Second Most Common Carpal Fracture | Dorsal Chip Pattern | FOOSH Mechanism
TRIQUETRAL FRACTURE TYPES
Critical Must-Knows
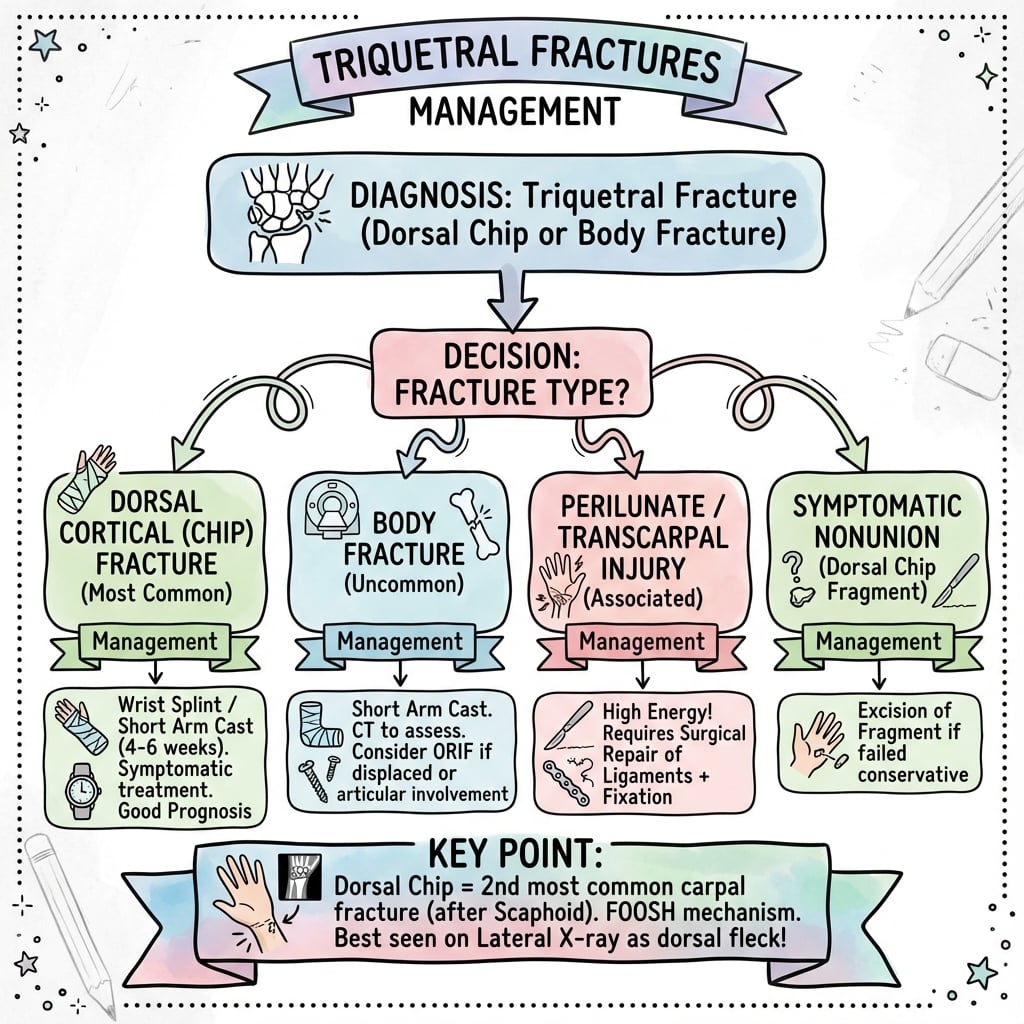
- Second most common carpal fracture after scaphoid
- Dorsal chip fractures are 93% of all triquetral fractures
- Best seen on lateral radiograph - dorsal cortex avulsion
- FOOSH with ulnar deviation is typical mechanism
- Excellent prognosis with conservative treatment for most
Clinical Pearls
- "Always check lateral view - dorsal chip easily missed on PA
- "Hamate impaction on triquetrum causes dorsal chip
- "Body fractures may indicate perilunate spectrum injury
- "Most dorsal chip fractures heal uneventfully with casting
High-Yield Triquetral Fracture Exam Points
Second Most Common
Triquetral fractures are the second most common carpal fracture (14-20%), after scaphoid fractures. The dorsal chip pattern is by far the most frequent, accounting for over 90% of cases.
