The Musician's Nerve
Levels
Critical Must-Knows
- The Ulnar Nerve supplies ALL interossei and the Adductor Pollicis.
- Ulnar Paradox: High lesions claw LESS than low lesions because FDP to ring/little is paralyzed.
- Froment's Sign tests the Adductor Pollicis (Patient uses FPL to hold paper).
- Cubital Tunnel Syndrome is the 2nd most common compression neuropathy.
Clinical Pearls
- "Wartenberg's Sign: Persistent abduction of the little finger (3rd Palmar Interosseous weak, EDM unopposed).
- "Jeanne's Sign: Hyperextension of Thumb MCPJ (FPB deep head weak).
- "Duchenne's Sign: The 'Claw Hand' (Hyperextension MCPJ, Flexion IPJ).
Exam Essentials
The Paradox
High vs Low Paradox Examiners love asking why a high lesion looks "better" (less clawing). Answer: "Because the FDP to the ring and little fingers is also paralyzed, removing the deforming flexor force at the IPJs."
Incision Safety
MABC Danger During cubital tunnel approach, watch out for the Medial Antebrachial Cutaneous (MABC) nerve crossing the field. Injury causes painful neuroma and numbness over the olecranon.
| Feature | High (Cubital Tunnel) | Low (Guyon's Canal) |
|---|---|---|
| Sensory Loss | Volar + Dorsal ulnar hand | Volar only (Usually) |
| FDP Function | Weak/Absent (Ring/Little) | Intact |
| Clawing | Mild (Paradox) | Severe |
| Tinel's | At Elbow | At Wrist |
AFIOMuscles Supplied (Hand)
| A | Adductor Adductor Pollicis. |
| F | Flexor FPB (Deep Head). |
| I | Interossei All Dorsal and Palmar. |
| O | Opponens Opponens Digiti Minimi (and ADM/FDM). |
| A | Adductor Adductor Pollicis. | I | Interossei All Dorsal and Palmar. |
| F | Flexor FPB (Deep Head). | O | Opponens Opponens Digiti Minimi (and ADM/FDM). |
Hook:All Fine Interossei Owe (the ulnar nerve).
U-L-N-A-RGuyon's Canal Contents
| U | Ulnar Nerve is Ulnar (medial) to Artery. |
| L | Ligament Volar Carpal Ligament (Roof). |
| N | Hook Hook of Hamate (Lateral wall). |
| A | Artery Ulnar Artery (Lateral to nerve). |
| R | Retinaculum Transverse Carpal Ligament (Floor). |
| U | Ulnar Nerve is Ulnar (medial) to Artery. | A | Artery Ulnar Artery (Lateral to nerve). |
| L | Ligament Volar Carpal Ligament (Roof). | R | Retinaculum Transverse Carpal Ligament (Floor). |
| N | Hook Hook of Hamate (Lateral wall). |
Hook:Anatomy of the canal.
SAM-FODecompression Sites (Elbow)
| S | Struthers Arcade of Struthers (8cm proximal). |
| A | Arcade Arcade of Osborne (FCU heads). |
| M | Medial Medial Intermuscular Septum. |
| F | Fascia Deep Flexor Pronator Aponeurosis. |
| O | Osborne Osborne's Ligament. |
| S | Struthers Arcade of Struthers (8cm proximal). | F | Fascia Deep Flexor Pronator Aponeurosis. |
| A | Arcade Arcade of Osborne (FCU heads). | O | Osborne Osborne's Ligament. |
| M | Medial Medial Intermuscular Septum. |
Hook:Sites of compression.
Overview
Definition
Ulnar Nerve Palsy: Compression or injury of the ulnar nerve leading to intrinsic muscle weakness and sensory loss.
The ulnar nerve is the nerve of fine movement and power grip. Its loss is devastating for manual dexterity.
Anatomy
Course of the Nerve
- Arm: Descends medial to brachial artery. Pierces medial intermuscular septum (Arcade of Struthers).
