Hindfoot Fusion | Deformity Correction | Salvage Procedure
INDICATION CATEGORIES
Critical Must-Knows
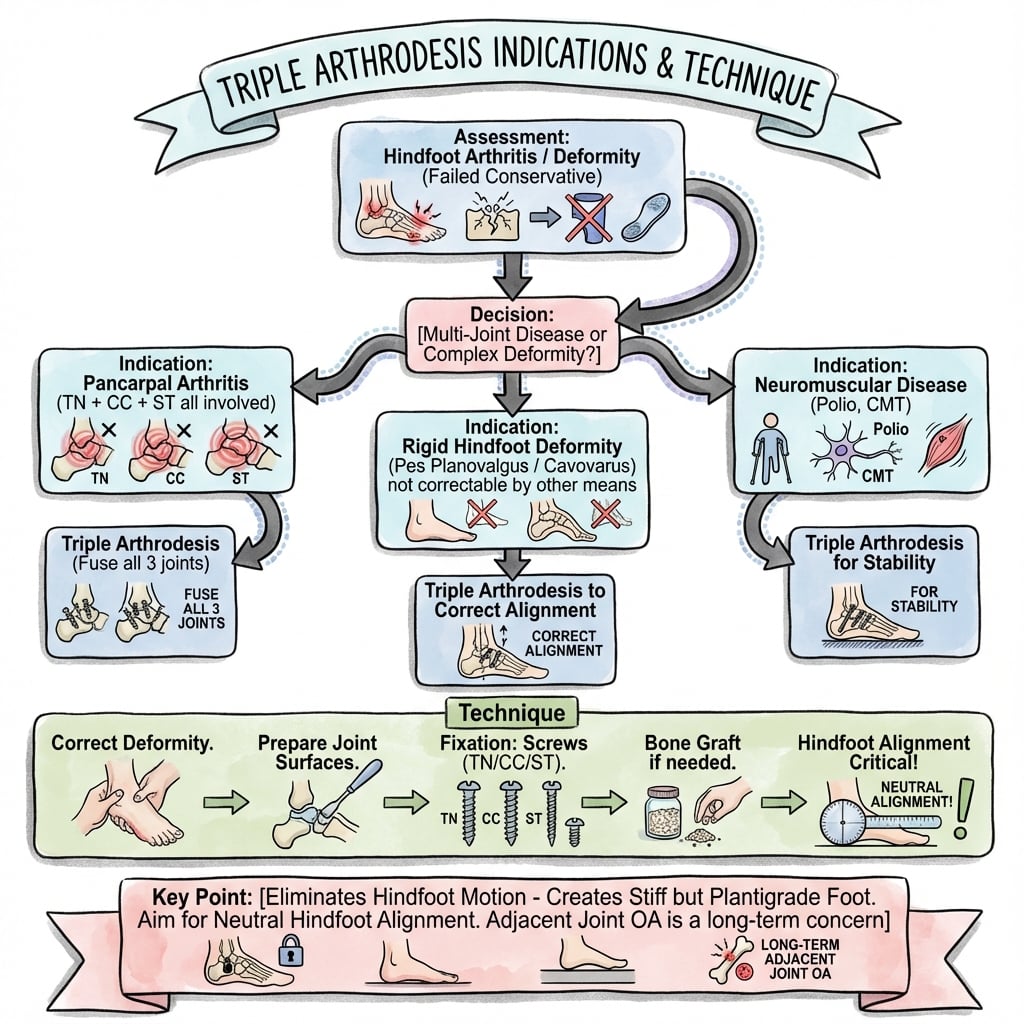
- Triple arthrodesis fuses talonavicular, subtalar, and calcaneocuboid joints - eliminates all hindfoot motion
- Primary indication: rigid hindfoot deformity with arthritis not amenable to isolated fusion
- Positioning critical: 5-7° hindfoot valgus prevents excessive lateral column loading
- Adjacent joint disease: 15-20% develop tibiotalar or midfoot arthritis within 10 years
- Contraindications: active infection, severe vascular insufficiency, tobacco use (relative)
Clinical Pearls
- "Examiners ask about optimal hindfoot position - 5-7° valgus prevents lateral overload
- "Know PTTD reconstruction vs triple arthrodesis decision-making algorithm
- "Understand why isolated subtalar fusion may be preferred in selective cases
- "Be able to discuss adjacent joint disease prevention strategies and counseling
Clinical Imaging
Imaging Gallery




Critical Triple Arthrodesis Exam Points
Joint Positioning
5-7° hindfoot valgus is critical. Varus positioning causes lateral column overload and pain. Neutral positioning may still overload lateral structures. Verify with intraoperative fluoroscopy in multiple planes.
Adjacent Joint Disease
15-20% develop tibiotalar or midfoot arthritis within 10 years. Counsel patients preoperatively. Younger, more active patients at higher risk. Consider isolated fusion when possible.
Fusion Sequence
Talonavicular joint fused first - establishes hindfoot alignment. Subtalar follows to lock position. Calcaneocuboid last to accommodate length. Order matters for deformity correction.
Nonunion Risk
10-15% overall nonunion rate with highest risk at calcaneocuboid (20-25%). Smoking cessation mandatory. Bone graft for cystic changes. Rigid fixation essential.