Lateral View Essential
Dorsal chip fractures are often missed on PA radiographs. The lateral view is essential - look for a small osseous fragment dorsal to the triquetrum. This is a common exam presentation.
Mechanism of Injury
Two mechanisms cause dorsal chips: 1) Hamate impaction - ulnar deviation drives hamate into triquetrum, avulsing dorsal cortex; 2) Ligament avulsion - strong radiotriquetral or lunotriquetral ligament pulls off bone.
Perilunate Association
Body fractures (not chips) may indicate greater arc perilunate injury. Always assess for carpal malalignment and associated injuries when body fracture is present.
At a Glance: Triquetral Fracture Management
| Fracture Type | Frequency | Management | Key Consideration |
|---|---|---|---|
| Type I - Dorsal chip | Over 90% | Cast 4-6 weeks | Excellent prognosis, most common type |
| Type II - Body fracture | Under 10% | Cast, ORIF if displaced | Assess for perilunate injury |
| Type III - Volar avulsion | Rare | Address associated injury | Part of perilunate spectrum |
| Comminuted body | Very rare | Complex reconstruction | High energy, poor prognosis |
TRIQ - TTRIQ - Triquetral Fracture Features
| T | Type: mostly dorsal chip Over 90% are dorsal avulsion fractures |
| R | Radiograph lateral Lateral view essential - missed on PA |
| I | Impaction mechanism Hamate impacts triquetrum with ulnar deviation |
| Q | Quick healing 4-6 weeks casting, excellent prognosis |
| T | Type: mostly dorsal chip Over 90% are dorsal avulsion fractures | I | Impaction mechanism Hamate impacts triquetrum with ulnar deviation |
| R | Radiograph lateral Lateral view essential - missed on PA | Q | Quick healing 4-6 weeks casting, excellent prognosis |
Hook:TRIQ - dorsal chip fractures heal Quickly with conservative treatment
CHIP - DCHIP - Dorsal Chip Features
| C | Common fracture Second most common carpal injury |
| H | Hamate impaction Ulnar deviation drives hamate into triquetrum |
| I | Immobilize in cast Short arm cast for 4-6 weeks |
| P | Prognosis excellent Most heal without complication |
| C | Common fracture Second most common carpal injury | I | Immobilize in cast Short arm cast for 4-6 weeks |
| H | Hamate impaction Ulnar deviation drives hamate into triquetrum | P | Prognosis excellent Most heal without complication |
Hook:CHIP fractures have excellent Prognosis with simple Immobilization
BODY - BBODY - Body Fracture Red Flags
| B | Beware perilunate Body fractures may indicate greater arc injury |
| O | Overt displacement Displaced fractures need ORIF |
| D | Dedicated CT scan CT for surgical planning |
| Y | Yield to surgery Displaced body fractures require fixation |
| B | Beware perilunate Body fractures may indicate greater arc injury | D | Dedicated CT scan CT for surgical planning |
| O | Overt displacement Displaced fractures need ORIF | Y | Yield to surgery Displaced body fractures require fixation |
Hook:BODY fractures Beware - may indicate perilunate injury
LOOKLateral View Findings
| L | Lateral X-ray best AP misses dorsal chip |
| O | Over lunate Fragment sits dorsal to lunate |
| O | Often small Easy to miss if not looking |
| K | Keep checking Gilula arcs Rule out perilunate |
| L | Lateral X-ray best AP misses dorsal chip | O | Often small Easy to miss if not looking |
| O | Over lunate Fragment sits dorsal to lunate | K | Keep checking Gilula arcs Rule out perilunate |
Hook:LOOK at the lateral view - essential for dorsal chip fractures!
Overview and Epidemiology
Definition
Triquetral fractures are fractures of the triquetral (triquetrum) carpal bone, located on the ulnar side of the proximal carpal row. The most common pattern is a dorsal cortical avulsion (chip fracture), though body fractures also occur.
