Avascular | Aneural | 4 Zones | Type II Collagen | Aggrecan Proteoglycans
ZONAL ORGANIZATION
Critical Must-Knows
- Articular cartilage is avascular, aneural, and alymphatic - limited healing capacity
- Type II collagen (90-95% of collagen) provides tensile strength and framework
- Aggrecan proteoglycans attract water, providing compressive stiffness
- Four zones with different collagen orientation and proteoglycan content
- Tide mark separates deep zone from calcified cartilage
Clinical Pearls
- "Superficial zone has highest collagen, lowest proteoglycan content
- "Deep zone has lowest collagen, highest proteoglycan content
- "Collagen orientation changes from tangential to perpendicular across zones
- "Cartilage nutrition depends on diffusion from synovial fluid and subchondral bone
Clinical Imaging
Histology and Structure of Articular Cartilage

Critical Articular Cartilage Exam Points
Avascular Nature
Articular cartilage lacks blood vessels, nerves, and lymphatics. This explains limited healing capacity. Nutrition depends on diffusion from synovial fluid (cyclic loading pumps nutrients) and subchondral bone. Full-thickness defects may heal if subchondral bone is breached.
Collagen-Proteoglycan Balance
Type II collagen network (15-22%) constrains swelling pressure from aggrecan proteoglycans (4-7%). Proteoglycans attract water through negative charge (GAG side chains). Collagen resists tension, proteoglycans resist compression.
Zonal Organization
Four distinct zones with different structure and function. Superficial zone (tangential collagen) resists shear. Deep zone (perpendicular collagen, high proteoglycan) resists compression. Calcified zone anchors cartilage to bone at tide mark.
Biphasic Material
Cartilage is biphasic: fluid phase (water) and solid phase (collagen-proteoglycan matrix). Under load, water flows through matrix (time-dependent behavior). This viscoelastic property provides shock absorption and load distribution.
CARTILAGECARTILAGE - Key Features
| C | Collagen Type II framework 90-95% of collagen, provides tensile strength |
| A | Avascular, aneural, alymphatic Limited healing capacity, diffusion-based nutrition |
| R | Resistant to compression Proteoglycans provide compressive stiffness |
| T | Tide mark separates zones Boundary between deep and calcified zones |
| I | Interstitial fluid 70-80% Water content provides biphasic behavior |
| L | Layered zonal structure Four zones with different architecture |
| A | Aggrecan proteoglycan Major proteoglycan attracting water |
| G | GAG chains (chondroitin, keratan) Negative charges attract water and cations |
| E | ECM turnover is slow Chondrocyte metabolism maintains matrix |
| C | Collagen Type II framework 90-95% of collagen, provides tensile strength | T | Tide mark separates zones Boundary between deep and calcified zones | A | Aggrecan proteoglycan Major proteoglycan attracting water |
| A | Avascular, aneural, alymphatic Limited healing capacity, diffusion-based nutrition | I | Interstitial fluid 70-80% Water content provides biphasic behavior | G | GAG chains (chondroitin, keratan) Negative charges attract water and cations |
| R | Resistant to compression Proteoglycans provide compressive stiffness | L | Layered zonal structure Four zones with different architecture | E | ECM turnover is slow Chondrocyte metabolism maintains matrix |
Hook:CARTILAGE has layered structure with collagen and proteoglycans in avascular tissue
ZONESZONES - Articular Cartilage Organization
| Z | Zero blood vessels All zones are avascular |
| O | Orientation changes (tangential to perpendicular) Collagen orientation defines zones |
| N | Number is four Superficial, middle, deep, calcified |
| E | Each zone has different function Superficial resists shear, deep resists compression |
| S | Superficial has most collagen, least proteoglycan Gradient from surface to depth |
| Z | Zero blood vessels All zones are avascular | E | Each zone has different function Superficial resists shear, deep resists compression |
| O | Orientation changes (tangential to perpendicular) Collagen orientation defines zones | S | Superficial has most collagen, least proteoglycan Gradient from surface to depth |
| N | Number is four Superficial, middle, deep, calcified |
Hook:ZONES of cartilage have changing collagen orientation from surface to bone
AGGRECANAGGRECAN - Major Proteoglycan
| A | Aggregate with hyaluronan Multiple aggrecans bind to HA via link protein |
| G | GAG side chains attached Chondroitin sulfate and keratan sulfate |
| G | Giant molecule (2-3 MDa) One of largest proteoglycans |
| R | Repels water into cartilage Negative charges attract water |
| E | Essential for compression resistance Provides swelling pressure |
