The Pure Motor Branch
- AIN is a purely motor nerve (except for sensory branches to the wrist joint).
- It supplies 3 muscles: FPL, FDP (Index/Middle), and Pronator Quadratus.
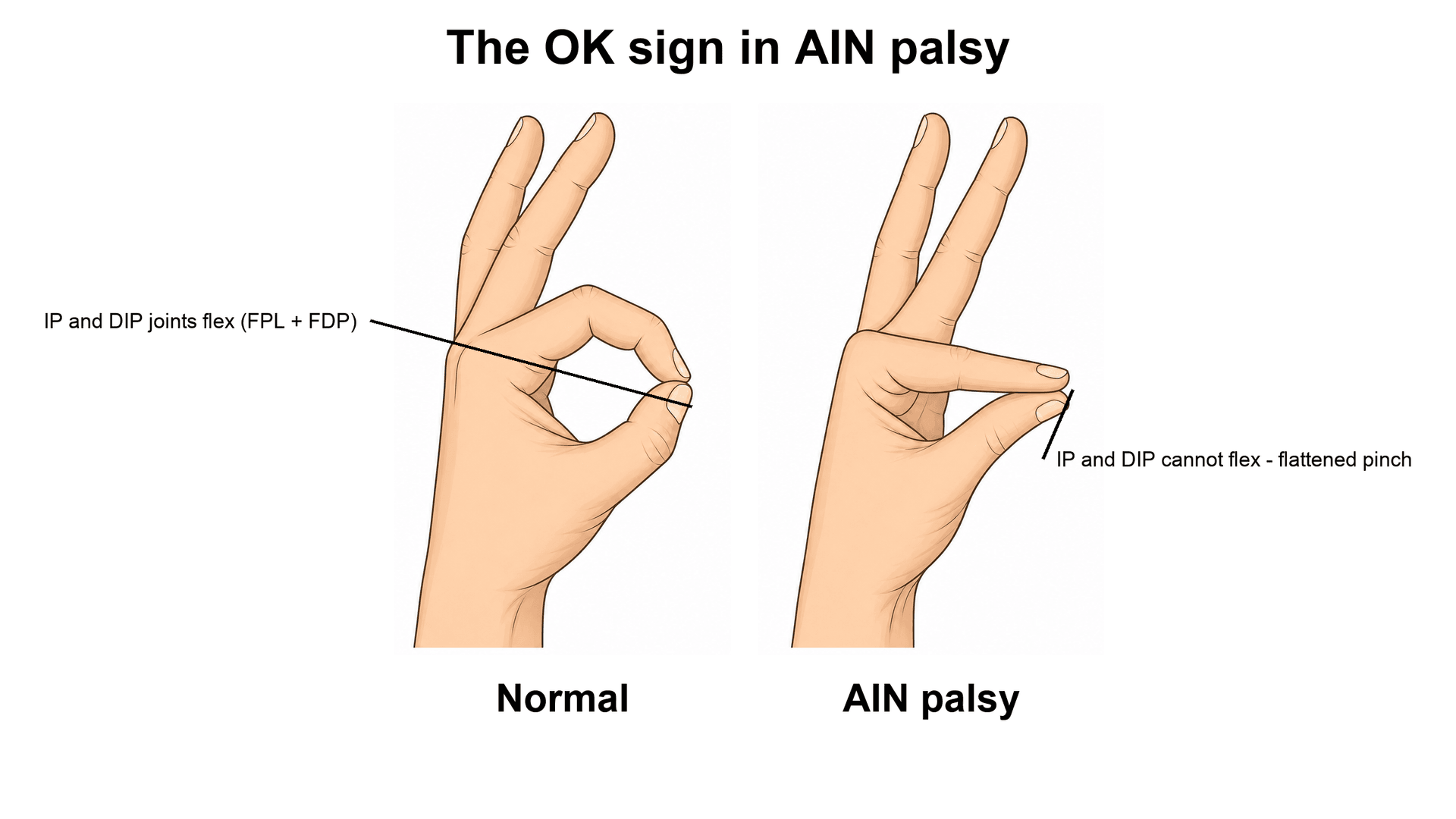
- Compression causes AIN Syndrome (Kiloh-Nevin): Inability to make the 'OK' sign.
- No cutaneous sensory loss in AIN syndrome (unlike Median nerve compression).
- Martin-Gruber Anastomosis is a crossover from AIN/Median to Ulnar nerve in the forearm.