Quick Decision Guide: Triple Arthrodesis vs Alternatives
| Clinical Scenario | Deformity Type | Treatment Choice | Key Pearl |
|---|---|---|---|
| Stage II PTTD, flexible flatfoot | Flexible, passively correctable | Medializing calcaneal osteotomy + FDL transfer | Preserve motion - avoid fusion if possible |
| Stage III PTTD, rigid flatfoot, isolated subtalar arthritis | Rigid, subtalar arthritis only | Isolated subtalar fusion | Preserves TN and CC motion - better function |
| Post-traumatic arthritis all 3 joints, rigid valgus | Rigid, pan-hindfoot arthritis | Triple arthrodesis | Gold standard for pan-hindfoot disease |
| Severe cavovarus, CMT disease, rigid | Rigid cavovarus, neuromuscular | Triple arthrodesis + soft tissue balancing | May need Achilles lengthening, peroneus longus-to-brevis |
TRIPLJoints Involved in Triple Arthrodesis
| T | Talonavicular Fused first - establishes hindfoot alignment |
| R | Rigid fixation required Screws or plates across all 3 joints |
| I | Interosseous structures removed Cartilage and subchondral bone preparation |
| P | Position in 5-7° valgus Critical for preventing lateral overload |
| L | Lateral column (calcaneocuboid) Highest nonunion risk - consider structural graft |
| T | Talonavicular Fused first - establishes hindfoot alignment | P | Position in 5-7° valgus Critical for preventing lateral overload |
| R | Rigid fixation required Screws or plates across all 3 joints | L | Lateral column (calcaneocuboid) Highest nonunion risk - consider structural graft |
| I | Interosseous structures removed Cartilage and subchondral bone preparation |
Hook:TRIPL reminds you this is a TRIPLE fusion - remember TN first, position in valgus, watch the lateral column!
SALVAIndications for Triple Arthrodesis
| S | Subtalar + TN + CC arthritis Pan-hindfoot disease requiring fusion |
| A | Arthritic rigid deformity Post-traumatic, primary OA, inflammatory |
| L | Late-stage PTTD (Stage III/IV) Fixed flatfoot with arthritis |
| V | Varus or valgus malalignment Neuromuscular: CMT, polio, stroke |
| A | After failed coalition resection Salvage when excision unsuccessful |
| S | Subtalar + TN + CC arthritis Pan-hindfoot disease requiring fusion | V | Varus or valgus malalignment Neuromuscular: CMT, polio, stroke |
| A | Arthritic rigid deformity Post-traumatic, primary OA, inflammatory | A | After failed coalition resection Salvage when excision unsuccessful |
| L | Late-stage PTTD (Stage III/IV) Fixed flatfoot with arthritis |
Hook:SALVA = 'salvage' procedure - when other options have failed or pan-hindfoot disease exists!
NAILSComplications of Triple Arthrodesis
| N | Nonunion 10-15% overall, highest at calcaneocuboid (20-25%) |
| A | Adjacent joint disease 15-20% tibiotalar or midfoot arthritis within 10 years |
| I | Infection 2-5% superficial, 1-2% deep |
| L | Lateral overload pain From varus or neutral positioning |
| S | Sural nerve injury Lateral approach risk - 5-10% numbness |
| N | Nonunion 10-15% overall, highest at calcaneocuboid (20-25%) | L | Lateral overload pain From varus or neutral positioning |
| A | Adjacent joint disease 15-20% tibiotalar or midfoot arthritis within 10 years | S | Sural nerve injury Lateral approach risk - 5-10% numbness |
| I | Infection 2-5% superficial, 1-2% deep |
Hook:NAILS = what holds the fusion together, but also the problems - nonunion tops the list!
Overview and Epidemiology
Triple arthrodesis is a hindfoot fusion procedure that involves simultaneous fusion of the talonavicular (TN), subtalar (ST), and calcaneocuboid (CC) joints. First described by Ryerson in 1923 for poliomyelitis deformities, it remains a powerful salvage procedure for rigid hindfoot deformity with pan-hindfoot arthritis.
Historical Evolution
Originally developed for poliomyelitis and neuromuscular deformities, triple arthrodesis is now most commonly performed for post-traumatic arthritis, failed PTTD reconstruction, and rigid flatfoot/cavovarus deformity. Modern techniques emphasize preservation of hindfoot height and optimal alignment to reduce adjacent joint stress.
Common Indications
- Post-traumatic arthritis: Calcaneal fracture sequelae
- End-stage PTTD: Stage III/IV rigid flatfoot
- Neuromuscular deformity: CMT, polio, stroke
- Inflammatory arthritis: RA, seronegative
- Failed coalition resection: Salvage procedure
- Charcot arthropathy: Neuropathic hindfoot
Patient Demographics
- Age: Typically 40-70 years
- Gender: Slight female predominance (PTTD-related)
- Risk factors: Diabetes, smoking, obesity
- Expectations: Pain relief over motion restoration
- Activity level: Generally lower demand patients
- Alternatives: Isolated fusions when possible
Pathophysiology and Mechanisms
Understanding the biomechanics of hindfoot motion is critical to appreciating the functional impact of triple arthrodesis and the development of adjacent joint disease.
Hindfoot Motion Loss
Triple arthrodesis eliminates essentially all hindfoot inversion/eversion (50-60° normally). This forces compensatory motion through the tibiotalar joint and midfoot, increasing stress by 200-300%. Patients lose adaptability to uneven terrain and have altered gait mechanics.
