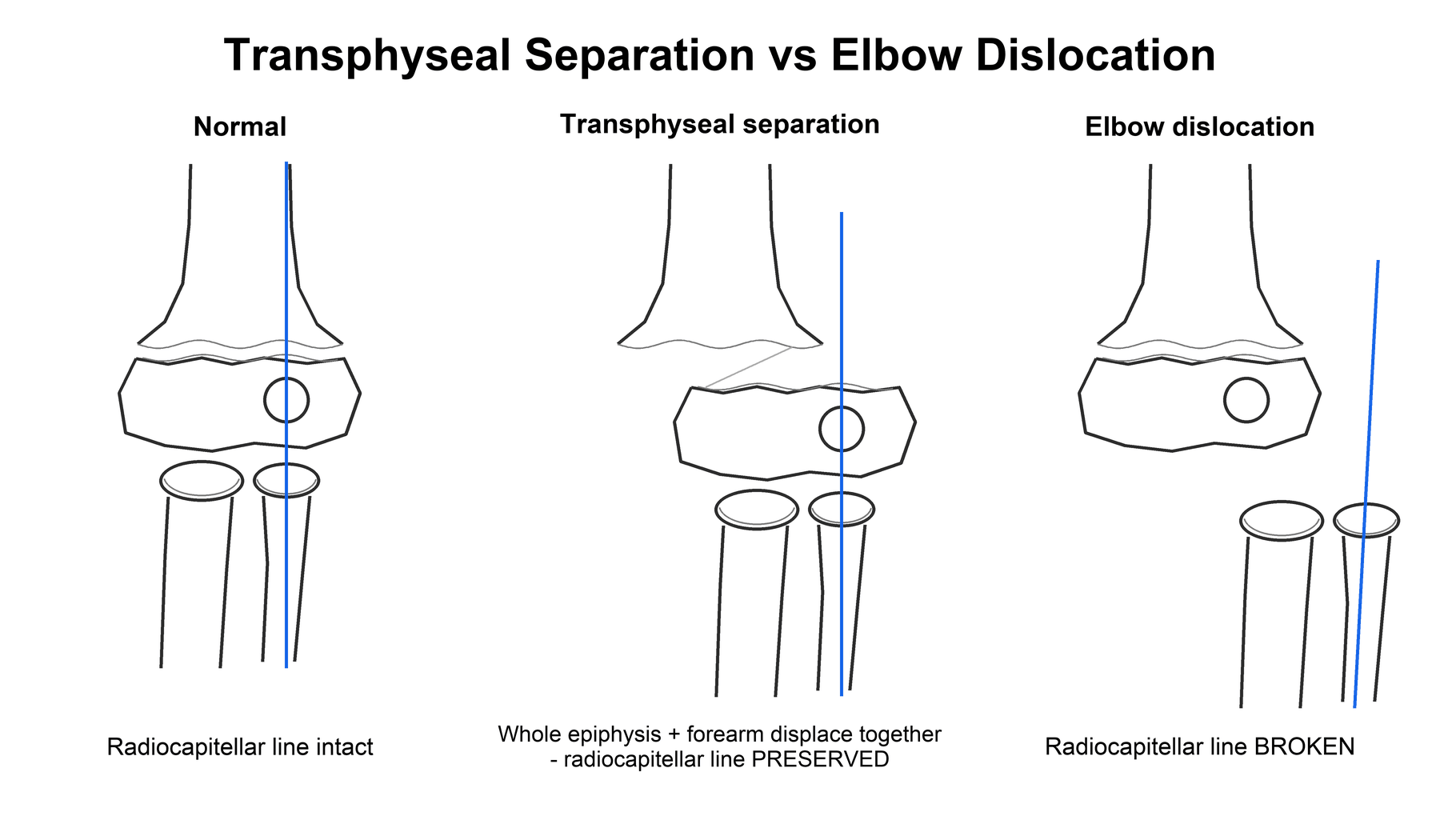
The whole distal epiphysis + forearm displace together (usually posteromedially). The radius and ulna keep their normal relationship to each other and to the capitellum (radio-capitellar line maintained) - only the physis is disrupted. Common in infants/toddlers.