- Parsonage-Turner Syndrome (Neuralgic Amyotrophy) can mimic AIN palsy.
- “Gantzer's Muscle (Accessory FPL head) is the most common cause of compression.
- “In MGA, intrinsic hand muscles (normally ulnar) are innervated by the Median nerve.
- “The 'Spinner's Bands' (of FDS) can also compress the AIN.
Neuralgic Amyotrophy AIN palsy is often viral/inflammatory (Parsonage-Turner), NOT compressive. History of viral illness, severe shoulder/arm pain, followed by weakness. Surgery (Decompression) does NOT help Parsonage-Turner and may make it worse.
Observation Most AIN palsies resolve spontaneously (6-12 months). Surgical exploration is reserved for clear mass lesions or failure to recover after 12 months. Always order an EMG to confirm denervation and rule out brachial plexitis.
- Motor
- FPL, FDP(I/M), PQ
- Sensory (Skin)
- None
- Test
- OK Sign
- Sign
- Teardrop
- Motor
- All flexors (exc FCU)
- Sensory (Skin)
- Radial 3.5 digits
- Test
- Fist
- Sign
- Hand of Benediction
- Motor
- Thenar (LOAF)
- Sensory (Skin)
- Radial 3.5 digits
- Test
- Opposition
- Sign
- Ape Hand
- Motor
- Intrinsics, FCU
- Sensory (Skin)
- Ulnar 1.5 digits
- Test
- Cross fingers
- Sign
- Claw Hand
PLuMPMuscles Innervated
Hook:The AIN creates a PLuMP forearm.
SPINCompression Sites
Hook:The nerve SPINs around local structures.
PAINParsonage Turner
Hook:PTS starts with PAIN.
Overview
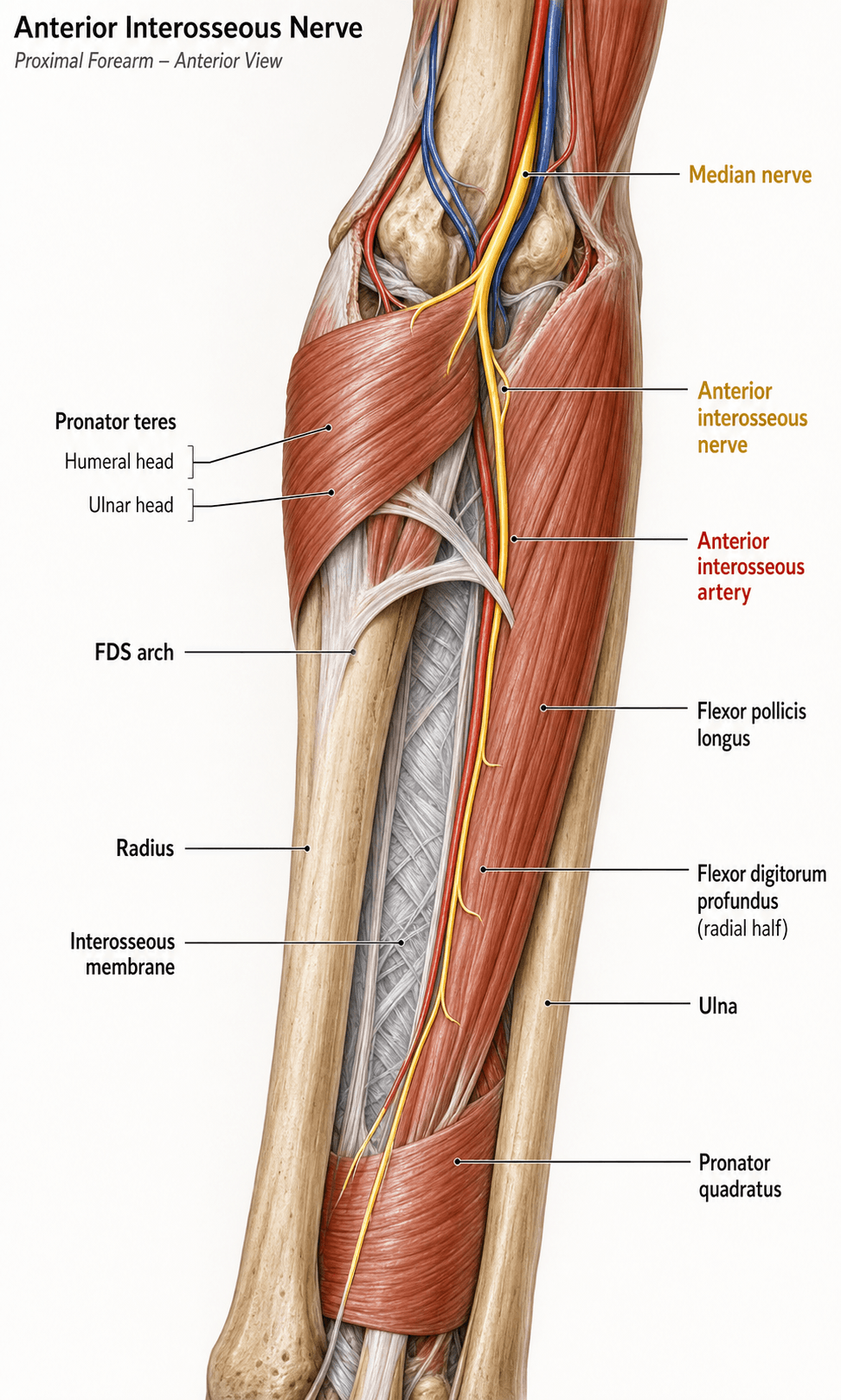
The Anterior Interosseous Nerve (AIN) is the largest branch of the Median Nerve in the forearm. It arises approximately 5-8 cm distal to the lateral epicondyle and courses deep on the interosseous membrane to supply the deep volar compartment.
It is classically described as a "pure motor" nerve, but it provides articular mechanoreceptor fibers to the wrist joint composed of Pacinian corpuscles and Ruffini endings.
Neurovascular
Course
- Origin: Leaves the Median nerve 5-8 cm distal to lateral epicondyle, as it passes between the two heads of Pronator Teres.
- Path: Travels initially parallel to the Median nerve, then dives deep.
- Relations: Runs between FPL (radially) and FDP (ulnarly) on the anterior surface of the Interosseous Membrane.
- Vessels: Accompanied by the Anterior Interosseous Artery (branch of Common Interosseous).