- Elbow: Passes behind Medial Epicondyle (Cubital Tunnel). Enters forearm between two heads of FCU (Osborne's Ligament).
- Forearm: Deep to FCU. Gives off Dorsal Cutaneous Branch (5cm prox to wrist).
- Wrist: Enters Guyon's Canal (superficial to Flexor Retinaculum).
The Dorsal Cutaneous Branch is key to localizing the lesion (High vs Low). Knowing the course aids exposure.
Pathophysiology
Sites of Compression
Cubital tunnel (elbow): Most common site
- Between medial epicondyle and olecranon
- Osborne ligament forms roof
- Nerve stretched with elbow flexion
- Traction and compression combine to cause injury
Guyon canal (wrist):
- Between hook of hamate and pisiform
- May be compressed by ganglion, fracture, or ulnar artery aneurysm
- Motor and sensory branches divide within canal
Mechanism of Nerve Injury
Compression:
- External pressure reduces intraneural blood flow
- Initially affects large myelinated fibers (sensory first)
- Prolonged compression causes axonal degeneration
- Schwann cell damage leads to demyelination
Traction:
- Nerve elongates with elbow flexion
- Cubital tunnel pressure increases 6-fold in flexion
- Chronic traction leads to fibrosis and adhesions
Double crush phenomenon:
- Compression at one site sensitizes nerve to compression at another
- Cervical radiculopathy may coexist with cubital tunnel syndrome
- Always examine entire upper extremity
Progression of Injury
Seddon classification applies:
- Neurapraxia: Demyelination, complete recovery expected
- Axonotmesis: Axon damage, recovery depends on distance to target
- Neurotmesis: Complete disruption, requires repair
Classification
McGowan Classification (Cubital Tunnel)
- Grade I (Mild): Sensory symptoms only (intermittent paresthesia). No weakness.
- Grade II (Moderate): Weakness of intrinsics. Wasting may be present. Constant numbness.
- Grade III (Severe): Profound weakness. Severe wasting. Paralysis.
Surgery is indicated for Grade II and III. Dellon's modification helps track recovery.
Clinical Signs
Froment's Sign: Screen for Adductor Pollicis weakness.
- Ask to hold paper between thumb and index (Key Pinch).
- Positive: IPJ flexes (FPL compensation). Jeanne's Sign: Hyperextension of MPJ during pinch (FPB weakness). Wartenberg's Sign: Persistent abduction of Little Finger.
- Mechanism: Weak 3rd Palmar Interosseous (can't adduct). Unopposed EDM (pulls into abduction). Duchenne's Sign (Claw):
- Hyperextension of MCPJs (unopposed EDC).
- Flexion of IPJs (unopposed FDP/FDS - lack of Lumbrical anti-gravity force).
Investigations
Nerve Conduction Studies (NCS):
- Slowing: Velocity less than 50 m/s across the elbow.
- Block: Conduction block (drop in amplitude) across elbow greater than 20 percent.
- EMG: Denervation potentials in ulnar muscles.
Imaging:
- Ultrasound: Can show nerve swelling (CSA greater than 10 mm squared, best at medial epicondyle) or dynamic subluxation. Pooled sensitivity ~0.85, specificity ~0.91 at the 10 mm squared cut-off.
- MRI: Useful for space-occupying lesions (tumours, ganglions in Guyon's canal).
