Lenke Classification | Bracing Protocols | Surgical Indications
- Lenke modifiers - Lumbar spine modifier (A/B/C based on CSVL), Sagittal thoracic modifier (-, N, +)
- Risser sign - Iliac apophysis ossification (0-5) predicts growth remaining
- Cobb angle - Angle between perpendiculars of most tilted vertebrae
- Bracing indications - Curves 25-40° in skeletally immature patients (Risser 0-2)
- SRS-30 outcomes - Pain, self-image, function, mental health, satisfaction
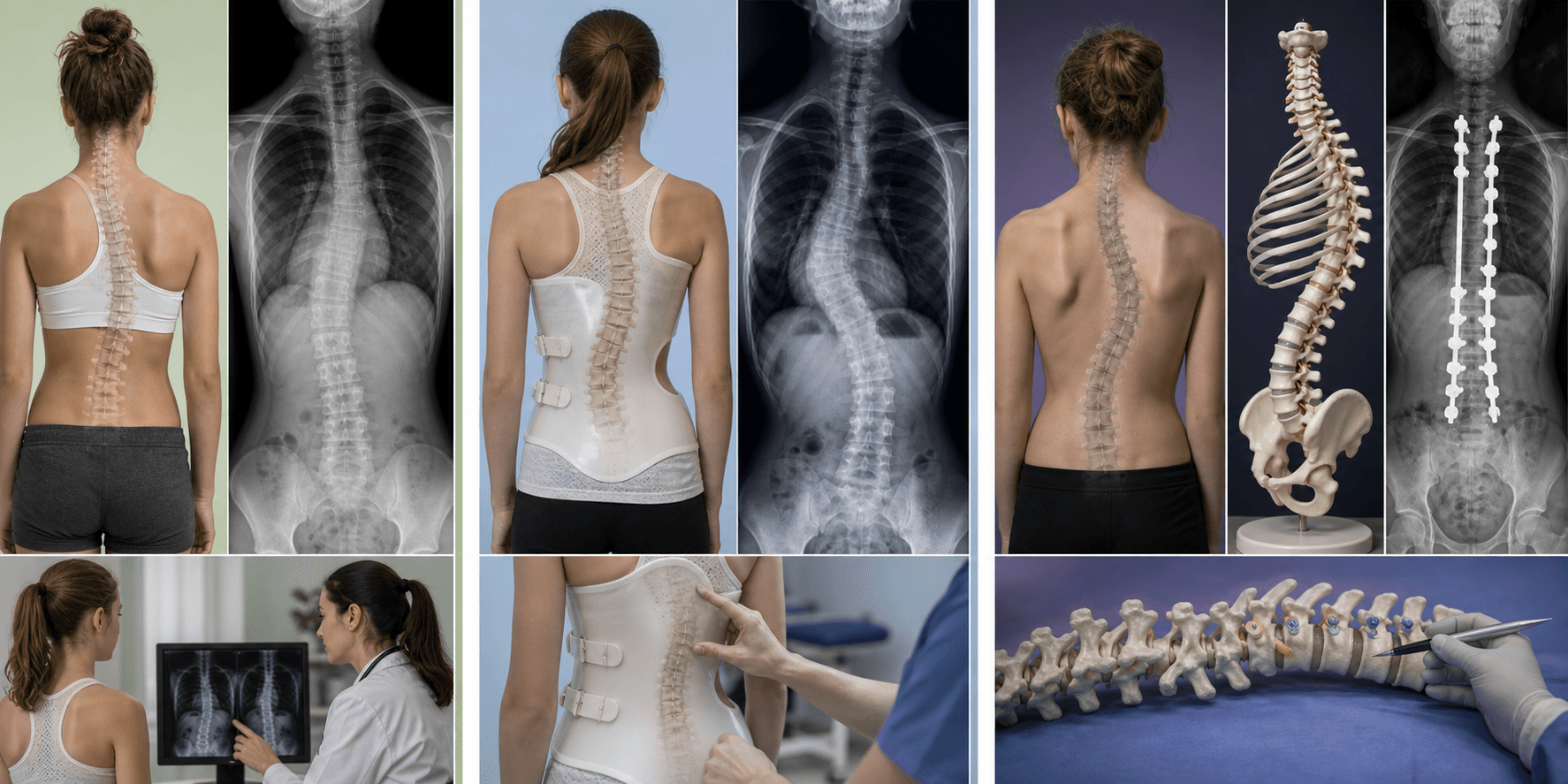
- “Main thoracic curves are RIGHT-sided (left = red flag for secondary cause)
- “Triradiate cartilage closure = Risser 0 but puberty started
- “Structural curves do NOT correct on side-bending radiographs
- “BrAIST study: bracing 72% vs observation 48% treatment success (curve staying under 50°)
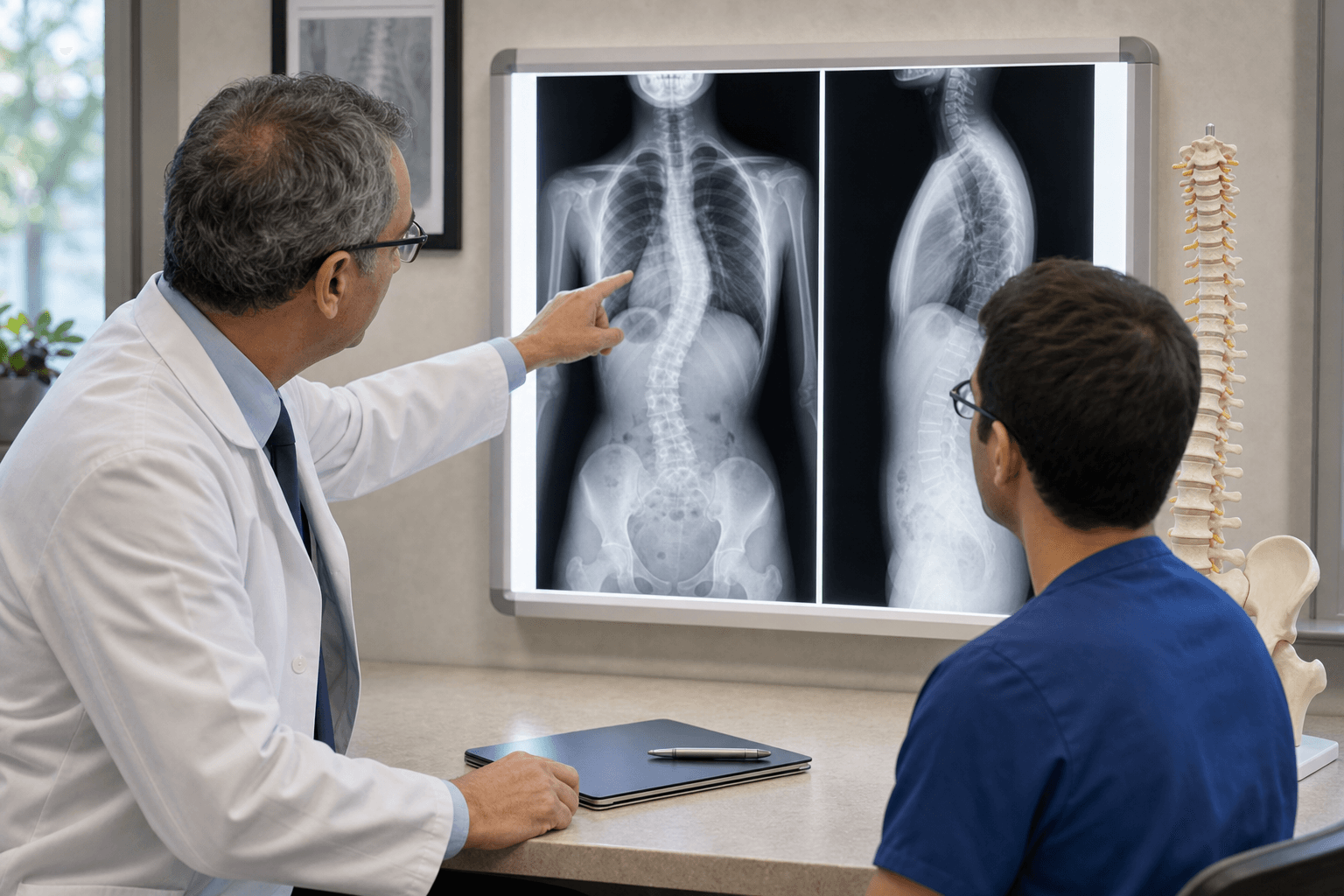
Clinical Imaging
Imaging Atlas




Never assume idiopathic if thoracic curve is left-sided. Investigate for: Syrinx, Chiari malformation, cord tumor, tethered cord. Order MRI spine before any surgery.
Triradiate cartilage closure (Y-cartilage of acetabulum) occurs around age 12-13. Risser sign measures iliac apophysis ossification (0-5). Both predict growth, but Risser is key for curve progression risk.
Structural curves: Do NOT correct to under 25° on side-bending films. Require fusion. Compensatory curves: Flexible, correct to under 25°. Should NOT be fused (leads to imbalance).
Goal: Fuse only structural curves, spare mobile segments. Lenke 1: Fuse only main thoracic (not compensatory lumbar). Key principle: Achieving spontaneous lumbar curve correction post-op.
| Cobb Angle | Risser Grade | Action | Rationale |
|---|---|---|---|
| Under 10° | Any | Observe - not scoliosis | Below diagnostic threshold |
| 10-25° | 0-2 (immature) | Observe every 4-6 months | Low risk progression |
| 25-40° | 0-2 (immature) | Brace 18+ hours/day | Prevent progression (BrAIST evidence) |
| 25-40° | 4-5 (mature) | Observe - no bracing | Growth complete, low progression risk |
| 40-45° | 0-2 (immature) | Intensive brace vs surgery | Borderline - discuss risks/benefits |
| Over 45-50° | Any | Surgery: PSF + instrumentation | Established surgical threshold |
MD TTLLLenke Classification (6 Curve Types)
Hook:'Medical Doctors Tackle Two Lumbar Lordoses' - remember the 6 Lenke curve patterns for surgical planning
RISSERRisser Sign Stages (0-5)
Hook:'Risser Sign Stages Show Expected Remaining growth' - critical for predicting curve progression risk
LAMP POSTRed Flags for Non-Idiopathic Scoliosis
Hook:'Light A Medical Post' - always check for these red flags before diagnosing idiopathic scoliosis
BRACEBracing Success Factors (SRS Criteria)
Hook:'Brace Really Achieves Curve Effectiveness' - remember BrAIST study showed 72% success vs 48% observation
Overview and Epidemiology
Definition
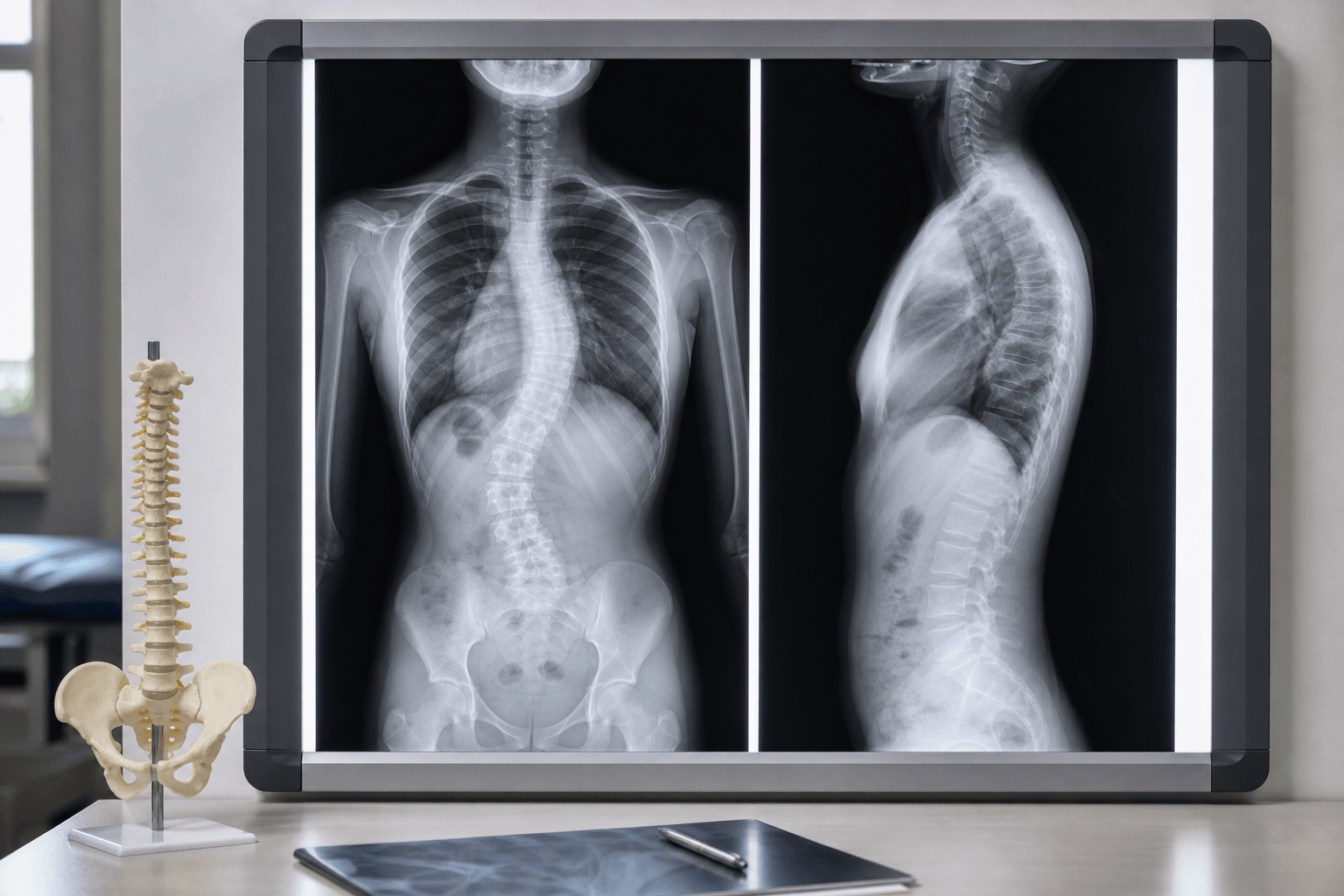
Adolescent Idiopathic Scoliosis (AIS) is a three-dimensional spinal deformity characterized by:
- Lateral curvature of the spine (Cobb angle 10° or greater)
- Vertebral rotation toward the convexity of the curve
- Age of onset: 10 years to skeletal maturity (approximately 18 years)
- Idiopathic: No identifiable underlying cause (diagnosis of exclusion)

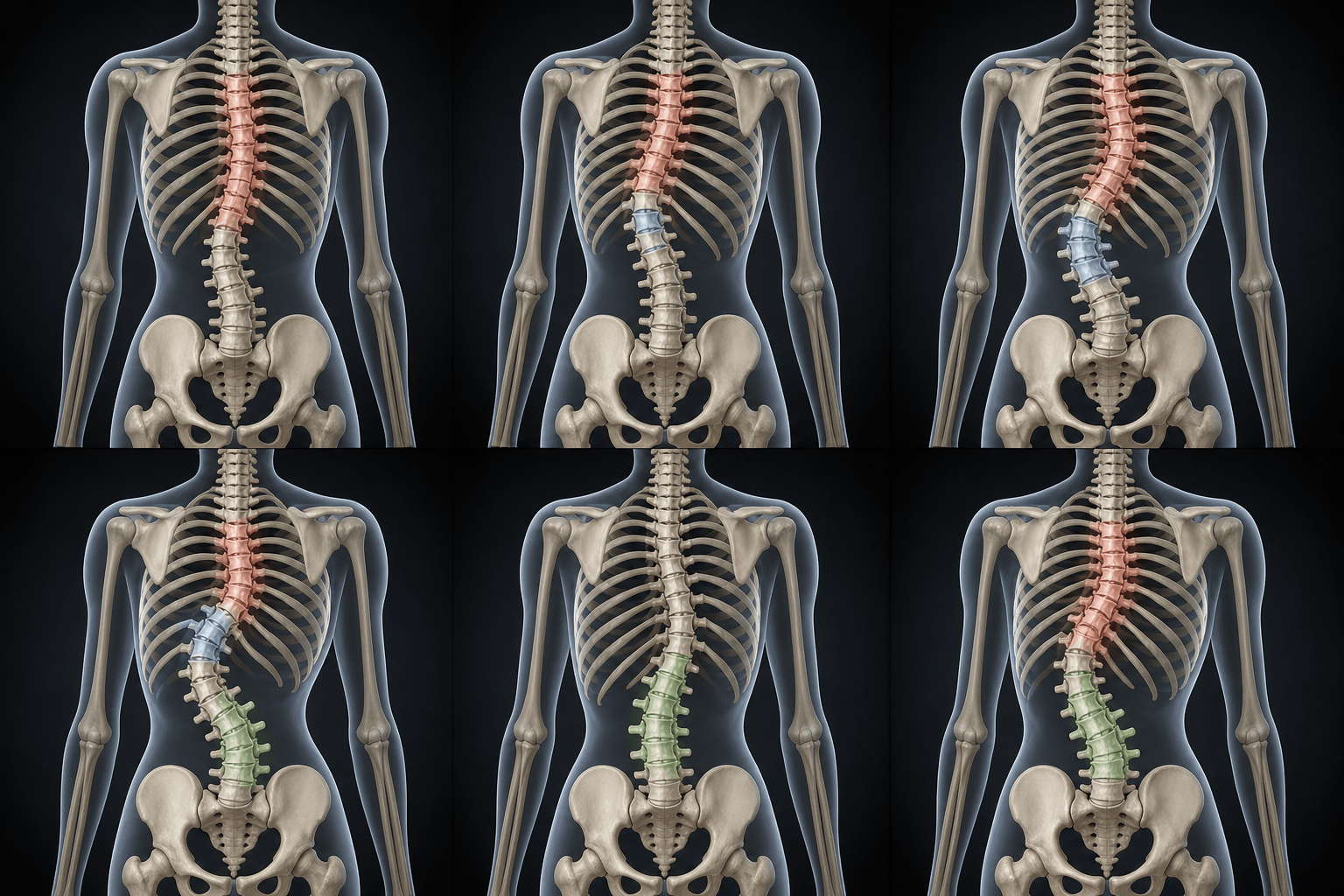
Not just coronal deformity: AIS involves complex 3D changes in coronal, sagittal, and axial planes.
Epidemiology
Prevalence
Key point: Small curves (10-20°) are common and equal between sexes. Larger curves requiring intervention are predominantly female.
Age Distribution
- Peak onset: Corresponds to peak growth velocity during puberty
- Girls: Age 10-12 (earlier than boys)
- Boys: Age 12-14
- Risk period: From onset of puberty to Risser 4-5 (skeletal maturity)
Geographic & Ethnic Variation
- Similar prevalence across ethnic groups for small curves