Joint Contributions to Hindfoot Motion
| Joint | Normal Motion | Function | Impact of Fusion |
|---|---|---|---|
| Subtalar | 40-50° inversion/eversion | Primary hindfoot motion, shock absorption | Largest motion loss - transfers stress to ankle |
| Talonavicular | 10-15° rotation, pronation/supination | Couples with subtalar, medial column stability | Loss affects midfoot motion, arch mechanics |
| Calcaneocuboid | 5-10° gliding, rotation | Lateral column length accommodation | Least motion lost but highest nonunion risk |
Neurovascular Structures
- Dorsalis pedis: Crosses talonavicular joint dorsomedially
- Deep peroneal nerve: Runs with dorsalis pedis - protect during exposure
- Sural nerve: Lateral approach - 5-10% injury rate
- Posterior tibial artery: Medial, usually safe from surgical approach
- Peroneal tendons: Lateral retinaculum must be preserved
Biomechanical Consequences
- 200-300% increased tibiotalar stress: Leads to ankle arthritis
- Midfoot compensatory motion: Increased Chopart and Lisfranc stress
- Altered gait: Reduced pushoff, decreased stride length
- Uneven terrain difficulty: Loss of hindfoot adaptability
- Leg length: May shorten 5-10mm with deformity correction
Classification and Patient Selection
Primary Indications
| Category | Etiology | Key Features | Surgical Considerations |
|---|---|---|---|
| Post-traumatic arthritis | Calcaneal fracture sequelae, talar fracture, Lisfranc injury | Rigid deformity, bone loss, malunion | May require bone graft, deformity correction |
| End-stage PTTD | Stage III/IV posterior tibial tendon dysfunction | Fixed flatfoot, TN/ST arthritis, talar head uncovering | Restore arch height, consider tibiotalar arthritis risk |
| Neuromuscular deformity | CMT, polio, stroke, cerebral palsy | Progressive cavovarus or valgus, muscle imbalance | Requires soft tissue balancing (Achilles, peroneal transfer) |
| Inflammatory arthritis | Rheumatoid, seronegative spondyloarthropathy | Multi-joint involvement, forefoot also affected | Consider pan-foot reconstruction, optimize medical therapy |
Isolated Fusion vs Triple Arthrodesis
Consider isolated subtalar or talonavicular fusion when disease is limited to one joint and deformity is correctable. Triple arthrodesis should be reserved for pan-hindfoot disease or when isolated fusion is insufficient to correct rigid deformity. This preserves more motion and reduces adjacent joint stress.
Clinical Assessment
History
- Pain location: Medial arch, lateral column, sinus tarsi
- Onset: Acute trauma vs chronic progressive
- Prior treatments: Orthotics, bracing, injections, previous surgery
- Functional loss: Distance walking, uneven terrain, stairs
- Neuromuscular symptoms: Weakness, imbalance, progression
- Medical comorbidities: Diabetes, vascular disease, smoking
- Expectations: Pain relief vs activity level restoration
Physical Examination
- Alignment: Varus, valgus, or neutral hindfoot position
- Flexibility: Passive correction with hindfoot inversion/eversion
- Tibialis posterior: Strength, single-limb heel rise ability
- Peroneal strength: Varus deformity may have weak evertors
- Ankle range: Dorsiflexion, plantarflexion - may compensate
- Neurovascular: Pulses, sensation, ABI if concerns
- Special tests: Hindfoot flexibility (Jack test), Coleman block
Assess Deformity Flexibility
Determine if deformity is flexible or fixed - this guides surgical planning. Use Coleman block test for cavovarus: if hindfoot corrects to neutral with forefoot blocked, consider forefoot-driven deformity requiring first ray osteotomy in addition to triple arthrodesis.
Clinical Patterns and Surgical Implications
| Deformity Pattern | Clinical Findings | Surgical Plan |
|---|---|---|
| Rigid flatfoot (PTTD Stage III) | Fixed valgus, arch collapse, forefoot abduction, TN pain | Triple arthrodesis to restore arch, neutral hindfoot alignment |
| Rigid cavovarus (CMT) | Fixed inversion, high arch, claw toes, lateral foot pain | Triple arthrodesis + soft tissue (Achilles, peroneus longus-to-brevis) |
| Post-traumatic arthritis | Stiffness, bone block, malunion, variable alignment | Triple arthrodesis, may need bone graft or osteotomy |
Investigations
Imaging Protocol
Views: AP, lateral, mortise foot; AP, lateral ankle
Key measurements:
- Lateral talo-first metatarsal angle (normal 0-10°)
- Calcaneal pitch (normal 20-30°)
- Talonavicular coverage angle
- Tibiotalar joint space and arthritis
Assess: Alignment, arthritis severity, bone quality, prior hardware
Indications: Complex deformity, malunion, bone defects, surgical planning
Utility:
- Precise joint arthritis assessment
- Bone loss quantification
- Hardware placement planning
- Subtalar coalition or coalition resection failure evaluation
Indications: Soft tissue pathology (PTTD, spring ligament), osteonecrosis assessment
Not routine: Bony detail better on CT; clinical exam usually sufficient for soft tissue
ABI (Ankle-Brachial Index): Mandatory if diabetes, smoking, age over 60, or pulse abnormalities
Threshold: ABI less than 0.7 requires vascular consultation; less than 0.5 is absolute contraindication
Radiographic Arthritis Grading
- Grade 0: Normal joint space
- Grade 1: Joint space narrowing only
- Grade 2: Narrowing + subchondral sclerosis
- Grade 3: Grade 2 + osteophytes
- Grade 4: Severe narrowing, cysts, bone-on-bone
Surgical indication: Grade 3-4 with rigid deformity
Laboratory Studies
- CBC, ESR, CRP: Baseline, infection screening
- HbA1c: Diabetes control (target under 7.5%)
- Vitamin D: Optimize fusion (target over 30 ng/mL)
- Nutritional panel: Albumin, prealbumin if malnourished
- Smoking status: Cotinine if patient reports cessation
Nonoperative Management
Triple arthrodesis is a salvage procedure reserved for failed conservative management and progressive rigid deformity with disabling pain.