- Termination: Passes deep to Pronator Quadratus, supplying it, and ends as sensory branches to the radiocarpal, midcarpal, and CMC joints.
The nerve lies strictly on the interosseous membrane.


Although the AIN is functionally "pure motor," its terminal continuation pierces pronator quadratus and gives articular (sensory) branches to the wrist — the volar radiocarpal, midcarpal, intercarpal and distal radioulnar joints. These afferents are the anatomical basis of total (or partial) wrist denervation (the Wilhelm procedure) — dividing the wrist's articular nerve supply to relieve degenerative wrist pain while preserving motion.
- The two principal targets are the AIN and the posterior interosseous nerve (PIN) — their terminal articular twigs are resected on the volar and dorsal wrist respectively; a limited AIN-plus-PIN neurectomy is the most commonly performed version.
- Because these twigs are sensory-only and lie distal to the last motor branch (to pronator quadratus), denervation does not weaken pronation, finger flexion or grip.
- A diagnostic local-anaesthetic block of the AIN/PIN that abolishes the pain predicts a good response before committing to neurectomy.
Classification Systems
Martin-Gruber Anastomosis (MGA)
- Definition: A crossover of motor fibers from Median (AIN) to Ulnar nerve in the forearm.
- Prevalence: ~15% of population.
- Types:
- Type I: To Thenar muscles (simulating high ulnar palsy if median injured?).
- Type II: To First Dorsal Interosseous (FDI).
- Type III: To Hypothenar.
The pattern of innervation guides the diagnosis.
- Significance: In a proximal Ulnar nerve lesion, intrinsic function may be spared (because fibers travel via Median and cross over distally). Sensation is NOT affected by MGA.
Always check MGA in conflicting EMG findings.
Clinical Assessment
Kiloh-Nevin Syndrome (AIN Palsy)
- Weakness: Loss of FPL (Thumb IP flexion) and FDP Index (DIP flexion).
- OK Sign: Patient cannot make a perfect "O". Instead, they make a "Teardrop" or pinch pinch (pad-to-pad) due to lack of DIP/IP flexion.
- Pronator: Weakness of pronation in the fully flexed elbow (PQ is the primary pronator here; PT is relaxed).
- Sensation: NORMAL. No numbness (different from Pronator Syndrome).
If numbness is present, it is NOT isolated AIN.