Differential Diagnosis
The classic trap is mistaking a more proximal lesion for a focal ulnar entrapment. Always examine the whole limb and the neck.
| Condition | Distinguishing Feature | Key Test |
|---|---|---|
| Cubital tunnel (high ulnar) | Dorsal ulnar sensory loss, FCU/FDP weak, Tinel at elbow | NCS slowing across elbow |
| Guyon's canal (low ulnar) | Dorsal sensation spared, FDP intact, severe clawing | MRI/US for hamate # or ganglion |
| C8/T1 radiculopathy | Neck pain, dermatomal sensory loss extends past wrist, median-innervated thenar also weak | MRI cervical spine; NCS normal across elbow |
| Thoracic outlet syndrome | Lower-trunk pattern, positional symptoms, vascular signs | Provocative tests, NCS/imaging |
| Pancoast tumour (lower plexus) | Constant pain, Horner's syndrome, weight loss | Apical chest imaging |
| Motor neurone disease (early) | Painless wasting, fasciculations, no sensory loss, spread beyond ulnar territory | EMG (widespread denervation) |
The Examiner's Favourite Trap
Painless intrinsic wasting with no sensory loss that does not respect the ulnar territory is a red flag for motor neurone disease, not cubital tunnel syndrome. Sensory loss extending proximal to the wrist crease points to a root (C8/T1) or plexus lesion, not the ulnar nerve.
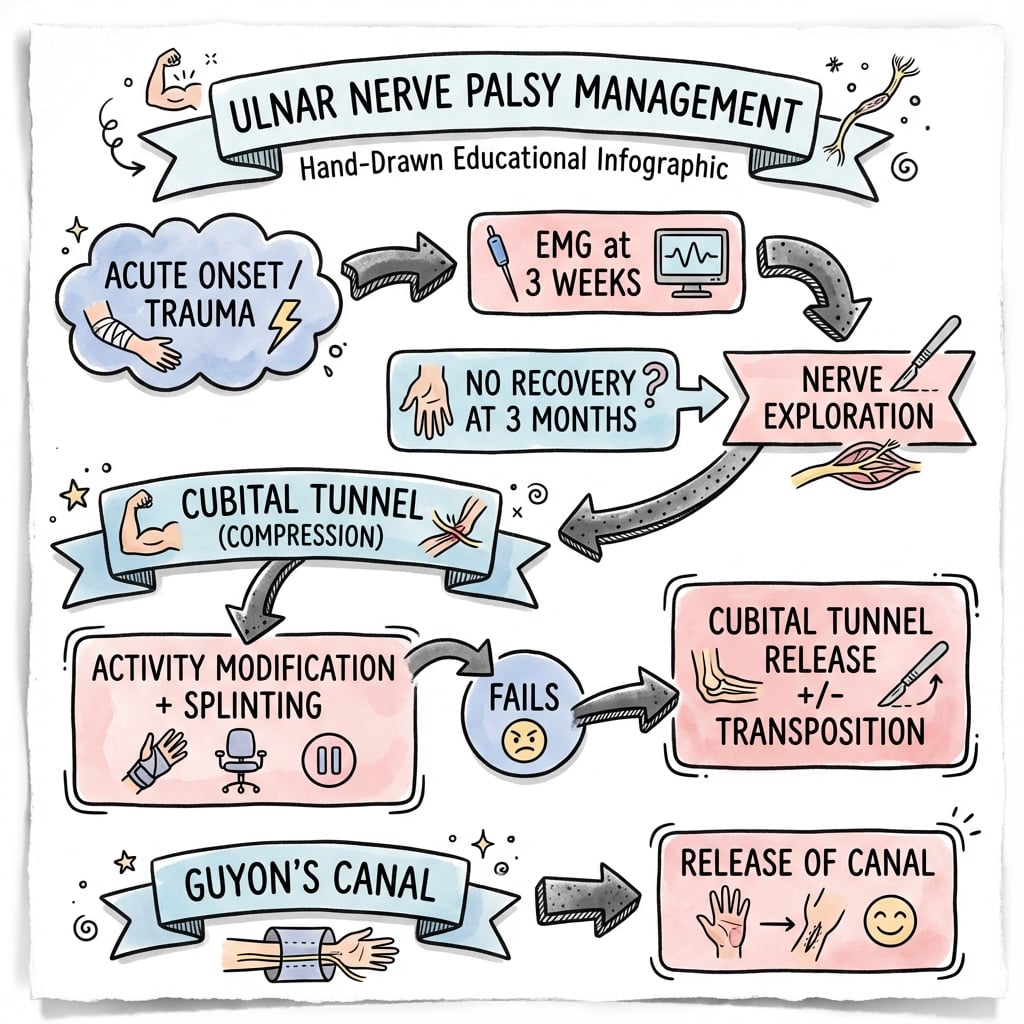
Management Algorithm
Conservative Management
- Indications: Grade I (Sensory only), Mild symptoms.
