Craniocervical Junction Disruption | High-Energy Trauma | Often Fatal
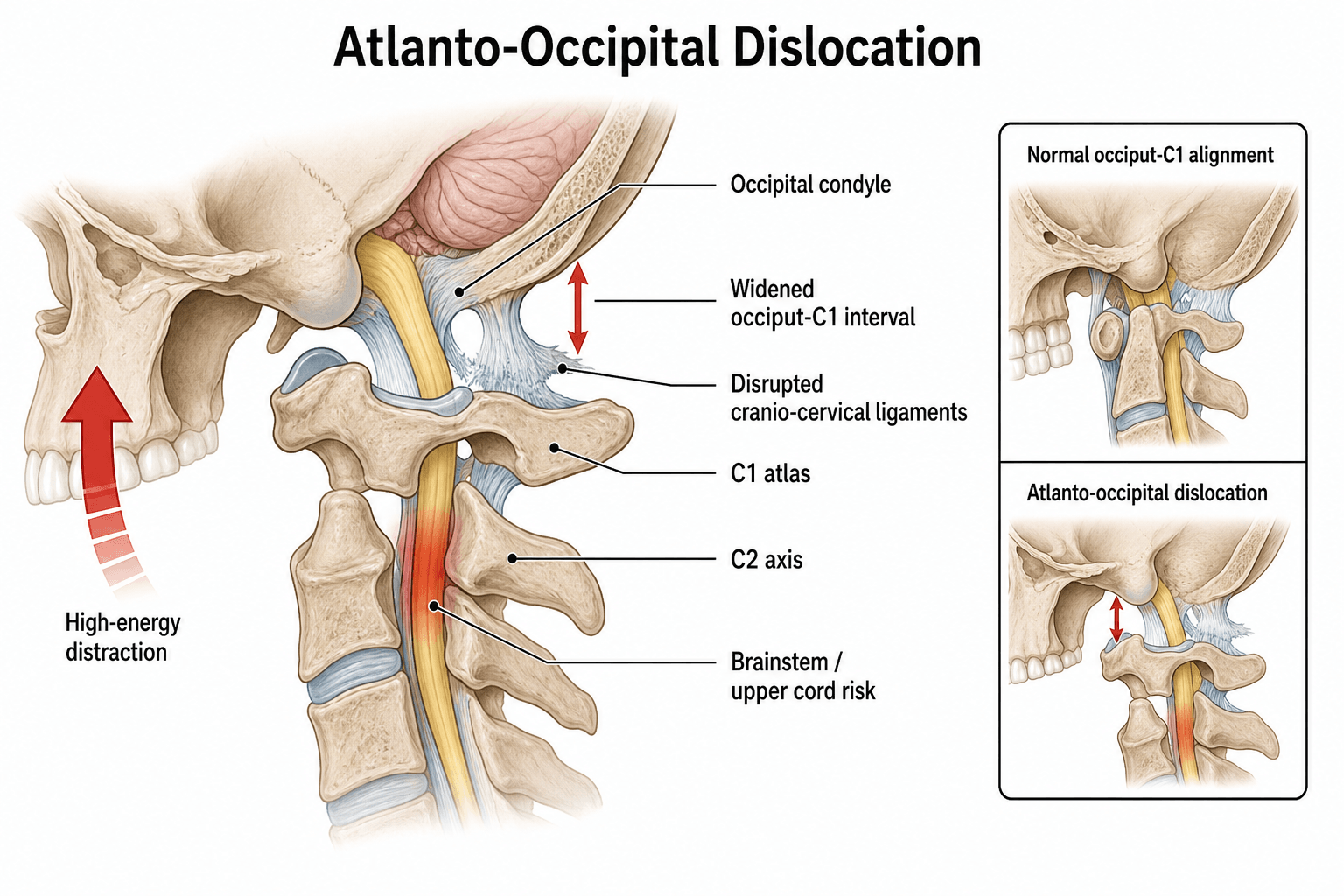
- Atlanto-occipital dislocation (AOD) is a high-energy craniocervical junction injury with high mortality
- Traynelis classification guides direction of displacement and stability assessment
- Powers ratio, condyle-C1 interval (CCI), and basion-dens interval (BDI) are key radiographic measurements
- Immediate rigid immobilisation in neutral position; traction is contraindicated
- Definitive treatment is occipitocervical fusion after reduction and stabilisation
- “AOD often missed on initial lateral cervical X-ray; CT is essential
- “Type II distraction injuries carry highest risk of neurological catastrophe
- “Paediatric patients have higher relative incidence due to ligamentous laxity
- “Never apply traction before confirming AOD type on imaging
High-energy trauma: Motor vehicle collision, fall from height, or pedestrian impact. Maintain high index of suspicion in any unconscious polytrauma patient with neck pain or neurological deficit.