Epidemiology
- Incidence: Second most common carpal fracture (14-20% of all carpal fractures)
- First: Scaphoid fractures (70-80%)
- Age distribution: Young to middle-aged adults
- Gender: Male predominance
- Mechanism: Usually FOOSH with ulnar deviation
Fracture Patterns
Dorsal Chip Fractures (Over 90%)
- Small cortical avulsion from dorsal surface
- Usually under 5mm in size
- Best seen on lateral radiograph
- Excellent prognosis with conservative treatment
Body Fractures (Under 10%)
- Through substance of triquetrum
- May be associated with perilunate injuries
- Higher energy mechanism
- May require surgical treatment
Volar Avulsion (Rare)
- Usually associated with perilunate dislocation
- Part of greater arc injury pattern
- Requires assessment for carpal instability
Understanding triquetral anatomy and fracture patterns is essential for diagnosis and management.
Anatomy/Biomechanics
Osseous Anatomy
Shape and Configuration
- Pyramidal shape: Triangular when viewed from ulnar aspect
- Largest bone: Of the proximal carpal row by volume
- Dorsal surface: Site of most common fracture pattern
- Volar surface: Pisiform articulation
Articular Surfaces
- Lunate (medial): Part of intercalated segment
- Hamate (distal): Articulates with proximal hamate pole
- Pisiform (volar): Small sesamoid articulation
- TFCC (proximal): Through ulnocarpal complex
Surface Features
- Dorsal ridge: Site of ligament attachments
- Volar groove: Pisiform articulates here
- Hamate facet: Distal articular surface
Blood Supply
Vascular Pattern
- Multiple dorsal and volar nutrient vessels
- No single dominant vessel (unlike lunate)
- Lower risk of AVN than other carpals
- Reliable healing potential
Vessel Entry Points
- Dorsal surface: Primary blood supply
- Volar surface: Secondary vessels
- Non-articular surfaces: Additional supply
Biomechanics
Carpal Kinematics
- Part of proximal row "intercalated segment"
- Moves with scaphoid and lunate as functional unit
- Limited independent motion
- Ulnar border of proximal row
Load Transmission
- Transmits force from ulnar carpus
- Less load than radial side
- Pisiform modifies force transmission
- Hamate contact with ulnar deviation
Mechanism of Dorsal Chip
Two mechanisms produce dorsal chip fractures:
Hamate Impaction (Primary)
- Wrist falls into extension and ulnar deviation
- Hamate dorsal pole impacts triquetral dorsum
- Shearing force avulses dorsal cortex
Ligamentous Avulsion
- Strong radiotriquetral ligament pulls off bone
- Lunotriquetral ligament may contribute
- Traction injury rather than impaction
Both mechanisms produce similar fracture patterns.
Classification Systems
Anatomical Classification
The most practical classification based on fracture location:
Type I - Dorsal Cortical Fracture (Chip)
- Over 90% of all triquetral fractures
- Small dorsal cortical avulsion
- Usually under 5mm fragment
- Excellent prognosis
- Treatment: Cast immobilization 4-6 weeks
Type II - Body Fracture
- Through the body of triquetrum
- Less than 10% of fractures
- May indicate higher energy injury
- Assess for associated injuries
- Treatment: Cast if undisplaced, ORIF if displaced
Type III - Volar Avulsion
- Rare isolated injury
- Usually part of perilunate spectrum
- Ligamentous origin (pisotriquetral, ulnotriquetral)
- Treatment: Address associated carpal injury
Type IV - Comminuted Body
- High-energy mechanism
- Significant fragment displacement
- Poor soft tissue envelope
- Treatment: Complex reconstruction, may need external fixation
This classification guides treatment selection and prognosis.
Classification Summary
| Type | Location | Frequency | Stability |
|---|---|---|---|
| Type I | Dorsal cortex | Over 90% | Stable |
| Type II | Body | Under 10% | Variable |
| Type III | Volar cortex | Rare | Usually part of perilunate |
| Type IV | Comminuted | Very rare | Unstable |
Classification determines treatment approach and expected outcome.