The forearm dislocates relative to the humerus with loss of the radio-capitellar relationship (the radius no longer points at the capitellum). True elbow dislocation is rare under 3 years - so an apparent 'dislocation' in a toddler is usually a transphyseal separation.
Overview & Epidemiology
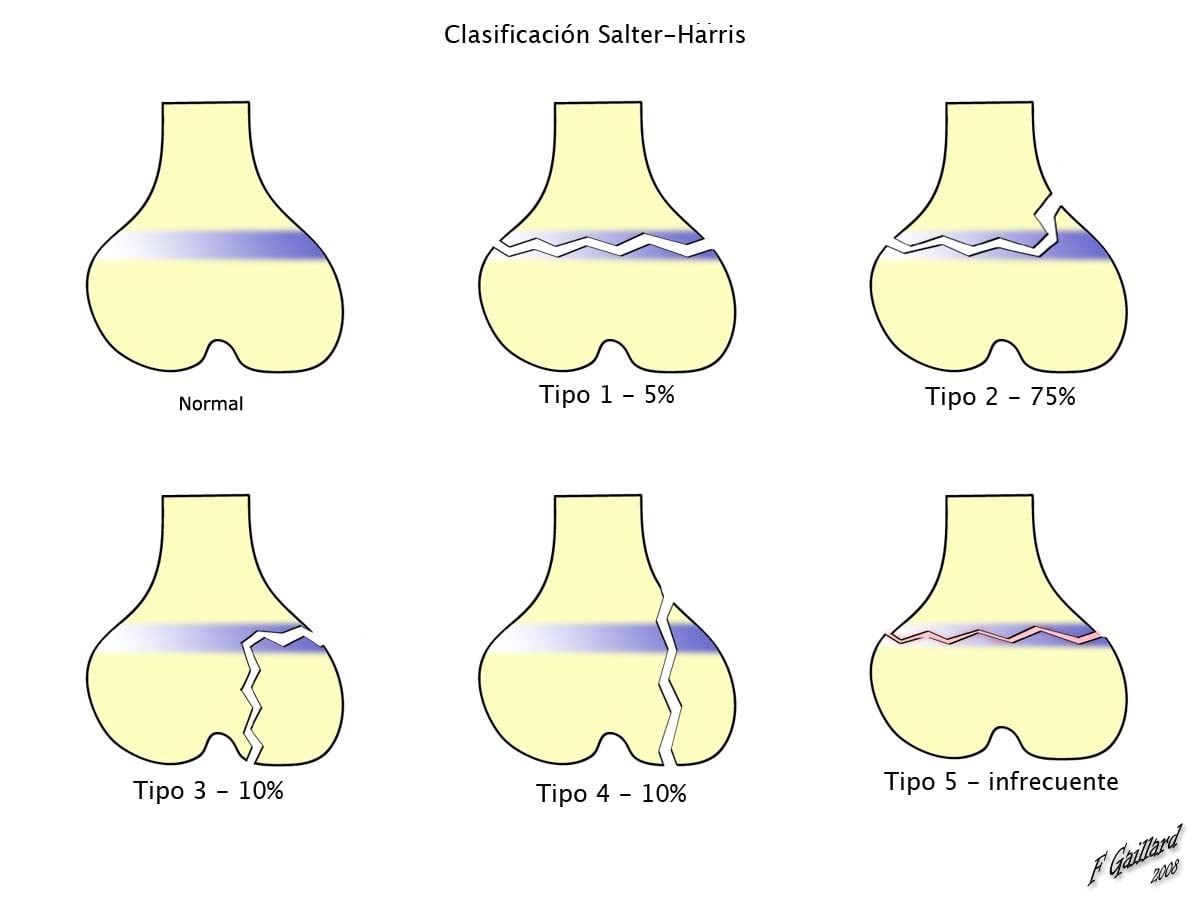
Transphyseal fractures of the distal humerus typically occur in children younger than 3 years. The three classic mechanisms are birth trauma (a difficult delivery), non-accidental trauma, and a fall from a small height. The injury is a physeal separation - in Salter-Harris terms a type I or II - so the entire distal humeral epiphysis (carrying the elbow joint and the forearm) shears off the metaphysis and displaces, most often posteromedially. It is rare, which is itself a trap: unfamiliarity drives the misdiagnosis as an elbow dislocation or a normal elbow.