- Caucasian females have higher prevalence of progressive curves requiring treatment
- No significant urban/rural difference
- Global consistency: Reported prevalence (2-3% of adolescents) is broadly similar across world regions; apparent differences mostly reflect screening method and Cobb threshold
Natural History
Curve Progression Risk
Depends on:
- Skeletal maturity: Risser 0-2 (immature) = high risk
- Curve magnitude: Larger curves progress more
- Curve pattern: Double curves progress more than single
- Age/pubertal status: Premenarchal/early puberty = high risk
Weinstein 50-year follow-up (landmark natural history study):
- Curves under 30° at maturity: Remain stable lifelong (no progression)
- Curves 30-50° at maturity: May progress 10-15° over adulthood (usually asymptomatic)
- Curves over 50° at maturity: Progress approximately 1° per year throughout adulthood
- Curves over 80°: Risk of restrictive lung disease, dyspnea, reduced quality of life
Impact on Health
Curves under 70°: Minimal impact on respiratory function. Curves over 80-100°: Restrictive lung disease, reduced FVC, dyspnea on exertion. Death from cor pulmonale in severe untreated cases.
Mild-moderate curves: No increased back pain vs general population. Severe curves (over 70°): Increased prevalence of mechanical back pain in adulthood (muscle fatigue, imbalance).
Body image concerns: Primary driver for seeking treatment. Self-esteem: Negative impact with visible deformity (rib hump, shoulder asymmetry). SRS-30 scores: Self-image domain shows largest improvement post-treatment.
Curves under 100°: Normal life expectancy. Curves over 100° (rare, untreated): Increased mortality from cardiopulmonary complications. Justifies surgical intervention at 45-50° threshold.
Key message for exams: AIS is primarily a cosmetic and progressive deformity rather than immediately life-threatening. Surgery aims to halt progression and prevent long-term cardiopulmonary decline.
Pathophysiology and Mechanisms
Spinal Biomechanics in AIS
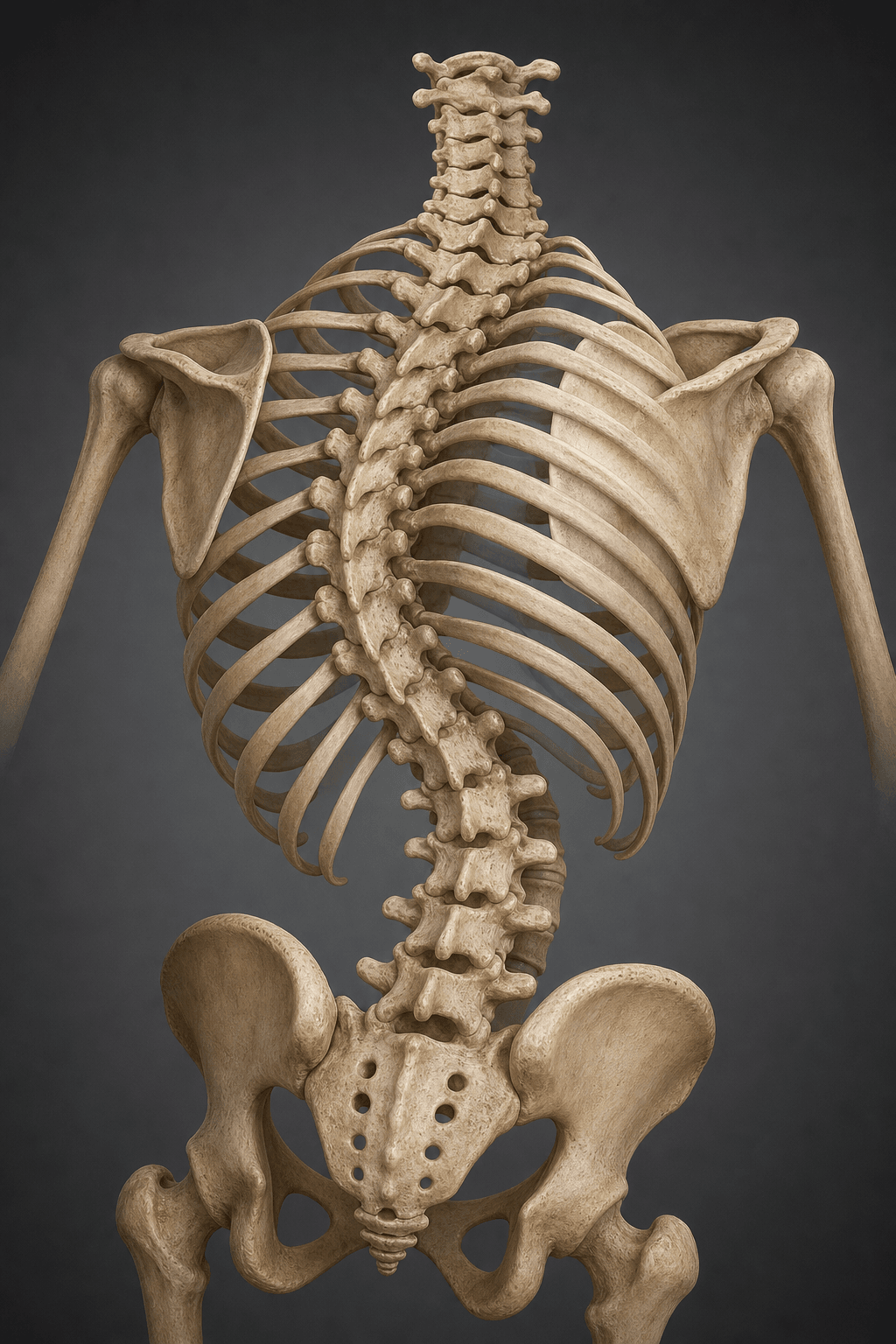
Three-Dimensional Deformity
AIS is NOT just coronal plane curvature. It is a complex 3D deformity:
- Coronal plane: Lateral curvature (Cobb angle measurement)
- Sagittal plane: Loss of normal thoracic kyphosis (hypokyphosis common)
- Axial plane: Vertebral rotation toward convexity of curve
Key concept: The rib hump seen on forward bend test is due to vertebral rotation, NOT just lateral curvature. Ribs follow rotated vertebrae, creating posterior prominence on convex side.
Hueter-Volkmann Principle
Asymmetric loading theory: Compression inhibits growth, tension stimulates growth.
- Concave side: Increased compression → slower growth
- Convex side: Relative tension → faster growth
- Result: Self-perpetuating vicious cycle during growth
Clinical implication: Curves under 30° may remain stable at skeletal maturity, but curves over 50° often progress 1° per year lifelong (even after growth completion).
Etiology: Why Idiopathic?
Idiopathic = unknown cause, but multiple factors implicated:
30% concordance in identical twins. CHD7, LBX1, GPR126 genes implicated. Family history increases risk 10-fold.
Relative anterior overgrowth theory. Hypokyphosis → increased anterior column loading → asymmetric progression.
Proprioceptive deficit theory. Subtle balance and postural control abnormalities in some patients.
Curve Progression Risk Factors
Sanders Skeletal Maturity System (alternative to Risser):
- Based on hand/wrist radiograph (distal radius, ulna physis)
- Stages 1-8: More granular than Risser for predicting growth
- Sanders 2-4 = peak growth velocity = highest curve progression risk
Classification Systems
Lenke Classification (Current Standard)
Purpose: Surgical planning - determines fusion levels.