Rigid cervical collar or halo applied immediately in neutral position. Log-roll precautions mandatory. Traction is absolutely contraindicated until imaging excludes distraction-type injury.
Powers ratio greater than 1.0 or CCI of 2.5 mm or more on CT indicates instability. BDI greater than 12 mm or BAI greater than 12 mm also abnormal. CT is first-line investigation.
Brainstem and upper cervical cord injury common. Survivors may have cranial nerve deficits, quadriparesis, or respiratory failure. Early occipitocervical fusion improves survival.
- Key Measurement
- Powers ratio greater than 1.0 or CCI of 2.5 mm or more
- Immediate Action
- Rigid collar, neutral position, CT scan
- Definitive Treatment
- Occipitocervical fusion after reduction
- Key Measurement
- CCI of 2.5 mm or more on coronal CT
- Immediate Action
- Halo or collar, avoid traction
- Definitive Treatment
- Posterior occipitocervical fusion
- Key Measurement
- BDI greater than 12 mm, longitudinal gap
- Immediate Action
- Neutral immobilisation only
- Definitive Treatment
- Urgent fusion after stabilisation
PCBRadiographic Measurements
Hook:PCB rules: Powers, CCI, BDI - measure these three on every trauma CT!
Overview and Epidemiology
Atlanto-occipital dislocation is one of the most lethal spinal injuries. The majority of patients die at the scene from brainstem transection or vascular disruption. Those who reach hospital require immediate recognition because inappropriate traction or delayed diagnosis converts a potentially survivable injury into a fatal one. Paediatric patients have a higher relative incidence due to ligamentous laxity and larger head-to-body ratio.
- High-energy MVC: Most common adult mechanism, often with associated injuries
- Fall from height: Significant axial load or hyperextension force
- Pedestrian impact: High-speed collision with direct craniocervical force
- Paediatric: Lower energy mechanisms can produce AOD due to ligamentous laxity
- Mortality: 70-85 percent overall; 15-30 percent reach hospital alive
- Neurological deficit: Cranial nerve palsies, quadriparesis, respiratory arrest
- Associated injuries: Head injury, thoracic trauma, long-bone fractures
- Survivors: Require lifelong occipitocervical fusion and rehabilitation
Pathophysiology
The atlanto-occipital joint relies on the alar ligaments, apical ligament, tectorial membrane, and joint capsules for stability. The occipital condyles articulate with the superior facets of C1 (atlas). Disruption of these restraints allows the occiput to translate or distract relative to C1. The vertebral arteries and brainstem are immediately at risk. Type II distraction injuries produce the greatest instability because all ligamentous tethers are sequentially torn.
- Function
- Limit rotation and lateral bending
- When Disrupted
- Allow anterior or posterior translation
- Function
- Secondary stabiliser of dens to occiput
- When Disrupted
- Contributes to longitudinal instability
- Function
- Posterior restraint to translation
- When Disrupted
- Permits anterior dislocation when torn
- Function
- Primary joint stability
- When Disrupted
- Complete disruption in all Traynelis types
Longitudinal distraction sequentially disrupts all ligaments from anterior to posterior. The occiput separates from C1, stretching the brainstem and vertebral arteries. Any traction applied before imaging confirmation can complete the distraction and cause immediate cardiorespiratory arrest.
Ligamentous laxity and larger head-to-neck ratio make children more susceptible. The fulcrum of injury is higher (C2-C3 in infants). AOD must be excluded in any child with unexplained neurological deficit after trauma, even with seemingly minor mechanisms.
Classification and Types
Traynelis Classification (Direction-Based)
- Direction
- Anterior displacement of occiput on C1
- Stability
- Unstable
- Key Imaging Finding
- Occipital condyles anterior to C1 facets on lateral view
- Direction
- Longitudinal distraction
- Stability
- Most unstable
- Key Imaging Finding
- Increased BDI and CCI, vertical separation
- Direction
- Posterior displacement of occiput on C1
- Stability
- Unstable
- Key Imaging Finding
- Occipital condyles posterior to C1 facets
Traynelis classification is the most widely used system because it directly informs reduction manoeuvres and the decision to avoid traction.