In infants and toddlers the distal humeral epiphysis is largely cartilaginous - the capitellum ossifies around 1 year and the other centres later (CRITOE) - so the fracture line and the displaced epiphysis are not directly visible on plain radiographs. The clue is MALALIGNMENT of the forearm with the humerus: the forearm axis no longer lines up with the humeral shaft, even though the radius and ulna remain aligned with each other. Comparison with the contralateral elbow, and recognising that the radio-capitellar line is preserved (excluding dislocation), helps make the diagnosis.
Anatomy & Biomechanics
The distal humeral epiphysis ossifies from several centres in the CRITOE order at roughly 1, 3, 5, 7, 9 and 11 years. In the under-3 age group of this injury, often only the capitellum (and sometimes the radial head) has begun to ossify, so most of the epiphysis - and the physis itself - is radiolucent cartilage. That single fact explains the whole diagnostic difficulty: the separation occurs through tissue the X-ray cannot show, and you must read it indirectly from bony alignment and from the position of the ossified capitellum relative to the metaphysis.

The physis is the mechanically weakest link in the immature elbow, so a shear/rotatory force (birth canal forces, a twist, or a fall) separates the epiphysis rather than dislocating the joint. Displacement is typically posteromedial, producing an apparent varus tilt that, if it heals malreduced, becomes cubitus varus. The medial crista of the trochlea / medial condylar ossification centre has a relatively tenuous blood supply, which is why osteonecrosis of the medial condyle is a recognised complication; and because the injury crosses the physis, partial growth arrest and progressive angular deformity are possible.
Classification
Mechanistically the injury is a Salter-Harris type I separation (through the physis only) in the youngest infants, or a type II (with a metaphyseal Thurston-Holland fragment) in slightly older children. The whole epiphysis moves with the forearm, distinguishing it from an isolated condylar fracture.
Clinical Assessment
- A young child (under 3) with a swollen, painful elbow and pseudoparalysis of the arm
- Often birth-related (presents in the first days of life) or after a fall/abuse
- Crepitus or a muffled "bag of bones" feel; assess the neurovascular status of the limb
- A history that does not fit the injury, or delayed presentation, should raise concern
In the under-3 age group this is a recognised abuse-associated fracture. Inconsistent or absent mechanism, other bruises/injuries, or carer behaviour that does not fit should trigger the local safeguarding pathway - examine fully for other injuries and involve child protection.
A transphyseal distal humerus fracture is a recognised abuse-associated injury in the under-3 age group. Where the mechanism is unclear or inconsistent, where there are other injuries, or where presentation is delayed, follow your local safeguarding pathway (full history, examination for other injuries, skeletal survey, social/child-protection involvement) alongside treating the fracture.
A neonate or infant who will not move the arm has pseudoparalysis (pain-driven non-use), and a transphyseal separation is only one cause - the examiner wants the full differential. The must-exclude is septic arthritis of the elbow or proximal humeral osteomyelitis: an irritable, often febrile baby with raised CRP/ESR, in whom ultrasound-guided aspiration is mandatory before attributing the non-use to a fracture. Distinguish obstetric brachial plexus palsy (a neurological flaccid 'waiter's tip' posture that is relatively painless and lacks the swelling/crepitus of a fracture) and a clavicular or proximal-humeral physeal birth fracture (also presents as pseudoparalysis after a difficult delivery). Plain films, both-elbow comparison and - where infection is possible - inflammatory markers and aspiration sort these out; never assume the cartilaginous transphyseal injury without excluding sepsis.
