First MTP Plantar Plate Injury | Hyperextension Mechanism | Athletes | Sesamoid Complex
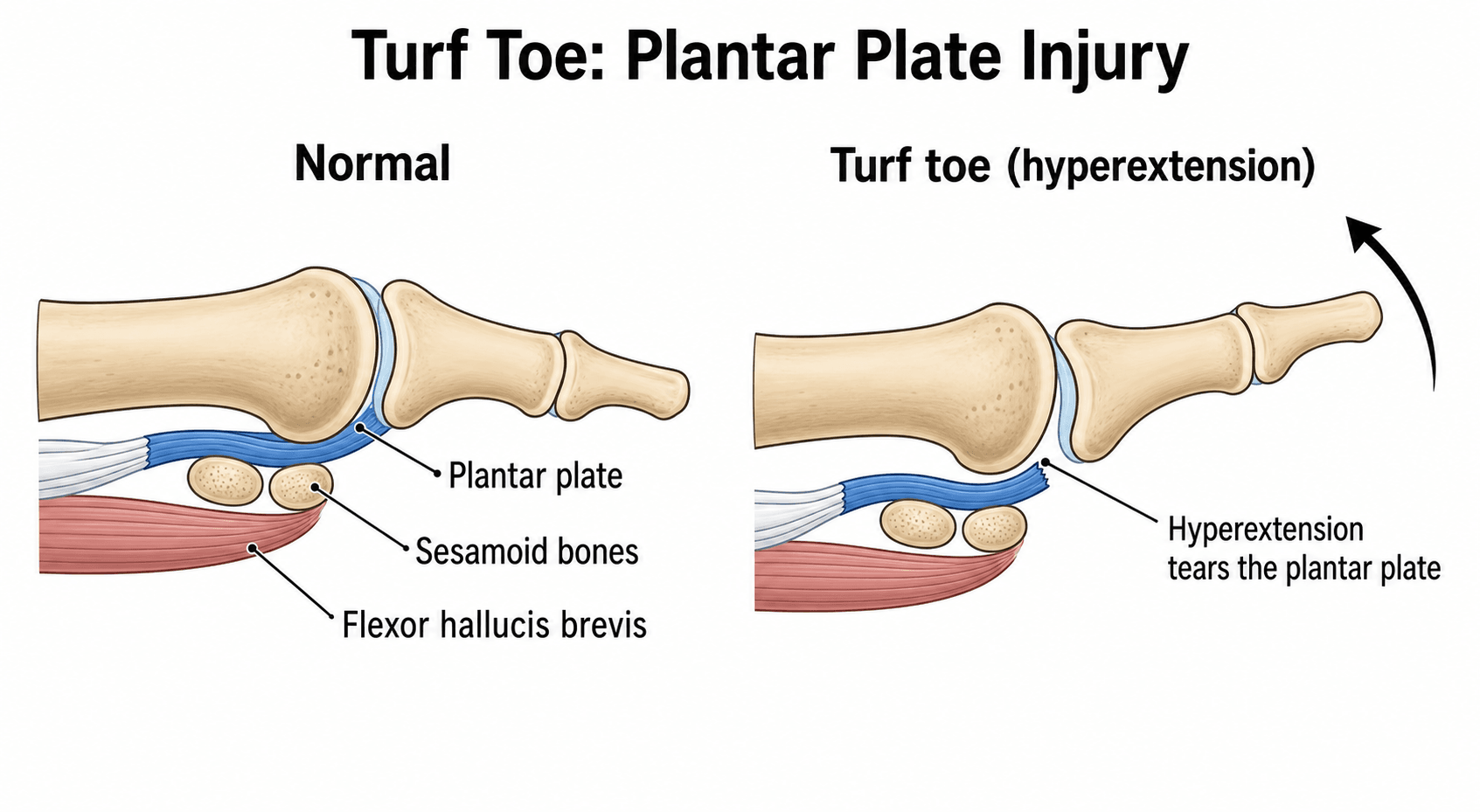
- Hyperextension injury of first MTP with forefoot fixed on ground
- Plantar plate complex (plantar plate + sesamoids + FHB) is key structure
- Anderson Grade 3 with instability or sesamoid retraction may need surgery
- MRI essential for Grade 2-3 to assess soft tissue and surgical planning
- Turf toe plate (carbon fiber insole) essential for return to sport prevention
- “Flexible footwear on hard artificial surface is the classic mechanism
- “Sesamoid proximal migration over 50% suggests complete rupture requiring surgery
- “Loss of push-off strength correlates with plantar plate injury severity
- “Chronic turf toe can lead to hallux rigidus (traumatic arthritis)
Hyperextension of first MTP joint while forefoot is fixed on ground. Body momentum drives proximal phalanx into forced dorsiflexion beyond 45 degrees. Hard artificial turf + flexible shoes = high risk.