Clinical Assessment
History
Mechanism of Injury
- FOOSH: Fall onto outstretched hand with ulnar deviation
- Direct blow: Rare, usually dorsum of wrist
- Sports injury: Contact sports, ball sports
- Motor vehicle accident: Dashboard injury
Key History Points
- Exact mechanism and position of wrist
- Energy of injury (height of fall, impact speed)
- Immediate symptoms and swelling pattern
- Prior wrist injuries or symptoms
- Hand dominance and occupational demands
Physical Examination
Inspection
- Swelling over ulnar wrist
- May be subtle with dorsal chip fractures
- Compare to contralateral side
- Assess for skin integrity
Palpation
- Triquetral tenderness: Over dorsal ulnar wrist
- Anatomic snuffbox: Negative (rules out scaphoid)
- DRUJ: Assess for associated injury
- Pisiform: May have concomitant tenderness
Range of Motion
- Limited by pain in acute setting
- Ulnar deviation particularly painful
- Assess forearm rotation (DRUJ involvement)
Neurovascular Assessment
- Usually preserved
- Check ulnar nerve function
- Document baseline for comparison
Special Tests
Watson Test (Scaphoid Shift)
- Should be negative
- If positive, consider additional carpal injury
Ballottement Test
- Lunotriquetral stability assessment
- Compare to contralateral side
- Positive = LT instability
Triquetral Shear Test
- Direct pressure on triquetrum
- Pain suggests triquetral pathology
- Specific for triquetral injury
ECU Subluxation Test
- Assess extensor carpi ulnaris
- May have associated injury
- Supinate and ulnar deviate wrist
Clinical examination guides imaging and treatment decisions.
Differential Diagnosis
Ulnar-sided wrist pain after a fall has a broad differential. The triquetral fracture must be distinguished from the conditions below, several of which can coexist with it.
Differential Diagnosis of Acute Ulnar-Sided Wrist Pain
| Condition | Distinguishing feature | Key investigation |
|---|---|---|
| Triquetral dorsal chip fracture | Point tenderness dorsal-ulnar; dorsal fragment on lateral film | Lateral radiograph (CT if occult) |
| Ulnar styloid fracture | Tenderness at styloid tip; often with distal radius fracture | PA radiograph |
| TFCC tear | DRUJ pain, positive fovea sign, painful forearm rotation | MRI / wrist arthroscopy |
| Lunotriquetral ligament injury | Positive ballottement test, LT interval changes | MRI, dynamic imaging |
| Pisiform fracture | Tenderness over pisiform, pain on pisotriquetral grind | Carpal tunnel / 30-degree supinated view |
| Hook of hamate fracture | Hypothenar pain, tenderness over hook, ulnar nerve symptoms | Carpal tunnel view / CT |
| Perilunate / greater arc injury | Carpal malalignment, disrupted Gilula arcs, DISI/VISI | PA and lateral radiographs, CT |
Clinical examination guides imaging and treatment decisions.
Investigations
Plain Radiographs
Standard Views
- PA view: May miss dorsal chip fractures
- Lateral view: Essential - shows dorsal fragment
- Oblique views: Additional perspective
Lateral View (Critical)
The lateral radiograph is essential for dorsal chip diagnosis:
- Small osseous fragment dorsal to carpal silhouette
- Usually located at level of triquetrum
- May be overlooked if not specifically sought
- Best identified with true lateral positioning
PA View Findings
- Body fractures may be visible
- Carpal alignment assessment
- Scapholunate and lunotriquetral intervals
- Often normal with isolated dorsal chip
Signs of Associated Injury
- Scapholunate widening (SL injury)
- LT overlap or widening
- Carpal arc disruption
- DISI or VISI pattern on lateral
CT Scanning
Indications
- Suspected body fracture not clear on X-ray
- Surgical planning for displaced fractures
- Assessment of comminution
- Evaluation for perilunate injury
Key CT Findings
- Fracture line orientation
- Fragment size and displacement
- Articular involvement
- Associated carpal injuries
MRI
Indications
- Suspected ligamentous injury
- Occult fracture not seen on X-ray/CT
- LT ligament assessment
- TFCC evaluation
Findings
- Bone marrow edema in fracture
- Ligament integrity assessment
- Associated soft tissue injury
Bone Scan
Limited Role
- Rarely needed
- May detect occult fracture
- Superseded by MRI for most indications
Investigations are summarized below.