Investigations & Imaging
Obtain plain radiographs of both elbows (AP and lateral) for comparison. Because the epiphysis is cartilaginous, look for indirect signs:
- the forearm is not aligned with the humerus, while the radius and ulna stay aligned with each other;
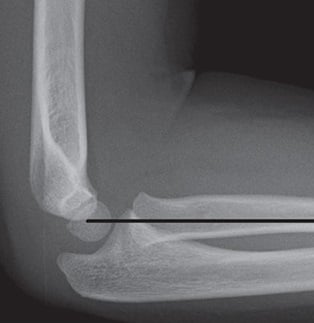
- the radio-capitellar line is preserved (the radial shaft axis points at the capitellum) - excluding dislocation;
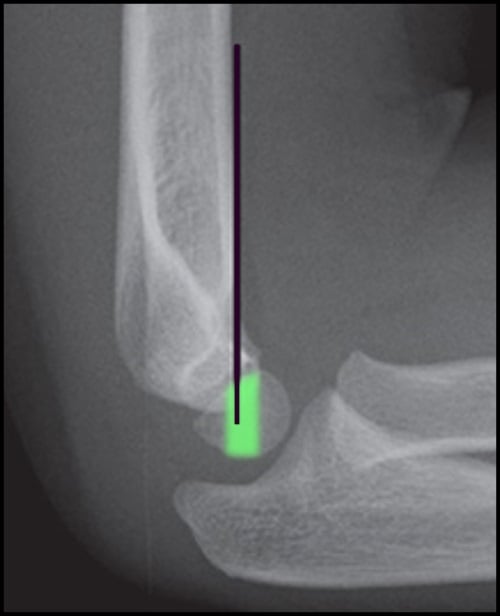
- the ossified capitellum moves with the proximal radius/ulna (posteromedially) relative to the metaphysis;
- a small metaphyseal (Thurston-Holland) flake may be the only bony sign in Salter-Harris II.
To actually demonstrate the cartilaginous epiphysis and confirm reduction, use:
- Intra-operative arthrogram - the commonest adjunct; outlines the epiphysis and confirms an accurate reduction before and after pinning;
- Ultrasound - no ionising radiation, shows the unossified epiphysis and its displacement, increasingly used at the bedside in neonates;
- MRI - definitive for cartilage but rarely needed acutely (and often requires sedation in this age).
Management Algorithm
Treatment is guided by displacement, age and the soft tissues, and mirrors supracondylar fracture principles. The aims are an anatomic reduction to restore the carrying angle and to protect the physis and its blood supply.
Immobilisation in an above-elbow cast/splint with close radiographic follow-up. Infants have enormous remodelling potential, so minor residual displacement in the plane of movement is well tolerated - but malalignment in the varus/valgus plane is not, so watch the carrying angle.
Surgical Technique
Under general anaesthesia, with image intensifier, apply longitudinal traction and correct the typical posteromedial displacement (and any rotation). Because the landmarks are cartilaginous, judge reduction by forearm-humerus alignment and confirm it with an arthrogram (a small volume of contrast into the joint outlines the epiphysis).
Complications
- Cause / note
- MOST common; from malunion (malreduction) - an alignment/cosmetic deformity
- Cause / note
- Vascular insult to the tenuous medial condylar blood supply
- Cause / note
- Physeal injury causing partial arrest, angular deformity or length issue
- Cause / note
- Cartilaginous epiphysis mistaken for dislocation or a normal elbow
If a cubitus varus deformity becomes established from malunion, it can be corrected later with a lateral closing-wedge (supracondylar) osteotomy to restore a near-normal carrying angle. Prevention - through accurate initial reduction confirmed on arthrogram - is far preferable.
The same tenuous central blood supply that produces medial-condyle osteonecrosis can cause a fishtail deformity of the distal humerus - a recognised late sequela of distal humeral physeal injury. Osteonecrosis or a growth disturbance of the central (trochlear/medial-condylar) portion of the physis leaves a V-shaped fishtail notch in the distal humeral metaphysis (the lateral and medial pillars grow while the centre does not). It is usually a delayed, often initially asymptomatic radiographic finding, but can cause ulnar deviation, stiffness and pain, and may predispose to a later condylar fracture and to ulnar-nerve symptoms. It is a key reason to follow these children well beyond union rather than discharging at fracture healing - the deformity declares itself only with continued growth.