| C | Constrained by collagen network Collagen limits proteoglycan swelling |
| A | Anchored in deep zone Highest concentration in deep zone |
| N | Negatively charged (COO-, SO4-) Fixed negative charge density |
| A | Aggregate with hyaluronan Multiple aggrecans bind to HA via link protein | R | Repels water into cartilage Negative charges attract water | A | Anchored in deep zone Highest concentration in deep zone |
| G | GAG side chains attached Chondroitin sulfate and keratan sulfate | E | Essential for compression resistance Provides swelling pressure | N | Negatively charged (COO-, SO4-) Fixed negative charge density |
| G | Giant molecule (2-3 MDa) One of largest proteoglycans | C | Constrained by collagen network Collagen limits proteoglycan swelling |
Hook:AGGRECAN aggregates provide negative charge attracting water for compression resistance
Overview

Articular cartilage is a specialized connective tissue covering the ends of bones in synovial joints. It provides a smooth, low-friction surface for joint motion and distributes loads to underlying subchondral bone.
Why articular cartilage structure matters clinically:
Limited Healing Capacity
The avascular, aneural nature of articular cartilage explains why cartilage injuries have limited healing potential. Partial-thickness defects do not heal spontaneously. Full-thickness defects exposing subchondral bone may heal with fibrocartilage.
Degenerative Disease
Understanding normal cartilage structure is essential to understand osteoarthritis pathophysiology. Loss of proteoglycans, collagen network disruption, and water content changes all contribute to cartilage degeneration.
Biphasic Material Concept
Articular cartilage is a biphasic material consisting of a fluid phase (water 70-80%) and solid phase (collagen-proteoglycan matrix 20-30%). Under load, water flows through the porous solid matrix, creating time-dependent viscoelastic behavior. This provides shock absorption and load distribution.
Key structural principles:
- Avascular, aneural, alymphatic: Nutrition by diffusion from synovial fluid and subchondral bone
- Zonal organization: Four zones with different collagen orientation and composition
- Composite material: Collagen network constrains proteoglycan swelling pressure
- Biphasic behavior: Solid matrix and mobile fluid phase interact
Concepts and Composition
Three main components: water, collagen, and proteoglycans make up 95-98% of cartilage.
Water - 70-80% of Wet Weight
Distribution:
- Superficial zone: 75-80%
- Middle zone: 70-75%
- Deep zone: 65-70%
- Water content decreases with depth
Functions of water:
- Provides nutrition pathway (diffusion)
- Enables load distribution (biphasic behavior)
- Lubricates surface (hydrodynamic effect)
- Carries metabolites and waste products
Water Flow Under Load
When cartilage is loaded, water flows from compressed regions through the porous collagen-proteoglycan matrix. This time-dependent flow creates viscoelastic behavior. Sustained loading causes creep (progressive deformation). Load removal allows recovery as water re-imbibes.
Water is held in cartilage by osmotic pressure from proteoglycans and constrained by collagen network.
Zonal Organization
Four distinct zones with different structure, composition, and mechanical properties.
Zonal Organization of Articular Cartilage
| Zone | Depth | Collagen Orientation | Proteoglycan Content | Water Content | Function |
|---|---|---|---|---|---|
| Superficial (tangential) | 5-10% | Parallel to surface | Lowest (15-20 mg/mL) | Highest (75-80%) | Shear resistance, low friction |
| Middle (transitional) | 40-60% | Oblique/random | Moderate (30-40 mg/mL) | Moderate (70-75%) | Transition zone |
| Deep (radial) | 30% | Perpendicular to surface | Highest (50-60 mg/mL) | Lowest (65-70%) | Compression resistance |
| Calcified cartilage | 5-10% | Anchored in bone | Intermediate | Low | Attachment to bone |
Superficial (Tangential) Zone - 5-10% Depth
Structure:
- Collagen fibrils parallel to articular surface
- Highest collagen content (greater than 80% dry weight)
- Lowest proteoglycan content (15-20 mg/mL)
- Highest water content (75-80%)
- Small diameter collagen fibrils densely packed
Cells:
- Flattened chondrocytes parallel to surface
- Highest cell density (15,000-20,000 cells/mm³)
- Express lubricin (proteoglycan 4, PRG4)
Mechanical properties:
- Highest tensile strength
- Resists shear forces
- Provides low-friction surface
Lubricin Production
Superficial zone chondrocytes uniquely express lubricin (also called PRG4, superficial zone protein). Lubricin is secreted onto articular surface and into synovial fluid, providing boundary lubrication and reducing friction. Loss of lubricin increases cartilage wear.