Imaging Strategy for Triquetral Fractures
| Modality | Primary Role | Key Advantage | Limitation |
|---|---|---|---|
| Lateral X-ray | Dorsal chip diagnosis | Quick, essential view | May miss body fractures |
| PA X-ray | Body fracture, alignment | Carpal assessment | Misses dorsal chips |
| CT scan | Surgical planning | Fracture detail | Radiation, cost |
| MRI | Ligament assessment | Soft tissue detail | Cost, availability |
The lateral radiograph is the most important view for dorsal chip diagnosis.
Management Algorithm
Conservative Management
Indications
- All dorsal chip fractures (Type I)
- Undisplaced body fractures (Type II)
- No carpal instability
- Elderly or low-demand patients
Protocol for Dorsal Chip Fractures
Immobilization
- Short arm cast or splint
- Wrist in neutral position
- Duration: 4-6 weeks
- May use removable splint for compliant patients
Follow-Up
- Week 2: Clinical review, comfort check
- Week 4-6: Assess tenderness, repeat X-ray
- Week 6: If non-tender, begin mobilization
Expected Outcomes
- Excellent prognosis for dorsal chip fractures
- Union in 4-6 weeks
- Full function typically restored
- Rare persistent symptoms
Symptomatic Non-Union
- Occurs in minority of cases
- Persistent dorsal wrist pain
- May require fragment excision
- Generally straightforward procedure
Conservative management is successful for the vast majority of triquetral fractures.
Most triquetral fractures are managed conservatively with excellent results.
Surgical Technique
Fragment Excision for Symptomatic Non-Union
Indications
- Symptomatic dorsal chip non-union
- Persistent pain after 3-6 months of conservative treatment
- Confirmed by imaging as source of symptoms
Patient Positioning
- Supine with arm table
- Tourniquet on upper arm
- Wrist pronated for dorsal access
Surgical Technique
Incision
- Small longitudinal incision (2-3 cm)
- Over dorsal ulnar wrist
- Centered on palpable fragment if detectable
Exposure
- Incise extensor retinaculum between EDM and ECU
- Retract tendons appropriately
- Identify dorsal chip fragment in capsule
- Usually embedded in dorsal ligament complex
Excision
- Carefully isolate fragment
- Excise completely with curette or rongeur
- Preserve as much ligament as possible
- Debride any fibrous tissue
- Check for additional fragments
Closure
- Repair retinaculum loosely
- Standard skin closure
- Soft dressing and splint
Postoperative Care
- Splint 1-2 weeks
- Early ROM exercises
- Full activity 4-6 weeks
Fragment excision is a straightforward procedure with excellent outcomes.
Surgical intervention is rarely needed but provides reliable outcomes when indicated.
Complications
Complications of Dorsal Chip Fractures
Symptomatic Non-Union
- Most common complication
- Occurs in 5-10% of dorsal chips
- Persistent dorsal wrist pain
- Treatment: Fragment excision with good results
Extensor Tendon Irritation
- Fragment may abrade overlying tendons
- EDC or EDM most commonly affected
- Presents as tendon pain or snapping
- Treatment: Fragment excision
Dorsal Wrist Impingement
- Large fragment blocks extension
- Mechanical symptoms with wrist motion
- Treatment: Surgical excision
Complications of Body Fractures
Malunion
- Rare with appropriate treatment
- May alter carpal kinematics
- Can lead to secondary arthritis
Nonunion
- More common than with dorsal chips
- May require bone grafting
- Associated with inadequate immobilization
Post-Traumatic Arthritis
- Uncommon with isolated triquetral fractures
- More common with associated injuries
- May require salvage procedures
Lunotriquetral Instability
- Can develop after body fractures
- LT ligament may be injured at time of fracture
- Presents with ulnar wrist pain and clicking
- Treatment: LT repair or fusion
Complications of Surgical Treatment
Wound Complications
- Infection (rare)
- Dehiscence
- Scar sensitivity
Hardware Issues
- Screw prominence
- K-wire migration
- May require removal
Tendon Injury
- ECU or EDM at risk
- Usually prevented with careful technique
- Repair if identified intraoperatively
Complication Summary
| Complication | Frequency | Prevention | Management |
|---|---|---|---|
| Symptomatic non-union | 5-10% of chips | Adequate immobilization | Fragment excision |
| Tendon irritation | Rare | Complete excision | Remove fragment |
| LT instability | Rare with body Fx | Recognize at injury | Ligament repair/fusion |
| Arthritis | Rare | Anatomic reduction | Activity modification to fusion |
Complications are uncommon, and outcomes are generally excellent.