Three Components:
- Curve type (1-6): Based on which curves are structural
- Lumbar spine modifier (A, B, C): Relationship of lumbar curve apex to CSVL
- Sagittal thoracic modifier (-, N, +): Thoracic kyphosis T5-T12
Determining Structural vs Non-Structural Curves
A curve is STRUCTURAL if it meets ANY of:
Cobb angle over 25° on standing AP radiograph (regardless of side-bending flexibility)
Fails to correct to under 25° on supine side-bending radiographs toward curve convexity
T5-T12 kyphosis under 20° (hypokyphotic) - renders thoracic curve structural even if small Cobb
CSVL-Lumbar Apex over 6mm (modifier C) - indicates lumbar curve must be addressed surgically
Lenke Type Descriptions:
| Type | Structural Curves | Typical Fusion Levels | Key Points |
|---|---|---|---|
| Type 1: Main Thoracic | MT only | T4/5 to T11/12/L1 | Most common, selective fusion, lumbar compensates |
| Type 2: Double Thoracic | PT + MT | T2-T12 | High left shoulder if PT not fused |
| Type 3: Double Major | MT + TL/L | T4-L3/4 | Both curves over 40°, largest curves |
| Type 4: Triple Major | PT + MT + TL/L | T1/2-L3/4 | Rare, all three regions structural |
| Type 5: TL/Lumbar | TL/L only | T10-L3 | Left-sided curves common |
| Type 6: TL-Main Thoracic | MT + TL/L | T3-L3 | Two structural curves, no lumbar compensation |
Key point: Type 1 (Main Thoracic) is the most common, accounting for 50-60% of surgical AIS cases.
Clinical Assessment
History: Key Questions
Usually asymptomatic, noticed by: Parent (clothing fit), school screening, physician checkup. Pain = red flag for non-idiopathic cause.
First-degree relative with scoliosis? 10x increased risk. Helps distinguish familial AIS from secondary causes.
Girls: Age at menarche (occurs Risser 1-2). Boys/Girls: Voice change, growth spurt, parental heights. Predicts remaining growth.
Pain, neurologic symptoms (weakness, numbness), bowel/bladder changes, night pain (tumor), rapid progression.
Physical Examination
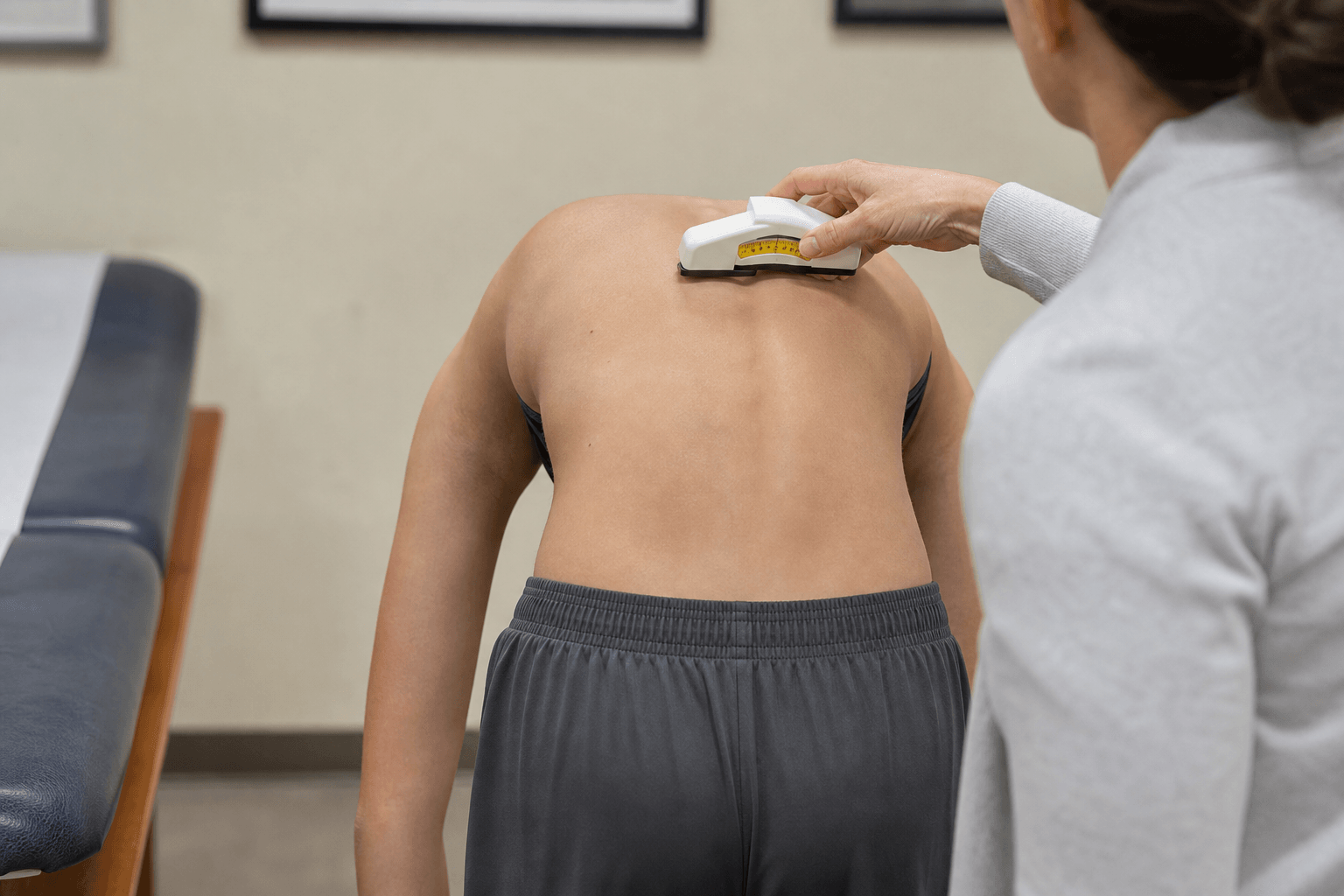
Adams Forward Bend Test
Gold standard screening test for scoliosis.
Technique:
- Patient stands with feet together, arms hanging freely
- Patient bends forward 90° at hips, knees straight
- Examiner views from behind, looks for asymmetry
Positive test: Rib hump or lumbar prominence on one side (indicates vertebral rotation).
Measurement: Use scoliometer (inclinometer) - angle of trunk rotation:
- 5-7° ATR (angle of trunk rotation): Refer for radiographs
- Over 7° ATR: High likelihood of Cobb angle over 20°
Shoulder Height Asymmetry
Left shoulder elevation suggests proximal thoracic curve (Lenke Type 2).
Key point: If Type 1 curve mistaken for Type 2, failure to fuse proximal thoracic leads to persistent shoulder asymmetry post-op.
Coronal Balance
Measure plumb line from C7 spinous process to sacral crease:
- Balanced: Plumb line within 2cm of sacral midline
- Decompensated: Over 2cm offset (poor surgical candidate without balance correction)
Sagittal Examination
Inspect for:
- Thoracic hypokyphosis (flat back) - common in AIS
- Lumbar hyperlordosis - compensatory mechanism
- Thoracic lordosis - severe cases, red flag
Neurologic Examination
Should be completely normal in AIS. Any abnormality = MRI spine mandatory.
Motor: 5/5 strength all myotomes. Sensory: Intact all dermatomes. Reflexes: 2+ symmetric, no clonus, negative Babinski. Abdominal reflexes: Symmetric (absent = cord pathology). Cavus feet: Inspect carefully (indicates neurologic disorder).
Skin Examination
- Café-au-lait spots (6+ spots over 5mm) = Neurofibromatosis-1
- Axillary freckling = NF-1 (Crowe's sign)
- Hairy patch, dimple over spine = Tethered cord, spinal dysraphism
- Port-wine stain = Consider vascular malformation
Differential Diagnosis
AIS is a diagnosis of exclusion. The following structural and non-structural causes of a spinal curve must be considered and confidently excluded before labelling a curve idiopathic.
| Diagnosis | Discriminating features | Key investigation |
|---|---|---|
| Adolescent idiopathic scoliosis | Right thoracic curve, painless, normal neurology, female predominance for larger curves, structural on bending | Standing PA/lateral + bending films |
| Congenital scoliosis | Sharp/short-segment curve, vertebral anomaly (hemivertebra, bar), may present younger | Plain films + CT for bony anatomy |
| Neuromuscular scoliosis | Long C-shaped curve, pelvic obliquity, abnormal tone/strength (CP, DMD, SMA) | Neurological exam + underlying-disease workup |
| Syringomyelia / Chiari / cord tumour | Left thoracic curve, abnormal abdominal reflexes, UMN signs, cavus feet | MRI whole spine + brain |
| Osteoid osteoma / osteoblastoma | Painful (classically night pain, NSAID-responsive), often painful/antalgic curve | CT (nidus); bone scan |
| Postural / non-structural scoliosis | Fully corrects on forward bend and on side-bending, no rib hump, no rotation | Examination; corrects on bending films |
| Leg-length discrepancy (compensatory) | Curve corrects when pelvis levelled (sitting or block under short leg), no true rotation | Standing block test; scanogram |
| Syndromic (Marfan, NF-1, connective tissue) | Dysmorphic/syndromic features, café-au-lait spots, joint laxity, tall stature | Genetics/clinical criteria; targeted imaging |
Investigations
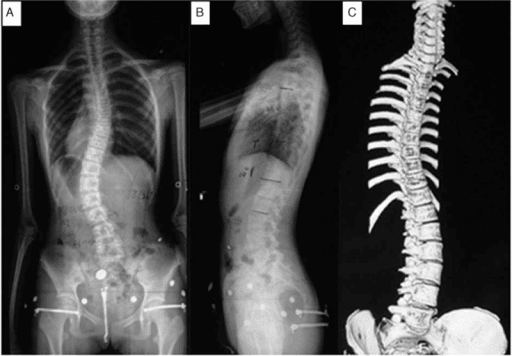
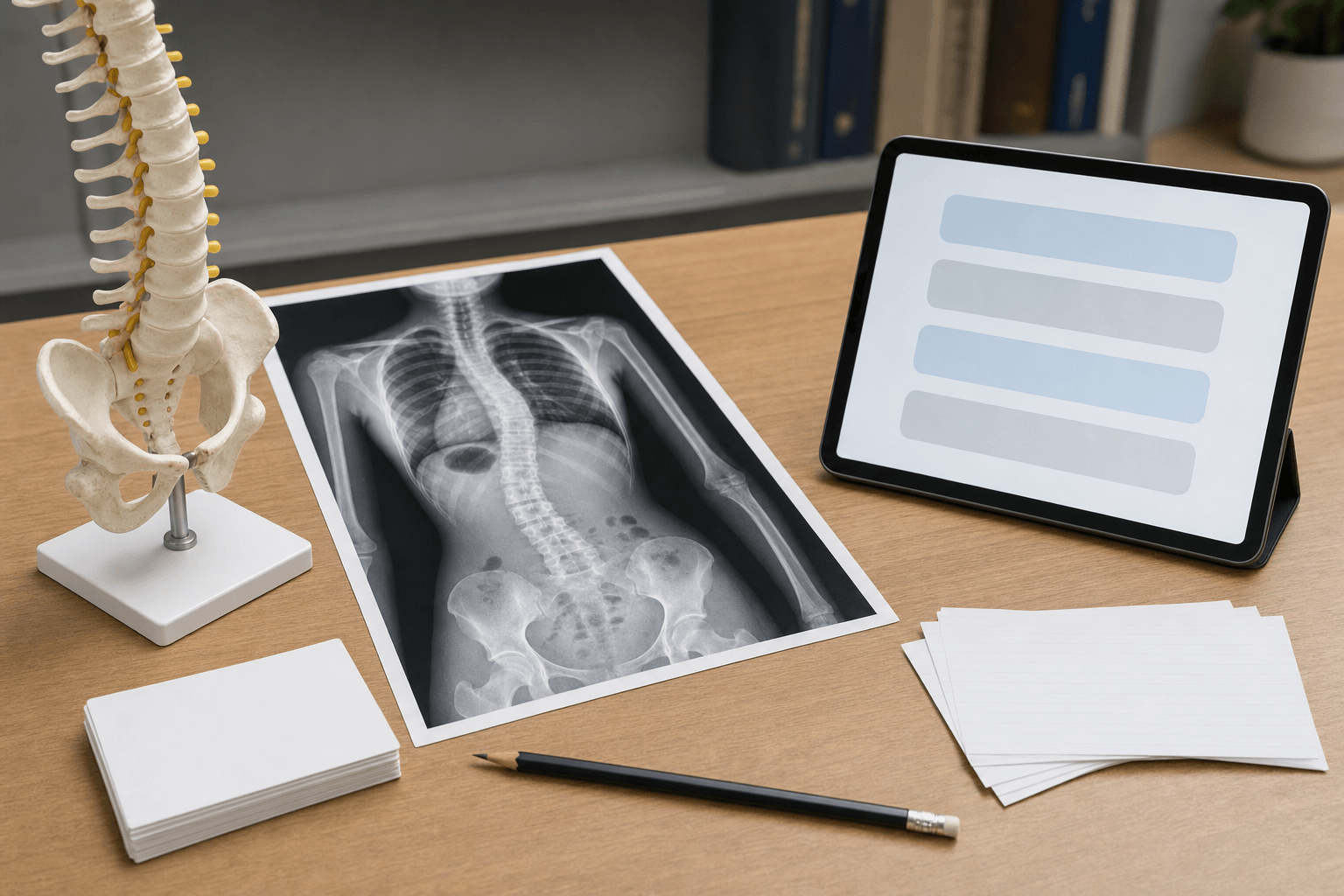
Radiographic Assessment
Initial Films
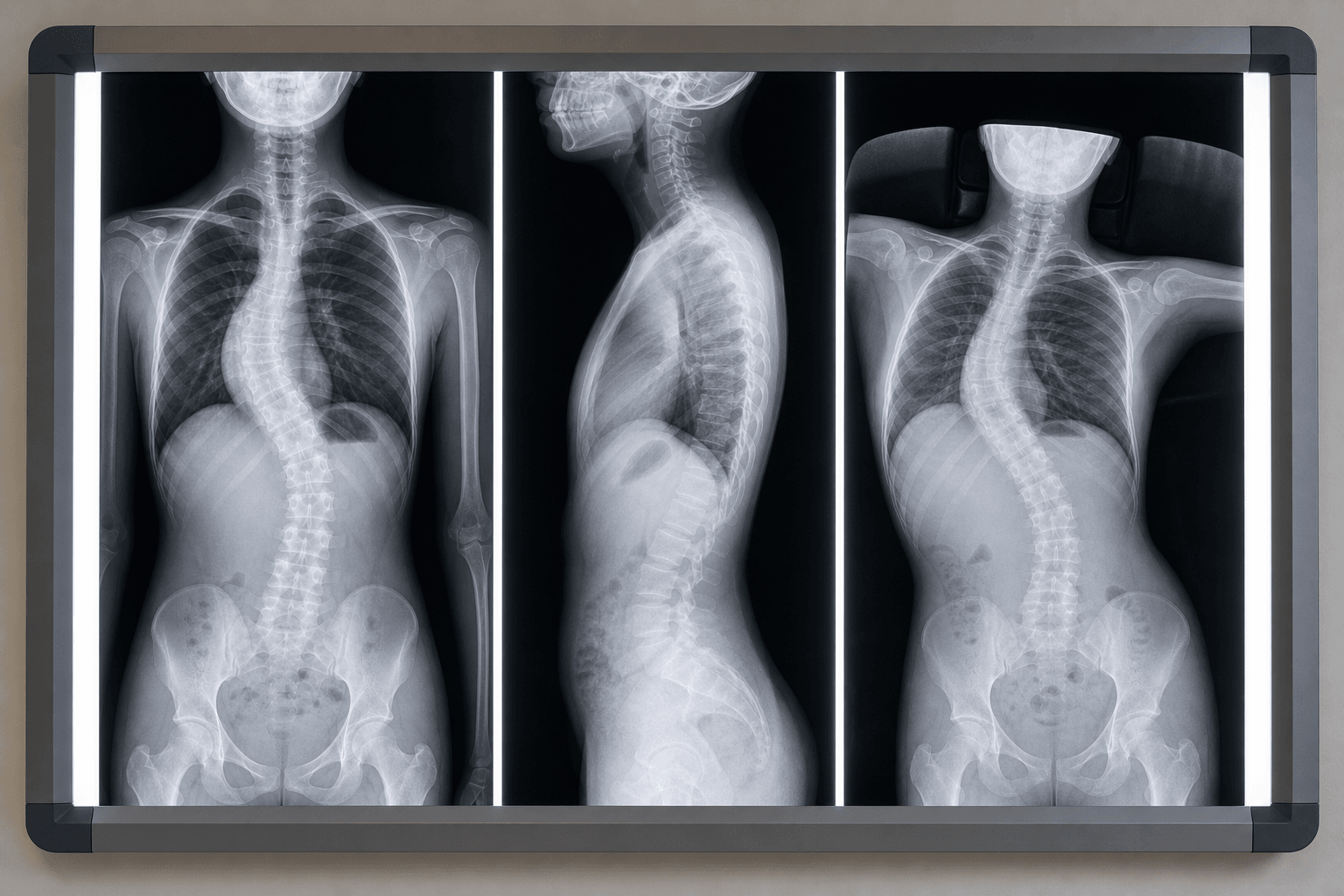
Standard views for diagnosis and monitoring:
-
PA Spine (NOT AP): Reduces radiation to breast tissue
- Include C7-sacrum on single 36-inch cassette
- Patient standing, arms forward on supports
- Measure Cobb angles, identify apex and end vertebrae
-
Lateral Spine: Assess sagittal profile
- Measure T5-T12 kyphosis (normal 20-40°)
- Assess lumbar lordosis (normal 40-60°)
- Identify thoracic lordosis (red flag)
When to order: Any patient with positive Adams test or scoliometer over 5-7°.