The superficial zone is the first line of defense against mechanical wear.
Mechanical Properties and Biomechanics
Articular cartilage has unique mechanical properties due to its biphasic composition and zonal organization.
Biphasic Theory of Cartilage Mechanics
Two phases:
- Solid phase: Collagen-proteoglycan matrix (20-30%)
- Fluid phase: Interstitial water (70-80%)
Behavior under load:
- Immediate response: Load carried by fluid phase (incompressible)
- Time-dependent response: Fluid exudes from matrix
- Equilibrium: Load carried by solid matrix (compressed)
- Recovery: Fluid re-imbibes when load removed
Cartilage Response to Load
Instantaneous deformation (1-2%). Load supported by fluid phase. No fluid flow yet. Cartilage behaves like incompressible material.
Water flows from compressed region through porous matrix. Progressive deformation (creep). Load gradually transferred to solid matrix. Interstitial fluid pressure decreases.
Fluid flow ceases. Equilibrium deformation reached (10-20%). Load fully supported by solid matrix (collagen and proteoglycans). Matrix compressed and stressed.
Osmotic pressure from proteoglycans draws fluid back into matrix. Cartilage swells and recovers original thickness. Recovery takes hours to days depending on load duration.
Clinical Relevance of Biphasic Behavior
Cyclic joint loading pumps fluid in and out of cartilage, facilitating nutrient transport from synovial fluid to chondrocytes. Immobilization impairs this pumping mechanism, reducing nutrition. Normal daily activities compress cartilage by 10-20%, which recovers overnight during sleep.
Biphasic behavior provides shock absorption and load distribution.
Clinical Relevance and Applications
Osteoarthritis Pathophysiology
Understanding normal cartilage structure is essential for understanding osteoarthritis pathophysiology:
Early OA Changes
Proteoglycan depletion is one of the earliest changes in OA. Loss of aggrecan reduces fixed negative charge, leading to decreased water content and compressive stiffness. Surface fibrillation occurs as protective superficial zone fails.
Progressive Degeneration
Collagen network disruption follows proteoglycan loss. Once the collagen arcade is damaged, cartilage cannot maintain integrity. Full-thickness defects expose subchondral bone, leading to bone-on-bone articulation.
Cartilage Repair Implications
Healing Capacity
Partial-thickness cartilage defects do not heal because articular cartilage is avascular. Full-thickness defects extending to subchondral bone may heal with fibrocartilage (Type I collagen) from marrow-derived mesenchymal stem cells. Fibrocartilage has inferior mechanical properties compared to hyaline cartilage.
Clinical Applications
Treatments based on cartilage biology:
- Microfracture/drilling: Penetrates subchondral bone to recruit MSCs for fibrocartilage repair
- ACI/MACI: Cultured chondrocytes to regenerate hyaline-like cartilage
- Osteochondral grafts: Transplant intact hyaline cartilage from non-weight-bearing areas
- Joint motion: Essential for cartilage nutrition via cyclic loading and diffusion
Cartilage Types: Differentiating the Three Subtypes
A common viva trap is to confuse hyaline articular cartilage with fibrocartilage and elastic cartilage. Distinguishing them by collagen type, location, and mechanical behaviour is high-yield.