Postoperative Care & Rehabilitation
The elbow is protected in an above-elbow cast for around 3-4 weeks (union is rapid at this age). Pins are removed in clinic once the fracture is united, and gentle range-of-motion returns quickly - infants and toddlers regain elbow movement readily and rarely need formal physiotherapy. Provide simple pin-site care advice and watch for pin-site irritation/infection.
Because the injury crosses the physis, follow-up should continue beyond union to detect progressive cubitus varus or growth disturbance. Counsel families that the carrying angle and any subtle deformity are best judged over months, and re-examine the contralateral elbow for comparison at review.
Outcomes & Prognosis
With timely diagnosis and restoration of alignment, outcomes are generally good: small published series report union with full range of motion and few deformities requiring further surgery. The dominant determinant of a poor result is late or missed diagnosis (the cartilaginous epiphysis) and residual varus/valgus malalignment. The main long-term issues are cubitus varus (cosmetic/alignment, correctable by osteotomy) and, less often, medial-condyle osteonecrosis or growth arrest - which is why follow-up continues past union.
Guidelines, Registries & Global Practice
There is no dedicated registry for this rare injury, and management is extrapolated from paediatric supracondylar fracture principles, which national bodies address directly (e.g. BOA/BOAST standards in the UK, and AAOS/POSNA guidance in North America) - emphasising timely assessment, neurovascular documentation and appropriate-urgency surgery. The one point with strong global consensus specific to this injury is the safeguarding obligation: across health systems (e.g. NICE/RCPCH child-maltreatment guidance in the UK and equivalent mandatory-reporting frameworks elsewhere), an unexplained or inconsistent fracture in a child under 3 must trigger a non-accidental-injury assessment including a skeletal survey. Practice on fixation vs casting in neonates varies by centre and resource setting, united by the principle that restoring alignment and protecting the physis matters more than the specific construct.
Mnemonics & Memory Aids
CRITOE
Hook:CRITOE at 1-3-5-7-9-11 years: in a transphyseal fracture most of the epiphysis is unossified, which is exactly why it is invisible on X-ray.
INFANT
Hook:An INFANT's elbow: malaligned forearm, think NAI, arthrogram, not a dislocation, pin it.
VANG
Hook:VANG: varus, AVN, malalignment sign, growth arrest - the transphyseal fracture essentials.
MCQ Practice Points
Q: A 2-year-old has a swollen elbow after a fall; the forearm is not aligned with the humerus but the radial shaft still points at the capitellum. Most likely diagnosis? A: Transphyseal distal humeral separation - the preserved radio-capitellar line excludes a dislocation, and true dislocation is rare under 3.
Q: Why can a displaced transphyseal fracture look almost normal on a plain radiograph? A: The distal humeral epiphysis is largely cartilaginous in the under-3 age group (only the capitellum has usually ossified - CRITOE 1-3-5-7-9-11 years), so the physis and the displaced epiphysis are radiolucent; the diagnosis is inferred from forearm-humerus malalignment.
Q: What single intra-operative investigation best confirms reduction of the cartilaginous epiphysis? A: An arthrogram (ultrasound or MRI are alternatives) - it outlines the epiphysis and confirms alignment before and after pinning.
Q: What is the most common late complication, and how is an established case corrected? A: Cubitus varus from malunion; an established deformity is corrected with a lateral closing-wedge (supracondylar) osteotomy.
Q: A transphyseal distal humerus fracture in a 10-month-old with no clear mechanism - what must you not forget? A: It is a recognised non-accidental-injury pattern - undertake a safeguarding assessment including a skeletal survey.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-month-old presents with a swollen elbow and is not using the arm; the parent's account of the injury is vague. Radiographs suggest the forearm is not aligned with the humerus. What is your diagnosis, how do you confirm it, and what else must you consider?”
“How would you treat a displaced transphyseal distal humerus fracture, and what complications would you warn about?”