Cobb Angle Measurement
Step-by-step technique:
- Identify end vertebrae: Most tilted vertebrae at top and bottom of curve (maximally tilted into concavity)
- Draw lines: Line along superior endplate of upper end vertebra, inferior endplate of lower end vertebra
- Perpendiculars: Draw perpendicular lines from each endplate line
- Measure angle: Angle of intersection = Cobb angle
Interobserver variability: ± 5° between measurements (same observer or different observers).
Clinical significance:
- Under 10°: Not scoliosis (spinal asymmetry)
- 10-25°: Mild scoliosis, observe
- 25-40°: Moderate, consider bracing if immature
- Over 40-50°: Severe, surgical threshold
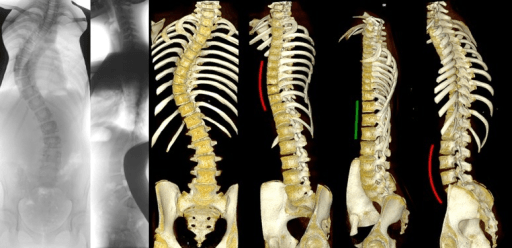
Specialized Imaging
| Imaging | Indication | Key Findings | Priority |
|---|---|---|---|
| MRI whole spine | Any red flag (left thoracic, pain, neuro signs) | Syrinx, Chiari, cord tumor, tethered cord | Mandatory before surgery |
| MRI brain | Chiari symptoms (headache, dysphagia) | Cerebellar tonsillar herniation over 5mm | If whole spine shows Chiari |
| CT spine | Congenital vertebral anomalies on XR | Hemivertebrae, bar, unsegmented bar | Pre-op planning if congenital |
| Hand/wrist XR | Sanders staging for growth prediction | Distal radius/ulna physis (Sanders 1-8) | Optional - Risser usually sufficient |
Key concept: MRI spine is mandatory before surgical correction if:
- Left thoracic curve
- Rapid progression
- Any neurologic signs/symptoms
- Male patient
- Painful scoliosis
- Age under 10 years
Prevalence of neural axis abnormalities: 5-10% of presumed AIS have MRI findings (syrinx most common).
Non-Operative Management
Observation Protocol
Indications for observation alone:
- Curves 10-25° in any patient
- Curves 25-40° in skeletally mature patients (Risser 4-5)
- Curves 25-40° in early immature patients where bracing compliance doubtful
Follow-Up Schedule
Every 4 months until skeletal maturity. Peak growth = peak risk. Obtain PA/lateral spine films each visit. Measure Cobb angles, document progression.
Every 6 months until Risser 4-5. Growth slowing. Continue PA/lateral films. If progression over 5° in 6 months, consider intervention.
Annual follow-up for 1-2 years, then discharge if stable. Curves under 30° unlikely to progress. Curves over 50° may progress 1° per year lifelong.
Progression definition: Increase in Cobb angle by over 5° between visits (accounting for measurement variability).
Bracing
BrAIST Study (2013) - Landmark Evidence
Key trial: Bracing in Adolescent Idiopathic Scoliosis Trial (BrAIST).
Design: Multicentre trial (randomised + preference cohorts), bracing vs observation, typical bracing indications (curves 20-40°, skeletal immaturity).
Results:
- 72% success with bracing vs 48% with observation in the combined analysis (success = curve staying under 50° / reaching maturity; propensity-adjusted OR 1.93)
- 75% vs 42% in the intention-to-treat randomised cohort (OR 4.11)
- Significant dose-response: more hours of brace wear correlated with greater success (P less than 0.001); brace prescribed for at least 18 hours/day
- Trial stopped early owing to the efficacy of bracing
Clinical impact: Bracing is now standard of care for appropriate candidates, and the benefit increases with longer daily wear time.
Bracing Indications (SRS Guidelines)
25-40° Cobb angle. Under 25° too small to justify treatment. Over 40° often requires surgery (bracing rarely prevents progression).
Risser 0-2 (significant growth remaining). Open triradiate cartilage or premenarchal. Bracing ineffective in mature patients.
Any curve type can be braced. Thoracic and thoracolumbar respond best. High thoracic and cervicothoracic difficult to control with standard TLSO.
Motivated patient and family. Realistic expectations. Psychological readiness for brace wear. Compliance monitoring essential.
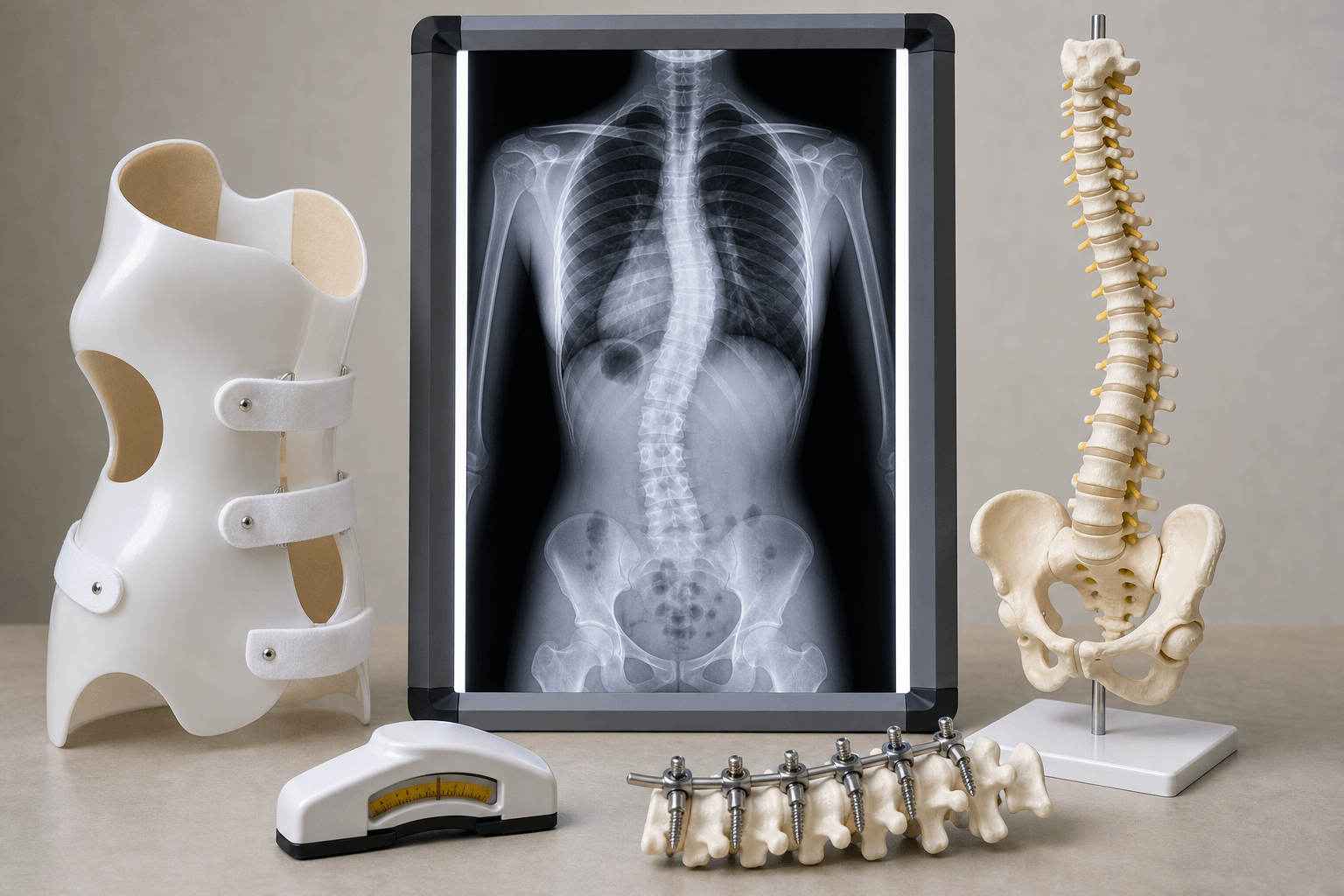
Brace Types
| Brace Type | Indications | Wear Time | Advantages/Disadvantages |
|---|---|---|---|
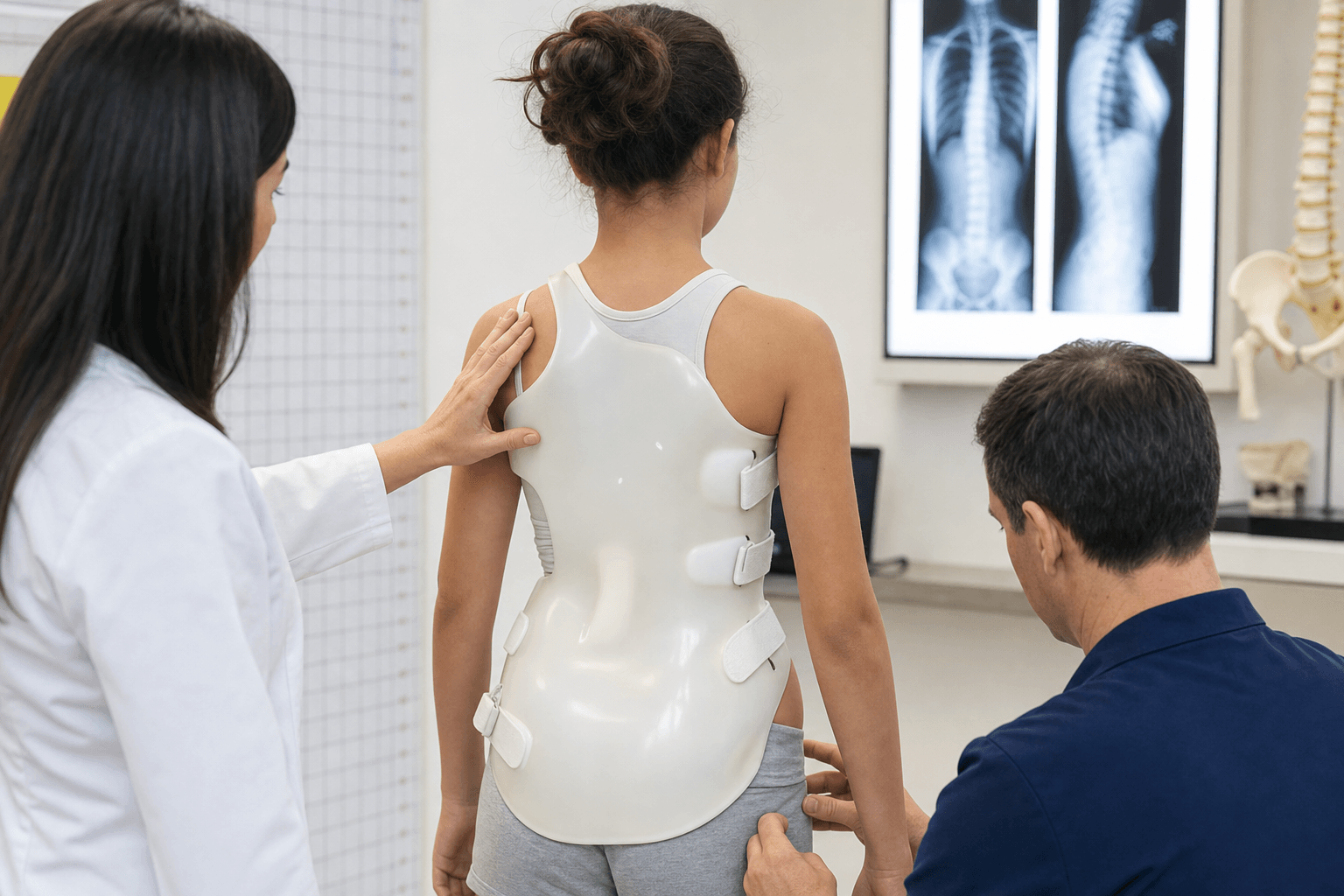
| TLSO (Boston) | Thoracic apex T8 or lower | 18-23 hours/day | Most common. Pressure pads at curve apex. Cannot address high thoracic curves. |
| Milwaukee CTLSO | High thoracic apex (T7 or higher) | 23 hours/day | Neck ring + TLSO. Poor cosmesis, compliance issues. Rarely used now. |
| Charleston bending brace | Thoracolumbar/lumbar curves | 8-10 hours (nighttime only) | Hypercorrects curve in lateral bending. Better compliance, similar outcomes. |
| Providence brace | Single thoracic or thoracolumbar | 8-10 hours (nighttime) | Custom-molded, nighttime wear. Improves compliance in adolescents. |
Principle of corrective bracing: Apply three-point pressure:
- Pressure at curve apex (convex side)
- Counter-pressure above curve (concave side)
- Counter-pressure below curve (concave side)
Goal: NOT to permanently correct curve, but to halt progression during growth.