Hyaline vs Fibrocartilage vs Elastic Cartilage
| Feature | Hyaline (articular) | Fibrocartilage | Elastic cartilage |
|---|---|---|---|
| Dominant collagen | Type II | Type I (plus some Type II) | Type II + elastin fibres |
| Typical sites | Articular surfaces, growth plate, costal, tracheal rings | Menisci, annulus fibrosus, pubic symphysis, repair tissue | External ear, epiglottis, Eustachian tube |
| Perichondrium | Absent over articular surface | Absent | Present |
| Proteoglycan content | High (aggrecan-rich) | Lower | Moderate |
| Mechanical role | Low-friction, compression and shear | Tensile load, energy absorption | Flexible support, recoil |
| Relevance to repair | Goal tissue (ACI/MACI/osteochondral graft) | Default repair tissue after microfracture (inferior, wears) | Not a repair tissue |
Why Repair Tissue Matters
Marrow-stimulation techniques (microfracture, drilling) fill defects with fibrocartilage dominated by Type I collagen. Fibrocartilage lacks the zonal collagen arcade and aggrecan density of native hyaline cartilage, so it has lower compressive and shear resistance and tends to deteriorate over time. This is the biological rationale for cell-based and osteochondral techniques that aim to restore hyaline (Type II) cartilage.
Controversies and Areas of Uncertainty
Best Repair Technique
There is no consensus single best technique for focal chondral defects. Microfracture is cheaper and single-stage but yields fibrocartilage with deterioration after 2 to 5 years; ACI/MACI and osteochondral techniques may give more durable hyaline-like tissue but are costlier and may be two-stage. Defect size, location, depth and patient age all modify the choice.
Tide Mark and Subchondral Bone
The role of the subchondral bone plate and calcified zone in osteoarthritis initiation versus consequence is debated. Whether tide-mark advancement and subchondral changes drive cartilage loss, or merely follow it, remains an active research question that influences whether therapies should target bone, cartilage, or both.
Cartilage Regeneration vs Repair
True regeneration of zonally organised hyaline cartilage with a restored collagen arcade has not been reliably achieved in humans. Current techniques produce repair tissue of variable quality. Whether scaffolds, growth factors, or gene/cell therapy can recreate the depth-dependent architecture is unresolved.
Lubrication Mechanisms
The relative contribution of boundary lubrication (lubricin, hyaluronan), fluid-film and interstitial-fluid-pressurisation mechanisms to the very low friction of cartilage is still actively studied, with implications for viscosupplementation and lubricin-based therapies.
Guidelines, Registries & Global Practice
Articular cartilage structure underpins the global burden of osteoarthritis and the choice of cartilage-repair strategies. Recommendations vary by society and by resource setting.
Global Epidemiology
Osteoarthritis is among the leading causes of disability worldwide, with the knee the most commonly affected large joint. Prevalence rises sharply with age and obesity and is increasing globally as populations age, making cartilage biology and preservation a worldwide priority rather than a regional one.
Symptomatic Chondral Defects
Focal chondral and osteochondral lesions are found in a substantial proportion of knee arthroscopies and are an important cause of pain and progression to osteoarthritis in younger, active patients - the group in whom cartilage-restoration procedures are most often considered.
Society Guidance on Cartilage Repair and OA Management
| Body | Region | Emphasis |
|---|---|---|
| ICRS (International Cartilage Regeneration & Joint Preservation Society) | Global | Standardised arthroscopic grading of chondral lesions and algorithm for defect size, depth and location guiding repair choice |
| AAOS | US | Evidence-based OA guidance; emphasis on non-operative measures (exercise, weight loss) first; cautious recommendations on intra-articular agents |
| NICE / BOA (UK) | UK | Core OA management of education, exercise and weight loss; ACI considered for selected knee defects within defined criteria |
| ESSKA / EFORT | Europe | Consensus on cartilage-defect management favouring restorative techniques in younger patients with isolated defects |
High-Resource Settings
Access to MRI for defect characterisation, arthroscopic grading, and the full range of restorative options (microfracture variants, ACI/MACI, osteochondral autograft/allograft). Cell-based therapies require licensed cell-culture facilities and are concentrated in specialist centres.
Limited-Resource Settings
Imaging and cell-based therapy access may be constrained, so single-stage marrow-stimulation and conservative management (activity modification, physiotherapy, weight management, analgesia) predominate. Joint-preserving surgery and timely arthroplasty for end-stage disease may also be limited by capacity.
