A1 Pulley | Stenosing Tenosynovitis | Injection | Release
Green Classification
Critical Must-Knows
- A1 Pulley: Location of stenosis at MCP level. Release A1, NOT A2.
- Ring and Middle Fingers: Most commonly affected digits.
- Steroid Injection: 70% success rate. Lower in diabetics (50%).
- A2 Pulley: CRITICAL - never release. Causes bowstringing if released.
- Diabetics: 10% prevalence, multiple digits, lower injection success.
Clinical Pearls
- "Palpable nodule at A1 (MCP level)
- "Worse in morning (tissue edema)
- "Diabetics: 10% prevalence, multiple fingers
- "Preserve A2 = fundamental principle
Clinical Imaging
Imaging Gallery



Critical Trigger Finger Exam Points
A1 Pulley Location
Stenosis occurs at A1 pulley (MCP level). Nodule in flexor tendon catches at pulley during motion. Release A1, never A2.
Preserve A2 Pulley
A2 is critical for tendon function. Releasing A2 causes bowstringing and loss of grip. A2 and A4 are the critical pulleys.
Diabetic Trigger Finger
10% prevalence in diabetics. Multiple digits common. Injection success only 50%. May need surgery first-line.
Injection Technique
Inject into tendon SHEATH, not tendon. At A1 pulley level. 70% success. May repeat once. Avoid tendon injection.
Quick Decision Guide
| Grade | Presentation | Treatment | Key Action |
|---|---|---|---|
| Grade 1 | Pain only, no catching | Conservative, splint | Trial of splint and activity modification |
| Grade 2 | Catching, active extension OK | Injection first | 70% success with steroid injection |
| Grade 3 | Locking, passive unlock needed | Injection or surgery | Consider surgery if injection fails |
| Grade 4 | Fixed locked | Surgery | A1 pulley release indicated |
A1-A2-A3-A4-A5Annular Pulley System
| A1 | MP level Release for trigger finger |
| A2 | Proximal phalanx CRITICAL - do NOT release |
| A3 | PIP level Minor pulley |
| A4 | Middle phalanx CRITICAL - do NOT release |
| A5 | DIP level Minor pulley |
| A1 | MP level Release for trigger finger | A4 | Middle phalanx CRITICAL - do NOT release |
| A2 | Proximal phalanx CRITICAL - do NOT release | A5 | DIP level Minor pulley |
| A3 | PIP level Minor pulley |
Hook:A2 and A4 are the CRITICAL pulleys - never release them! A1, A3, A5 are minor and can be released safely.
DRAGTrigger Finger Risk Factors
| D | Diabetes 10% prevalence, multiple digits, lower injection success |
| R | Rheumatoid arthritis Inflammatory tenosynovitis |
| A | Age (50-60 years) Peak incidence |
| G | Gripping repetitively Occupational exposure |
| D | Diabetes 10% prevalence, multiple digits, lower injection success | A | Age (50-60 years) Peak incidence |
| R | Rheumatoid arthritis Inflammatory tenosynovitis | G | Gripping repetitively Occupational exposure |
Hook:DRAG = Diabetes, RA, Age 50-60, Gripping - know the risk factors for trigger finger!
SHEATHInjection Technique
| S | Steroid Triamcinolone or methylprednisolone |
| H | Horizontal at MCP Inject at MCP crease |
| E | Enter sheath Into sheath, NOT tendon |
| A | Aspirate first Ensure not in tendon |
| T | Test resistance Low resistance = in sheath |
| H | Half ml steroid 0.5ml steroid + 0.5ml LA |
| S | Steroid Triamcinolone or methylprednisolone | E | Enter sheath Into sheath, NOT tendon | T | Test resistance Low resistance = in sheath |
| H | Horizontal at MCP Inject at MCP crease | A | Aspirate first Ensure not in tendon | H | Half ml steroid 0.5ml steroid + 0.5ml LA |
Hook:SHEATH = where you inject! Into the tendon sheath, not the tendon itself.
Overview and Epidemiology
Why Trigger Finger Matters
Trigger finger is extremely common in the exam. Key points: A1 pulley location, preserve A2, injection 70% success, diabetics have higher prevalence and lower injection response.
Trigger Finger (stenosing tenosynovitis) is catching or locking of a digit due to stenosis at the A1 pulley.
Demographics
- Prevalence: 2-3% general population
- Gender: Female greater than male (6:1)
- Age: Peak 50-60 years
- Digits: Ring greater than middle greater than thumb greater than index greater than small
Middle-aged women are the classic demographic.