Plantar plate complex includes: fibrocartilaginous plantar plate, medial and lateral sesamoids, flexor hallucis brevis (FHB) insertions, and plantar capsule. This complex provides 90% of plantar restraint to hyperextension.
Grade 3 injuries have complete plantar plate disruption with joint instability. Look for: sesamoid proximal migration over 50%, traumatic hallux valgus, positive vertical instability test. May need surgical repair.
Turf toe plate (carbon fiber/steel shank insole) limits MTP dorsiflexion and is standard for return to sport. Reduces recurrence by restricting the injurious dorsiflexion arc. Also consider high-top cleats and stiffer shoe soles.
Overview and Epidemiology
The term was coined in 1976 (Bowers and Martin) after American football moved from grass to artificial turf. The harder, less forgiving surface combined with lighter, more flexible shoes allowed excessive first MTP dorsiflexion. The original Arkansas series (Coker 1978) and subsequent reviews link the rising incidence to this shoe-surface change.
- Population: Common in athletes; well described in American football, also soccer, rugby, basketball, dance, wrestling
- Peak age: Adolescent and young adult athletes (roughly 15-35 years)
- Surface: More frequent on hard artificial surfaces than natural grass
- Footwear: Lighter, flexible-soled shoes increase risk
- Gender: Reflects participation in high-risk contact and cutting sports
- Artificial turf (hard, less forgiving)
- Flexible-soled shoes (allow excess MTP dorsiflexion)
- Previous turf toe (chronic symptoms reported in about half at long-term follow-up; Clanton)
- Hallux rigidus / prior first MTP disease (altered biomechanics)
- First ray hypermobility
Anatomy and Biomechanics
The plantar plate complex is NOT just the plantar plate - it includes the fibrocartilaginous plantar plate, both sesamoids, the FHB tendon insertions, and the plantar capsule. Injury to ANY component can cause turf toe syndrome.
Plantar Plate Structure
- Fibrocartilaginous structure (Type II collagen)
- 8-10mm thick plantarly, thins dorsally
- Originates from metatarsal neck (plantar surface)
- Inserts on proximal phalanx base
- Primary restraint to MTP hyperextension
- Resists forces up to 45 degrees dorsiflexion
- Beyond this threshold, rupture occurs
- Contributes to 90% of plantar stability
- Superficial layer blends with plantar fascia
- Deep layer attaches to sesamoids
- Integrates with collateral ligaments laterally
Understanding plantar plate anatomy is essential for surgical repair.
Pathophysiology and Mechanism
Turf toe occurs when the forefoot is fixed on the ground (e.g., by a tackler landing on the heel) while body momentum drives the proximal phalanx into forced dorsiflexion. The plantar plate is tensioned beyond its 45-degree threshold and tears.
Injury Mechanism Sequence
Foot planted on hard surface (artificial turf). Another player may land on the heel, forcing the foot into dorsiflexion while the forefoot remains fixed.
Body momentum continues forward. Proximal phalanx is driven into dorsiflexion beyond the 45-degree physiological limit. Plantar plate stretched.
Tensile failure of plantar plate - either stretching (Grade 1), partial tear (Grade 2), or complete rupture (Grade 3). Sesamoids may displace proximally.
Associated injury to capsule, collaterals, and surrounding soft tissues. Hemorrhage and edema develop. Functional loss of push-off.
