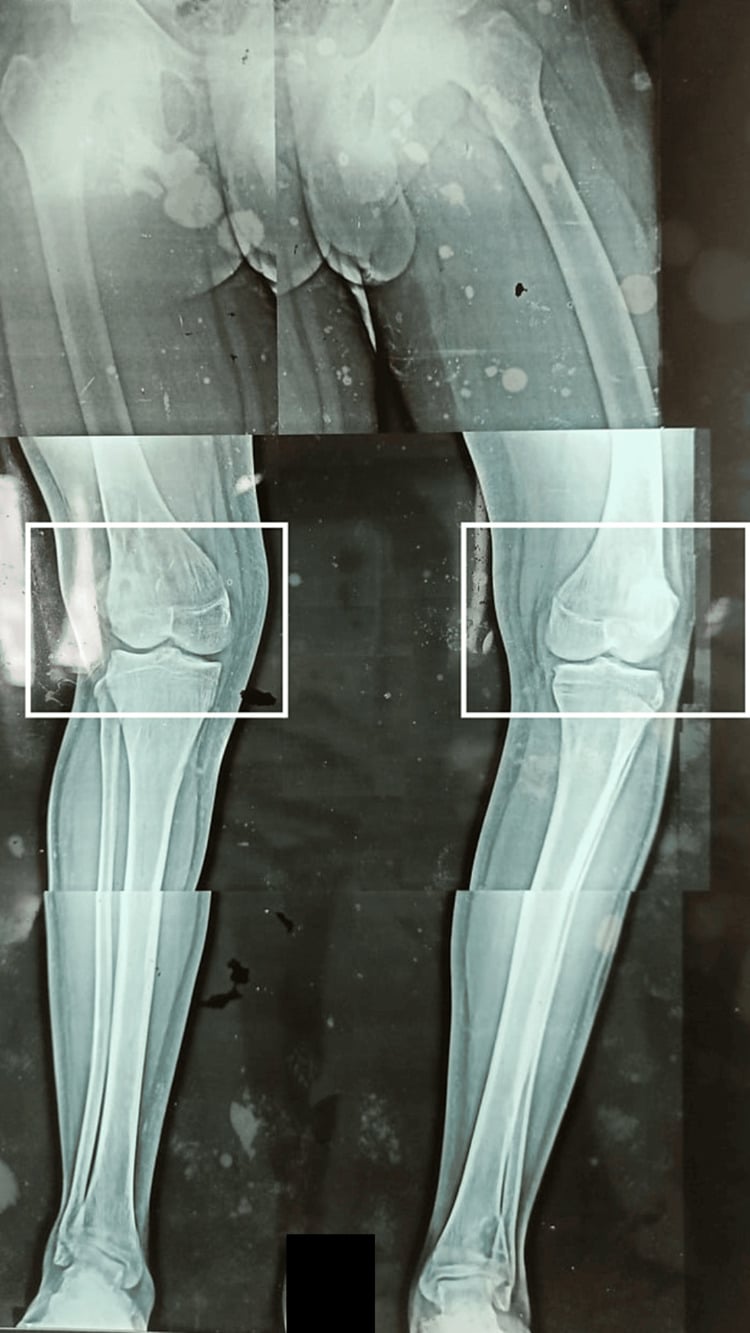
Genu Valgum One Side, Varum the Other
- WINDSWEPT DEFORMITY is an ASYMMETRIC coronal-plane lower-limb deformity in which ONE leg has GENU VALGUM (knock-knee) and the OTHER has GENU VARUM (bow-leg), so the legs appear 'swept' to one side; the analogous HIP windswept pattern (ABDUCTION of one hip, ADDUCTION of the other) is classically seen in cerebral palsy (and contributes to hip displacement).
- The crucial conceptual point is that windswept deformity is a SYMPTOM/SIGN with MULTIPLE possible aetiologies, NOT a single disease; the clinician's task when faced with it is to identify the UNDERLYING DISORDER, which then directs management.
- The AETIOLOGIES fall into FOUR groups described in the systematic review: RICKETS and other METABOLIC bone disease (the LARGEST group - nutritional/hypophosphataemic rickets, renal osteodystrophy); SKELETAL DYSPLASIAS and other GENETIC disorders; TRAUMA (physeal injury/malunion causing asymmetric growth); and a 'descriptive'/idiopathic group without a specific underlying disorder - in which ALL patients were otherwise-healthy children of African descent presenting between about 2 and 3 years of age.