Postoperative Care
Conservative Treatment Protocol
Immobilization Phase (0-6 Weeks)
Week 0-2
- Short arm cast or thermoplastic splint
- Wrist neutral position
- Immediate finger motion
- Elevate to reduce swelling
Week 2-4
- Continue immobilization
- May switch to removable splint if compliant
- Begin gentle finger exercises if not already
Week 4-6
- Clinical review
- Assess tenderness over triquetrum
- Radiograph to confirm position
- If non-tender, may discontinue splint
Rehabilitation Phase (6-12 Weeks)
Week 6-8
- Begin active wrist ROM
- Avoid resisted activities
- Progress as tolerated
Week 8-12
- Progressive strengthening
- Return to normal activities
- Sport-specific training if applicable
Surgical Treatment Protocol
Immediate Postoperative (0-2 Weeks)
- Volar splint
- Wound care
- Finger motion
- Elevation
Early Mobility (2-6 Weeks)
- Removable splint
- Gentle wrist ROM
- Avoid loading
- Suture removal at 10-14 days
Progressive Loading (6-12 Weeks)
- Discontinue splint
- Progressive strengthening
- K-wire removal at 6 weeks if applicable
- Return to activities 8-12 weeks
Follow-Up Schedule
| Timepoint | Conservative | Surgical |
|---|---|---|
| Week 2 | Comfort check | Wound check |
| Week 6 | X-ray, assess healing | X-ray, ROM |
| Week 12 | Final if healed | Final if healed |
| As needed | Symptomatic review | Hardware concerns |
Most patients achieve full recovery with straightforward rehabilitation.
Outcomes and Prognosis
Dorsal Chip Fractures
Healing Rate
- Over 95% heal with conservative treatment
- Union typically at 4-6 weeks
- Fibrous union may be asymptomatic
Functional Outcomes
- Excellent ROM recovery (95-100% of normal)
- Full grip strength return
- Return to previous activity level
- High patient satisfaction
Symptomatic Non-Union Rate
- 5-10% develop symptoms
- Persistent dorsal wrist pain
- Easily treated with excision
- Excellent results after excision
Body Fractures
Healing Rate
- Good healing with appropriate treatment
- Union at 6-8 weeks typical
- Higher nonunion rate if inadequately treated
Functional Outcomes
- Good outcomes with anatomic reduction
- May have some residual stiffness
- Depends on associated injuries
- Return to previous activity in most
Associated Injury Impact
- Perilunate spectrum injuries have worse prognosis
- LT instability may persist
- May require additional procedures
Prognostic Factors
Favorable Factors
- Dorsal chip pattern
- Isolated injury
- Early treatment
- Compliant patient
Unfavorable Factors
- Body fracture with displacement
- Associated perilunate injury
- Delayed diagnosis
- High-energy mechanism
Return to Activity
Conservative Treatment
- Sedentary work: 1-2 weeks with splint
- Light manual: 6-8 weeks
- Heavy manual: 8-12 weeks
- Contact sports: 8-12 weeks
Surgical Treatment
- Similar timelines
- May be slightly longer for body ORIF
- Athlete return at 3-4 months
The prognosis for triquetral fractures is excellent overall.