Nonoperative Treatment Algorithm
Stepwise Conservative Management
- Reduce impact activities: Avoid running, jumping, prolonged standing
- Assistive devices: Walking aids for distance ambulation
- Workplace modifications: Seated work, reduced walking requirements
- Realistic expectations: Accept activity limitations vs surgical fusion
- Custom AFO (ankle-foot orthosis): Arizona brace, UCBL (rigid flatfoot)
- CROW boot: Charcot restraint orthotic walker for neuropathic feet
- Custom insoles: Arch support, lateral posting, cushioning
- Rocker-bottom shoes: Reduce forefoot pressures, aid propulsion
- NSAIDs: Short courses for flare-ups
- Corticosteroid injections: Temporary relief (3-6 months), diagnostic
- Physical therapy: Stretching, strengthening, gait training
- Weight loss: Reduce hindfoot loading in obese patients
When Conservative Fails
Indications for surgery: Failure of 3-6 months of appropriate conservative management (orthoses, activity modification, injections) with persistent disabling pain and functional limitation. Patient must accept loss of hindfoot motion and adjacent joint disease risk.
Management Algorithm
Treatment Algorithm for Hindfoot Deformity with Arthritis
Systematic Decision-Making
Passive correction test: Attempt to manually correct deformity
- Flexible deformity: Corrects to neutral passively → consider joint-preserving procedures (osteotomy, tendon transfer)
- Rigid deformity: Does not correct → fusion required
Tests: Coleman block test (cavovarus), hindfoot inversion/eversion stress (flatfoot)
Weight-bearing radiographs + CT if needed
- Isolated joint arthritis: Single joint (TN or ST) → consider isolated fusion
- Two-joint arthritis: TN + ST → consider double arthrodesis
- Pan-hindfoot arthritis: All three joints (TN, ST, CC) → triple arthrodesis indicated
Key: Minimize number of joints fused to reduce adjacent joint stress
All patients require failed conservative management before fusion
- Custom AFO or UCBL orthosis (rigid hindfoot support)
- Activity modification (avoid impact, prolonged standing)
- NSAIDs, corticosteroid injections (diagnostic + therapeutic)
- Physical therapy (stretching, strengthening, gait training)
Proceed to surgery: If persistent disabling pain after adequate conservative trial
Mandatory optimization:
- Smoking cessation: 6 weeks minimum (verify with cotinine)
- Diabetes control: HbA1c under 7.5%
- Vascular assessment: ABI over 0.7 (consult vascular if under 0.7)
- Nutrition: Albumin over 3.5, vitamin D over 30 ng/mL
- Weight loss: BMI reduction if obese (reduces wound complications)
Choose appropriate fusion:
- Isolated subtalar: ST arthritis only, correctable deformity
- Talonavicular: TN arthritis, flexible ST joint
- Double arthrodesis: TN + ST disease, sparing CC
- Triple arthrodesis: Pan-hindfoot arthritis, rigid deformity requiring all three joints fused
Counsel: Loss of hindfoot motion, 6 weeks non-weightbearing, 10-15% nonunion, 15-20% adjacent joint disease
Conservative Trial Documentation
Document adequate conservative trial before proceeding with triple arthrodesis. This includes 3-6 months of appropriate orthotic management (AFO or UCBL), activity modification, and medical management. Fusion without conservative trial may not meet insurance requirements and medicolegal standards.
Surgical Technique
Patient Positioning and Preparation
Operating Room Setup
Supine on radiolucent table (or lateral for isolated lateral approach).