Evidence Base
Biphasic Theory of Articular Cartilage
- Articular cartilage is a biphasic material (solid matrix + interstitial fluid)
- Under load, fluid flows through porous matrix creating time-dependent behavior
- Aggregate modulus describes equilibrium compressive properties
- Permeability determines rate of fluid flow and creep response
Zonal Organization and Collagen Architecture
- Described arcade-like collagen architecture from deep to superficial zones
- Collagen orientation changes from perpendicular (deep) to tangential (superficial)
- Zonal organization provides different mechanical functions
- This architecture has been confirmed by modern imaging techniques
Proteoglycan Swelling Pressure in Cartilage
- Directly measured cartilage swelling pressure and compared it with the osmotic pressure of constituent proteoglycans
- Fixed negative charge density on proteoglycan GAG chains generates Donnan osmotic (swelling) pressure
- Swelling pressure provides the compressive resistance of cartilage
- Collagen network constrains proteoglycan swelling, creating matrix prestress
The Biology of Lubricin: Near Frictionless Joint Motion
- Lubricin (PRG4) is a surface-active mucinous glycoprotein that coats the cartilage surface and provides boundary lubrication
- Prevents cell and protein adhesion and preserves superficial-zone chondrocytes
- Lubricin-null joints show damage to the superficial zone, implicating lubricin deficiency in arthropathy after trauma or inflammatory arthritis
- Recombinant rhPRG4 is a candidate therapeutic for transient lubricin deficiency
The Basic Science of Articular Cartilage: Structure, Composition, and Function
- Comprehensive review of articular cartilage as an avascular, aneural, alymphatic hyaline tissue with low cellularity
- Defines the four zones (superficial, middle, deep, calcified) and the gradient of collagen orientation and proteoglycan content
- Explains the collagen-proteoglycan composite and biphasic mechanical behaviour underlying load-bearing
- Limited intrinsic repair capacity follows directly from avascularity and low chondrocyte turnover
Autologous Chondrocyte Transplantation for Deep Cartilage Defects
- First-in-human series of autologous chondrocyte implantation (ACI) in 23 patients with full-thickness defects of 1.6 to 6.5 cm squared
- 14 of 16 femoral condylar transplants achieved good-to-excellent results at 2 years; patellar transplants performed less well
- Biopsy showed hyaline-like cartilage in 11 of 15 femoral transplants, in contrast to fibrocartilage from marrow-stimulation techniques
- Established that cultured autologous chondrocytes can resurface femorotibial cartilage defects