Weaning Protocol
When to start: Skeletal maturity (Risser 4-5, 2+ years post-menarche).
Gradual weaning:
- Reduce to 16 hours/day for 3 months
- Reduce to 12 hours/day (nighttime only) for 3 months
- Discontinue brace, obtain PA/lateral films
- Follow-up at 6 months, 12 months post-weaning
Rebound phenomenon: Curve may increase 5-10° after brace discontinuation (acceptable if stays under 50°).
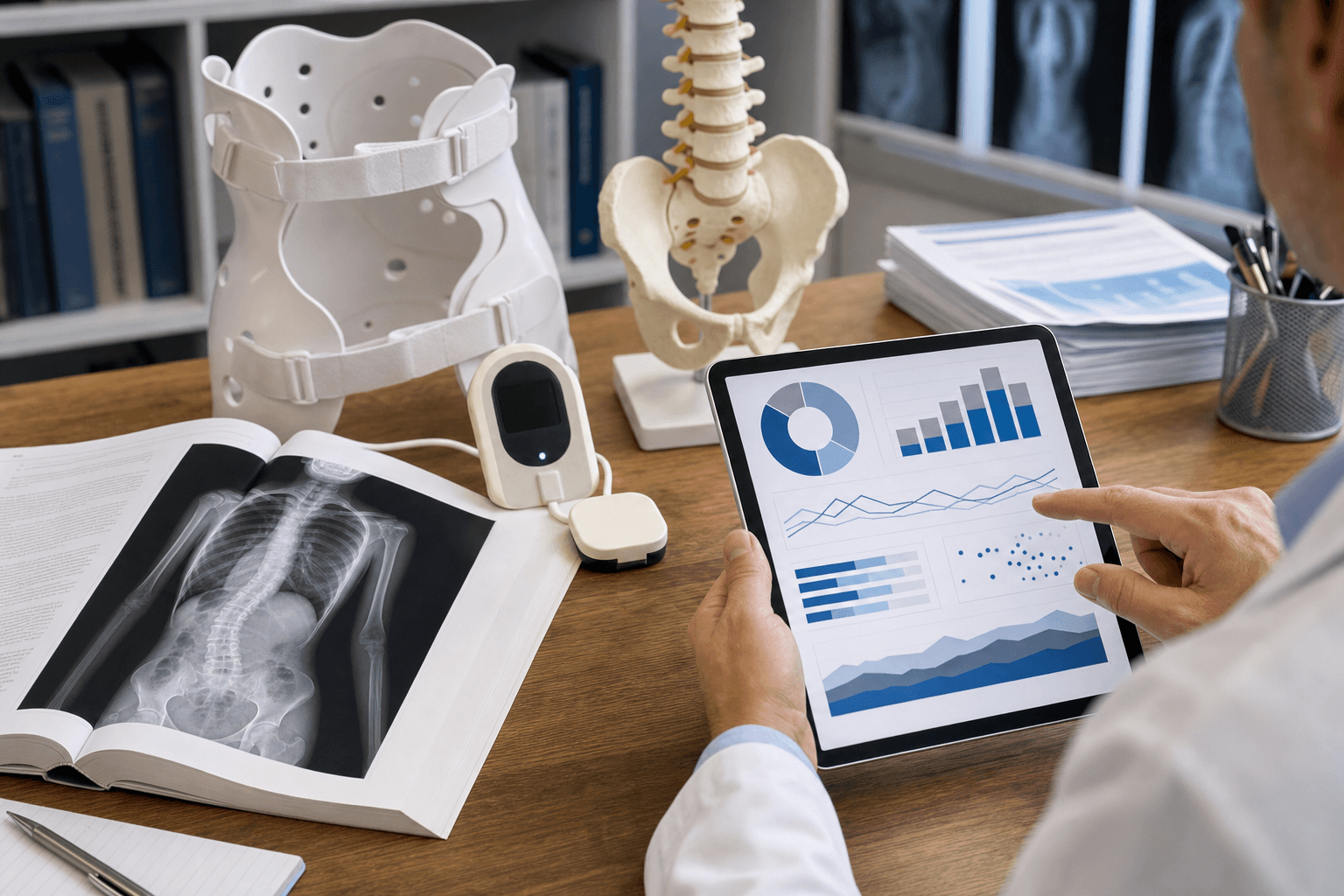
Monitoring Compliance
Challenge: Adolescent non-compliance is common (social stigma, discomfort).
Strategies:
- Temperature sensors in brace - logs hours worn
- Frequent follow-up - every 4-6 months with radiographs
- Peer support groups - connect patients with others in braces
- Positive reinforcement - emphasize success stories, avoiding surgery
Management Algorithm
Comprehensive Treatment Decision Tree
The management of AIS follows a systematic algorithm based on curve magnitude and skeletal maturity:
Step 1: Confirm Diagnosis
Adams forward bend test + scoliometer over 5-7° ATR → Order standing PA/lateral spine radiographs
Under 10° = not scoliosis (observe). Over 10° = scoliosis diagnosis confirmed (proceed to Step 2)
Step 2: Rule Out Secondary Causes (Red Flag Assessment)
Before assuming idiopathic, exclude: Left thoracic curve (syrinx/Chiari), Pain (tumor), Neurologic signs (cord pathology), Male sex (higher suspicion), Age under 10 (congenital/neuromuscular). Order MRI spine if ANY red flags present.
Key point: Always rule out secondary causes before proceeding with treatment.
Surgical Technique
Surgical Indications
Primary indication: Cobb angle 45-50° or greater. Curves over 50° progress lifelong (1° per year). Surgery prevents cardiopulmonary compromise.
Curve progressing over 5-10° despite bracing (in immature patient). Indicates bracing failure, surgery needed to prevent worsening.
Patient-reported concern about appearance. Rib hump, waistline asymmetry, shoulder imbalance. Quality of life indication (SRS-30 scores).
Atypical in AIS - investigate other causes. Back pain in large curves (over 70°) can be surgical indication in adult patients.
Absolute threshold: No universally agreed cutoff. 45-50° is consensus surgical threshold.
Relative indications:
- 40-45° in immature patient with rapid progression
- Over 50° regardless of symptoms (prevent respiratory decline)
- Over 70-80° = cardiopulmonary compromise risk
Goals of Surgery
- Halt progression: Spinal arthrodesis prevents further curvature
- Correct deformity: Reduce Cobb angle 50-70% (not 100% - risks neurologic injury)
- Maintain balance: Coronal and sagittal balance essential
- Preserve motion: Fuse only structural curves, spare compensatory segments
- Improve cosmesis: Reduce rib hump, shoulder asymmetry

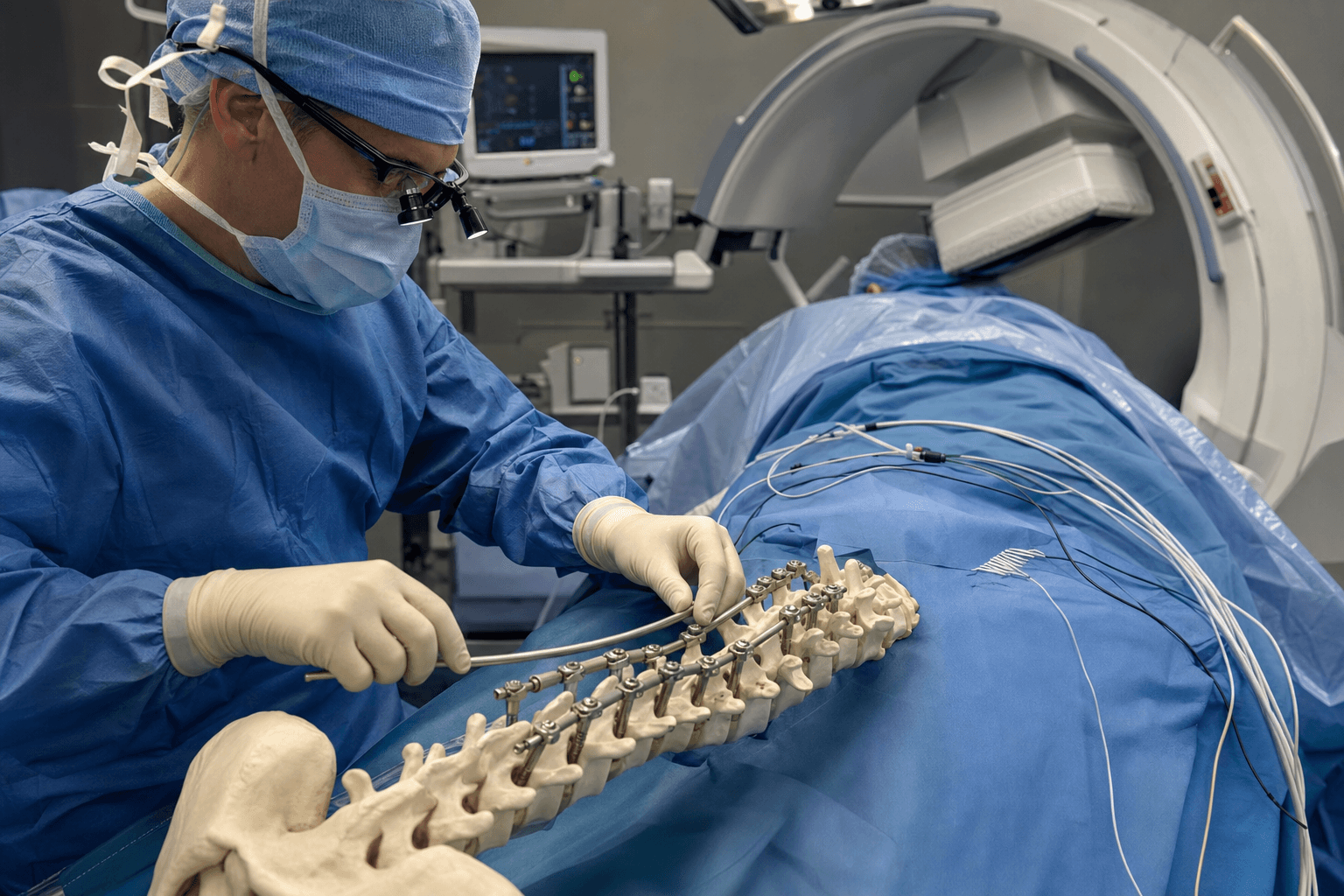
Posterior Spinal Fusion (PSF) - Standard Approach
Most common surgical technique for AIS.