Evidence Base
- Population registry of 6542 carpal fractures: scaphoid 60%, triquetrum 25%, hamate 5%, trapezium 4%
- Triquetrum is the second most commonly fractured carpal bone
- Mean age at injury 41 years; 69% of patients male
- Carpal fractures had only a small negative effect on hand function and EQ-5D at one year
- Series of 231 triquetral fractures with 65 followed for a mean of 47 months
- Dorsal chip caused by the chisel action of the dorso-proximal hamate against the extended, ulnar-deviated wrist
- Conservative immobilisation for 3 weeks was successful; fragment union when it occurred took 6 to 8 weeks
- No post-traumatic carpal instability and no avascular necrosis observed; all body fractures united
- Cadaveric and radiographic study disproving the avulsion-only theory of dorsal chip fractures
- Mechanism is a chisel action of the ulnar styloid on the dorsum of the triquetrum
- A forceful fall in dorsiflexion and ulnar deviation can also fracture the triquetral body
- A prolonged ulnar styloid projecting beyond the ulnar head was consistently noted
- Prospective comparison of radiography with CT as the gold standard in 61 wrist examinations
- Only 20% of triquetral fractures were detected prospectively on radiographs
- 30% of all wrist fractures were not diagnosed prospectively on plain films
- CT should be considered after a negative radiograph when clinical suspicion persists
- Retrospective series of 178 emergency carpal fractures over 6 years
- The triquetrum was the most frequently affected bone, ahead of the scaphoid in this cohort
- Almost all triquetral fractures were treated conservatively
- Young men carried the highest risk of carpal fracture and CT was usually required
The evidence supports conservative management for most triquetral fractures with excellent expected outcomes.
Viva Scenarios
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Missed Triquetral Fracture
"A 25-year-old man presents 2 weeks after a fall onto his hand. He has ongoing ulnar wrist pain. PA radiograph was reported as normal. How do you evaluate this patient?"
Triquetral Body Fracture Assessment
"A 30-year-old motorcyclist presents after a crash. X-rays show a displaced triquetral body fracture. How do you approach this injury?"
Symptomatic Triquetral Non-Union
"A patient returns 6 months after a triquetral dorsal chip fracture, still complaining of dorsal wrist pain with gripping. Radiographs confirm non-union. How do you manage this?"
MCQ Practice Points
Fracture Frequency
Q: What is the second most common carpal fracture? A: Triquetral fractures are the second most common carpal fracture (14-20%), after scaphoid fractures which account for 70-80% of all carpal fractures.
Fracture Pattern
Q: What percentage of triquetral fractures are dorsal chip fractures? A: Over 90% of triquetral fractures are dorsal chip (cortical avulsion) fractures. Body fractures account for less than 10%.
Radiographic Diagnosis
Q: Which radiographic view is most important for diagnosing triquetral dorsal chip fractures? A: The lateral radiograph is essential. Dorsal chip fractures are frequently missed on PA views but clearly visible as a small osseous fragment dorsal to the carpus on the lateral.
Mechanism of Injury
Q: What is the primary mechanism causing triquetral dorsal chip fractures? A: Hamate impaction - when the wrist falls into extension and ulnar deviation, the hamate dorsal pole impacts the triquetral dorsum, avulsing a fragment of dorsal cortex.
Treatment Approach
Q: What is the standard treatment for an isolated triquetral dorsal chip fracture? A: Conservative management with short arm cast for 4-6 weeks. Over 95% heal with immobilization, and the prognosis is excellent.
Non-Union Management
Q: How should symptomatic non-union of a triquetral dorsal chip be treated? A: Surgical fragment excision through a dorsal approach. This is a straightforward procedure with excellent outcomes in over 95% of patients.
Understanding these key concepts will help with exam success.
Guidelines, Registries & Global Practice
Global Epidemiology (Registry & Population Evidence)
There is no dedicated triquetral-fracture trial registry; the strongest evidence comes from national fracture registries and large carpal-fracture series that report relative frequency, demographics and treatment patterns.