- Splinting: Night splinting with elbow in 45 deg flexion (prevents max stretch).
- Activity: Avoid prolonged flexion (phone use).
- Glide: Nerve gliding exercises.
Success rate is roughly 50 percent for mild cases. Patient education is key.
Surgical Technique
Tendon Transfers for the "Claw Hand" (Anti-Claw)
-
Goal: Prevent MCP hyperextension (which allows EDC to extend IPJs).
-
Static: 'Lasso' procedures (Zancolli) - Capsulodesis.
-
Dynamic:
- Stiles-Bunnell / Brand: Use FDS (Middle or Ring) split into 2 slips. Pass through lumbrical canal. Insert into Lateral Bands.
- This restores the "intrinsic plus" position.
- Requires motor relearning.
- Fowler: EIP to Lateral Bands.
Steps for Stiles-Bunnell:
- Harvest FDS to Middle Finger.
- Split into two tails.
- Pass volar to transvere metacarpal ligament.
- Attach to Radial Lateral Bands of Ring and Little fingers.
- Tension with wrist in neutral and fingers in intrinsic plus.
This technique creates a dynamic tenodesis effect.
- Stiles-Bunnell / Brand: Use FDS (Middle or Ring) split into 2 slips. Pass through lumbrical canal. Insert into Lateral Bands.
Specific Details
Ulnar Nerve Transposition Technique:
- Incision posterior to medial epicondyle.
- Identify and protect MABC.
- Release Arcade of Struthers (ensure no kink).
- Release Cubital Tunnel retinaculum.
- Release FCU fascia (Osborne).
- Isolate nerve. Excision of Medial Intermuscular Septum is CRITICAL to prevent kinking when transposed.
- Move anteriorly. Secure with fascial sling or bury (submuscular).
Complications
MABC Neuroma
- Incidence: Common if incision is too anterior.
- Symptoms: Painful numbness over olecranon.
- Prevention: Find the nerve. Protect it.
The MABC is often mistaken for a vein.
Postoperative Care
- Soft dressing.
- Avoid hyperflexion.
- Immediate finger movement.
- Removal of sutures.
- Start nerve gliding.
- Strengthening exercises.
- Return to heavy work (if submuscular, may delay to 3 months).
Prognosis
- Outcome: Good for Grade I/II.
- Grade III: Recovery of intrinsics is unpredictable (often incomplete).
- Age: Older patients recover less motor function.
- Diabetes: Poor prognostic factor ("Double Crush").
Recurrence of symptoms after simple decompression forces a decision: Re-do decompression (if adhesions) or Transposition (if subluxation). Most surgeons opt for Submuscular Transposition in revision cases.
Controversies & Areas of Uncertainty
Decompression vs Transposition
The Bartels RCT and subsequent meta-analyses show equivalent clinical outcomes with fewer complications after simple decompression, even when the nerve subluxes. Yet many surgeons still transpose a subluxating nerve. The honest exam answer: simple decompression is the evidence-based default, with transposition reserved for frank instability, prior trauma, valgus deformity, or revision.
- Does subluxation mandate transposition? Bartels found subluxation did not affect simple-decompression outcomes; some surgeons disagree based on iatrogenic-instability concerns.
- Endoscopic vs open release: Equivalent symptom relief; endoscopic offers less scar tenderness but a higher haematoma rate. No clear winner.
- Subcutaneous vs submuscular transposition: No high-level evidence of superiority for either; choice is driven by soft-tissue cover and surgeon preference.