Risk Factors
- Diabetes: 10% prevalence (vs 2% general)
- Rheumatoid arthritis: Inflammatory tenosynovitis
- Gout: Crystal-induced
- Repetitive gripping: Occupational
- Carpal tunnel: Associated conditions
Screen diabetics for trigger finger.
Pathophysiology and Mechanisms
Pulley Anatomy
There are 5 annular pulleys (A1-A5) and 3 cruciate pulleys (C1-C3). A2 and A4 are CRITICAL for tendon function - never release them. A1, A3, A5 are minor and can be safely released.
Flexor Tendon Sheath Anatomy:
- A1 Pulley: At MCP joint level - where trigger finger occurs
- A2 Pulley: Over proximal phalanx - CRITICAL, do not release
- A3 Pulley: At PIP joint level - minor
- A4 Pulley: Over middle phalanx - CRITICAL, do not release
- A5 Pulley: At DIP joint level - minor
Pathophysiology:
- Repetitive friction causes tendon sheath thickening at A1
- Nodule forms in flexor tendon (FDS or FDP)
- Nodule catches at narrowed A1 pulley
- Results in catching, triggering, or locking
Classification Systems
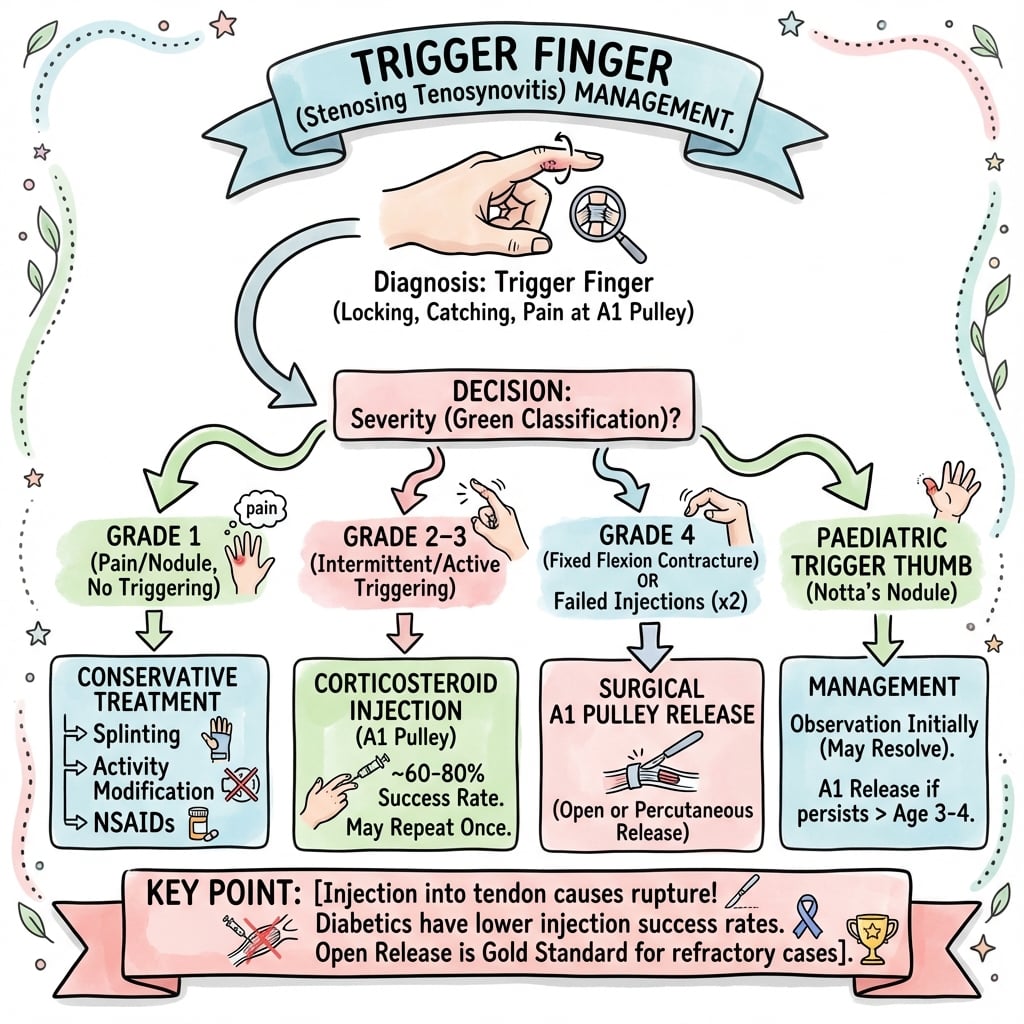
Green Severity Grading
| Grade | Description | Clinical Features | Treatment |
|---|---|---|---|
| Grade 1 | Pain, palpable nodule | History of catching, no demonstrable catching | Splinting, activity modification |
| Grade 2 | Catching | Demonstrable catching, can actively extend | Steroid injection (70% success) |
| Grade 3 | Locking | Requires passive extension to unlock | Injection or surgery |
| Grade 4 | Fixed locked | Unable to passively extend the digit | Surgical release indicated |
Higher grades progressively more likely to need surgery.