Imaging and Electrodiagnostics
Electrodiagnostics
- EMG: Gold standard. Shows active denervation (fibrillations, positive sharp waves) in FPL, FDP I/II, and PQ.
- Timing: Changes appear 3-4 weeks after onset.
- Differential: Brachial Plexitis (Parsonage-Turner) will show patchy involvement of other nerves (e.g., Suprascapular, Long Thoracic).
Look for "denervation edema" on MRI if EMG is equivocal.
Differential Diagnosis
The acute, painless loss of thumb-and-index pinch has a short but high-stakes differential. The two errors that fail vivas are operating on a neuritis and missing a tendon rupture.
- Sensory loss
- None
- Pronator quadratus
- Weak (denervated)
- Key discriminator
- Pure motor loss of FPL + FDP-index, normal sensation
- Sensory loss
- Usually none in AIN form
- Pronator quadratus
- Weak
- Key discriminator
- Severe prodromal shoulder/arm pain then weakness; often multifocal on EMG
- Sensory loss
- Present (palmar median + radial 3.5 digits)
- Pronator quadratus
- Variable
- Key discriminator
- Numbness AND volar forearm aching; positive provocative tests
- Sensory loss
- Present (radial 3.5 digits)
- Pronator quadratus
- Weak
- Key discriminator
- Adds thenar and FCR/PL/FDS weakness plus sensory loss
- Sensory loss
- None
- Pronator quadratus
- Normal
- Key discriminator
- Lost tenodesis arc; normal EMG; mechanical cause
- Sensory loss
- None
- Pronator quadratus
- Weak
- Key discriminator
- Conduction block on EDX; responds to IVIg, not surgery
Surgical Technique
Henry's Approach
- Incision: Curvilinear incision crossing the elbow crease obliquely (Lateral to Medial).
- Interval: Between Pronator Teres (Median N) and Brachioradialis (Radial N).
- Superficial: Protect the Lateral Cutaneous Nerve of the Forearm (MCN).
The MCN is often at risk during the incision.
The AIN's own terminal motor branch — to pronator quadratus — is the workhorse donor for restoring intrinsic hand function in a high ulnar nerve palsy. The pronator-quadratus branch is expendable (forearm pronation is preserved by pronator teres), it carries a useful complement of motor axons, and it lies right beside the deep motor branch of the ulnar nerve at the distal forearm — close to the denervated intrinsic targets.
- Technique (in brief): the AIN/pronator-quadratus branch is coapted to the deep motor fascicle of the ulnar nerve at the wrist, most often as a supercharged end-to-side (SETS) transfer — the donor is sewn into the side of the recovering ulnar nerve so it reinnervates ("babysits") the intrinsics while the native ulnar axons regenerate down the limb.
- Why it works anatomically: a distal donor converts a slow proximal repair into a coaptation millimetres from the motor end-plates, helping to beat the 12-18-month denervation clock for the intrinsics.
(The broader menu and principles of nerve transfers are covered separately — the point here is the AIN-specific donor anatomy.)
Complications
- Iatrogenic Injury: Damage to Median nerve or Radial Artery.
- Failure: Failure to improve (incorrect diagnosis).
- Scar: Hypertrophic scarring at the antecubital fossa.
- Hematoma: Rich vascular supply.
- Neuroma: Of the Lateral Antebrachial Cutaneous Nerve (LCAN).
- Recurrence: Incomplete release (e.g., missed Gantzer's).
- CRPS: Always a risk.
- Hypersensitivity: In the scar.
Rehabilitation
- Splinting: None usually required unless weak.
- Motion: Maintain full passive ROM.
- Strengthening: Once re-innervation signs appear.
- Sensory: Not needed (no sensory loss).
Prognosis
- Neuritis: 80-90% recovery within 1 year.
- Compression: Excellent recovery if decompressed early (if true compression).
- Trauma: Poor outcome if nerve transected (requires grafting).
- Time: Recovery continues for up to 18 months, but plateau occurs earlier.
Clinical Relevance
Conservative (Standard)
- Indication: Spontaneous palsy (Neuritis/Viral) without a mass.
- Duration: 3-12 months. Most resolve.
- Therapy: Maintain PROM to prevent contractures.
- NSAIDs: For pain (if Neuralgic Amyotrophy).
Avoid surgical release in the acute inflammatory phase.
Guidelines, Registries & Global Practice
Global Epidemiology
- Isolated AIN palsy is rare, accounting for well under 1% of all upper-limb mononeuropathies in electrodiagnostic referral series.