- Role of nerve transfers (SETS): Promising for high/severe lesions, but evidence is largely retrospective; outcomes are strongly time-dependent (better with surgery under 12 months).
- Conservative management: Splinting and nerve gliding help mild disease, but compliance is poor and high-quality RCT evidence is limited.
Evidence Base
Simple Decompression vs Anterior Subcutaneous Transposition (RCT)
- Prospective single-blind RCT, 152 patients randomised (75 simple decompression, 77 anterior subcutaneous transposition), 1-year follow-up
- Good/excellent outcome similar: 49/75 (decompression) vs 54/77 (transposition); difference not statistically significant
- Complication rate significantly lower with simple decompression: 9.6 percent vs 31.1 percent (RR 0.32, 95 percent CI 0.14 to 0.69)
- Subluxation of the nerve did NOT influence outcome of simple decompression
Submuscular Transposition (Musculofascial Lengthening)
- Prospective series, 121 patients (161 limbs), mean follow-up 45.6 months
- 88 percent good-to-excellent results (65 percent excellent, 23 percent good); recurrence in only 0.5 percent
- Significant improvement in both motor and sensory scores (p less than 0.001), including in diabetic and severe-compression subgroups
Endoscopic vs Open In-Situ Release (Meta-analysis)
- Systematic review and meta-analysis, 5 studies, 655 patients (226 endoscopic, 429 open)
- No significant difference in good/excellent Bishop score or VAS reduction between techniques
- Endoscopic release: less scar tenderness/elbow pain (OR 0.19) but higher post-operative haematoma rate (OR 5.70)
- Reoperation rates similar (endoscopic 4.9 percent vs open 4.1 percent)
Anterior Interosseous-to-Ulnar Motor Nerve Transfer (Supercharged End-to-Side)
- Retrospective review, 32 patients undergoing AIN-to-ulnar motor transfer for high ulnar lesions
- Overall mean recovery BMRC 2.9/5; supercharged end-to-side (SETS) outperformed end-to-end (3.2 vs 2.6)
- Earlier surgery (under 12 months) gave better recovery than later surgery (BMRC 3.7 vs 2.2, p less than 0.01)
- No donor deficits; the AIN 'babysits' denervated intrinsics while the proximal ulnar axons regenerate
Ultrasound Cross-Sectional Area for Diagnosis (Meta-analysis)
- Meta-analysis of 14 studies of ulnar nerve cross-sectional area (CSA) on ultrasound
- Greatest case-control difference in CSA at the medial epicondyle
- Using a 10 mm squared cut-off: pooled sensitivity 0.85, specificity 0.91, diagnostic OR 53.96
- CSA in healthy nerves rarely exceeds 10 mm squared at any level
Population Incidence of Ulnar Neuropathy at the Elbow
- First population-based incidence study (Siena, Italy; 251,930 residents, 1995 to 1999)
- Mean annual crude incidence 24.7 per 100,000 person-years (standardised 20.9)
- Marked male predominance (men 32.7 vs women 17.2 per 100,000); incidence rises with each decade of age
- Incidence roughly one-thirteenth that of carpal tunnel syndrome, confirming it as the 2nd commonest upper-limb compression neuropathy
AAOS / BOA-BOAST & EFORT Consensus on Cubital Tunnel
- Diagnosis is primarily clinical, supported by electrodiagnostic studies; routine imaging is not required for typical cases
- A trial of non-operative management (activity modification, night splinting, nerve gliding) is recommended for mild (McGowan I) disease
- Surgery is indicated for motor involvement/wasting (McGowan II to III) or failed conservative care; simple decompression is first-line
- Transposition is reserved for nerve instability/subluxation, prior trauma, valgus deformity or revision
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: The Claw Hand
"A 60-year-old man presents with a clawed ring and little finger. He has wasting of the first dorsal interosseous. Sensation is decreased on the volar small finger but NORMAL on the dorsum of the hand."