Clinical Assessment
History
- Catching or clicking: During flexion/extension
- Locking: May need passive unlock
- Worse in morning: Tissue edema after rest
- Pain at palm: Over MCP crease
- Progressive: Gets worse over time
Ask about diabetes and occupation.
Examination
- Palpable nodule: At A1 pulley (MCP crease)
- Tenderness: Over A1 pulley
- Triggering: Demonstrable with flexion/extension
- Grade: Can actively extend, needs passive, or fixed?
- Other fingers: Check all digits
Always palpate at the MCP crease, not PIP.
Differential Diagnosis
Distinguishing Trigger Finger from Mimics
| Condition | Key feature | Discriminator from trigger finger |
|---|---|---|
| Trigger finger | Palpable nodule at A1 (MCP crease) with catching/locking on flexion | Triggering reproduced; nodule moves with tendon |
| Dupuytren's disease | Palpable cord/nodule in palmar fascia, fixed flexion contracture | Cord is superficial and fixed; no triggering, no active unlocking |
| MCP/PIP joint pathology (OA, loose body) | Mechanical locking with joint-line tenderness, crepitus | Locking is at the joint, not the pulley; radiographs abnormal |
| Sagittal band rupture (boxer's knuckle) | Extensor tendon subluxation at MCP, snapping on extension | Dorsal not volar; snapping on extension over the knuckle |
| Inflammatory/infective flexor tenosynovitis | Diffuse sheath swelling, Kanavel signs if septic | No discrete nodule; systemic/inflammatory features, pain on passive extension |
| FDS/FDP anomaly or partial tendon laceration | Mechanical catching without nodule, often post-injury | History of trauma; no A1 nodule; may need imaging |
Investigations
Investigation Protocol
Clinical diagnosis in most cases. Palpable nodule at A1 with triggering is pathognomonic. No imaging needed routinely.
HbA1c or fasting glucose if not known diabetic. Diabetics have 10% trigger finger prevalence and need careful counseling about lower injection success.
Rarely required. Can show tendon sheath thickening, A1 pulley thickening, tendon nodule. Useful if diagnosis uncertain.
No imaging is required for typical trigger finger with clear clinical findings.
Management Algorithm
Non-Operative Management
Conservative Options
Reduce gripping activities. Especially repetitive gripping. Modify work tasks if occupational.
Night splint keeping MCP in extension. Prevents tendon nodule catching overnight. Variable success.
Short-term anti-inflammatory. May reduce symptoms but won't resolve stenosis.
Conservative treatment has limited long-term success as sole treatment.
Surgical Technique
Open A1 Pulley Release
Surgical Steps
Local anesthesia. Wide-awake local anesthesia no tourniquet (WALANT) preferred. Hand on table.
Transverse incision at MCP crease. 1-1.5cm. Follow skin crease for cosmesis.
Blunt spread to expose A1 pulley. Identify and protect digital nerves (lateral).
Incise A1 pulley longitudinally. Divide completely. STOP at A2.
Test tendon excursion. Ask patient to flex/extend. Confirm no triggering.
Skin only. Interrupted sutures or steri-strips. Soft dressing.
Simple, quick procedure (less than 10 minutes). LA suitable.
Complications
Complications of Trigger Finger Treatment
| Complication | Incidence | Prevention/Management |
|---|---|---|
| Incomplete release | 5% | Ensure complete A1 division, check glide |
| Digital nerve injury | Less than 1% | Direct vision, stay central, protect nerves |
| Bowstringing | Rare | NEVER release A2 - critical pulley |
| Infection | Less than 1% | Sterile technique |
| Stiffness | 5% | Early motion, hand therapy if needed |
| Recurrence | Less than 3% | Complete release, address underlying disease |
A2 pulley injury causing bowstringing is a serious complication. Prevention is key - know anatomy.
