Bennett's Fractures
Intra-articular Fracture-Subluxation | Thumb MC Base | AOL Anchors Fragment
FRACTURE PATTERN CLASSIFICATION
Critical Must-Knows
- APL is the main deforming force - pulls shaft dorsally, radially, proximally
- AOL (anterior oblique ligament) keeps volar fragment reduced to trapezium
- Over 1mm articular step = surgical indication
- Reduction: Traction, Abduction, Pressure on MC base (TAP maneuver)
Clinical Pearls
- "Know the difference: Bennett (2-part) vs Rolando (comminuted)
- "K-wire MC1-trapezium is most common fixation method
- "Roberts view = true AP of thumb CMC (hyperpronated thumb)
- "Saddle joint anatomy is FREQUENTLY tested in vivas
Clinical Imaging
Imaging Gallery




Classic Eponymous Fracture
Deforming Forces
APL pulls shaft dorsally/radially and proximally. Adductor pollicis contributes to deformity. These forces make closed reduction unstable.
Key Ligament - AOL
Anterior oblique ligament (beak ligament) is KEY. Keeps volar fragment attached to trapezium. This is why fragment stays reduced.
Quick Decision Guide - Bennett's Fracture Management
| Scenario | Decision | Rationale |
|---|---|---|
| Non-displaced, stable in cast | Consider conservative | Rare - most require fixation |
| Articular step under 1mm after CR | Thumb spica + close follow-up | Must monitor for displacement |
| Articular step over 1mm | Surgical fixation (CRPP or ORIF) | Prevent arthritis |
| Large fragment over 30% | Consider lag screw fixation | Good purchase for compression |
| Small fragment under 15% | K-wire fixation preferred | Screw purchase inadequate |
| Failed closed reduction | Open reduction (Wagner approach) | Direct visualization needed |
| Comminuted pattern (Rolando) | ORIF +/- external fixation | Worse prognosis expected |
| Post-traumatic arthritis | CMC arthrodesis or arthroplasty | Salvage procedure |
Mnemonics and Memory Aids
BENNETTBENNETT for Fracture Features
| B | Base of thumb metacarpal involved |
| E | Edward Bennett described in 1882 |
| N | Not a simple fracture - it's a fracture-subluxation |
| N | Need to reduce - APL pulls shaft dorsally |
| E | Extra-articular fragment stays (AOL intact) |
| T | Thumb function depends on anatomic reduction |
| T | Treatment closed reduction and K-wire or ORIF |
| B | Base of thumb metacarpal involved | N | Need to reduce - APL pulls shaft dorsally | T | Treatment closed reduction and K-wire or ORIF |
| E | Edward Bennett described in 1882 | E | Extra-articular fragment stays (AOL intact) | ||
| N | Not a simple fracture - it's a fracture-subluxation | T | Thumb function depends on anatomic reduction |
Hook:The fracture is named BENNETT - remember what makes it special!
APLAPL for Deforming Forces
| A | Abductor pollicis longus is the key deforming force |
| P | Pulls the shaft Proximally, Laterally (radially) |
| L | Leaves the volar fragment attached to trapezium |
| A | Abductor pollicis longus is the key deforming force |
| P | Pulls the shaft Proximally, Laterally (radially) |
| L | Leaves the volar fragment attached to trapezium |
Hook:APL is the villain - it Abducts, Pulls, and Luxates the thumb!
AOLAOL for Stability
| A | Anterior Oblique Ligament - strongest CMC ligament |
| O | Originates from trapezium to volar MC1 base |
| L | Ligament remains intact, keeping volar fragment reduced |
| A | Anterior Oblique Ligament - strongest CMC ligament |
| O | Originates from trapezium to volar MC1 base |
| L | Ligament remains intact, keeping volar fragment reduced |
Hook:AOL is the hero - it keeps the small fragment at home (Always On Location)
Overview and Epidemiology
Overview
Bennett's fracture is an intra-articular fracture-subluxation of the first carpometacarpal (CMC) joint, first described by Edward Hallaran Bennett in 1882. It represents the most common fracture involving the thumb metacarpal base (approximately 80% of thumb MC base fractures) and is considered an unstable injury due to the powerful deforming forces acting on the thumb. The fracture pattern consists of a small triangular volar-ulnar fragment that remains in anatomic position (held by the intact anterior oblique ligament) while the metacarpal shaft subluxates dorsally and radially, pulled by the abductor pollicis longus (APL). Anatomic reduction is essential to preserve the critical function of the thumb CMC joint and prevent post-traumatic arthritis.