- BE PRECISE ABOUT 'LARGEST GROUP' - it is a count of ARTICLES, not of patients. The review pooled 45 publications, most of which its own authors classify as LOW level of evidence, and reports no patient-level denominator. So rickets generated the most literature; NO study has established what proportion of children with windswept deformity actually have it. The English-language-only search compounds this, since nutritional rickets is concentrated in settings that publish in other languages. Screen for it because it is common, treatable and dangerous to miss - not because a prevalence figure supports it.
- NEUROMUSCULAR disease, particularly CEREBRAL PALSY, is a classic cause of the windswept pattern (especially at the HIPS - one hip abducted/externally rotated and the other adducted/internally rotated), reflecting asymmetric muscle tone, and it is relevant to hip surveillance/displacement in CP.
- The WORK-UP therefore aims to FIND THE CAUSE: a careful history and examination, full-length standing ALIGNMENT RADIOGRAPHS to characterise the deformity (and localise it to bone/physis), and a METABOLIC SCREEN (calcium, phosphate, alkaline phosphatase, vitamin D, renal function/PTH) to detect rickets/metabolic disease, with genetic assessment where a dysplasia is suspected.
- MANAGEMENT is AETIOLOGY-DIRECTED: treat RICKETS/metabolic disease MEDICALLY (and much of the deformity may correct or stabilise), correct residual or structural deformity ORTHOPAEDICALLY (guided growth/hemiepiphysiodesis or osteotomy as appropriate), and manage the neuromuscular (CP) or dysplastic context accordingly - the error to avoid is correcting the deformity surgically while missing a treatable underlying metabolic cause.
- “Windswept deformity = genu VALGUM in one leg + genu VARUM in the other (legs 'swept' one way); at the HIPS = abduction of one + adduction of the other (classic in cerebral palsy).
- “It is a SYMPTOM with many causes, not a disease - FIND the underlying cause. FOUR review groups: RICKETS/metabolic (largest), skeletal dysplasias/genetic, trauma/physeal injury, idiopathic (all African-descent, healthy, ~2-3y); neuromuscular/CP is separately recognised.
- “'Largest group' counts ARTICLES, not patients - the review pooled 45 mostly LOW-level-evidence papers, English-language only, with no patient denominator. No prevalence for any aetiology has been measured. Screen for rickets because it is treatable and dangerous to miss, not because a figure supports it.
- “Work-up: alignment radiographs + METABOLIC SCREEN (Ca/PO4/ALP/vitamin D/renal-PTH) + history/exam (+/- genetics). Treat the CAUSE (medical for rickets) then correct residual deformity (guided growth/osteotomy). Don't operate while missing a treatable metabolic cause.
Genu valgum in one leg + genu varum in the other (legs swept one way). At the hips: one abducted + one adducted (classic in cerebral palsy).
It is a symptom with many causes - rickets/metabolic disease produced the most published cases (an article count, not a prevalence), plus skeletal dysplasia, trauma/physeal injury, idiopathic and neuromuscular. Screen before you correct.
Definition, Causes & Work-up
Windswept deformity is an asymmetric coronal deformity - genu valgum in one leg and genu varum in the other (the analogous hip pattern - one hip abducted, one adducted - is classic in cerebral palsy). It is a sign with many causes, not a single disease, so the task is to find the underlying cause. The aetiological groups are rickets/metabolic bone disease (the largest), skeletal dysplasias/genetic disorders, trauma (physeal injury/malunion), an idiopathic group (healthy children of African descent at ~2-3 years), and neuromuscular disease (CP). The work-up is history/examination, full-length alignment radiographs, and a metabolic screen (calcium, phosphate, alkaline phosphatase, vitamin D, renal function/PTH), with genetics where a dysplasia is suspected.