- Hard artificial turf: Doesn't absorb energy
- Flexible shoes: Allow excessive MTP motion
- Cleats caught in turf: Fixed forefoot
- High-velocity sports: Football, soccer, rugby
- Direct blow: Another player landing on heel
- Acute hemorrhage into plantar capsule
- Inflammatory response (swelling, edema)
- Scar formation (may cause stiffness)
- Sesamoid healing (may form nonunion)
- Chronic instability if not treated properly
Anatomical Variants Affecting Injury
- Prevalence
- Variable
- Effect on Turf Toe
- Increased leverage, higher risk
- Prevalence
- 10-30%
- Effect on Turf Toe
- May mimic fracture on imaging
- Prevalence
- Common in females
- Effect on Turf Toe
- Increased MTP dorsiflexion range
- Prevalence
- Older athletes
- Effect on Turf Toe
- Altered mechanics, may protect or predispose
Classification - Anderson Grading System
- Pathology
- Plantar plate STRETCH
- Clinical Findings
- Minimal swelling, localized tenderness, normal ROM
- MRI Findings
- Edema around plantar plate, no tear
- Treatment
- Rest 1-2 weeks, taping, early RTS
- Pathology
- Plantar plate PARTIAL TEAR
- Clinical Findings
- Moderate swelling, ecchymosis, pain with dorsiflexion, decreased ROM
- MRI Findings
- Partial tear visible, sesamoid position normal
- Treatment
- Walking boot 3-4 weeks, protected WB
- Pathology
- Plantar plate COMPLETE RUPTURE
- Clinical Findings
- Severe swelling, ecchymosis, joint instability, loss of push-off
- MRI Findings
- Complete disruption, sesamoid migration over 50%
- Treatment
- Immobilization 6-8 weeks, may need surgery
Look for the "3 S's" of Grade 3 turf toe:
- Sesamoid migration (proximal over 50%)
- Sesamoid diastasis (intersesamoid ligament rupture)
- Stress test positive (vertical instability)
Distinguishing Features by Grade
- Grade 1: Can walk with minimal discomfort
- Grade 2: Significant antalgic gait, difficulty push-off
- Grade 1: Return in days; Grade 2: Return in weeks
- Grade 2: Swelling moderate, joint STABLE
- Grade 3: Swelling severe, joint UNSTABLE
- Grade 2: Sesamoid position NORMAL
- Grade 3: Sesamoid PROXIMAL MIGRATION over 50%
- Stabilize metatarsal head
- Apply vertical force to proximal phalanx
- Positive if more than 2mm dorsal translation
- Pathognomonic for Grade 3
Accurate grading guides treatment and prognosis counseling.
Clinical Presentation and Examination
- Mechanism: Forced hyperextension during sport
- Onset: Immediate pain at great toe
- Sensation: May report "pop" or "tear" feeling
- Function: Difficulty with push-off, antalgic gait
- Sport: Football, soccer, rugby, basketball
- Surface: Often artificial turf
- Footwear: Flexible-soled shoes or cleats
- Inspection: Swelling, ecchymosis (plantar more than dorsal)
- Palpation: Tenderness plantar to first MTP
- ROM: Pain with passive dorsiflexion
- Stability: Vertical instability test (Grade 3)
- Sesamoids: Point tenderness over sesamoids
- Strength: Weakness of FHB (push-off test)
- Gait: Antalgic with toe-off avoidance
Special Tests
- Technique
- Stabilize MT head, dorsally translate PP
- Positive Finding
- Greater than 2mm dorsal translation
- Significance
- Grade 3 plantar plate rupture
- Technique
- Dorsiflex MTP with knee extended
- Positive Finding
- Pain at 30-45 degrees
- Significance
- Plantar plate/capsule injury
- Technique
- Direct pressure over sesamoids
- Positive Finding
- Focal tenderness
- Significance
- Sesamoid fracture or contusion
- Technique
- Single leg heel raise, push off great toe
- Positive Finding
- Weakness or avoidance
- Significance
- FHB dysfunction, functional loss
Clinical findings suggesting Grade 3:
- Massive swelling with ecchymosis extending to arch
- Unable to weight-bear on toes
- Palpable gap in plantar plate
- Positive vertical instability test
- Obvious great toe position change (traumatic hallux valgus)
Differential Diagnosis
- Mechanism / History
- Forced first MTP HYPERextension, forefoot fixed
- Key Distinguishing Features
- Plantar tenderness, pain on passive dorsiflexion, vertical instability if Grade 3
- Investigation
- MRI: plantar plate tear, sesamoid position
- Mechanism / History
- Forced first MTP HYPERflexion (soft surface, barefoot sports)
- Key Distinguishing Features
- DORSAL capsular pain, pain on forced plantarflexion
- Investigation
- MRI: dorsal capsule injury
- Mechanism / History
- Direct axial load or repetitive stress
- Key Distinguishing Features