Anatomy and Biomechanics
Anatomy and Biomechanics
Thumb CMC Joint Anatomy
Articular Surfaces:
- Saddle-shaped (bi-concave/bi-convex) joint
- Allows circumduction and opposition
- Most mobile CMC joint in the hand
- Critical for grip strength (accounts for 40% of hand function)
Ligamentous Stabilizers:
| Ligament | Location | Function |
|---|---|---|
| Anterior Oblique (AOL) | Volar-ulnar | PRIMARY STABILIZER - resists dorsal subluxation |
| Dorsoradial (DRL) | Dorsal-radial | Secondary stabilizer |
| Posterior Oblique (POL) | Dorsal-ulnar | Rotational stability |
| Intermetacarpal (IML) | Between MC1-MC2 | Limits abduction |
| Dorsal Intermetacarpal | Dorsal | Limits flexion |
The AOL (Beak Ligament):
- Origin: Volar tubercle of trapezium
- Insertion: Volar-ulnar base of MC1
- Strongest stabilizer of CMC joint
- Remains attached to volar fracture fragment
- This is why the small fragment stays reduced
Muscle Forces
Deforming Forces on Metacarpal Shaft:
- APL: Pulls shaft dorsally and radially (MAIN DEFORMER)
- Adductor pollicis: Pulls shaft ulnarly
- EPL/EPB: Contribute to extension
Result:
- Shaft subluxates dorsal, radial, and proximal
- Volar-ulnar fragment stays anatomic (AOL intact)
- Creates step-off and joint incongruity
Fracture Mechanics
Mechanism:
- Axial load on partially flexed thumb
- Typically from punching, fall on outstretched thumb
- Impact transmitted along thumb ray to CMC joint
Fracture Pattern:
- Two-part fracture (simple Bennett)
- Triangular volar-ulnar fragment (typically small)
- Larger metacarpal shaft fragment (subluxated)
Classification Systems
Classification
Bennett vs Rolando vs Extra-articular
Bennett Fracture (Two-Part):
- Two-part intra-articular fracture
- Volar-ulnar fragment attached to trapezium
- Most common pattern (80%)
Rolando Fracture (Three-Part or Comminuted):
- Comminuted intra-articular fracture
- Y-shaped or T-shaped pattern
- Worse prognosis due to articular damage
Extra-articular Base Fracture:
- Transverse or oblique fracture
- Does not involve CMC joint
- Better prognosis
Bennett's fracture is the most common pattern accounting for approximately 80% of thumb metacarpal base fractures.
Clinical Presentation
Clinical Presentation
History
Mechanism:
- Axial load on flexed thumb (punching)
- Fall onto extended thumb
- Sports injury (skiing, football, rugby)
- Motor vehicle accident
Symptoms:
- Immediate pain at thumb base
- Swelling over thenar eminence
- Inability to grip or pinch
- Thumb deformity (shortened/pronated)
Physical Examination
Inspection:
- Swelling at thenar eminence
- Ecchymosis at thumb base
- Thumb appears shortened
- Possible angulation/deformity
Palpation:
- Point tenderness over CMC joint
- Crepitus with gentle motion
- Assess metacarpal stability
Assessment:
- Document neurovascular status
- Check for associated injuries
- Test thumb opposition (if tolerable)
Key Examination Findings
Positive Grind Test:
- Axial load + rotation at CMC joint
- Produces pain and crepitus
- Indicates CMC pathology
Instability Assessment:
- Compare to contralateral thumb
- Assess dorsal-volar translation
- Document baseline laxity
Investigations
Investigations
Radiographic Assessment
Standard Views:
- PA (Posteroanterior): Oblique view of CMC best
- True Lateral: Shows dorsal subluxation
- Roberts View: Thumb fully pronated, beam perpendicular
- Stress Views: If ligamentous injury suspected
Robert's View Technique:
- Place thumb flat on cassette (hyperpronated)
- Beam perpendicular to thumb MC
- Shows CMC joint in true AP
Radiographic Findings
Key Measurements:
- Articular step-off (greater than 1mm = significant)
- Fragment size (% of articular surface)
- Degree of subluxation
Signs of Bennett's:
- Triangular volar-ulnar fragment at CMC
- Dorsal/radial subluxation of MC shaft
- Widening of CMC joint space
- Overlap of MC1 and trapezium on lateral
CT Imaging
Indications:
- Complex fracture patterns
- Surgical planning
- Assessment of fragment size
- Evaluation of articular congruity
CT Findings:
- Better delineation of fragment size
- Assessment of comminution
- 3D reconstruction for surgical planning
MRI (Rarely Needed)
Indications:
- Suspected ligamentous injury without fracture
- Occult fracture evaluation
- Post-reduction instability
Differential Diagnosis
The painful, swollen thumb base after axial loading has several mimics. The Roberts (true AP) and true lateral views, plus CT where needed, distinguish them.