ALPTraynelis Classification
Hook:ALP: Anterior, Longitudinal, Posterior - the three directions of atlanto-occipital dislocation!
Clinical Assessment
- Mechanism: High-energy MVC, fall, or pedestrian strike
- Consciousness: Unconscious at scene raises suspicion dramatically
- Associated injuries: Head, chest, abdominal trauma common
- Symptoms in awake patients: Severe neck pain, occipital headache, cranial nerve symptoms
- Airway: Secure first; high cervical injury risks respiratory arrest
- Neurological: Cranial nerve examination (especially IX-XII), motor/sensory levels
- Neck: Swelling, step-off, crepitus; do not manipulate until imaged
- Associated: Scalp lacerations, facial fractures, long-bone injuries
Technique for suspected AOD: Apply rigid cervical collar or halo ring in neutral position only. Log-roll with in-line stabilisation. Obtain urgent CT from occiput to T1 with sagittal and coronal reconstructions. If Type II distraction pattern is present on CT, maintain neutral position without any attempt at closed reduction using traction. Traction in Type II injuries can convert a partial ligamentous disruption into complete separation.
- Key Discriminating Feature
- Abnormal Powers ratio, CCI, or BDI
- Investigation
- Urgent CT with measurements
- Key Discriminating Feature
- Fixed rotation, normal CCI/BDI
- Investigation
- Dynamic CT or open-mouth view
- Key Discriminating Feature
- Unilateral condyle displacement, stable joint
- Investigation
- CT classification (Anderson-Montesano)
- Key Discriminating Feature
- Lateral mass spread on open-mouth view
- Investigation
- CT for transverse ligament integrity
The unconscious polytrauma patient cannot report neck pain. AOD must be excluded by CT in every high-energy mechanism patient who arrives intubated or with Glasgow Coma Scale less than 8. A normal lateral cervical X-ray does not rule out AOD; up to half of cases are missed on plain films.
Investigations
Imaging Protocol
Indication: All high-energy trauma patients, especially unconscious or with neck pain Technique: Thin-slice (less than or equal to 1 mm) from occiput to T1 with sagittal and coronal reformats Measurements: Calculate Powers ratio, CCI (bilateral), BDI, BAI on every scan Red flags: Any measurement exceeding threshold requires immediate spine team notification
Indication: Assess vertebral artery integrity before any reduction or surgical planning Finding: Vertebral artery occlusion or dissection alters timing of surgery and anticoagulation decisions
Indication: Neurological deficit unexplained by CT, or to assess ligamentous and cord injury Findings: Tectorial membrane disruption, cord oedema, brainstem signal change Limitation: MRI does not change immediate management; CT measurements remain gold standard for diagnosis
Plain lateral cervical radiographs are unreliable for AOD. The Powers ratio requires precise identification of the basion and opisthion, which are often obscured. CT with multiplanar reconstructions is mandatory. Document the exact measurements in the radiology report and communicate abnormal values immediately to the trauma and spine teams.
Additional Craniocervical Alignment: the Wackenheim Line and the Harris Rule of 12s
Beyond the Powers ratio and the condyle-C1 interval, two further alignment checks are high-yield and easy to apply on the sagittal CT or lateral film.