- Focal sesamoid tenderness, pain on dorsiflexion loading
- Investigation
- Sesamoid views, CT for sharp margins vs bipartite
- Mechanism / History
- Overuse, dancers/runners
- Key Distinguishing Features
- Chronic plantar pain, smooth corticated edges on X-ray
- Investigation
- X-ray, MRI bone marrow oedema
- Mechanism / History
- Insidious, prior trauma or arthritis
- Key Distinguishing Features
- DORSAL osteophyte, painful and limited dorsiflexion, crepitus
- Investigation
- Weight-bearing X-ray: joint narrowing, osteophytes
- Mechanism / History
- Atraumatic, sudden nocturnal onset
- Key Distinguishing Features
- Erythema, warmth, exquisite tenderness, no clear injury
- Investigation
- Serum urate, joint aspirate (negatively birefringent crystals)
- Mechanism / History
- High-energy hyperextension
- Key Distinguishing Features
- Gross deformity, locked joint
- Investigation
- X-ray: frank dislocation, sesamoid entrapment
Investigations
Plain X-ray Assessment
- AP foot (weight-bearing if possible)
- Lateral foot (assess sesamoid position)
- Oblique foot (additional detail)
- Sesamoid view (axial projection)
- Sesamoid fracture (sharp margins)
- Sesamoid proximal migration (compare to contralateral)
- Joint subluxation or diastasis
- Avulsion fractures (plantar phalanx base)
- Compare position to contralateral foot
- Proximal migration over 50% = complete rupture
- Diastasis = intersesamoid ligament rupture
- Cannot assess soft tissue injury
- Bipartite sesamoid may mimic fracture
Always compare sesamoid position to contralateral side.
Management Algorithm
Complications
- Incidence
- 20-30%
- Risk Factors
- Grade 3, delayed treatment
- Prevention/Management
- Adequate healing, proper rehabilitation
- Incidence
- 10-15%
- Risk Factors
- Cartilage injury, repeated trauma
- Prevention/Management
- Protect joint, may need fusion long-term
- Incidence
- 5%
- Risk Factors
- Grade 3 without repair
- Prevention/Management
- Surgical repair if unstable
- Incidence
- 10-15%
- Risk Factors
- Return too early, no prevention
- Prevention/Management
- Turf toe plate, proper timing
- Incidence
- Rare
- Risk Factors
- Displaced fracture
- Prevention/Management
- Excision if symptomatic
- Incidence
- 5-10%
- Risk Factors
- Grade 3 not repaired
- Prevention/Management
- Late surgical stabilization
Hallux rigidus (first MTP arthritis) is the most significant long-term complication. Occurs in 10-15% of Grade 3 injuries due to cartilage damage. May eventually require cheilectomy or fusion. Prevention involves adequate initial treatment and protection.
Grading and Treating the Hallux Rigidus Sequela
Because post-traumatic hallux rigidus is the defining late complication, it is worth knowing how it is graded and managed - examiners often follow a turf-toe question straight into it.
- Dorsiflexion
- 40-60 degrees (10-20% loss)
- Radiograph
- Normal
- Pain
- None
- Dorsiflexion
- 30-40 degrees
- Radiograph
- Dorsal osteophyte, minimal/no joint-space loss
- Pain
- Mild/occasional, at extremes
- Dorsiflexion
- 10-30 degrees
- Radiograph
- Moderate osteophytes, joint-space narrowing and sclerosis
- Pain
- Moderate/constant near maximal ROM
- Dorsiflexion
- Less than 10 degrees (and/or marked plantarflexion loss)
- Radiograph
- Severe changes, sesamoid involvement
- Pain
- Constant, but NO pain at mid-range on grind
- Dorsiflexion
- As grade 3
- Radiograph
- As grade 3
- Pain
- Definite PAIN AT MID-RANGE of passive motion (positive mid-range grind)
For mild-to-moderate disease (grades 1-2, early 3) with reasonable cartilage, cheilectomy (excision of the dorsal osteophyte plus the dorsal ~25-30% of the metatarsal head) relieves dorsal impingement and improves dorsiflexion; a Moberg dorsal closing-wedge phalangeal osteotomy can be added to shift the motion arc into dorsiflexion. For severe disease (grades 3-4), first MTP arthrodesis is the gold standard - reliable pain relief, fused at roughly 10-15 degrees of dorsiflexion relative to the floor and 10-15 degrees of valgus with neutral rotation. Implant arthroplasty is generally avoided at the first MTP in young/active patients (historically high failure/osteolysis with silastic and metallic implants); synthetic-cartilage (e.g. polyvinyl-alcohol) implants are an alternative with mixed evidence, but fusion remains the durable choice for the active post-turf-toe athlete.