Differential Diagnosis of the Injured Thumb Base
| Diagnosis | Key distinguishing feature | Why it matters |
|---|---|---|
| Bennett's fracture | Two-part intra-articular fracture with volar-ulnar fragment + dorsoradial shaft subluxation | Unstable; usually needs fixation |
| Rolando fracture | Comminuted T- or Y-shaped intra-articular base fracture | Worse prognosis; harder to fix |
| Extra-articular thumb base fracture | Transverse/oblique fracture sparing the CMC joint | Often managed in a thumb spica cast |
| Pure CMC dislocation | Joint dislocated with no significant bony fragment; ligamentous failure | Reduces but is unstable; needs ligament assessment/repair |
| First MCP ulnar collateral injury (skier's/gamekeeper's thumb) | Tenderness and instability at the MCP joint, not the CMC base | Stener lesion may need surgery; different anatomy |
| Trapezium fracture / scaphoid fracture | Tenderness localised to carpus; CT clarifies | Different fixation and immobilisation |
| Thumb CMC osteoarthritis (acute flare) | Older patient, chronic grind-test pain, osteophytes, no acute fragment | Non-operative or arthroplasty, not fracture fixation |
Management Algorithm
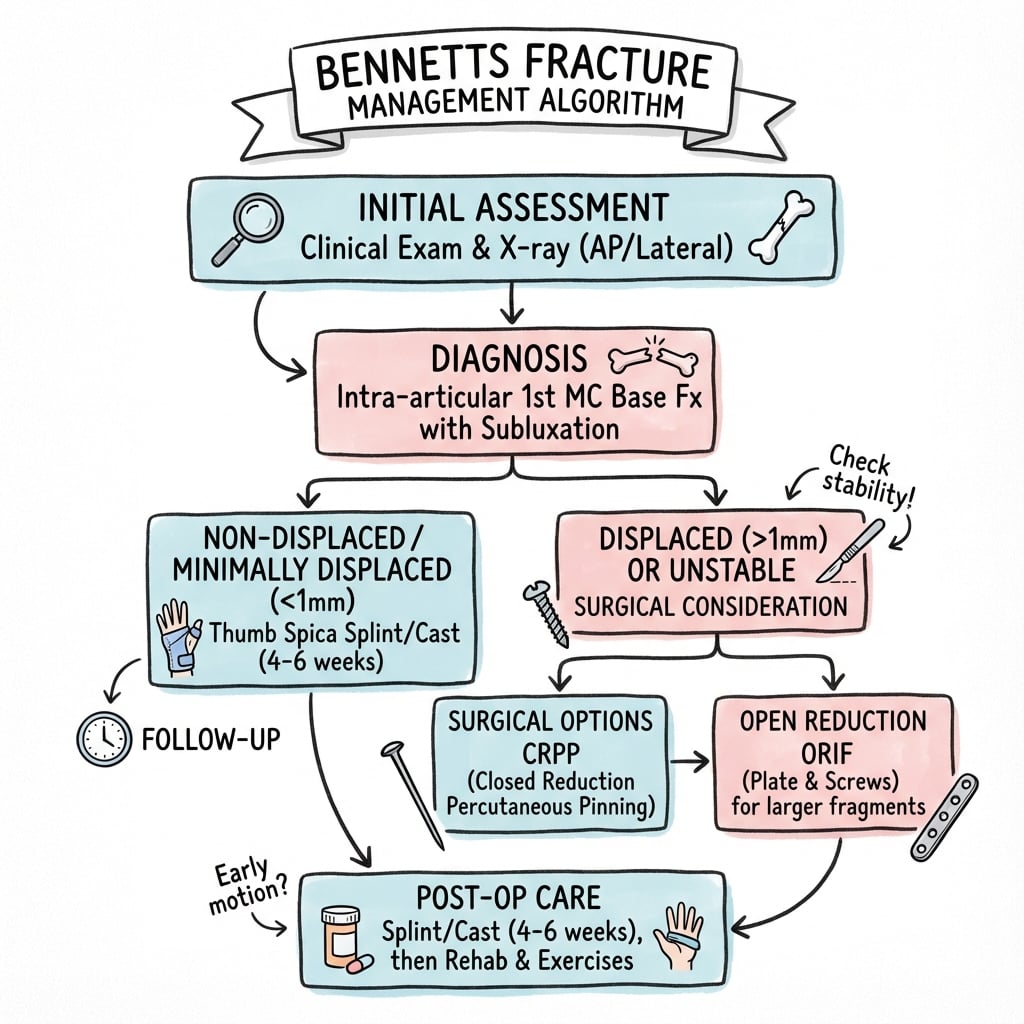
Management
Treatment Goals
- Anatomic articular reduction (less than 1mm step)
- Stable fixation allowing early motion
- Restore CMC joint stability
- Prevent post-traumatic arthritis
Decision-Making and Controversies
- Reduction quality versus fixation method: comparative cohorts and a meta-analysis show CRPP and ORIF give similar arthritis rates and functional scores when an acceptable reduction is achieved; the reduction itself matters more than the construct. [PMID 12631486] [PMID 37929064]
- The under-1 mm dogma is debated: older series tie residual displacement to arthritis [PMID 2307882] [PMID 7714650], yet a 7-year ORIF series found no correlation between reduction accuracy (gap/step under 2 mm) and arthritis [PMID 22438128]. Anatomic reduction remains the sensible goal, but the linear relationship is not absolute.