- Examples
- Nutritional/hypophosphataemic rickets, renal osteodystrophy
- Note
- Largest group - treat medically (deformity may correct)
- Examples
- Various dysplasias/genetic disorders
- Note
- Genetic assessment; deformity correction in context
- Examples
- Physeal injury / malunion (asymmetric growth)
- Note
- Localise to the physis; guided growth/osteotomy
- Examples
- Otherwise-healthy children (all of African descent, ~2-3 y)
- Note
- No specific underlying disorder identified
- Examples
- Cerebral palsy (esp. hip windswept)
- Note
- Not one of the review's four groups; asymmetric tone, relevant to hip surveillance
Management
- Find and treat the cause: rickets/metabolic disease is treated medically (correcting it may resolve or stabilise much of the deformity); manage the dysplastic or neuromuscular (CP) context.
- Correct residual/structural deformity: guided growth (hemiepiphysiodesis) in the growing child, or osteotomy for established/severe deformity - aetiology- and physis-appropriate.
- Hip windswept (CP): address within CP hip surveillance/management (tone management, soft-tissue/bony surgery).
- Avoid the error: do NOT correct surgically while a TREATABLE metabolic cause (rickets) is missed - screen first.
The single most important lesson with windswept deformity is that it is a sign rather than a diagnosis, and the aetiology must be established before treatment. The largest aetiological group is rickets and other metabolic bone disease, which is medically treatable - and correcting the metabolic abnormality may resolve or substantially improve the deformity - so a metabolic screen (calcium, phosphate, alkaline phosphatase, vitamin D, renal function and PTH) is essential, and the error to avoid is proceeding to surgical correction while missing a treatable cause such as rickets. The other groups - skeletal dysplasias and genetic disorders, trauma with physeal injury, an idiopathic group (classically otherwise-healthy young children of African descent presenting at two to three years), and neuromuscular disease such as cerebral palsy (especially the hip windswept pattern) - each direct different management. Once the cause is identified and treated, residual or structural deformity is corrected appropriately, with guided growth in the growing child or osteotomy for established deformity.
Why the Deformity Is Asymmetric
- The paradox. A systemic bone problem such as rickets weakens both physes equally, so it is not obvious why one knee should go valgus and the other varus rather than both the same way. The asymmetry is thought to arise where a generalised bone-quality problem is expressed asymmetrically by asymmetric mechanical loading.
- The Hueter-Volkmann principle. Increased compression across a physis slows its growth (and reduced compression accelerates it), so asymmetric weight-bearing or posture - habitual asymmetric sitting/lying, gait asymmetry, or a leg-length discrepancy shifting load - can drive one physis into valgus growth and the other into varus.
- A unilateral insult or dominance. A preceding unilateral problem (trauma, infection, or a Blount-type medial-physeal insult on one side) or limb dominance can tip one leg while the other follows the systemic/postural tendency. In cerebral palsy, asymmetric muscle tone (adductor/abductor imbalance) drives the hip windswept and, in turn, the knees.
Q: Why is windswept deformity asymmetric when many causes (e.g. rickets) are systemic and bilateral?
A: A systemic bone problem weakens both physes, but the asymmetry arises where it is expressed asymmetrically by asymmetric mechanical loading - the Hueter-Volkmann principle (increased compression across a physis slows growth), so asymmetric weight-bearing/posture (sitting/lying, gait, a leg-length discrepancy) drives one physis into valgus and the other into varus. A preceding unilateral insult (trauma/infection/Blount) or limb dominance can tip one side; in CP asymmetric muscle tone drives the hip (and knee) windswept.
Correcting Windswept: Opposite Sides, Metabolic Control First
- Opposite corrections on the two legs. Because one knee is valgus and the other varus, the guided growth is side-specific and opposite: the valgus knee is tethered on the medial physis (a tension-band plate on the medial distal femur ± medial proximal tibia, so the lateral side catches up), while the varus knee is tethered on the lateral physis - so the same child receives a medial plate on one leg and a lateral plate on the other.
- Control the metabolic disease first. Guided growth in active rickets is unreliable - the soft physes tether poorly and rebound after plate removal - so the vitamin-D/phosphate abnormality should be optimised first or concurrently; much deformity may then remodel without surgery.
- Osteotomy for the mature or severe. Corrective osteotomy (at the deformity apex) is reserved for the skeletally mature, or for severe or failed guided growth; monitor for rebound after plate removal in the young child.
Q: How does correction differ in windswept deformity, and what must come first?