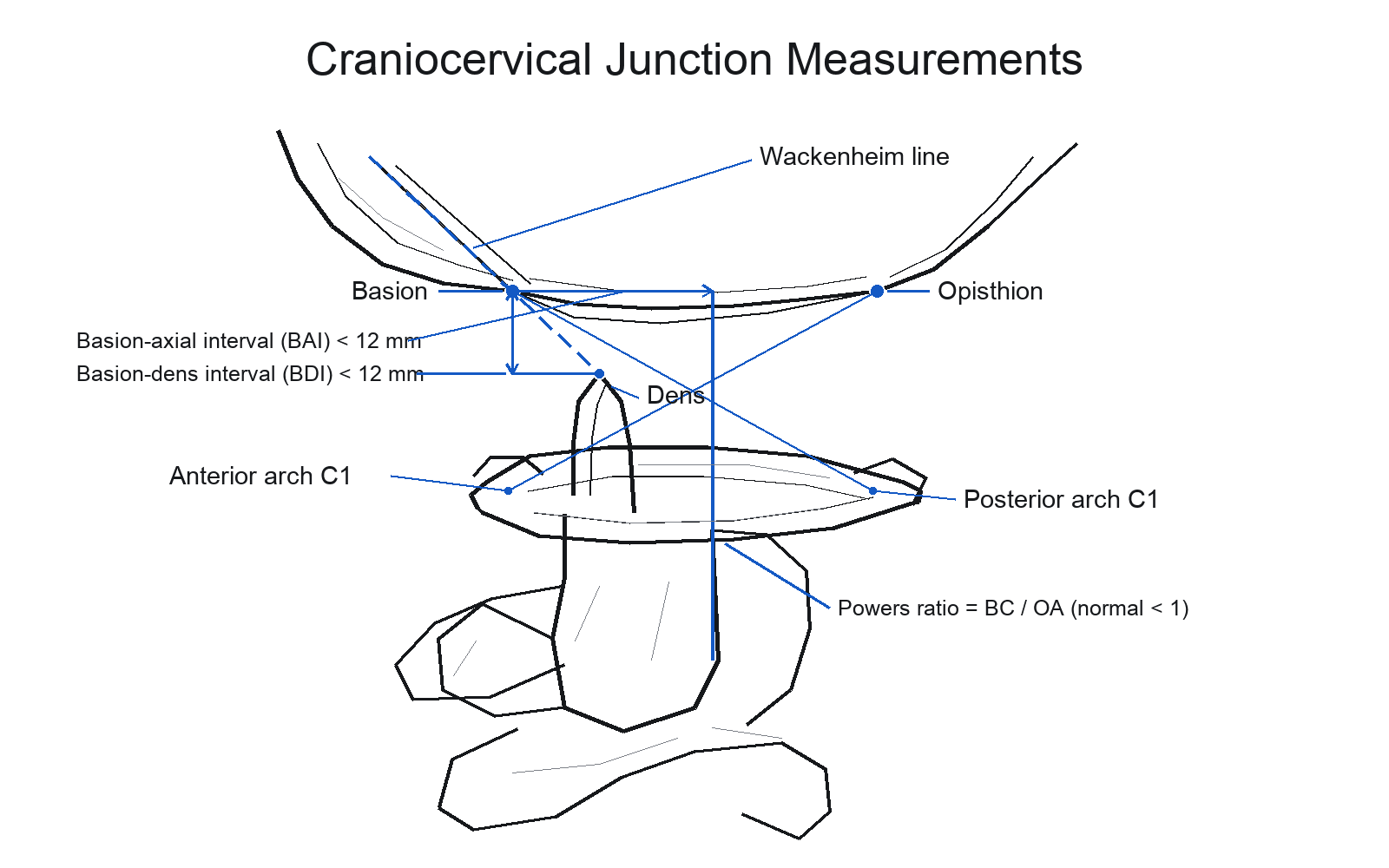
- A line drawn along the posterior surface of the clivus and extended caudally should fall tangential to (just touch) the posterior aspect of the tip of the dens.
- In AOD the occiput-to-dens relationship is disrupted, so the line no longer touches the dens normally; the same line is crossed by the dens in basilar invagination.
- The basion-dens interval (BDI) - basion to the tip of the dens - should be under 12 mm.
- The basion-axial interval (BAI) - basion to the posterior axial line (the rostral extension of the posterior cortex of the C2 body) - should also be under 12 mm.
- Either value over 12 mm is abnormal. The Harris method is generally more reliable than the Powers ratio, particularly for distraction (Type II) and posterior (Type III) patterns, which the Powers ratio can miss.
Add the Wackenheim line (the clivus extended should touch the dens tip) and the Harris rule of 12s (BDI and BAI each under 12 mm) to the Powers ratio and CCI. The Harris measurements are more reliable than the Powers ratio for distraction and posterior dislocations - exactly the patterns the Powers ratio under-detects - so apply them on every craniocervical trauma CT.
Management Algorithm
Immediate Management (All Types)
Goal: Prevent further distraction or translation while obtaining definitive imaging
Stabilisation Sequence
Rigid collar application in neutral position Log-roll precautions with manual in-line stabilisation Airway management without neck extension if possible Rapid transport to trauma centre with spine capability
Maintain neutral alignment; do not remove collar until CT reviewed CT cervical spine within 30 minutes of arrival Calculate all measurements (Powers, CCI, BDI, BAI) Notify spine team immediately if any threshold exceeded
Type I and III: Gentle closed reduction under fluoroscopy if displaced, then halo or collar Type II: Strict neutral position, no traction attempted All types: Occipitocervical fusion within 24-72 hours once medically optimised
Traction is contraindicated in Type II distraction injuries. Applying weight can increase the longitudinal gap, stretch the brainstem, and cause immediate death. If the CT demonstrates vertical separation, maintain neutral collar or halo without any distractive force. Reduction, if required, is performed surgically after exposure.