Pre-Operative Planning
Key decisions:
- Proximal fusion level: Guided by Lenke classification
- Stable vertebra (SV) = first vertebra bisected by CSVL
- Neutral vertebra (NV) = least rotated, most parallel endplates
- Distal fusion level: Critical to avoid coronal imbalance
- Generally to neutral/stable vertebra or one level distal
- Lumbar modifier C (CSVL beyond apex) requires fusion into lumbar spine
Proximal level: Fuse to upper end vertebra or one level above if needed for shoulder balance. Distal level: Fuse to lower end vertebra, stable vertebra, or neutral vertebra (whichever is most distal). Key rule: Better to over-fuse proximally than distally (preserving lumbar motion is priority).
Surgical Technique
Positioning:
- Prone on Jackson table or radiolucent spinal frame
- Chest rolls under shoulders, iliac crests (avoid abdomen compression)
- Arms abducted 90° on arm boards
- All pressure points padded
- Neutral spine position (avoid extreme flexion/extension)
Neuromonitoring:
- SSEP (somatosensory evoked potentials) - monitors dorsal columns
- MEP (motor evoked potentials) - monitors corticospinal tracts
- EMG (electromyography) - monitors nerve root irritation
- Stagnara wake-up test if neuromonitoring unavailable
Incision:
- Midline posterior incision from 2 levels above to 2 levels below planned fusion
- Subperiosteal dissection to expose spinous processes, laminae, transverse processes
- Expose out to tips of transverse processes for screw placement
This systematic exposure provides optimal access for safe pedicle screw placement while preserving the biomechanics of the posterior spinal elements.
Intra-Operative Neuromonitoring
SSEP (Somatosensory Evoked Potentials):
- Monitors dorsal column function (position/vibration sense)
- Stimulate peripheral nerve (tibial, median), record at scalp
- Alarm criteria: 50% amplitude decrease OR 10% latency increase
MEP (Motor Evoked Potentials):
- Monitors corticospinal tract function (motor)
- Stimulate motor cortex (transcranial), record at muscle (foot, hand)
- More sensitive than SSEP for detecting motor injury
- Alarm criteria: 50-80% amplitude decrease
Management of alarm:
- Stop surgical maneuver immediately
- Check anesthesia: MAP over 70, Hgb over 8, temp normal
- If no improvement, release correction (loosen rods/screws)
- If signals recover, attempt correction more gradually
- If signals do not recover, perform Stagnara wake-up test
Stagnara wake-up test (historical, rarely needed now):
- Lighten anesthesia mid-case
- Patient wakes, squeezes hands, moves feet on command
- Confirms motor function intact despite neuromonitoring alarm
Anterior Spinal Fusion (ASF)
Less commonly used since advent of pedicle screw posterior instrumentation.
Indications (limited):
- Thoracolumbar/lumbar curves (T12-L4) where anterior release improves flexibility
- Lenke 5 curves with severe rigidity on side-bending films
- Selective anterior fusion to spare fusion levels (controversial)
Approach:
- Open thoracotomy or thoracoabdominal incision (invasive, painful)
- Video-assisted thoracoscopic surgery (VATS) - less invasive option
Disadvantages:
- More painful post-op (vs posterior approach)
- Risk of pulmonary complications
- Does not address sagittal hypokyphosis as well as posterior DVR
- Generally replaced by posterior-only techniques
Current role: Anterior release followed by posterior instrumentation (two-stage) for severe rigid curves over 80-90°.

Minimally Invasive Techniques
Emerging approaches:
- Anterior scoliosis correction (ASC): Vertebral body tethering (VBT)
- ApiFix device: Gradual correction via ratcheting implant
- Magnetically controlled growing rods (MCGR): For EOS, not AIS
Vertebral Body Tethering (VBT):
- Concept: Modulate growth via Hueter-Volkmann principle
- Thoracoscopic placement of flexible tether on convex side
- Restricts convex growth, allows concave "catch-up"
- Indication: Curves 40-65°, skeletally immature (Risser 0-2)
- Advantages: Preserves motion, no fusion, less invasive
- Disadvantages: Tether breakage (10-15%), over-correction, long-term data lacking
Status: Investigational in many countries, not yet standard of care for AIS.
Complications
Intra-Operative Complications
Incidence: Under 1% with neuromonitoring. Causes: Pedicle screw malposition, over-distraction, hypotension, cord ischemia. Prevention: SSEP/MEP, wake-up test, gradual correction.
Incidence: 5-10%. Cause: Dissection around lamina/facets. Management: Primary repair with 4-0 suture, fibrin glue, subfascial drain. Risk: CSF leak, pseudomeningocele.
Average: 800-1200mL for PSF. Risk factors: Large curves, long fusions, revision surgery. Prevention: Controlled hypotension, antifibrinolytics (TXA), cell saver, pre-op autologous donation.
Rare (under 0.1%). Mechanism: Anterior vertebral body perforation (pedicle screw or anterior instrumentation). Major vessels at risk: Aorta, IVC, segmental vessels. Life-threatening emergency.
Early Post-Operative Complications
| Complication | Incidence | Presentation | Management |
|---|---|---|---|
| Infection (superficial) | 1-2% | Wound drainage, erythema, fever | I&D, antibiotics, usually spares hardware |
| Infection (deep) | 0.5-1% | Fever, elevated CRP/ESR, MRI enhancement | I&D, long-term IV antibiotics, may require hardware removal |
| Implant failure | Under 1% | Acute pain, loss of correction on XR | Revision surgery if symptomatic/progressive |
| Pneumothorax | 1-2% | Dyspnea, decreased breath sounds | Chest XR, chest tube if large (over 20%) |
| Ileus | 5-10% | Nausea, vomiting, abdominal distension | NPO, NGT, correct electrolytes, usually resolves 3-5 days |
Superior mesenteric artery (SMA) syndrome:
- Cause: Acute lordotic positioning on Jackson table → compression of duodenum between SMA and aorta
- Presentation: Intractable vomiting POD 3-7, inability to tolerate PO
- Diagnosis: Upper GI series shows duodenal compression/obstruction
- Treatment: NGT decompression, TPN, prone positioning (relieves duodenal compression), usually resolves 1-2 weeks
Late Post-Operative Complications
Pseudarthrosis
Definition: Non-union of intended fusion mass.
Incidence: 1-2% with modern pedicle screw instrumentation (higher with hooks/wires).
Risk factors:
- Smoking (rare in adolescents)
- Long fusion constructs (over 12 levels)
- Inadequate decortication
- Infection
- Poor nutrition
Presentation:
- Often asymptomatic
- Back pain at fusion site
- Progressive loss of correction
- Implant failure (rod fracture)
Diagnosis:
- CT scan with fine cuts through fusion mass
- Dynamic XR (flexion/extension) - motion at pseudarthrosis site
- Rod fracture on plain films (implies pseudarthrosis)
Management:
- Asymptomatic pseudarthrosis - observe if well-balanced, no progression
- Symptomatic pseudarthrosis - revision fusion (posterior ± anterior), bone graft, possible re-instrumentation
Proximal Junctional Kyphosis (PJK)
Definition: Kyphosis over 10° at junction between fused and mobile segments (within 2 levels of UIV).
Incidence: 20-30% after PSF for AIS (most cases mild, asymptomatic).
Mechanism:
- Stress riser at proximal end of construct
- Ligamentous injury during dissection
- Over-correction of main curve creating compensatory kyphosis
- Osteoporotic vertebra fracture (more common in adults)
Presentation:
- Cosmetic concern (visible kyphosis at base of neck/upper back)
- Neck pain (if severe)
- Rarely neurologic compromise
Management:
- Mild PJK (under 20°) - observe, usually stable
- Severe PJK (over 30°) or progressive - revision with proximal extension of fusion
Prevention:
- Avoid over-distraction of proximal screws
- Gradual transition from corrected to uncorrected spine (avoid sharp angle)
- Consider tethering proximal screws (semi-rigid connection)
Adding-On Phenomenon
Definition: Progression of compensatory curve distal to fusion into structural curve.
Cause: Under-fusion - distal fusion level selected too proximal, leaving unstable curve below.
Most common in: Lenke 1 curves where lumbar modifier underestimated (should have been modifier C, fused into lumbar spine).
Presentation:
- Progressive coronal imbalance
- Shoulder asymmetry
- Back pain
Management:
- Distal extension of fusion to include adding-on levels
- Rarely, proximal extension if shoulder imbalance
Prevention:
- Careful pre-op assessment of lumbar modifier
- Fuse to neutral/stable vertebra (not one level proximal)
- Consider lumbar fusion if modifier B/C
Crankshaft Phenomenon
Definition: Continued anterior spinal growth after posterior-only fusion in very immature patients.
Mechanism:
- Anterior vertebral bodies (growth plates) continue growing
- Posterior fusion mass acts as tether
- Results in progressive deformity despite solid posterior fusion
Risk factors:
- Open triradiate cartilage at time of surgery
- Risser 0 patients
- Pre-pubertal patients (under age 10)
Rare in AIS (more common in early-onset scoliosis).
Prevention:
- Delay surgery until triradiate closure if possible
- Consider anterior fusion if surgery required in very immature patient
- Modern high-density pedicle screw constructs may resist crankshaft (debated)
Postoperative Care

Immediate Post-Operative Period (POD 0-3)
ICU/HDU Monitoring (First 24 Hours)
Standard protocol:
- Neuromonitoring: Continue SSEP/MEP for first 2-4 hours post-op (detect delayed neurologic changes)
- Neurologic checks: Hourly motor/sensory assessment (5/5 strength all extremities)
- Pain control: Multimodal analgesia (IV opioids, ketorolac, paracetamol)
- Hemodynamic monitoring: Goal MAP over 70 mmHg (maintain spinal cord perfusion)
- Log-roll only: No independent bed mobility for first 24 hours
Ward Care (POD 1-3)
Day 1: Sit at edge of bed with PT/OT assistance. Assess orthostatic tolerance.
Day 2: Stand and ambulate 5-10 meters. No bending, lifting, twisting (BLT precautions).
Day 3: Ambulate to bathroom independently. Stairs practice with PT if needed for home discharge.
Goal: Independent ambulation by POD 3-4. Modern pedicle screw constructs allow early mobility without post-op bracing.
Hospital Discharge (POD 4-6)
Discharge criteria:
- ✓ Adequate pain control on oral medications
- ✓ Independent ambulation (no assistive device needed)
- ✓ Tolerating regular diet
- ✓ Bowel function restored
- ✓ Neurologic exam normal (5/5 strength, intact sensation)
- ✓ Wound clean/dry/intact, no signs of infection
- ✓ Patient/family educated on home precautions
Discharge medications:
- Oral opioids (oxycodone 5mg PRN, 1-2 week supply)
- Paracetamol 1g QID
- Bowel regimen (docusate, senna)
- ± Gabapentin if neuropathic pain
Activity restrictions:
- No BLT (bending, lifting over 5kg, twisting) for 6 weeks
- No contact sports for 6 months (until fusion solid)
- Return to school at 2-3 weeks (light activities, no PE)
- Swimming allowed at 6 weeks (wound fully healed)
Outpatient Follow-Up Schedule
Wound check - Remove surgical clips/staples. Assess healing. No radiographs needed. Address any concerns (pain, mobility, psychosocial adjustment).
First XR assessment - Standing PA/lateral spine films. Measure Cobb angles, assess hardware position, evaluate coronal/sagittal balance. Clear for return to light activities (no contact sports yet).
Clinical + XR - Assess fusion progression (bridging bone visible), hardware integrity. Clear for most activities including non-contact sports. Continued BLT precautions until 6 months.
Clinical + XR - Confirm solid fusion (bridging bone bilaterally). Clear for ALL activities including contact sports. Discharge to annual follow-up.
Annual XR - Monitor for late complications (PJK, adding-on, hardware failure). Continue until skeletal maturity (Risser 5) + 2 years. Then discharge.
Red Flags for Early Return
Neurologic changes: New weakness, numbness, bowel/bladder dysfunction (rare but emergent). Wound concerns: Drainage, erythema, dehiscence, fever (infection). Severe pain: Uncontrolled despite medications (hardware failure, hematoma). Intractable vomiting: POD 3-7 (SMA syndrome). Shortness of breath: Pneumothorax, pulmonary embolism (rare).