A: The two legs need opposite guided growth: the valgus knee is tethered on the medial physis (medial plate → lateral catches up) and the varus knee on the lateral physis - so one leg gets a medial plate and the other a lateral plate. But the underlying metabolic disease (rickets) must be controlled first/concurrently - guided growth in active rickets tethers poorly and rebounds - and much deformity may remodel with medical treatment alone. Osteotomy (at the apex) is reserved for the skeletally mature or severe/failed cases; monitor for rebound after plate removal.
Mnemonics & Memory Aids
SWEPT
Hook:SWEPT: Symptom not disease, Windswept (valgum+varum), Evaluate metabolically (rickets), Plus other causes, Treat the cause then correct.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child presents with one knock-knee and one bow-leg. What is this called, how do you think about it, and how do you manage it?”
What it is
- Genu valgum in one leg + genu varum in the other (legs swept one way)
- Hip windswept: one hip abducted + the other adducted (classic in cerebral palsy)
- A SIGN/symptom with many causes - not a single disease
Aetiologies
- Four review groups: rickets/metabolic (largest by ARTICLE count, not patients)
- Skeletal dysplasias/genetic disorders; trauma (physeal injury/malunion)
- Idiopathic (all African descent, otherwise healthy, ~2-3 y)
- Neuromuscular (CP) is separately recognised, not one of the four groups
- No prevalence measured for any aetiology; review pooled 45 mostly low-level, English-only papers
Work-up & management
- History/exam + full-length alignment radiographs + metabolic screen (Ca/PO4/ALP/vit D/renal-PTH)
- Treat the cause (medical for rickets - deformity may correct)
- Correct residual/structural deformity (guided growth/osteotomy); don't miss a treatable metabolic cause
Evidence & Key Studies
Windswept deformity - a disease or a symptom? A systematic review of aetiologies
- A PRISMA systematic review of 45 articles - but read its own closing caveat: the authors state that, by the Oxford criteria, MOST OF THE INCLUDED ARTICLES ARE OF LOW LEVEL OF EVIDENCE. The systematic method is sound; the material it pools is largely case reports and small series, so this is not high-level evidence about aetiology.
- Windswept deformity (simultaneous genu valgum and genu varum) is best regarded as a symptom with multiple possible aetiologies rather than a single disease.
- FOUR groups were described: 'rickets and other metabolic disorders', 'skeletal dysplasias and other genetic disorders', 'trauma', and 'descriptive articles without a specific underlying disorder' - with rickets the largest.
- CRITICAL QUALIFICATION ON 'LARGEST': the groups count ARTICLES, not patients. No patient-level denominator or prevalence is reported, so 'rickets is the largest group' means it generated the most publications - it does NOT establish that most children with windswept deformity have rickets. No study has measured the true aetiological distribution in any population.
- In the group without a specific underlying disorder, ALL patients were of African descent, otherwise healthy, presenting between two and three years of age.
- Further limitations: the search was restricted to ENGLISH-LANGUAGE articles, which matters greatly for a deformity whose major causes include nutritional rickets in low- and middle-income settings, and articles with windswept deformity as an incidental ancillary finding were included alongside those studying it directly.
The conceptualisation of windswept deformity as a symptom rather than a disease, the four aetiological groups with rickets the largest, and the observation that all patients in the group without a specific underlying disorder were otherwise-healthy children of African descent presenting at two to three years come from Jansen (DOI), a PRISMA systematic review of 45 articles restricted to English-language publications, whose authors state that most included articles are of LOW level of evidence. The definition, the hip windswept pattern in cerebral palsy, the metabolic work-up, the Hueter-Volkmann explanation for the asymmetry, and aetiology-directed management are standard, well-established teaching.
What is not established: the groups above count articles, not patients, so there is no measured prevalence for any aetiology and no published figure for what proportion of children with windswept deformity have rickets, a dysplasia, or no identifiable cause. Cerebral palsy is a separately recognised cause rather than one of the review's four groups. There is no validated severity classification for windswept deformity, no threshold defining when it warrants correction, no comparative trial of guided growth against osteotomy in this pattern, and no published rebound rate after plate removal specific to windswept limbs - the caution about operating during active rickets is a reasoned principle from physeal biology, not a measured failure rate.