Rehabilitation and Return to Sport
Rehabilitation Phases
Goals: Control pain, protect healing tissue
- RICE protocol, protected weight-bearing
- Gentle ROM exercises (within pain limits)
- Maintain cardiovascular fitness (upper body)
- Avoid push-off activities
Goals: Restore ROM, begin strengthening
- Full ROM exercises (active and passive)
- FHB strengthening (towel scrunches, marble pick-up)
- Pool therapy for protected gait
- Balance and proprioception exercises
Goals: Sport-specific preparation
- Progressive resistance exercises
- Single-leg heel raises, push-off drills
- Agility training (cutting, pivoting)
- Turf toe plate in athletic shoes
Goals: Full sport participation
- Sport-specific skills without restriction
- Full-contact practice clearance
- Must pass functional testing
- Turf toe plate mandatory for competition
Return to Sport Criteria
- Grade 1
- Full
- Grade 2
- Full
- Grade 3
- Near-full (90%)
- Grade 1
- Full
- Grade 2
- 90% contralateral
- Grade 3
- 85% contralateral
- Grade 1
- Pass
- Grade 2
- Pass
- Grade 3
- Pass
- Grade 1
- Pass
- Grade 2
- Pass
- Grade 3
- Pass
- Grade 1
- 1-2 weeks
- Grade 2
- 3-6 weeks
- Grade 3
- 3-6 months
All athletes with turf toe should use a turf toe plate (carbon fiber or steel shank insole) for return to sport. This restricts the injurious MTP dorsiflexion arc and is the cornerstone of recurrence prevention. Also consider stiffer-soled shoes and high-top footwear.
Outcomes and Prognosis
Prognostic Factors
- Grade 1-2 injury
- Early diagnosis and treatment
- Stable MTP joint
- No sesamoid migration
- Compliant with rehabilitation
- Proper prevention (turf toe plate)
- Grade 3 with instability
- Sesamoid proximal migration
- Traumatic hallux valgus
- Delayed presentation
- Premature return to sport
- Cartilage injury on MRI
Outcomes by Grade (Gupta et al., 2023; McCormick & Anderson, 2010)
- Grade I: Return as tolerated, typically 3-5 days; players generally regain prior performance
- Grade II: Approximately 2-4 weeks lost; good recovery with protected return and taping support
- Grade III: 4-6 weeks or more (longer if operative); about 70% of higher-grade injuries maintain prior performance level
- Surgery: Fewer than 2% of all turf toe injuries require operative repair (reserved for unstable Grade III, bony injury)
- Chronic sequelae: Clanton's long-term series reported persistent symptoms in roughly half of athletes at over 5-year follow-up, including hallux rigidus
Guidelines, Registries & Global Practice
Turf toe is a soft-tissue sports injury, so there is no implant registry and no single high-level guideline; practice is driven by expert reviews and society sports-medicine guidance. The principles below are consistent worldwide across FRCS, FRACS, EBOT, ABOS, DNB/MS and SICOT examination frameworks.