- Ipsilateral hip: Bump under hip to internally rotate leg slightly
- Contralateral leg: Padded, leg holder or frog-leg position
- Thigh tourniquet: High thigh, padded, typically 250-300 mmHg
- Bony prominences: Sacrum, contralateral heel, elbows
- Nerve protection: Ulnar nerves padded, peroneal nerve at fibular head (contralateral)
- Tourniquet time: Plan for less than 90 minutes, deflate for closure
- Foot free-draped: Allow manipulation and positioning
- Proximal to mid-calf: Adequate exposure for hardware, bone graft harvest
- C-arm access: Confirm AP, lateral, and oblique foot views possible
- Sterile tourniquet: If planning prolonged case
Consent Points
- Nonunion: 10-15% overall, up to 25% calcaneocuboid
- Adjacent joint arthritis: 15-20% within 10 years
- Infection: 2-5% superficial, 1-2% deep
- Nerve injury: 5-10% sural nerve numbness (lateral approach)
- Malposition: Requiring revision surgery (2-5%)
- DVT/PE: Standard orthopedic risk
Equipment Checklist
- Implants: Multiple 6.5mm or 7.0mm cannulated screws, consider plates for CC
- Power tools: Oscillating saw, burr, drill
- Reduction aids: Laminar spreaders, bone clamps, K-wires
- Bone graft: Local (resected bone) + consider iliac crest or allograft
- Fluoroscopy: C-arm with radiolucent table
Complications
| Complication | Incidence | Risk Factors | Prevention/Management |
|---|---|---|---|
| Nonunion | 10-15% overall, 20-25% calcaneocuboid | Smoking, diabetes, malnutrition, poor fixation | Smoking cessation, bone graft, rigid fixation. Revision with bone graft + new fixation. |
| Adjacent joint arthritis | 15-20% tibiotalar or midfoot within 10 years | Young, active patients; increased joint stress | Counsel preoperatively; consider isolated fusion if possible. May require ankle fusion. |
| Infection (superficial) | 2-5% | Diabetes, smoking, obesity, poor wound care | Optimize comorbidities, wound care. Oral antibiotics, local wound care usually sufficient. |
| Deep infection | 1-2% | Diabetes, vascular disease, hardware | IV antibiotics, surgical debridement ± hardware removal after fusion healed. |
| Sural nerve injury | 5-10% numbness, 1-2% painful neuroma | Lateral approach, excessive retraction | Careful dissection, gentle retraction. Neuroma excision + nerve burial if painful. |
| Malposition (varus/valgus) | 2-5% requiring revision | Inadequate intraoperative assessment | Verify alignment fluoroscopically before final fixation. Revision osteotomy if symptomatic. |
| Lateral column overload | 10-15% if hindfoot in neutral or varus | Neutral or varus positioning | Position hindfoot in 5-7° valgus. Lateral column pain may require salvage procedures. |
Nonunion Management
Nonunion (10-15%) is the most common major complication. Diagnosed by persistent pain, lack of bridging bone on CT at 4-6 months. Management: If asymptomatic, observe. If symptomatic, revision fusion with bone graft (iliac crest or BMP) and new fixation - consider plate augmentation for calcaneocuboid nonunion.
Early Complications (0-6 weeks)
- Wound dehiscence: 3-5%, higher with diabetes, smoking
- Hematoma: 2-3%, usually self-limiting
- DVT/PE: Standard orthopedic risk (0.5-1%)
- Compartment syndrome: Rare (less than 1%), high index of suspicion
- Hardware prominence: 5-10%, may require removal after fusion
Late Complications (over 6 months)
- Nonunion: 10-15%, highest at CC joint
- Adjacent joint arthritis: 15-20% tibiotalar or midfoot
- Persistent pain: 20-30%, often lateral column overload
- Stress fracture: 5th metatarsal, navicular (compensatory stress)
- Hardware failure: Screw breakage (2-3%), usually after fusion solid
Postoperative Care and Rehabilitation
Immediate Postoperative Period
- Strict elevation: Foot above heart level, minimize dependency
- Ice therapy: 20 minutes on/off while awake
- Non-weightbearing: Crutches or walker, no foot contact with floor
- DVT prophylaxis: Aspirin 325mg daily or LMWH per protocol
- Pain management: Multimodal analgesia, opioid weaning
- Wound check: Remove sutures/staples at 10-14 days if wounds healed
- Cast change: Replace splint with well-molded short leg cast, non-weightbearing
- X-rays: AP and lateral foot to assess alignment and hardware position
- Continue: Strict non-weightbearing for 6 weeks total
- Clinical assessment: Pain, swelling, wound healing
- X-rays: AP, lateral, mortise to assess early fusion
- Weightbearing: If early fusion signs, transition to weightbearing as tolerated in CAM boot
- If no fusion: Continue non-weightbearing cast for additional 2-4 weeks
Strict Non-Weightbearing for 6 Weeks
Non-weightbearing for the first 6 weeks is critical to prevent nonunion and hardware failure. Patients must use crutches or walker with zero foot contact. Early weightbearing increases nonunion risk from 10-15% to 20-30%.
Outcomes and Prognosis
Functional Outcomes by Indication
| Indication | Pain Relief | Satisfaction | Functional Outcome | Notes |
|---|---|---|---|---|
| Post-traumatic arthritis | Good (80-85%) | Moderate (70%) | Moderate - limited by adjacent joint stress | Younger patients, higher adjacent joint disease risk |
| End-stage PTTD | Excellent (85-90%) | Good (75%) | Good for pain relief, limited mobility | Older, lower-demand patients generally satisfied |
| Neuromuscular deformity | Good (75-80%) | Variable (60-70%) | Limited by underlying disease progression | May require revision for recurrent deformity |
| Inflammatory arthritis | Good (80%) | Good (70-75%) | Limited by systemic disease | Often pan-foot disease requiring additional procedures |
Predictors of Poor Outcome
Risk factors for poor functional outcome and dissatisfaction:
- Young age (under 40): Higher activity demands, longer time for adjacent joint disease
- Varus or neutral positioning: Lateral column overload pain
- Tobacco use: Higher nonunion, revision, and persistent pain rates
- Workers' compensation: Lower satisfaction in some studies (confounded by litigation)
- Pre-existing adjacent joint arthritis: Progression to pantalar fusion (20-30%)
Long-term Outcomes (over 5 years)
- Fusion maintenance: 85-90% remain fused long-term
- Pain relief: 75-80% report significant pain improvement
- Walking distance: Improved in 70%, limited by adjacent joint pain in 20%
- Satisfaction: 70-75% would undergo surgery again
- Revision rate: 10-15% for nonunion, malposition, or adjacent joint disease
Adjacent Joint Surveillance
- Tibiotalar arthritis: 10-15% within 10 years, higher in young/active
- Midfoot arthritis: 5-10% within 10 years (Lisfranc, naviculocuneiform)
- Monitoring: Annual X-rays for first 3 years, then as clinically indicated
- Symptoms: New onset ankle or midfoot pain, stiffness, swelling
- Treatment: Conservative first (orthotics, activity modification); ankle fusion if severe
Controversies and Areas of Uncertainty
Double vs Triple Arthrodesis
Whether to spare the calcaneocuboid joint is the central modern debate. The Fadle prospective trial found medial double arthrodesis equals triple for union, correction and function when the CC joint is uninvolved, with shorter surgery. Counterpoint: long-term adjacent-joint and lateral-column data are limited, and CC arthritis can be under-appreciated preoperatively.