SAFEManagement Priorities
Hook:SAFE approach saves lives in atlanto-occipital dislocation!
Complications
- Incidence
- 70-85 percent overall mortality
- Risk Factors
- High-energy mechanism, delayed diagnosis
- Management
- Prevention via early recognition and immobilisation
- Incidence
- 10-20 percent of survivors
- Risk Factors
- Type II distraction, aggressive manipulation
- Management
- CTA confirmation, anticoagulation if dissection
- Incidence
- 5-15 percent
- Risk Factors
- Smoking, osteoporosis, inadequate fixation
- Management
- Revision with extended construct or bone stimulator
- Incidence
- Common in survivors (IX-XII)
- Risk Factors
- Brainstem stretch at time of injury
- Management
- Supportive, may improve over months
- Incidence
- High in upper cervical cord involvement
- Risk Factors
- Phrenic nerve or brainstem injury
- Management
- Prolonged ventilation, tracheostomy
A missed or delayed diagnosis of atlanto-occipital dislocation converts a potentially survivable injury into a fatal one. Every polytrauma patient with a high-energy mechanism must have CT measurements performed and documented. The single most important intervention is rigid neutral immobilisation from the scene onward.
Outcomes and Prognosis
- Survival to Hospital
- 20-30 percent
- Neurological Outcome
- Variable cranial nerve and cord injury
- Long-term Function
- Good with successful fusion and rehabilitation
- Survival to Hospital
- Less than 10 percent
- Neurological Outcome
- High rate of brainstem injury
- Long-term Function
- Poor; most do not survive to surgery
- Survival to Hospital
- Higher relative survival
- Neurological Outcome
- Better ligamentous healing potential
- Long-term Function
- Fusion still required; growth considerations
Best prognosis: Early recognition, Type I or III injury, successful closed reduction, rigid occipitocervical fusion within 72 hours, absence of vertebral artery injury. Poor prognosis: Type II distraction pattern, unconscious at scene, associated severe head injury, delayed diagnosis beyond 24 hours. Key threshold: The first 60 minutes after arrival determine whether the patient reaches the operating theatre alive.
Guidelines, Registries & Global Practice
- Rare but lethal: Represents less than 1 percent of cervical spine injuries but carries the highest mortality
- Adult peak: High-speed motor vehicle collisions in unrestrained occupants
- Paediatric peak: Falls and pedestrian impacts; higher relative incidence than adults
- Survival bias: Most data come from patients who reach trauma centres alive
- High-resource: Immediate CT with multiplanar reconstructions, CTA, and 24-hour spine coverage for fusion
- Limited-resource: Plain films plus clinical assessment; transfer to centre with CT and surgical capability
- Universal principle: Rigid neutral immobilisation from the scene is the single most important intervention worldwide
- Surgery: Modern occipital plating and screw constructs are standard wherever neurosurgical or orthopaedic spine expertise exists
- Diagnosis Emphasis
- CT with CCI, Powers ratio, BDI/BAI on every high-energy trauma
- Initial Management
- Rigid collar or halo in neutral; no traction until type known
- Surgical Timing
- Urgent fusion within 24-72 hours once stable
- Diagnosis Emphasis
- Clinical suspicion plus CT measurements; document all values
- Initial Management
- Log-roll and collar; transfer to major trauma centre if AOD suspected
- Surgical Timing
- Same-day or next-day fusion when patient optimised
- Diagnosis Emphasis
- High index of suspicion in unconscious polytrauma patients
- Initial Management
- ATLS protocol with spine precautions; CT before any manipulation
- Surgical Timing
- Early surgical stabilisation improves survival
There is no dedicated international registry for atlanto-occipital dislocation because of its rarity and high pre-hospital mortality. Evidence is drawn from case series and expert consensus. The consistent message across all guidelines is: maintain neutral rigid immobilisation, obtain CT with measurements immediately, avoid traction in distraction injuries, and proceed to occipitocervical fusion as soon as the patient is medically stable.