- The majority of spontaneous (non-traumatic) cases are now regarded as a forme fruste of neuralgic amyotrophy (Parsonage-Turner syndrome) rather than mechanical entrapment.
- Neuralgic amyotrophy itself has a reported incidence of roughly 1 per 1,000 person-years when actively sought, far higher than older estimates of about 2-3 per 100,000 - the AIN/median territory is among the most frequently affected.
- Male predominance and a frequent antecedent trigger (viral illness, vaccination, surgery, strenuous exertion) are described across populations.
Side-by-Side Guidance (no single national framework)
- Position on spontaneous AIN palsy
- Electrodiagnosis to confirm and exclude broader plexopathy; observe spontaneous cases; reserve surgery for a defined mass or documented compression
- Position on spontaneous AIN palsy
- Distinguish neuritis from entrapment before any decompression; expectant management for idiopathic palsy
- Position on spontaneous AIN palsy
- Anatomical decompression only where a structural compressor is demonstrated; growing role for MRI/ultrasound to detect hourglass constrictions in non-recovering cases
- Position on spontaneous AIN palsy
- Oral corticosteroids may shorten the painful phase if started early; nerve imaging and selective interfascicular neurolysis for hourglass constrictions that fail to recover
There is broad international agreement: confirm with electrodiagnosis, observe idiopathic palsy for 12 or more months, and operate only for a structural lesion or a demonstrated fascicular constriction.
Registry & Imaging Notes
- There is no implant registry relevant to AIN palsy (a soft-tissue, non-arthroplasty condition); the evidence base is built on case series and electrodiagnostic/imaging cohorts.
- High-resolution 3T MR neurography and high-frequency ultrasound have shifted practice in well-resourced centres, enabling pre-operative localisation of hourglass constrictions (see Sneag et al.).
High- vs Limited-Resource Practice Variation
- Well-resourced settings: ready access to nerve conduction studies, MR neurography and microsurgical neurolysis; earlier, more selective surgery for imaging-proven constrictions.
- Limited-resource settings: diagnosis is predominantly clinical (the "OK sign"/teardrop pinch and preserved sensation), electrodiagnosis and advanced imaging may be unavailable, and management is necessarily conservative with longer observation; tendon transfers remain the universally available salvage for persistent paralysis.
Controversies & Areas of Uncertainty
- Neuritis vs entrapment: The dominant modern view (Miller-Breslow, Seror) is that most spontaneous AIN palsies are a neuritis, not mechanical entrapment. A minority remain genuinely compressive. There is no reliable bedside test to separate them at presentation, so electrodiagnosis and time are used as the discriminator.
- Does Gantzer's muscle actually compress the AIN? Anatomically the accessory FPL head usually lies POSTERIOR to both the median nerve and the AIN (al-Qattan), which argues against it being a frequent true compressor despite its traditional billing as "the most common cause."
- Role and timing of surgery: Whether and when to decompress idiopathic palsy is unsettled. Most authors observe for 12 or more months because surgery has not shortened recovery in comparison series; others explore earlier when a discrete compressor is suspected.
- Hourglass constrictions: High-resolution MRI/ultrasound increasingly reveal fascicular hourglass constrictions or torsion in non-recovering "neuritis" (Sneag). Whether these are best treated by interfascicular neurolysis, resection-and-graft, or continued observation is an active question.
- Corticosteroids in neuralgic amyotrophy: Early oral steroids may shorten the painful phase, but high-quality evidence for improved long-term motor recovery is limited.
MCQ Practice Points
Q: Which muscle is the most common cause of mechanical AIN compression? A: Gantzer's Muscle (Accessory head of FPL).
Q: What is the sensory deficit in a pure AIN palsy? A: None (it is a pure motor nerve to muscles). Articular branches only.
Q: A Martin-Gruber anastomosis typically involves fibers moving from where to where? A: Median to Ulnar.
Q: What condition typically mimics AIN palsy with a prodrome of pain? A: Parsonage-Turner Syndrome (Neuralgic Amyotrophy).
Q: When should EMG be performed in suspected AIN palsy? A: Wait 3-4 weeks after symptom onset. Earlier EMG may be falsely negative as denervation changes take time to develop. Pronator Quadratus testing is pathognomonic.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old wakes up with inability to bend the tip of his thumb. No pain. No trauma. Sensation normal.”
“A patient has a complete transection of the Ulnar nerve at the elbow. But he still has strong First Dorsal Interosseous function. Explain.”