- Grade-based treatment (Anderson / McCormick-Anderson scheme) is used internationally
- Conservative first: rest, immobilisation and rehabilitation for the large majority; fewer than 2% need surgery (Gupta 2023)
- MRI is the imaging standard for Grade II-III and surgical planning
- Rigid forefoot support (turf toe plate / carbon-fibre insole) for return to sport and prevention
- Threshold for surgery in elite vs recreational athletes (career considerations)
- Imaging access: MRI routine in high-resource settings; clinical grading and radiographs predominate where MRI is scarce
- Custom orthoses / carbon plates readily available in high-resource settings; improvised stiff-soled footwear or steel-shank inserts used elsewhere
- Return-to-sport criteria more formalised in professional sports medicine programmes
- Position on Turf Toe Management
- Grade-based algorithm; conservative care for most; surgical repair for unstable Grade III, sesamoid retraction or diastasis
- Position on Turf Toe Management
- Foot and ankle sports injury principles; MRI for instability; rehabilitation-led return with forefoot stiffening
- Position on Turf Toe Management
- Emphasis on restoring the plantar plate-sesamoid restraint and stable, pain-free push-off when operating
- Position on Turf Toe Management
- Graduated, criteria-based return to sport; protective footwear and load management to prevent recurrence
Wherever you sit your exam, the safe answer is the same: grade the injury, image instability with MRI, treat the great majority conservatively, reserve surgery for the unstable Grade III, and mandate a rigid turf toe plate for return to sport.
Controversies and Areas of Uncertainty
No randomised data compare repair with non-operative care for unstable Grade III. Decisions rest on case series and expert opinion (Coker 1978; Waldrop 2021). The unresolved question is which Grade III injuries truly need repair versus prolonged immobilisation.
The vertical (Lachman-type) instability test and the "over 50%" sesamoid migration threshold are widely quoted but not rigorously validated; inter-observer reliability and exact cut-offs remain uncertain.
Optimal timing is not evidence-defined. Premature return risks conversion to a higher grade or chronic instability, but precise functional clearance criteria vary between programmes.
Turf toe plates and stiffer footwear are biomechanically rational and standard, but high-quality trials quantifying recurrence reduction are lacking - most evidence is mechanistic or observational (Frimenko 2012).
MCQ Practice Points
Q: What is the mechanism of turf toe? A: Hyperextension of the first MTP joint with the forefoot fixed on the ground. Body momentum drives the proximal phalanx into forced dorsiflexion beyond 45 degrees.
Q: What is the primary structure injured in turf toe? A: Plantar plate (plantar capsular-sesamoid complex). This includes the plantar plate, sesamoids, and FHB insertions - provides 90% of plantar restraint to hyperextension.
Q: What finding on X-ray suggests a complete (Grade 3) plantar plate rupture? A: Sesamoid proximal migration greater than 50% compared to contralateral foot. Also look for sesamoid diastasis (intersesamoid ligament rupture).
Q: What are the surgical indications for turf toe? A: CRUSH: Complete rupture with instability, Retraction of sesamoid over 50%, Unstable MTP joint, Sesamoid diastasis, Hallux valgus (traumatic).
Q: What is the most important preventive measure for return to sport after turf toe? A: Turf toe plate (carbon fiber insole). Restricts the injurious MTP dorsiflexion arc and is the cornerstone of recurrence prevention on return to sport.
At a Glance
Turf toe is a hyperextension injury of the first MTP joint caused by forced dorsiflexion beyond 45° while the forefoot is fixed on the ground—classically occurring on artificial turf with flexible footwear. The plantar plate complex (plantar plate, sesamoids, FHB) provides 90% of plantar restraint and is the key structure injured. The Anderson grading system (1-3) guides management: Grade 1-2 are treated conservatively with rest and taping, while Grade 3 (complete rupture with instability or sesamoid retraction over 50%) may require surgical repair. A turf toe plate (carbon fiber insole) is mandatory for return to sport to prevent recurrence.
TURFTurf Toe Features
Hook:TURF toe happens on TURF surfaces!
PLATESPlantar Plate Complex
Hook:The PLATES under the great toe prevent hyperextension!
CRUSHGrade 3 Surgical Indications
Hook:CRUSH injuries need surgery!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old NFL wide receiver hyperextended his great toe during a tackle on artificial turf. He has significant swelling, ecchymosis extending to the arch, and plantar MTP tenderness. He cannot push off. X-rays show no fracture but the tibial sesamoid appears proximally migrated compared to contralateral. What is your diagnosis and management?”
“A 19-year-old university footballer presents 2 days after hyperextending his great toe. Examination shows moderate swelling, ecchymosis, tenderness plantarly, and pain with passive dorsiflexion beyond 30 degrees. The MTP joint is STABLE on vertical instability test. X-rays normal. MRI shows partial tear of plantar plate distal to the sesamoids with edema but sesamoids are in normal position. He has an important match in 2 weeks. How do you manage him?”