Postoperative Care
Postoperative Protocol
Soft dressing. Immediate finger ROM encouraged. No splint needed.
Active and passive ROM. Full motion as tolerated. Keep wound dry.
Remove sutures. Most patients fully functional by this point. Scar massage.
Return to all activities. Including gripping and lifting. Scar tenderness may persist.
Return to work: Light duties immediately. Full duties 2-4 weeks.
Outcomes and Prognosis
Success Rates:
- Conservative (splint): Variable (30-40%)
- Injection: 70% (lower in diabetics - 50%)
- Surgery: 95-100%
Prognostic Factors:
| Factor | Better Outcome | Worse Outcome |
|---|---|---|
| Duration | Short (under 6 months) | Long (over 1 year), fixed locked |
| Diabetes | Non-diabetic | Diabetic (50% injection success) |
| Grade | Lower grade | Higher grade (4 = surgery) |
| Digits | Single digit | Multiple digits |
Most patients do very well with injection or surgery.
Controversies and Areas of Uncertainty
Number of injections before surgery
Most surgeons offer one or two injections before recommending release, but the optimal ceiling is debated. With recurrence around 56% at one year (Rozental 2008), some advocate proceeding to surgery sooner, particularly in high-risk patients, rather than repeating injections of diminishing benefit.
Open vs percutaneous release
Randomised data show equivalent clinical outcomes for open and percutaneous (including ultrasound-guided) release. Percutaneous is faster and incisionless but carries a higher theoretical risk of digital nerve injury and incomplete release, especially in the thumb. Choice is largely operator-expertise dependent.
Ultrasound guidance for injection
Ultrasound-guided injection improves accuracy and may speed early recovery, but several trials show no difference in 3-6 month outcomes versus a blind landmark-based injection. Routine use is not yet standard and depends on availability.
Diabetics: inject or operate first?
Injection success is markedly lower in diabetes (≈30-50%) and type 1 patients respond poorly. Whether to attempt injection at all in insulin-dependent diabetics, given transient glycaemic disturbance and low success, remains a point of practice variation.
Paediatric trigger thumb is different
Paediatric trigger thumb (Notta's node) is a distinct entity, not adult stenosing tenosynovitis. Many resolve spontaneously in the first years of life; surgery is considered for persistent fixed flexion, and injection has little role. Do not extrapolate adult management to children.
Evidence Base
- Two RCTs, 63 participants pooled
- Corticosteroid plus lidocaine superior to lidocaine alone at 4 weeks (RR 3.15, 95% CI 1.34 to 7.40)
- Number needed to treat to benefit = 3
- Benefit lasted up to 4 months in one trial; no adverse events reported
- Double-blind RCT, 50 adults in general practice
- Triamcinolone vs saline: satisfactory immediate response 16/25 vs 5/25 (p less than 0.001)
- Greater reduction in pain and perceived improvement with steroid
- Beneficial effect maintained across 12 months of follow-up
- 118 trigger digits (98 nondiabetic, 26 diabetic)
- Injection success: nondiabetics 57% vs diabetics 32% (p = 0.04)
- All 5 type 1 diabetic digits failed injection and required surgery
- Surgical A1 release successful in 71/72 (99%), no excess complications in diabetics
- 124 digits prospectively followed for 1 year after injection
- 56% had symptom recurrence (median 5.6 months); freedom from recurrence 70% at 6 months, 45% at 12 months
- Insulin-dependent diabetes, younger age, multiple digits and other upper-limb tendinopathies predicted failure
- Duration and severity of symptoms did NOT predict outcome
- 62 resistant trigger digits randomised to open vs percutaneous A1 release
- Ultrasound-measured bowstringing increased at 12 weeks in both groups, greater after open release
- Bowstringing resolved by 24 weeks with no inter-group difference
- No association between bowstringing and any clinical outcome
- 72 grade 2+ trigger digits randomised to open surgery vs ultrasound-guided needle release
- Both groups improved significantly in VAS and Quinnell grade at 7 and 30 days
- No significant difference between techniques at any timepoint up to 180 days
- Level II therapeutic evidence
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Classic Trigger Finger
"A 55-year-old woman has catching in her ring finger for 2 months. She feels a click at the palm and sometimes needs to straighten the finger with her other hand. There is a tender nodule at the MCP crease. What is your management?"