Long-Term Monitoring
Years 1-5:
- Annual clinical + radiographic follow-up
- Monitor for PJK, adding-on, hardware failure
- SRS-30 outcomes questionnaire (assess QOL, self-image, pain)
After skeletal maturity + solid fusion:
- Discharge from routine follow-up
- PRN follow-up if develops pain or concerns
- Counsel: Curves should remain stable lifelong after solid fusion
Pregnancy counseling (for female patients):
- AIS surgery does NOT contraindicate pregnancy
- Spinal fusion does NOT affect ability to deliver vaginally
- Epidural anesthesia usually possible (inform anesthetist of fusion levels)
- Discuss at skeletal maturity/pre-pregnancy planning
Outcomes and Prognosis

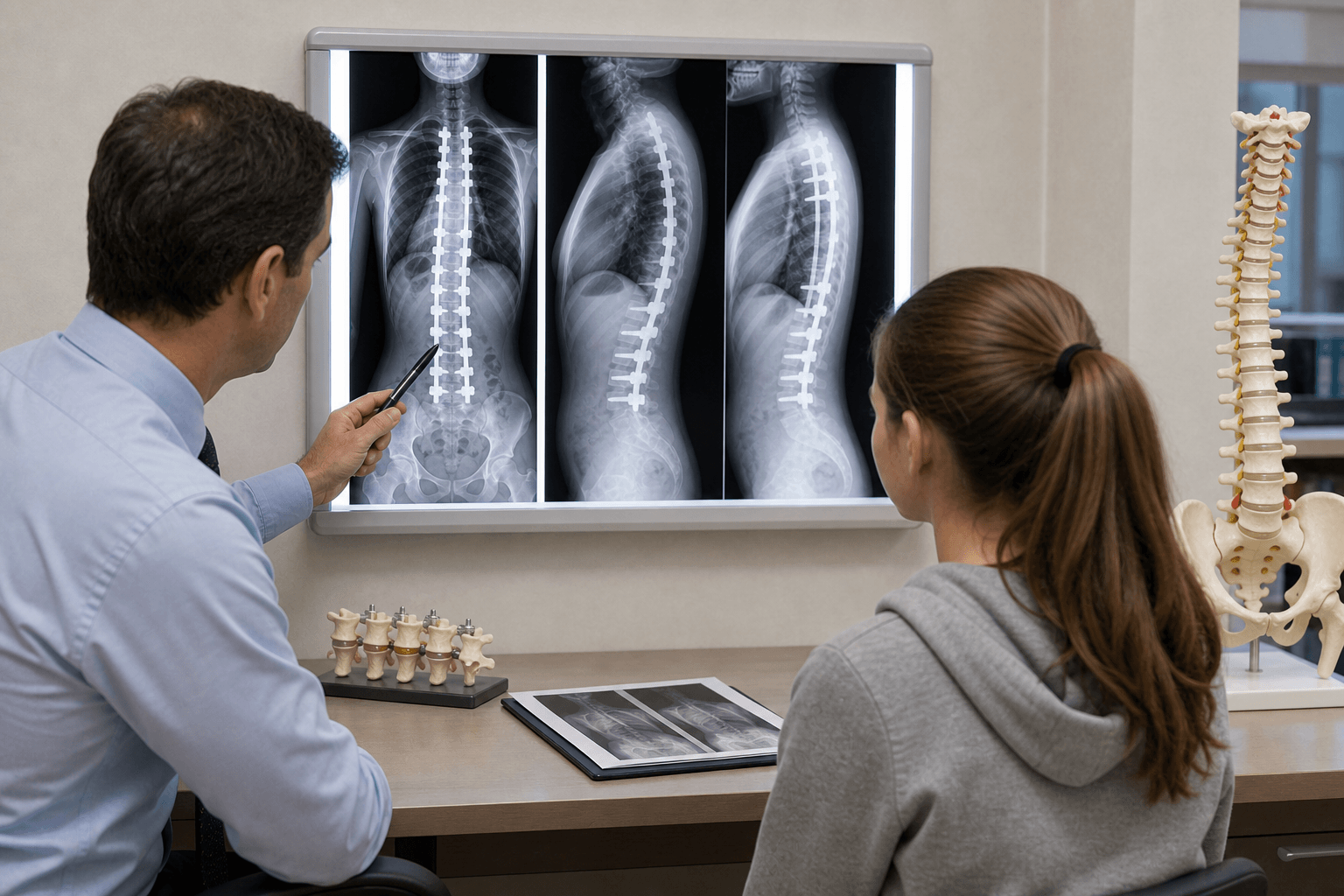
Radiographic Outcomes
Curve Correction
Key point: Goal is NOT 100% correction (risks neurologic injury). 50-70% correction with balanced spine = excellent outcome.
Sagittal Profile Restoration
Modern DVR technique (direct vertebral rotation):
- Restores physiologic thoracic kyphosis (20-40°)
- Avoids flat back syndrome (complication of older hook systems)
- Maintains lumbar lordosis (40-60°)
Sagittal balance more important than coronal correction for long-term patient satisfaction.
Patient-Reported Outcomes
SRS-30 Questionnaire
Five domains (score 1-5, higher = better):
- Pain: Minimal change (AIS rarely painful pre-op)
- Self-image: Largest improvement (major driver of satisfaction)
- Function: Returns to baseline by 6-12 months
- Mental health: Improves post-op (body image confidence)
- Satisfaction: Over 90% satisfied at 2+ years post-op
Key finding: Self-image improvement is primary benefit of surgery (not pain relief, which was minimal pre-op).
Return to Activities
| Activity | Timeframe | Restrictions | Evidence |
|---|---|---|---|
| School (academic only) | 2-3 weeks | No PE, no heavy backpack | Safe, promotes psychosocial recovery |
| Light exercise (walking, stationary bike) | 6 weeks | No BLT, no impact | Cardiovascular maintenance |
| Non-contact sports (swimming, running) | 3-4 months | Avoid contact, collision | Most patients resume by 4 months |
| Contact sports (football, rugby) | 6-12 months | After fusion solid on XR | Risk of hardware failure if premature |
| Full unrestricted activity | 12 months | No restrictions | Fusion solid, hardware incorporated |
Practical note: Return-to-sport clearance commonly requires written approval from the treating surgeon (for school/club liability) in many health systems.
Long-Term Health Outcomes
Cardiopulmonary Function
Post-surgical curves:
- Curves corrected to under 50° = normal pulmonary function lifelong
- No increased mortality vs general population
- Justifies surgical intervention at 45-50° threshold (prevents progression to over 80°)
Back Pain
SRS adult outcomes data:
- Treated AIS (surgery or brace): Similar back pain prevalence to general population at 20-30 year follow-up
- Untreated AIS over 70°: Increased mechanical back pain (muscle fatigue, imbalance)
- Fusion does NOT cause increased back pain if balanced
Adjacent Segment Degeneration
Concern: Fusion increases stress on adjacent mobile segments.
Evidence:
- Mild degenerative changes on MRI in 30-40% at 10+ years (asymptomatic)
- Symptomatic adjacent segment disease requiring surgery: Under 5% at 20 years
- Risk factors: Fusion to L3 or more distal (higher lumbar stress), sagittal imbalance
Key principle: Selective fusion (sparing lumbar spine when possible) reduces adjacent segment issues.
Complication Rates
Neurologic injury: Under 1% (with neuromonitoring). Dural tear: 5-10% (usually repaired without sequelae). Excessive blood loss: 5-10% require transfusion. Vascular injury: Under 0.1% (life-threatening).
Infection (superficial): 1-2%. Infection (deep): 0.5-1%. Pneumothorax: 1-2%. SMA syndrome: 1-3%. Ileus: 5-10% (resolves spontaneously).
Pseudarthrosis: 1-2% (modern screws). PJK: 20-30% (mostly asymptomatic). Adding-on: 5-10% (preventable with proper fusion level selection). Hardware failure: Under 5%.
Overall revision rate: 5-10% at 10 years. Indications: Infection, pseudarthrosis, PJK (severe), adding-on, hardware prominence. Most revisions occur in first 2 years.
Predictors of Good Outcome
Favorable factors:
- ✓ Pre-op curve 45-70° (optimal surgical range)
- ✓ Balanced spine post-op (C7 plumb line within 2cm of sacrum)
- ✓ Restoration of thoracic kyphosis (DVR technique)
- ✓ Selective fusion (sparing lumbar segments when appropriate)
- ✓ Patient satisfaction with cosmetic improvement
Unfavorable factors:
- ✗ Pre-op curve over 90° (rigid, difficult correction, higher complication rate)
- ✗ Sagittal imbalance post-op (flat back, positive sagittal balance)
- ✗ Over-fusion (fusing compensatory lumbar curves unnecessarily)
- ✗ Persistent shoulder asymmetry (failure to address proximal thoracic curve if structural)
Prognosis Summary
Excellent prognosis for appropriately selected and treated patients:
- Over 90% patient satisfaction at 2+ years
- Maintained curve correction with minimal loss over time
- Normal life expectancy and quality of life
- Low complication and revision rates with modern techniques
- Ability to participate in full activities including pregnancy and sports
Key message: AIS surgery is highly successful when performed for appropriate indications with meticulous technique and proper fusion level selection.
Evidence Base
- Multicentre trial (randomised + preference cohorts) of bracing vs observation for AIS (typical bracing indications: age, skeletal immaturity, curve 20-40°)
- Combined-cohort treatment success (curve staying under 50° / reaching maturity): 72% with bracing vs 48% with observation (propensity-adjusted OR 1.93, 95% CI 1.08-3.46)
- Intention-to-treat (randomised cohort): 75% success with bracing vs 42% with observation (OR 4.11, 95% CI 1.85-9.16)
- Significant positive dose-response between hours of brace wear and success (P less than 0.001); brace prescribed for at least 18 hours/day
- Trial stopped early owing to the efficacy of bracing
- Retrospective comparison of 78 thoracic AIS patients treated with Cotrel-Dubousset instrumentation: hooks (31), hook-pattern screws (23), and segmental pedicle screws (24)
- Major curve correction: 55% with hooks, 66% with hook-pattern screws, 72% with segmental pedicle screws (loss of correction 6%, 2%, 1% respectively)
- Apical rotational correction (Perdriolle) far better with segmental screws: 59% vs 26% (hook pattern) vs 19% (hooks)
- 13 of ~400 screws (3%) malpositioned, with no neurologic impairment and no adverse effect on outcome
- Best restoration of hypokyphosis with segmental screws - a triplanar correction advantage over hooks
- Three-component system: curve type (1-6), lumbar modifier (A/B/C based on CSVL-to-lumbar-apex relationship), and sagittal thoracic (T5-T12) modifier (minus / N / plus)
- Independent-group reliability good-to-excellent: curve-type interobserver kappa 0.74 / intraobserver 0.89; lumbar modifier 0.80 / 0.84; sagittal modifier 0.94 / 0.97
- Distinguishes structural from non-structural curves in proximal thoracic, main thoracic, and thoracolumbar/lumbar regions to guide arthrodesis levels
- Shown to be substantially more reliable than the King classification
- Incorporates the sagittal plane, addressed only descriptively by earlier systems
- International consensus guideline (Delphi process) on conservative treatment of idiopathic scoliosis during growth - 68 recommendations
- 25 recommendations on bracing, 18 on physiotherapeutic scoliosis-specific exercises (PSSE), 14 on assessment
- Three grade-A recommendations (level-of-evidence I): two for bracing and one for assessment, reflecting the BrAIST and PSSE trials
- Recognises high-quality bracing evidence (one large multicentre trial) and emerging PSSE evidence (three single-centre RCTs)
- Notes heterogeneity of study protocols limits generalisability and calls for standardised research methods
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 13-year-old girl is referred by her school screening program for asymmetry on forward bend test. How would you assess her?”
“A 12-year-old premenarchal girl presents with a 32-degree right thoracic curve. Risser 0. How would you manage her?”
“A 14-year-old girl with a 58-degree right thoracic curve (T5-T12) and 35-degree left lumbar curve (T12-L4) is referred for surgery. How would you classify and plan treatment?”
“You are called to see a patient on post-op day 4 after PSF for AIS. She is nauseated, vomiting, and unable to tolerate oral intake. Abdomen is distended. What is your approach?”
“A 12-year-old boy presents with a 40-degree left thoracic curve. He has mild back pain at night. What concerns you and how would you proceed?”
MCQ Practice Questions
Quick Reference MCQ Points
Q: What is the recommended daily brace wear time per the BrAIST study, and what is the key relationship? A: At least 18 hours/day is prescribed, and there is a significant dose-response - more hours of wear means greater success (overall 72% with bracing vs 48% observation).
Q: What is the surgical strategy for Lenke Type 1 curve? A: Selective thoracic fusion only (spare lumbar curve). Lumbar curve is compensatory and will spontaneously improve after thoracic correction.
Q: What does Lumbar Modifier C indicate? A: CSVL is greater than 6mm lateral to lumbar apical vertebra - lumbar curve is STRUCTURAL and must be included in fusion.
Q: What investigation is mandatory before surgery for a left thoracic curve? A: MRI whole spine - left thoracic curves in AIS are red flags for syrinx, Chiari malformation, cord tumor, or tethered cord.
Q: What is the expected progression rate for curves over 50° after skeletal maturity? A: Approximately 1° per year throughout adulthood (Weinstein 50-year natural history study).