“A 32-year-old former professional rugby player presents with 2 years of progressive great toe pain and stiffness. He had multiple turf toe injuries during his career, including one Grade 3 injury treated conservatively. X-rays show first MTP joint space narrowing, dorsal osteophytes, and subchondral sclerosis. He has 15 degrees dorsiflexion (normal 70 degrees). What is your diagnosis and management?”
DEFINITION
- First MTP hyperextension injury
- Plantar plate complex injury
- Artificial turf + flexible shoes = risk
- Sesamoid complex is key stabilizer
- FHB insertions form plantar restraint
ANDERSON GRADING
- Grade 1: Stretch - 1-2 wks RTS
- Grade 2: Partial tear - 3-6 wks RTS
- Grade 3: Complete rupture - 3-6 months
- Grade based on clinical + MRI findings
- Instability distinguishes Grade 2 vs 3
GRADE 3 INDICATORS
- Sesamoid migration over 50%
- Positive vertical instability test
- Sesamoid diastasis
- Traumatic hallux valgus
IMAGING
- X-ray: sesamoid position, fracture
- MRI: grade confirmation, surgical planning
- Compare sesamoids to contralateral
- Forced dorsiflexion views for instability
- T2 shows plantar plate edema/tear
SURGICAL INDICATIONS (CRUSH)
- Complete rupture + instability
- Retraction sesamoid over 50%
- Unstable joint on exam
- Sesamoid diastasis
- Hallux valgus (traumatic)
KEY POINTS
- Turf toe plate ESSENTIAL for RTS
- MRI for all Grade 2-3
- Grade 3: 50-70% return same level
- Long-term: hallux rigidus risk
Evidence Base and Key Studies
Original Turf Toe Series - University of Arkansas Football
- 18 first MTP joint injuries over three football seasons caused 92 missed practices and 7 missed games - disproportionate morbidity versus 74 ankle sprains
- Survey of 94 large US colleges (70% response) implicated artificial turf and lighter, more flexible footwear as contributors
- Rest is the treatment of first choice; taping and a 0.51-mm spring-steel splint were beneficial both pre- and post-injury
- Steroid injection to force early return was contraindicated; late and early surgical repair of capsular rupture could be of benefit
Turf Toe: Anatomy, Diagnosis, and Treatment (Grading Framework)
- Defines the three-grade plantar plate scheme: Grade I sprain/attenuation, Grade II partial rupture, Grade III complete rupture of the plantar capsuloligamentous complex
- Grade I athletes return as tolerated; Grade II typically ~2 weeks; Grade III at least 10-16 weeks to recover
- Some complete (Grade III) ruptures require surgical repair of the plantar plate-sesamoid complex
- MRI is central to confirming grade, defining sesamoid position and planning surgery
Etiology and Biomechanics of First MTP Joint Sprains
- Synthesises the anatomy, biomechanics and incidence of first MTP sprains, with Robert Anderson among the authors
- Hallux push-off is pivotal to acceleration and cutting, explaining the disproportionate functional impact of plantar plate injury
- Forced dorsiflexion beyond the physiological limit loads the plantar plate-sesamoid restraints to failure
- Identifies gaps in mechanical-property data needed to engineer protective footwear and playing surfaces
Assessment and Surgical Treatment of First MTP Sports Injuries
- Most turf toe injuries are managed conservatively with rest, immobilisation and a structured rehabilitation programme
- Surgery is reserved for torn plantar restraints producing an unstable first MTP joint
- Describes repair of the plantar plate and its variants with the expectation of return to play
- Emphasises restoring push-off stability rather than range alone
Updated Review - Rehabilitation and Return-to-Play Outcomes
- Fewer than 2% of turf toe injuries require surgery - typically Grade III with bony injury or severe instability
- Non-operative rehabilitation runs 3 phases up to ~10 weeks; operative rehabilitation 4 phases up to ~20 weeks
- Low-grade injuries usually regain prior performance; about 70% of higher-grade injuries (operative or non-operative) maintain their level
- Grade I returns in ~3-5 days, Grade II loses ~2-4 weeks, Grade III loses 4-6 weeks or more