Optimal Hindfoot Position
5-7 degrees valgus is widely taught to avoid lateral overload, but the precise target is not evidence-defined and likely varies with forefoot posture and limb alignment. What is robust (Pell/Myerson) is that accurate alignment - not a single magic number - drives satisfaction.
Biologics and Bone Graft
Routine use of BMP, autograft or bone-graft substitutes to lower nonunion is not supported by high-level evidence; benefit is inferred mainly in high-risk joints (calcaneocuboid) and high-risk patients (smokers, diabetics, revision). Cost and off-label status temper enthusiasm.
Approach & Weightbearing
Single-incision/sinus-tarsi vs two-incision exposure, and the safe timing of weightbearing, remain practice-dependent rather than guideline-defined. Earlier protected weightbearing is attractive but must be balanced against nonunion risk, particularly in tobacco users and diabetics.
Evidence Base and Key Trials
Talonavicular vs Triple Arthrodesis: Peak Pressure in Adjacent Joints
- Dynamic loading model in 8 cadaver specimens with intra-articular pressure sensors
- Ankle joint peak pressure higher after triple arthrodesis (5.7 MPa) than talonavicular arthrodesis (5.2 MPa)
- Naviculocuneiform joint peak pressure also higher after triple than after isolated talonavicular fusion
- More even, lower pressure distribution after selective (talonavicular) fusion
Triple Arthrodesis: 25- and 44-Year Average Follow-up of the Same Patients
- 57 patients (67 feet), mostly neuromuscular (poliomyelitis 55%, CMT 9%), reviewed at mean 25 and 44 years
- By the second (44-year) follow-up ALL ankles showed degenerative change; midfoot (naviculocuneiform, tarsometatarsal) arthritis also progressed
- Pseudarthrosis in 13 feet (about 19%); residual deformity in 78% but non-progressive
- Despite progressive arthritis, 54 of 57 patients (95%) remained satisfied with the operation
Double vs Triple Arthrodesis for Stage III Adult-Acquired Flatfoot (Prospective RCT)
- Prospective comparative study, 23 patients (13 double, 10 triple), stage III PTTD, 1-year follow-up
- All feet in both groups united by 4 months; no difference in time to union (3.4 vs 3.3 months)
- No significant difference in AOFAS hindfoot score improvement or radiographic correction (calcaneal pitch, Meary angle)
- Operative time significantly shorter for double arthrodesis (56 vs 92 min, p less than 0.001)
Tobacco Use and Complications After Ankle and Hindfoot Arthrodesis
- National database cohort: 1948 smokers and 131 smokeless-tobacco users undergoing ankle/hindfoot arthrodesis, matched to controls
- At 2 years, smokeless-tobacco users had higher nonunion (OR 2.35, 95% CI 1.31-4.20) and infection (OR 6.08) vs tobacco-naive controls
- Tobacco use raised early wound disruption/dehiscence (OR 3.00) and hardware removal (OR 5.01)
- Authors recommend screening for ALL tobacco forms and cessation before elective fusion
Clinical Outcome After Primary Triple Arthrodesis
- 111 patients (132 feet), rigid screw fixation with realignment (no wedge resection), mean 5.7-year follow-up
- 101 of 111 patients (91%) would have the operation again, independent of preoperative diagnosis
- Patient satisfaction significantly associated with postoperative ALIGNMENT (p = 0.001), not with presence of ankle arthritis
- Radiographic ankle arthritis progressed significantly, yet did not drive dissatisfaction; only 3 nonunions and 11 complications overall
Triple Arthrodesis in Older Adults: Long-term Follow-up
- 17 patients (18 feet), mean age 66, predominantly posterior tibial tendon rupture and rheumatoid disease, mean 42-month follow-up
- 3 nonunions (one talonavicular, two calcaneocuboid) - confirming the calcaneocuboid as the highest-risk joint
- 6 patients (7 feet) developed progressive ankle degeneration; 7 developed midfoot degenerative change
- 14 of 17 patients satisfied; all had less pain, though 11 retained some discomfort
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Indication and Decision-Making (2-3 minutes)
"A 58-year-old woman with longstanding posterior tibial tendon dysfunction presents with worsening medial foot pain and inability to walk more than 100 meters. She has tried custom orthotics and bracing for 12 months without relief. Examination shows fixed flatfoot deformity with hindfoot valgus that does not correct passively. Weight-bearing radiographs demonstrate talonavicular subluxation with joint space loss, subtalar arthritis, and some calcaneocuboid narrowing. She asks about surgical options. What is your assessment and management?"