- ORIF trade-off: ORIF offers modestly higher grip/pinch strength and less adduction deformity, but at a higher complication rate. [PMID 37929064]
- No RCT exists: every recommendation rests on retrospective evidence; individualise by fragment size, reducibility, displacement and patient demand. [PMID 36514567]
Non-Operative Treatment
Indications (Rare):
- Non-displaced fractures (less than 1mm step)
- Perfect reduction maintained in cast
- Elderly/low-demand patients
Technique:
- Closed reduction under fluoroscopy
- Thumb spica cast in slight extension/abduction
- Close radiographic follow-up (weekly x 3)
- Total immobilization 4-6 weeks
Closed Reduction Technique (TAP Maneuver):
- Longitudinal Traction on thumb
- Abduction of thumb ray
- Direct Pressure over MC base (push volar-ulnar)
- Pronation of thumb
- Hold position, apply thumb spica
Problems with Non-Operative:
- High rate of redisplacement
- Difficult to maintain reduction
- Most require surgical stabilization
Non-operative treatment is rarely successful for true Bennett's fractures due to the powerful deforming forces.
Surgical Technique
Surgical Technique
Closed Reduction and Percutaneous K-Wire Fixation
Most Common Technique
Step-by-Step:
- Closed reduction under fluoroscopy
- K-wire (1.1-1.4mm) through MC1 into trapezium
- May add second K-wire through fragment
- Or pin MC1 to MC2 (prevents redisplacement)
- Protect with thumb spica
- Remove wires at 4-6 weeks
K-Wire Options:
- MC1 to trapezium: Direct joint stabilization
- MC1 to MC2: Indirect stabilization
- Through fragment: Fragment fixation (if large enough)

K-Wire Placement Tips
Avoid placing wires too close to articular surface. Entry point should be proximal enough to avoid CMC joint penetration. Fluoroscopy in multiple planes is essential.
Complications
Complications
Early Complications
Malreduction:
- Most common complication
- Greater than 1mm step leads to arthritis
- May require revision surgery
Pin Site Infection:
- Occurs in 2-5% of K-wire cases
- Usually superficial
- Treat with oral antibiotics
- Early wire removal if deep infection
Loss of Reduction:
- More common with conservative treatment
- May occur after wire removal
- Close radiographic follow-up essential
Late Complications
Post-Traumatic Arthritis:
- Most significant long-term complication
- Risk increases with articular incongruity
- May require CMC arthrodesis or arthroplasty
- Incidence: 20-30% at long-term follow-up
Stiffness:
- Common, especially after prolonged immobilization
- Early motion when fracture stable
- Hand therapy essential
Weakness:
- Grip and pinch strength affected
- Usually recovers over 6-12 months
- May have persistent subtle weakness
CMC Instability:
- Ligamentous incompetence after healing
- May require ligament reconstruction
- Rare if fracture anatomically reduced
Malunion:
- Results from inadequate reduction
- Causes altered CMC mechanics
- May accelerate arthritic change
- Corrective osteotomy rarely indicated
Postoperative Care
Postoperative Care
Timeline
| Phase | Timeframe | Focus |
|---|---|---|
| Protection | Weeks 0-4/6 | Immobilization, swelling control |
| Early Motion | Weeks 4/6-8 | K-wire removal, gentle ROM |
| Strengthening | Weeks 8-12 | Progressive grip/pinch |
| Return to Activity | 12+ weeks | Sport-specific, full function |
Immobilization Protocol
Post-Op Care:
- Thumb spica splint/cast for 4-6 weeks
- Protect pin sites if K-wires present
- Elevation and ice for initial swelling
- Regular neurovascular checks
Pin Site Care:
- Daily cleaning with normal saline or dilute betadine
- Monitor for signs of infection (erythema, drainage)
- No submersion in water
- Patient education on warning signs
Proper immobilization and pin site care are essential for preventing complications.