Record in every high-energy trauma patient:
- Traynelis type once CT is obtained
- Exact values of Powers ratio, CCI (bilateral), BDI, and BAI
- Decision to avoid traction and rationale
- Time of spine team notification and surgical plan A missed or mismanaged atlanto-occipital dislocation is a recurring source of preventable death and litigation worldwide. Always measure and document the craniocervical parameters on CT.
Controversies & Areas of Uncertainty
Some surgeons attempt gentle closed reduction under fluoroscopy for Type I and III injuries before fusion, while others proceed directly to open reduction and fixation. No randomised data exist; practice is driven by surgeon experience and the degree of initial displacement.
Halo immobilisation provides superior rigidity but carries pin-site and pulmonary complications. Modern screw constructs are so stable that some centres use only a rigid collar for 8-12 weeks. Choice remains institution-dependent.
Standard constructs stop at C2. Extension to C3 is used when C2 bone quality is poor or additional stability is required. No comparative data define the threshold for extension.
CTA is routine, but the decision to anticoagulate a dissected vertebral artery before fusion versus after remains variable. Multidisciplinary discussion with neurosurgery and vascular neurology is recommended.
MCQ Practice Points
Q: What is the most unstable Traynelis type of atlanto-occipital dislocation? A: Type II (longitudinal distraction). Type II produces sequential disruption of all ligamentous tethers and creates the greatest risk of brainstem stretch. Traction is contraindicated because it can complete the distraction and cause immediate cardiorespiratory arrest.
Q: What is the abnormal threshold for the condyle-C1 interval (CCI) on coronal CT? A: 2.5 mm or more. The CCI is measured on the coronal reconstruction between the occipital condyle and the superior articular facet of C1. Values of 2.5 mm or more indicate atlanto-occipital instability and mandate urgent spine consultation. CCI is the most sensitive single measurement in both adults and children.
Q: Why is traction contraindicated in certain atlanto-occipital dislocations? A: Traction risks completing a partial distraction injury (Type II). In longitudinal distraction injuries, the ligaments are already torn in sequence; any additional distractive force can separate the occiput completely from C1, stretching the brainstem and vertebral arteries and causing immediate death. Neutral rigid immobilisation is used instead until surgical fusion.
Q: What is the Powers ratio and what value indicates anterior atlanto-occipital dislocation? A: Powers ratio is basion-posterior C1 arch distance divided by opisthion-anterior C1 arch distance. A ratio greater than 1.0 indicates anterior displacement of the occiput on C1 (Traynelis Type I). Although still taught, modern practice relies on CT measurements (CCI, BDI) because plain-film landmarks are often obscured.
Q: What is the definitive treatment for a survivor of atlanto-occipital dislocation? A: Occipitocervical fusion using an occipital plate with C1 lateral mass and C2 pedicle screws. After anatomic reduction (Types I and III), rigid internal fixation provides immediate stability. Post-operative halo or collar immobilisation for 8-12 weeks is standard. Wiring techniques have been replaced by modern screw-rod constructs with higher fusion rates.
Q: Why must atlanto-occipital dislocation be excluded even after apparently minor trauma in children? A: Children have ligamentous laxity and a larger head-to-body ratio that allows the craniocervical junction to be injured at lower energy than would be required in adults. A normal plain cervical series does not exclude AOD; CT with CCI measurement is mandatory in any child with neck pain or neurological symptoms after trauma.