Scenario 2: Surgical Technique Deep Dive (3-4 minutes)
"You have decided to proceed with triple arthrodesis for a patient with post-traumatic pan-hindfoot arthritis. Walk me through your surgical technique, including approach, joint preparation sequence, and fixation strategy."
Scenario 3: Nonunion Complication Management (2-3 minutes)
"A 52-year-old diabetic man underwent triple arthrodesis 8 months ago. He has persistent lateral foot pain despite following non-weightbearing protocol and progressive weightbearing as instructed. Clinical exam shows tenderness over the calcaneocuboid joint with some motion. CT scan shows solid fusion of talonavicular and subtalar joints but nonunion of calcaneocuboid with sclerotic bone ends and a 3mm gap. How do you manage this patient?"
MCQ Practice Points
Anatomy Question
Q: Which joint in a triple arthrodesis has the highest risk of nonunion and why?
A: The calcaneocuboid joint has the highest nonunion risk (20-25% vs 10-15% overall) due to its smaller surface area, poor vascularity, and high compression forces across the lateral column during weightbearing. Additional risk factors include smoking, diabetes, and inadequate fixation. Strategies to reduce CC nonunion include structural bone graft and plate fixation (vs screws alone) in high-risk patients.
Positioning Question
Q: What is the optimal hindfoot position during triple arthrodesis and what happens if positioned incorrectly?
A: 5-7 degrees hindfoot valgus is optimal. Positioning in neutral or varus causes lateral column overload pain in 60% of patients (vs 15% with valgus), leading to peroneal tendonitis, sural nerve irritation, and 5th metatarsal stress fractures. Valgus positioning distributes load more evenly across hindfoot and reduces compensatory lateral column stress. Verify intraoperatively with fluoroscopy (mortise view) and clinical assessment (heel bisects Achilles).
Complication Question
Q: What is the incidence and natural history of adjacent joint arthritis after triple arthrodesis?
A: 15-20% of patients develop tibiotalar or midfoot arthritis within 10 years after triple arthrodesis, increasing to 50-65% by 20-30 years. This occurs because eliminating hindfoot motion increases tibiotalar joint stress by 200-300% and midfoot stress by 150-200% during gait. Risk factors include younger age, higher activity level, and neutral/varus hindfoot positioning. Counsel patients preoperatively about this long-term risk and need for surveillance.
Indication Question
Q: How do you distinguish between a patient who needs isolated subtalar fusion vs triple arthrodesis?
A: Isolated subtalar fusion is indicated for arthritis limited to the subtalar joint with preserved talonavicular and calcaneocuboid joints, and correctable deformity. Triple arthrodesis is indicated for pan-hindfoot arthritis involving all three joints (TN, ST, CC) or when severe rigid deformity cannot be corrected by isolated fusion. Advantages of isolated ST fusion: preserves TN and CC motion (better function), reduces adjacent joint stress (10% vs 30% adjacent arthritis at 10 years), and lower nonunion risk (8% vs 15%). Always consider least extensive fusion that achieves goals.
Surgical Technique Question
Q: In what order should the three joints be fused during triple arthrodesis and why does sequence matter?
A: Talonavicular first, subtalar second, calcaneocuboid third. TN fusion establishes overall hindfoot alignment in sagittal and transverse planes (arch height, forefoot abduction/adduction). Subtalar fusion locks this position and sets hindfoot varus/valgus. Calcaneocuboid adjusts lateral column length to accommodate medial column position. Incorrect sequence makes deformity correction difficult or impossible - if you fuse ST first in wrong position, cannot correct via TN later.
Evidence Question
Q: What is the effect of smoking on triple arthrodesis outcomes?
A: Tobacco use substantially increases nonunion, infection and wound complications after ankle/hindfoot arthrodesis. In a matched national cohort (Winter et al, FAI 2024), tobacco users had higher early wound dehiscence (OR 3.0) and hardware removal (OR 5.0), and smokeless-tobacco users had higher 2-year nonunion (OR 2.35) and infection (OR 6.0) than tobacco-naive controls. Smoking causes microvascular compromise and impaired bone healing. Management: screen for all tobacco forms (not just cigarettes), mandate documented cessation preoperatively (cotinine if needed), and consider bone graft augmentation and extended non-weightbearing in users.