“The radiology report on a 2-year-old's elbow says 'lateral condyle fracture'. The whole forearm looks displaced posteromedially with the capitellum. How do you reconcile this, and how does the CRITOE sequence help your interpretation?”
Who & how
- Children under 3; birth trauma, NON-ACCIDENTAL trauma, or low fall
- Separation through the distal humeral physis (SH I/II); whole epiphysis + forearm displace (usually posteromedial)
- Recognised abuse-associated injury - screen for NAI
Diagnosis
- Epiphysis cartilaginous so not directly visible on plain films (CRITOE 1-3-5-7-9-11y)
- Clue: forearm NOT aligned with humerus, but radio-capitellar line PRESERVED (vs dislocation)
- Confirm with arthrogram (or ultrasound/MRI); compare contralateral elbow
Treatment
- Displaced: closed reduction + percutaneous pinning (like supracondylar), arthrogram-assisted
- Undisplaced/neonate: immobilisation + close follow-up (high remodelling potential)
- Aim: anatomic reduction to restore carrying angle, protect physis/blood supply
Complications
- Cubitus varus (most common, malunion) corrected by lateral closing-wedge osteotomy if established
- Medial condyle osteonecrosis; growth arrest
- Missed diagnosis from the invisible cartilaginous epiphysis
At a Glance - Rapid Reference
- Key point
- Children under 3 (birth trauma, non-accidental injury, low-energy fall)
- Key point
- Salter-Harris I/II separation through the distal humeral physis; whole epiphysis + forearm displace, usually posteromedially
- Key point
- Recognised abuse-associated injury - screen for non-accidental injury
- Key point
- Forearm NOT aligned with humerus, but radio-capitellar line PRESERVED
- Key point
- Arthrogram (intra-operative), ultrasound, or MRI - the epiphysis is cartilaginous
- Key point
- Displaced: closed reduction + percutaneous pinning (like supracondylar); undisplaced: cast
- Key point
- Cubitus varus (commonest), medial-condyle osteonecrosis, growth arrest, missed diagnosis
Evidence & Key Studies
Fracture-separation of the distal humeral epiphysis
- Original series of 16 patients defining the injury: ALL showed posteromedial displacement of the distal humeral epiphysis on the initial radiograph - the cardinal diagnostic sign.
- Child abuse was documented or suspected in 6 of the 16 fractures - establishing the non-accidental-injury association.
- Treated by closed reduction and immobilisation (elbow 90 degrees flexion, forearm pronated, 3 weeks); cubitus varus developed in 3 from inadequate reduction but did not progress.
Transphyseal Fracture of the Distal Humerus
- Typically occurs in children younger than 3 years from birth trauma, non-accidental trauma, or a fall from a small height; prompt accurate diagnosis is crucial.
- Recognising that the forearm is not aligned with the humerus on plain radiographs aids diagnosis; surgery is most commonly performed with the aid of an arthrogram (closed reduction and percutaneous pinning, as for supracondylar fractures).
- The most common complication is cubitus varus from malunion (also medial-condyle osteonecrosis and growth arrest); a corrective lateral closing-wedge osteotomy can restore the carrying angle.
The original description - posteromedial displacement as the cardinal sign, the abuse association (6 of 16) and cubitus varus from inadequate reduction - is the DeLee et al. series, which also underpins the DeLee classification (J Bone Joint Surg Am 1980;62(1):46-51, PMID 7351415). The age group, mechanisms (including non-accidental trauma), the forearm-humerus malalignment clue, arthrogram-assisted CRPP and the complication profile come from the Abzug et al. review (DOI); the neonatal diagnostic-and-outcome data from the Galeotti et al. case series (DOI); the quantitative imaging/misdiagnosis and complication figures from the Nguyen et al. systematic review (DOI); and the reduction-quality/outcome comparison from the Chen et al. series (DOI). The CRITOE ossification sequence and the Salter-Harris and DeLee classifications are standard, long-established paediatric concepts. (See also our Supracondylar Humerus Fracture, Lateral Condyle Fractures and Physis topics.)