Clinical Imaging
Craniocervical Junction Anatomy and Injury Patterns
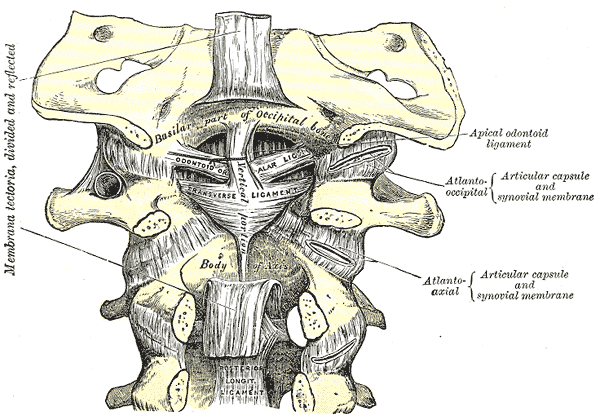
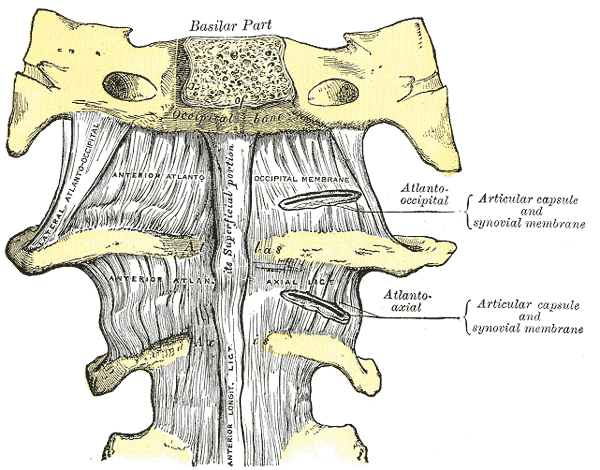
Atlanto-occipital dislocation is fundamentally a soft-tissue (ligamentous) injury: the bony craniocervical junction is intrinsically unstable and relies almost entirely on ligaments. The structures disrupted in AOD - the tectorial membrane, the paired alar ligaments and the apical odontoid ligament - are shown below.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old unrestrained driver is brought in after a high-speed head-on collision. He is unconscious with a Glasgow Coma Scale of 6. He has been placed in a rigid collar. Lateral cervical X-ray shows an increased basion-dens interval. What is your immediate management and suspected diagnosis?”
“A 4-year-old child is brought to the emergency department after a fall from a first-floor balcony. The child is conscious but complains of severe occipital headache and refuses to move the neck. The mechanism seems relatively low energy. Open-mouth and lateral cervical views appear normal. What is your next step?”
Key Anatomy
- Atlanto-occipital joint relies on alar ligaments, apical ligament, tectorial membrane, and capsules
- Occipital condyles articulate with C1 superior facets; disruption allows translation or distraction
- Brainstem and vertebral arteries are immediately at risk with any displacement
- Type II distraction produces the greatest instability and highest mortality
Traynelis Classification
- Type I: Anterior displacement of occiput on C1 (most common survivable pattern)
- Type II: Longitudinal distraction (most unstable; avoid traction)
- Type III: Posterior displacement of occiput on C1
- Classification directly informs reduction strategy and traction safety
Radiographic Diagnosis
- Powers ratio greater than 1.0 indicates anterior dislocation (lateral view or sagittal CT)
- CCI of 2.5 mm or more on coronal CT is the most sensitive single measurement
- BDI greater than 12 mm or BAI greater than 12 mm also abnormal
- CT with multiplanar reconstructions is mandatory; plain films miss up to 50 percent
Immediate Management
- Rigid cervical collar or halo in neutral position from the scene
- Log-roll precautions; secure airway without neck extension if possible
- Urgent CT occiput to T1 with measurements; CTA for vertebral arteries
- Never apply traction before confirming Traynelis type on CT
Definitive Treatment
- Occipitocervical fusion (occipital plate + C1 lateral mass + C2 pedicle screws)
- Achieve anatomic reduction first (Types I and III) under fluoroscopy
- Post-operative halo or rigid collar for 8-12 weeks
- Early fusion (within 72 hours) improves survival in patients who reach hospital
Evidence Base and Key Trials
Traumatic atlanto-occipital dislocation. Case report
- Original description of the three-part classification system still used worldwide
- Type I anterior, Type II longitudinal, Type III posterior displacement patterns
- Emphasised that traction is dangerous in distraction injuries
- Reported that CT is required for accurate diagnosis
The pathological anatomy of fatal atlanto-occipital dislocations
- Described the ligamentous and osseous disruption patterns in fatal AOD cases
- Confirmed that alar ligaments and tectorial membrane failure allow fatal displacement
Atlanto-occipital dislocation: part 1--normal occipital condyle-C1 interval in 89 children
- Established normal condyle-C1 interval (CCI) values from reconstructed CT in 89 children: mean 1.28 mm; no normal joint exceeded 2.5 mm, with marked left-right symmetry and no change with age
- Proposed the CCI (measured on reconstructed CT) as the most reliable indicator of occipito-C1 disruption - abnormal widening or asymmetry signifies AOD
Atlantooccipital dislocation in children: presentation, diagnosis, and management
- Reviewed presentation and management of AOD specifically in the pediatric population
- Highlighted differences in injury patterns and outcomes compared to adults due to ligamentous laxity