Guidelines, Registries & Global Practice
Global Epidemiology
- Indication shift: Historically poliomyelitis/neuromuscular (still dominant in polio-endemic and limited-resource regions); now mostly post-traumatic arthritis and end-stage flatfoot in high-income settings
- Age: Typically 40-70 years; neuromuscular cases present younger
- Sex: Slight female predominance where adult-acquired flatfoot (PTTD) drives caseload
- Risk load: Diabetes, smoking and peripheral vascular disease are the dominant modifiable drivers of nonunion and wound failure worldwide
- Terminology: Adult-acquired flatfoot is increasingly termed progressive collapsing foot deformity (PCFD)
Registry & Evidence Signals
- Arthrodesis registries are sparse: National registries (AOANJRR, NJR, AJRR) focus on arthroplasty, so hindfoot-fusion outcomes rest on case series and a small number of comparative trials
- Best comparative data: Pell/Myerson (primary triple outcomes) and the Fadle prospective double-vs-triple trial
- Consistent signal: Calcaneocuboid is the highest-risk joint for nonunion across series
- Trend: Where the CC joint is uninvolved, medial double arthrodesis is increasingly preferred to spare it
Side-by-Side Guideline & Society Positions (Perioperative Optimisation)
| Body / Region | Smoking | Glycaemic Control | Thromboprophylaxis |
|---|---|---|---|
| AAOS / ACFAS (US) | Cessation strongly advised before elective fusion; counsel on nonunion risk | Optimise HbA1c (commonly under 7.5-8%) before elective surgery | Risk-stratified chemoprophylaxis; routine prophylaxis not mandated for isolated foot/ankle surgery |
| BOA / BOFAS / NICE (UK) | Smoking cessation support offered preoperatively | Perioperative diabetes pathway; defer elective surgery if poorly controlled | NICE NG89: individualised VTE assessment; mechanical +/- pharmacological prophylaxis |
| AO Foundation / EFORT (Europe) | Cessation emphasised for bone healing; biology-first principles | Optimise metabolic status; address vitamin D and nutrition | Follow national VTE guidance; balance bleeding vs thrombosis risk |
High-Resource Practice
- Rigid screw +/- plate fixation, intraoperative fluoroscopy, CT to confirm union when in doubt
- Access to structural allograft, biologics and orthotic/AFO services
- Multidisciplinary diabetes, vascular and smoking-cessation pathways before elective fusion
Limited-Resource Practice
- Neuromuscular (post-polio) deformity remains a major indication; younger patients
- Fixation may rely on staples/K-wires and longer cast immobilisation where implants are scarce
- Conservative bracing prioritised; surgery reserved for disabling rigid deformity with limited follow-up imaging
Documentation & Consent (Globally Applicable)
Consent and records should capture:
- Risks discussed: nonunion (10-15% overall, up to 20-25% calcaneocuboid), adjacent ankle/midfoot arthritis (15-20% within 10 years, near-universal at very long term), permanent loss of hindfoot motion, infection, nerve injury
- Alternatives offered: isolated subtalar or talonavicular fusion, medial double arthrodesis, continued conservative management
- Modifiable risk optimisation: documented tobacco cessation, glycaemic control, vascular (ABI) assessment, nutrition/vitamin D
- Intraoperative alignment: fluoroscopic confirmation of 5-7 degrees hindfoot valgus before final fixation (alignment is the strongest driver of satisfaction)
- Surveillance: early CT if pain persists with equivocal radiographs; periodic review for adjacent-joint disease
TRIPLE ARTHRODESIS
Clinical summary
Key Anatomy and Biomechanics
- •Three joints fused: talonavicular, subtalar, calcaneocuboid - eliminates all hindfoot motion
- •Subtalar joint provides 40-50° inversion/eversion - largest motion loss
- •Triple arthrodesis increases tibiotalar stress 200-300% - causes adjacent joint disease
- •Sural nerve at risk with lateral approach - 5-10% numbness, protect during dissection
- •Calcaneocuboid has poorest vascularity - highest nonunion risk (20-25%)
Indications and Classification
- •Primary indication: rigid hindfoot deformity with pan-hindfoot arthritis
- •Post-traumatic arthritis most common (calcaneal fracture sequelae)
- •End-stage PTTD (Stage III/IV) with fixed flatfoot and arthritis
- •Neuromuscular: CMT, polio, stroke - progressive cavovarus or valgus
- •Contraindications: active infection, severe vascular disease (ABI under 0.5), active smoking (relative)
Surgical Algorithm
- •Two-incision approach: medial for TN, lateral (sinus tarsi) for ST and CC
- •Joint sequence: TN first (establishes alignment), ST second (locks position), CC third (length)
- •Position hindfoot in 5-7° valgus - prevent lateral overload (verify fluoroscopically)
- •Fixation: 2 screws TN (rotational control), 1-2 screws ST, 1-2 screws or plate CC
- •Postoperative: strict non-weightbearing 6 weeks, progressive WB in boot weeks 6-12
Surgical Pearls
- •TN fusion first - establishes sagittal/transverse alignment; wrong sequence prevents correction
- •5-7° valgus critical - neutral/varus causes 60% lateral pain vs 15% with valgus
- •Protect sural nerve on lateral approach - runs posteroinferior with short saphenous vein
- •CC needs rigid fixation ± bone graft - highest nonunion risk especially smokers/diabetics
- •Verify alignment before final fixation - mortise fluoroscopy and clinical heel bisection
Complications and Management
- •Nonunion 10-15% overall, 20-25% calcaneocuboid - diagnose with CT, revise if symptomatic
- •Adjacent joint arthritis 15-20% within 10 years - counsel preoperatively, surveillance X-rays
- •Lateral overload from varus/neutral positioning - requires salvage osteotomy or fusion
- •Smoking doubles nonunion (26% vs 11%) - mandatory 6-week cessation, consider bone graft
- •Infection 2-5% superficial, 1-2% deep - optimize diabetes/vascular status preoperatively
Key Evidence and Outcomes
- •Fusion rate 85-90% at 1 year with modern rigid fixation
- •Patient satisfaction 70-75% - good pain relief but limited function
- •Saltzman 25/44-yr follow-up: essentially all ankles develop arthritis long-term, yet 95% satisfaction
- •Pell/Myerson: satisfaction tracks postoperative ALIGNMENT, not adjacent arthritis - position matters most
- •Fadle RCT: when CC joint is spared, double arthrodesis equals triple for union and correction
- •Tobacco (smoked or smokeless) raises nonunion, infection and wound complications - cessation critical