Guidelines, Registries & Global Practice
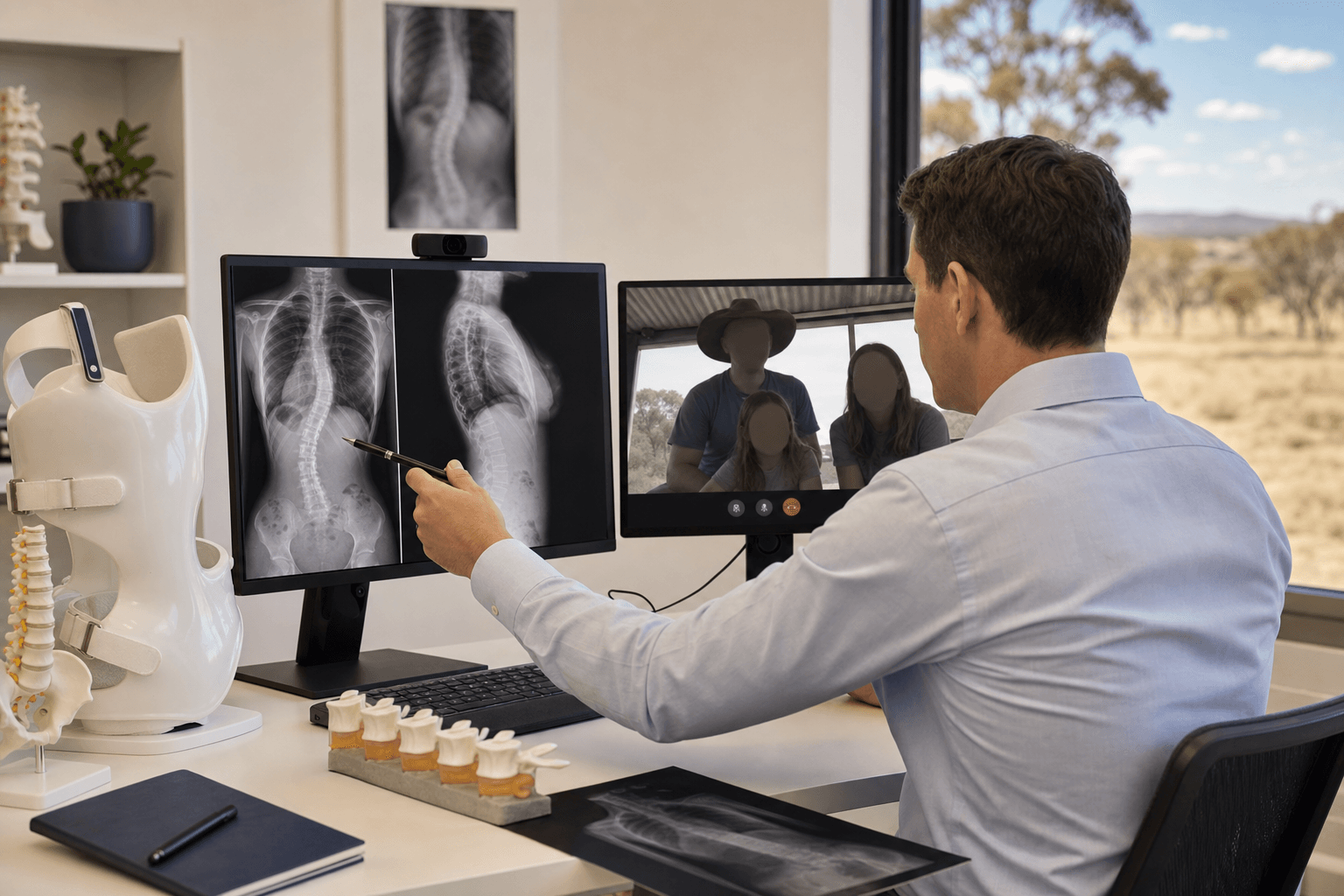
OrthoVellum is a worldwide resource: this section gives the global standard of care plus the key regional differences a candidate may be examined on, drawing on the major society guidelines as cited evidence rather than any single country's health system.
Global Epidemiology
AIS is the most common form of paediatric spinal deformity, defined as a coronal Cobb angle of at least 10° in children aged 10-18 with no identifiable cause (per the US Preventive Services Task Force review). Population estimates are consistent across high-income settings:
| Parameter | Figure | Notes |
|---|---|---|
| Prevalence (curves ≥10°) | Approximately 2-3% of adolescents | Most small curves are clinically insignificant and sex-balanced |
| Sex ratio (larger curves) | Female predominance, rising with curve magnitude (up to ~7:1 for curves over 30°) | Small curves near 1:1; female sex strongly predicts progression |
| Age of onset | 10 years to skeletal maturity (peak at pubertal growth spurt) | Girls present earlier than boys |
| Neural-axis abnormality on MRI | Reported in a minority of presumed-AIS cases; higher with atypical features (left thoracic, neurology, pain) | Drives the red-flag MRI policy |
Prevalence figures are broadly similar across world regions where school or population screening has been performed; reported variation largely reflects differing screening methods and curve thresholds rather than true biological difference. The female-to-male ratio rising with curve size is the most reproducible epidemiological signal.
Major Guidelines, Side by Side
The two dominant international frameworks are the Scoliosis Research Society (SRS) surgical/clinical tradition and the International Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) conservative-care guideline, which genuinely differ in emphasis. National screening policy is the clearest area of divergence.
| Body / Region | Position | Evidence level |
|---|---|---|
| SOSORT 2016 (international) | Bracing recommended for progressive curves during growth; physiotherapeutic scoliosis-specific exercises (PSSE) endorsed - 3 grade-A recommendations | Grade A (LoE I) for bracing and assessment |
| BrAIST / SRS (operative tradition) | Bracing standard of care for curves ~20-40° in immature patients; surgery for curves ~45-50°+ | Level I RCT evidence for bracing |
| USPSTF 2018 (USA) | Evidence insufficient to assess benefits/harms of routine school screening of asymptomatic adolescents (I statement) | I statement (insufficient) |
| PSSE (Schroth and others) | Adjunct to reduce progression during growth; emphasised in SOSORT, less so in operative-led systems | LoE II (single-centre RCTs) |
A genuine practice tension exists: SOSORT and many European/Asian centres actively promote scoliosis-specific exercises and intensive conservative care, whereas the US evidence-appraisal tradition (USPSTF) regards both routine screening and exercise therapy as having insufficient evidence. Both nonetheless agree that bracing slows progression of moderate curves in skeletally immature patients - the one conclusion supported by Level I data (BrAIST).
Screening Policy Variation
Retained in parts of Asia (e.g. several programmes in East Asia) and historically in some US states - aims for early, brace-eligible detection.
USPSTF found routine screening evidence insufficient (I statement). Many systems rely on opportunistic primary-care detection.
Adams forward-bend test plus scoliometer remains the universal first-line clinical screen wherever screening occurs.
Devices, Implants and Resource Setting
Spinal instrumentation systems are regulated as high-risk implantable devices across major jurisdictions (e.g. FDA Class II/III in the USA, CE-marked Class III in Europe, TGA-approved in Australia); AVBT/vertebral body tethering has more limited and evolving regulatory approval and remains a selected-patient option rather than standard care. There is no dedicated international AIS implant registry equivalent to the arthroplasty joint registries; outcome evidence instead comes from prospective society cohorts and multicentre studies such as those cited above.
In limited-resource settings, presentation is often later and with larger, more rigid curves because screening and timely bracing are less available, shifting management toward primary surgery (sometimes staged anterior release plus posterior fusion for rigid curves) and away from the brace-led pathways feasible where early detection is routine.
Definition & Epidemiology
- AIS = lateral curvature over 10° (Cobb angle) + vertebral rotation, age 10-18, unknown cause
- Prevalence: 2-3% of adolescents. Female:Male = 7:1 for curves over 30°
- Peak onset: Puberty (girls age 10-12, boys 12-14). Coincides with peak growth velocity
- Etiology: Multifactorial - genetic (30% twin concordance), biomechanical, neuromuscular theories
Red Flags for Non-Idiopathic Scoliosis
- Left thoracic curve (AIS is typically RIGHT thoracic) - think syrinx, Chiari, tumor
- Pain (especially night pain) - AIS is painless. Pain = tumor (osteoid osteoma), infection
- Neurologic signs (weakness, hyperreflexia, clonus, Babinski, cavus feet) - cord pathology
- Age under 10 (infantile/juvenile) or male sex - higher risk of secondary cause
- Rapid progression (over 10° in 6 months) - congenital, neuromuscular, tumor
- Skin findings (café-au-lait = NF-1, hairy patch = dysraphism, port-wine stain = vascular)
Clinical Assessment - Key Maneuvers
- Adams forward bend test: Patient bends 90° forward, examiner looks for rib hump (indicates rotation)
- Scoliometer (inclinometer): Measures angle of trunk rotation. Over 7° ATR → likely Cobb over 20°
- Shoulder height: Left elevation suggests proximal thoracic curve (Lenke Type 2)
- Coronal balance: C7 plumb line to sacral crease (within 2cm = balanced)
- Neurologic exam: MUST be normal in AIS. Any abnormality → MRI mandatory
Risser Sign (Skeletal Maturity)
- Grades 0-5 based on iliac crest apophysis ossification (seen on PA spine film)
- Risser 0: No ossification - most growth remaining (1-2 years) - HIGHEST RISK
- Risser 1-3: Progressive ossification 0-25%, 25-50%, 50-75%
- Risser 4: 75-100% but not fused - near maturity
- Risser 5: Complete fusion to ilium - skeletal maturity, growth complete
- Triradiate cartilage (Y-cartilage of acetabulum): Closure = puberty onset but still growing
Lenke Classification (6 Curve Types)
- Type 1 (Main Thoracic): Most common (50-60%). Right thoracic structural, lumbar compensatory. Selective thoracic fusion
- Type 2 (Double Thoracic): Proximal + main thoracic both structural. Fuse both (T2-T12)
- Type 3 (Double Major): Thoracic + lumbar both structural. Fuse both (T4-L3)
- Type 4 (Triple Major): Proximal + main + lumbar all structural. Long fusion (T1-L3)
- Type 5 (TL/Lumbar): Thoracolumbar or lumbar only. Fusion T10-L3
- Type 6 (TL-Main Thoracic): Both TL and main thoracic structural. Fusion T3-L3
Lenke Modifiers
- Lumbar Modifier (A/B/C): Distance from CSVL to lumbar apex
- Modifier A: CSVL between lumbar pedicles - lumbar not structural, no fusion needed
- Modifier B: CSVL touches lumbar vertebra - borderline, surgeon judgment
- Modifier C: CSVL lateral to entire lumbar vertebra (over 6mm) - lumbar STRUCTURAL, must fuse
- Sagittal Thoracic Modifier (-/N/+): T5-T12 kyphosis
- Minus (-): Under 10° (hypokyphotic) - renders thoracic structural
- Normal (N): 10-40° (physiologic)
- Plus (+): Over 40° (hyperkyphotic) - rare in AIS
Structural vs Non-Structural Curves
- Structural: Cobb over 25° on standing film OR fails to correct to under 25° on side-bending
- Non-structural (compensatory): Flexible, corrects to under 25° on side-bending
- Structural curves MUST be fused. Non-structural should NOT be fused (leads to imbalance)
- Side-bending films essential for pre-op planning - distinguish structural from compensatory
Management Algorithm
- Curves under 10°: Not scoliosis, observe
- 10-25° (immature): Observe every 4-6 months
- 25-40° (Risser 0-2): Brace 18-23 hours/day (BrAIST: 72% success vs 48% observation)
- 25-40° (Risser 4-5 mature): Observe, no bracing (growth complete)
- 40-45° (immature): Intensive brace vs surgery discussion
- Over 45-50°: Surgery - posterior spinal fusion with pedicle screws
Bracing - BrAIST Study Findings
- Indication: Curves 25-40°, Risser 0-2 (skeletally immature)
- Success: 72% in bracing group vs 48% observation (success = stays under 50° at maturity)
- Dose-response: significant positive association between hours of wear and success (P less than 0.001); brace prescribed at least 18 hours/day
- Goal: Halt progression until skeletal maturity (not permanent correction)
- Rebound: 5-10° increase after brace discontinuation is expected
- Compliance: Temperature sensors monitor wear time. Psychosocial support essential
Surgical Indications
- Primary: Cobb angle 45-50° or greater (consensus threshold)
- Progression: Curve over 5-10° increase despite bracing in immature patient
- Cosmesis: Patient-reported significant deformity affecting quality of life
- Prevention: Curves over 50° progress 1°/year lifelong, risk cardiopulmonary compromise over 80°
Posterior Spinal Fusion - Key Principles
- Gold standard: Pedicle screw instrumentation (replaced hooks/wires)
- Advantages: Three-column fixation, better derotation, lower pseudarthrosis, no post-op brace
- Fusion levels: Guided by Lenke classification. Fuse structural curves, spare compensatory
- Goal: 50-70% Cobb angle correction (not 100% - risks neurologic injury)
- Neuromonitoring: SSEP + MEP mandatory. Alarm = stop, release correction, check anesthesia
- DVR (Direct Vertebral Rotation): Concave rod cantilever derotates vertebrae, restores kyphosis
Complications - Key Points
- Neurologic injury: Under 1% with neuromonitoring. MEP over 50-80% drop = alarm
- SMA syndrome: POD 3-7, vomiting, duodenal obstruction. Rx: NPO, NGT, prone positioning
- Infection: 1-2%. Deep infection may require hardware removal + long-term IV antibiotics
- Pseudarthrosis: 1-2%. Often asymptomatic. Symptomatic needs revision fusion
- Proximal junctional kyphosis (PJK): 20-30%. Over 10° kyphosis at UIV+1/2. Usually mild
- Adding-on: Distal compensatory curve becomes structural. Prevention: fuse to neutral/stable vertebra
MRI Spine - When Mandatory
- Left thoracic curve (20-30% neural axis abnormality)
- Any neurologic signs or symptoms
- Painful scoliosis (especially night pain)
- Rapid progression (over 10° in 6 months)
- Male patient with scoliosis
- Age under 10 years
- Before ALL surgical corrections (5-10% prevalence syrinx/Chiari even without red flags)
Exam High-Yield Facts
- BrAIST: bracing 72% vs observation 48% success; significant dose-response with hours worn (at least 18 hours/day prescribed)
- Lenke Type 1 = most common (50-60%). Selective thoracic fusion, spare lumbar
- Modifier C (CSVL over 6mm from lumbar apex) = must fuse lumbar spine
- Curves over 50° progress 1°/year lifelong (even after skeletal maturity)
- MEP more sensitive than SSEP for detecting motor pathway injury
- SMA syndrome: POD 3-7, prone positioning therapeutic
- Pedicle screws achieve three-column fixation, better than hooks (two-column)
- Goal of surgery: 50-70% correction (not 100%), maintain coronal and sagittal balance