Population & Registry Evidence on Triquetral Fractures
| Source (region) | Cohort | Key finding | Evidence |
|---|---|---|---|
| Swedish Fracture Registry (Sweden) | 6542 carpal fractures | Triquetrum 25% of carpal fractures (2nd after scaphoid 60%); mean age 41, 69% male | Level IV registry |
| Boeddrich, Germany | 178 ED carpal fractures | Triquetrum most frequent in cohort; almost all treated conservatively | Level IV |
| Höcker, Austria | 231 triquetral fractures | Dorsal chip predominates; 3-week immobilisation successful; no AVN/instability | Level IV |
| Welling, USA (CT vs XR) | 61 wrist examinations | Only 20% of triquetral fractures seen on radiographs; 30% of wrist fractures occult | Level III |
Registry and cohort data are consistent across Europe and North America: the triquetrum is the second most commonly fractured carpal bone, the dorsal cortical (chip) pattern predominates, and the population is skewed towards young adult men. Plain radiographs substantially under-detect these fractures, so persistent clinical suspicion should drive further imaging.
Guideline & Society Positions
No single national society publishes a stand-alone triquetral-fracture guideline; management is governed by general carpal-fracture and wrist-trauma principles. The table below summarises where authoritative guidance is drawn from across major bodies.
Society & Guideline Guidance (Carpal/Wrist Trauma)
| Body (region) | Position relevant to triquetral fracture | Evidence basis |
|---|---|---|
| AAOS (USA) | Carpal fractures other than scaphoid managed by general fracture principles; CT for occult or displaced injury | Expert consensus |
| BOA / BSSH (UK) | Wrist-trauma standards emphasise excluding perilunate injury and dedicated views when radiographs are normal but tenderness persists | Consensus standards |
| AO Foundation (global) | Isolated stable triquetral fractures: cast immobilisation; ORIF reserved for displaced body fractures and perilunate patterns | Expert consensus |
| EFORT / NICE (Europe, UK) | No specific triquetral guidance; cross-sectional imaging recommended where plain films are non-diagnostic and suspicion remains | Consensus / NG38 fracture principles |
Practice Variation & Australian Context
- Consistent across systems: conservative management (short-arm cast or splint, typically 3 to 6 weeks) is standard worldwide for isolated dorsal chip and undisplaced body fractures, reflecting Level IV evidence of reliable union without instability or avascular necrosis.
- Variation: immobilisation duration varies (3 weeks in the Höcker series versus the more commonly quoted 4 to 6 weeks); thresholds for CT after a normal radiograph differ by access and local protocol.
- Surgery: reserved for displaced body fractures, perilunate spectrum injuries and symptomatic dorsal chip non-union (fragment excision) in all systems.
- Australia: the fall-onto-outstretched-hand mechanism is common in sport and occupational settings; the orthopaedic community follows the same international evidence, with hand-surgery subspecialists managing perilunate and complex injuries and general orthopaedic surgeons performing fragment excision. Digital imaging and ready CT access aid detection of subtle dorsal chips, and the excellent prognosis means most patients, including those under workers compensation pathways, return to work within weeks.
Triquetral Fractures - Rapid Recall
Clinical summary
Key Statistics
- •Second most common carpal fracture (14-20%)
- •Over 90% are dorsal chip fractures
- •Dorsal chip = excellent prognosis
- •Body fracture = assess for perilunate
- •Non-union rate 5-10% (usually asymptomatic)
Imaging Pearls
- •Lateral view ESSENTIAL - chips missed on PA
- •Small osseous fragment dorsal to carpus
- •PA view: check carpal alignment, Gilula arcs
- •CT for body fracture surgical planning
Mechanism
- •FOOSH with ulnar deviation
- •Hamate impaction on triquetrum
- •OR ligament avulsion (radiotriquetral/LT)
- •Body fracture = higher energy
Treatment Algorithm
- •Dorsal chip: Cast 4-6 weeks
- •Body undisplaced: Cast 6-8 weeks
- •Body displaced: ORIF with screws/K-wires
- •Symptomatic non-union: Fragment excision
Body Fracture Red Flags
- •May indicate perilunate spectrum
- •Assess Gilula arcs
- •Check for DISI/VISI on lateral
- •CT/MRI for full evaluation
Outcomes
- •Over 95% heal with conservative treatment
- •Symptomatic non-union easily treated
- •Fragment excision has excellent results
- •Return to activity 6-12 weeks typical