Basic Science Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Articular Cartilage Composition (~3 min)
"Describe the composition of articular cartilage and explain how each component contributes to its mechanical function."
Scenario 2: Zonal Organization (~4 min)
"Describe the zonal organization of articular cartilage. How does structure relate to function in each zone?"
Scenario 3: Biphasic Mechanics (~3 min)
"Explain the biphasic nature of articular cartilage. How does this contribute to load-bearing and nutrition?"
Management Algorithm
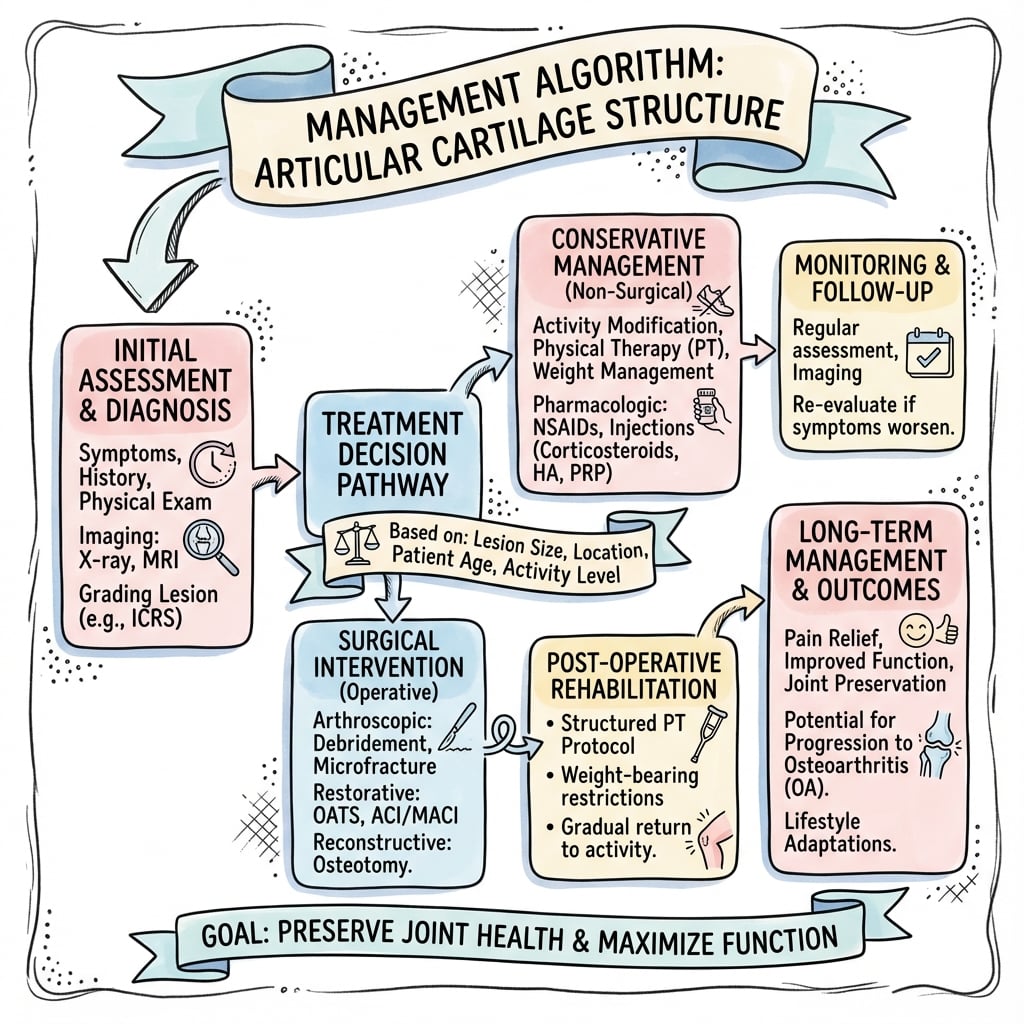
ARTICULAR CARTILAGE STRUCTURE
Clinical summary
Composition by Weight
- •70-80% water (fluid phase in biphasic model)
- •15-22% collagen (90-95% Type II, provides tensile strength)
- •4-7% proteoglycans (aggrecan with GAG chains, compression resistance)
- •1-2% cells and other proteins (chondrocytes, COMP, fibronectin)
Zonal Organization (4 Zones)
- •Superficial (5-10%): tangential collagen, high collagen, low proteoglycan, shear resistance
- •Middle (40-60%): oblique collagen, intermediate composition, transitional
- •Deep (30%): perpendicular collagen, low collagen, high proteoglycan, compression resistance
- •Calcified (5-10%): mineralized, tide mark boundary, anchors to subchondral bone
Type II Collagen Network
- •Type II collagen is 90-95% of total collagen (Type IX, XI minor collagens)
- •Fibril diameter 20-40 nm (smaller than Type I)
- •Orientation: tangential (superficial) to perpendicular (deep) - arcade structure
- •Provides tensile strength and constrains proteoglycan swelling
Aggrecan Proteoglycan
- •Major proteoglycan (90% of total), molecular weight 2-3 million Da
- •GAG side chains: chondroitin sulfate and keratan sulfate
- •Aggregates: 50-100 aggrecans bind to hyaluronan via link protein
- •Negative charges (SO4-, COO-) attract water via Donnan osmotic pressure
Biphasic Mechanics
- •Fluid phase (water) and solid phase (collagen-proteoglycan matrix)
- •Immediate load on fluid (incompressible), then water flows out (creep)
- •Equilibrium at hours: load on solid matrix, 10-20% deformation
- •Recovery after unloading: osmotic pressure draws water back in
Key Mechanical Properties
- •Aggregate modulus: 0.5-0.9 MPa (equilibrium compression)
- •Tensile modulus: 5-25 MPa (zone and direction dependent)
- •Hydraulic permeability: 0.5-5 × 10⁻¹⁵ m⁴/N·s
- •Viscoelastic: creep, stress relaxation, hysteresis
Clinical Pearls
- •Avascular, aneural, alymphatic: limited healing capacity
- •Nutrition by diffusion from synovial fluid and subchondral bone
- •Cyclic loading pumps nutrients in/out (immobilization impairs nutrition)
- •Lubricin from superficial zone provides boundary lubrication
- •OA: proteoglycan loss → reduced stiffness, collagen damage → fissures