Scenario 2: Failed Decompression
"A patient had a simple decompression 6 months ago. Symptoms persisted and are now worse. There is snapping."
Scenario 3: The Musician
"A violinist complains of numbness in the small finger when playing. Symptoms resolve with rest."
MCQ Practice Points
Anatomy
Q: What structure forms the roof of the Cubital Tunnel? A: Osborne's Ligament (Arcuate ligament bridging the two heads of FCU).
Paradox
Q: Why is clawing less severe in high ulnar nerve palsy? A: Paralysis of the FDP to the ring/little fingers reduces the flexion moment at the IP joints.
Signs
Q: What muscle is being compensated for in Froment's Sign? A: Adductor Pollicis (Compensated by FPL).
Guyon's Canal
Q: What are the three zones of Guyon's Canal? A: Zone 1 (Mixed - motor and sensory), Zone 2 (Motor only - around hook of hamate), Zone 3 (Sensory only).
Wartenberg's Sign
Q: What causes Wartenberg's Sign (abducted little finger)? A: Weakness of the 3rd Palmar Interosseous (adductor) with unopposed EDM (abductor) action.
Nerve Course
Q: Where does the dorsal cutaneous branch of the ulnar nerve arise? A: Approximately 5cm proximal to the wrist. This helps differentiate high vs low lesions (intact in Guyon's Canal lesions).
Guidelines, Registries & Global Practice
Global Epidemiology
- Cubital tunnel syndrome (ulnar neuropathy at the elbow) is the 2nd most common upper-limb compression neuropathy after carpal tunnel syndrome.
- Population-based incidence: roughly 20 to 25 per 100,000 person-years (Siena, Italy cohort), with a clear male predominance and rising incidence with age.
- Strong association with manual/occupational elbow flexion and leaning, and with diabetes, smoking and prior elbow trauma/valgus deformity.
Side-by-Side Guideline Comparison
| Issue | AAOS (US) | BOA / BSSH (UK) | AO / EFORT (Europe) |
|---|---|---|---|
| Diagnosis | Clinical + NCS; imaging selective | Clinical first; NCS to confirm/grade | Clinical + NCS; ultrasound increasingly used |
| Mild disease (McGowan I) | Trial of conservative care | Activity modification, night splint | Conservative; nerve gliding |
| First-line surgery | Simple in-situ decompression | Simple decompression | Simple decompression |
| Transposition | Instability/revision/valgus | Instability/subluxation | Subluxation, prior trauma, revision |
Practice Variation: High vs Limited Resource Settings
- High-resource: Routine access to NCS/EMG, high-resolution ultrasound, and endoscopic release; nerve transfers (SETS AIN-to-ulnar) available in tertiary hand units.
- Limited-resource: Diagnosis often clinical without electrodiagnostics; open simple decompression is the mainstay due to low cost and minimal equipment; tendon transfers for fixed claw deliver high value where microsurgical reconstruction is unavailable.
- Therapy: Skilled hand therapists for 'anti-claw' (lumbrical-bar) splinting and nerve-gliding programmes substantially improve outcomes and are emphasised across all settings.
Clinical summary
Localization
- •Dorsal Sensation Intact = Wrist (Low)
- •Dorsal Sensation Lost = Elbow (High)
- •FDP Intact = Wrist (Low) to More Clawing
- •FDP Weak = Elbow (High) to Less Clawing
Compression Sites (SAM-FO)
- •Struthers (Arcade)
- •Arcade of Osborne
- •Medial Septum
- •Fascia
- •Osborne's Ligament
Signs
- •Froment: Adductor (Thumb IP Flex)
- •Wartenberg: 3rd Palmar (Little finger Abd)
- •Jeanne: FPB (Thumb MCP Ext)
- •Duchenne: Claw
Treatment Algorithm
- •Mild: Observation, Splinting, Activity Modification
- •Moderate: Simple Decompression vs Transposition
- •Severe: Anterior Transposition
- •Fixed Claw: Tendon Transfers