“You decompressed an AIN palsy 6 months ago. No recovery. Patient is upset.”
Anatomy
- Origin: Median N (5-8cm distal to lateral epicondyle)
- Muscles: FPL, FDP (Index/Middle), Pronator Quadratus
- No Cutaneous Sensation (pure motor)
- Runs on anterior surface of interosseous membrane
- C8-T1 nerve root origin
Clinical
- Sign: Teardrop pinch (Cannot make OK sign)
- Syndrome: Kiloh-Nevin (AIN palsy)
- Mimic: Parsonage-Turner (Neuralgic Amyotrophy)
- Test: Pronation with elbow flexed (isolates PQ)
- No numbness - distinguishes from Pronator Syndrome
Variants & Compression
- Martin-Gruber Anastomosis (Median to Ulnar crossover)
- Gantzer's Muscle (accessory FPL head) - most common cause
- Pronator Teres deep head compression
- FDS arch (Spinner's bands) compression
- Lacertus fibrosus compression
Management
- Conservative: Observation 6-12 months (most recover)
- Surgical: Reserved for mass lesions or failure after 12 months
- Salvage: Tendon transfers (BR to FPL, FDP side-to-side)
- EMG: Confirm denervation 4 weeks post-onset
- DO NOT operate on Parsonage-Turner
Evidence Base
Nonoperative Treatment of AIN Paralysis (Foundational Natural-History Series)
- 10 patients with spontaneous partial AIN paralysis followed prospectively; all presented with a typical history of pain
- 7 of 10 had signs of involvement of nerves beyond the AIN on examination or EMG, supporting a neuritis rather than focal compression
- 8 patients treated by observation showed recovery by 6 months and full recovery within 1 year
- Surgical decompression did not shorten recovery time compared with observation
Gantzer's Muscle - Anatomical Study of the Accessory Head of FPL
- 25 cadaver limbs dissected; Gantzer's muscle present in 13 of 25 (52%)
- The accessory head was supplied by the anterior interosseous nerve in every specimen in which it was present
- It arose from the medial humeral epicondyle in 85%, with a dual epicondyle-plus-coronoid origin in the remainder
- It always lay POSTERIOR to BOTH the median nerve and the anterior interosseous nerve
Proximal Martin-Gruber Anastomosis at the Elbow (Largest EDX Series)
- Prospective 4-year electrodiagnostic detection of a proximal (elbow-level) Martin-Gruber anastomosis - the largest such series reported
- 16 cases identified, all with crossover fibres reaching an ulnar-innervated branch
- Detection via the first dorsal interosseous was more sensitive than via abductor digiti minimi
- A proximal MGA can mimic ulnar neuropathy at the elbow and create a discrepancy between clinical and electrodiagnostic findings
AAEM Case Report #25 - Electrodiagnosis of AIN Syndrome
- Illustrative case (57-year-old woman) with weakness of FPL and FDP to the index finger and no sensory deficit
- Median motor and sensory conduction studies were normal; needle EMG abnormalities were confined to FPL, FDP-index and pronator quadratus
- Reviews the literature distinguishing idiopathic AIN syndrome (part of neuralgic amyotrophy) from anatomic causes such as a fibrous band or anomalous muscle
- Establishes the role of electrodiagnosis - especially pronator quadratus sampling - in localising the lesion to the AIN
AIN Lesions - Clinical and Electrophysiological Features
- Consecutive series of 13 patients with AIN lesions referred for electrodiagnosis
- Only 3 had a correct initial clinical diagnosis and 3 were wrongly labelled tendon ruptures - highlighting frequent misdiagnosis
- 5 lesions were of mechanical origin and 7 were attributed to neuritis; all showed EDX abnormalities, most commonly in the pronator quadratus
- Late spontaneous recovery was common and only one patient underwent surgical exploration
MRI Bullseye Sign for Hourglass Constrictions in Parsonage-Turner Syndrome
- 6 patients with Parsonage-Turner syndrome and absent or minimal recovery underwent high-resolution MRI followed by surgical exploration
- Involved nerves included the anterior interosseous and pronator teres fascicles of the median nerve, plus suprascapular, axillary and radial nerves
- 23 constriction sites across 10 nerves were identified on MRI; a peripheral-bright, central-dark 'bullseye sign' lay immediately proximal to 21 of 23 sites
- All MRI-identified constrictions were confirmed at operation