Scenario 2: Diabetic with Multiple Triggers
"A 60-year-old diabetic man has triggering in his ring, middle, and index fingers. He has had one injection to each finger with only partial improvement. What is your approach?"
Scenario 3: Fixed Locked Finger
"A 70-year-old woman presents with her middle finger locked in flexion for 2 weeks. She cannot straighten it actively or passively. Her MCP is tender. What is your management?"
MCQ Practice Points
A1 Pulley Location
Q: At what level does trigger finger occur? A: A1 pulley at the MCP joint level. This is where the stenosis and nodule catching occurs.
Critical Pulley
Q: Which pulley must be preserved during trigger finger release? A: A2 pulley. A2 and A4 are critical for tendon function. Releasing A2 causes bowstringing.
Injection Success
Q: What is the success rate of steroid injection for trigger finger? A: 70% in general population. Only 50% in diabetics.
Diabetes Prevalence
Q: What is the prevalence of trigger finger in diabetics? A: 10% (vs 2-3% general population). Multiple digits common. Lower injection success.
Most Common Digit
Q: Which digit is most commonly affected in trigger finger? A: Ring finger (30%), followed by middle (25%), thumb (20%), index (15%), small (10%).
WALANT Technique
Q: What is WALANT and why is it ideal for trigger finger release? A: Wide Awake Local Anesthesia No Tourniquet. Allows patient to actively flex/extend to confirm complete release and resolution of triggering.
Guidelines, Registries & Global Practice
Global epidemiology: Lifetime prevalence is approximately 2-3% in the general population, rising to 5-20% in people with diabetes. Peak onset is in the fifth-to-sixth decade, with a female predominance (roughly 2-6:1 across series). Trigger finger is one of the commonest reasons for elective hand surgery worldwide and is a recognised marker of impaired glucose tolerance.
Side-by-side guidance:
| Body / Source | First-line | Surgery | Notable position |
|---|---|---|---|
| AAOS / ASSH (US) | Corticosteroid injection for adult primary trigger finger | Reserved for failed injection or fixed locking | Injection is the default initial intervention |
| BSSH / BOA (UK) | Single corticosteroid injection; up to two before surgery | Open A1 release if injections fail | Emphasises informed consent re digital nerve and recurrence |
| Consensus (EFORT / European hand societies) | Injection, with splinting as adjunct | Open or ultrasound-guided percutaneous release | Percutaneous release accepted where expertise exists |
| General principle | Stepwise: activity modification then injection | Definitive A1 release | Diabetics counselled toward earlier surgery |
Registry and outcome data: Trigger finger is not tracked by arthroplasty registries (no implant), so the evidence base is observational and trial-derived rather than registry-derived. Pooled trial and cohort data consistently show injection short-term success of roughly 55-70% (markedly lower in diabetes, ~30-50%), recurrence in around half of patients by one year, and open surgical release success exceeding 95% with complication rates under 3%.
High- vs limited-resource practice variation:
- High-resource settings: Office-based injection, WALANT release, and increasing use of ultrasound-guided percutaneous release; readily available hand therapy.
- Limited-resource settings: Greater reliance on a single definitive open release to avoid repeat visits; injection still first-line where steroid is accessible. Ultrasound guidance is less available, so blind injection and open release predominate.
Medicolegal/consent essentials (universal): Document grade and prior treatment, and consent specifically for digital nerve injury, incomplete release/recurrence, infection, and the principle of A1 release with A2 preservation. Record diabetes status and the counselling given about lower injection success.
TRIGGER FINGER
Clinical summary
Pathology
- •Stenosing tenosynovitis at A1 pulley
- •Ring greater than middle most common
- •Nodule catches at narrowed pulley
- •Diabetics: 10% prevalence
Clinical
- •Catching/locking with flexion
- •Worse in morning
- •Palpable nodule at MCP crease
- •Tender at A1 pulley
Green Classification
- •1: Pain, no catching
- •2: Catching, active extension
- •3: Locking, passive unlock
- •4: Fixed locked = surgery
Treatment
- •Injection: 70% success (50% diabetics)
- •Surgery: 95%+ success
- •Grade 4 = surgery first-line
- •Can repeat injection once if partial response
Surgical Principle
- •Release A1 pulley completely
- •PRESERVE A2 pulley (critical)
- •Check tendon glide
- •Protect digital nerves (lateral)
Key Points
- •A2 and A4 = critical pulleys
- •Diabetics: 10% prevalence
- •Ring finger most common
- •Multiple digits in diabetics