Outcomes and Prognosis
Outcomes and Prognosis
Prognostic Factors
Good Prognosis:
- Anatomic reduction (less than 1mm step)
- Small articular fragment
- Young patient
- Early treatment
- Stable fixation
Poor Prognosis:
- Articular step greater than 2mm
- Large fragment involvement
- Delayed treatment
- Associated soft tissue injury
- Comminuted pattern (Rolando)
Long-Term Results
Anatomic Reduction:
- 80-90% good/excellent results
- Low rate of symptomatic arthritis
- Near-normal grip/pinch strength
Non-Anatomic Reduction:
- 50-60% good results
- Higher rate of arthritis
- May require salvage procedure
Comparison to Rolando Fracture
| Factor | Bennett's | Rolando |
|---|---|---|
| Pattern | 2-part | Comminuted |
| Fixation | Easier | More difficult |
| Prognosis | Better | Worse |
| Arthritis Rate | 20% | 40-50% |
Evidence Base
Evidence Base
The contemporary evidence base for Bennett's fracture is built almost entirely on retrospective cohorts and two systematic reviews — there is no randomised controlled trial. The recurring themes are that (1) the quality of articular reduction historically correlated with long-term arthrosis, (2) open and closed techniques give broadly similar functional outcomes when an acceptable reduction is achieved, and (3) cast-only management gives poor long-term results.
Reduction Quality and Post-Traumatic Arthritis
- 41 Bennett's fractures reviewed at a median 7.3 years
- Symptom-free in 15 of 18 fractures healed in excellent position versus only 6 of 13 with residual displacement
- Radiographic arthritis in 3 of 14 with excellent reduction versus 7 of 10 with residual displacement
One-Millimetre Threshold — Medium-to-Long-Term Review
- 76 Bennett's fractures; 21 reviewed at mean 7 years 7 months
- Fractures healing with up to 1 mm displacement had superior clinical and radiological results
- Only 1 of 76 patients required later CMC fusion
- The method of achieving and holding reduction was 'immaterial' provided under-1 mm displacement was obtained
Non-Operative Treatment — 13-Year Follow-Up
- 20 of 22 cast-treated Bennett's fractures followed to 13 years
- 18 of 20 subjectively satisfactory, but 7 had radiographic CMC arthrosis (2 severe and painful)
- Non-anatomic reduction present in 6 of the 7 patients who developed arthrosis
Conservative Management — 26-Year Follow-Up
- 17 conservatively (cast-only) treated fracture-dislocations reviewed at mean 26 years
- All had reduced range of movement and grip strength; 12 had a characteristic hand deformity
- Persistent CMC subluxation with marked degenerative change on radiographs
CRPP versus ORIF — Comparative Cohort
- 32 single-large-fragment Bennett's fractures; ORIF versus closed transarticular K-wiring; mean 7-year follow-up
- Treatment type did not influence clinical outcome or prevalence of radiological arthritis
- The percutaneous group had a significantly higher incidence of first-metacarpal adduction deformity, attributed to wire placement near the fracture line
Open Reduction and Screw Fixation — 7-Year Outcomes
- 24 Bennett's fractures fixed with lag screws; mean follow-up 83 months
- Reduction maintained in 96% when two lag screws were used
- Pinch and grip strength about 92% and 89% of the contralateral side at 4 months
- No correlation between reduction accuracy (gap/step under 2 mm) and development of arthritis in this series
ORIF versus Closed Reduction — Systematic Review and Meta-Analysis
- Six retrospective studies pooled (no RCTs available)
- ORIF associated with higher grip and pinch strength, better thumb extension/flexion and smaller mean adduction deformity
- No difference in post-traumatic arthritis or functional scores
- Higher complication rate with ORIF
Systematic Review of Management Outcomes
- PRISMA review of 13 studies and 558 patients (439 operative, 119 conservative)
- Post-traumatic osteoarthritis reported in 50 of 558 (9%) where stated; pain in 13%; reoperation in 2%; no nonunion
- No randomised controlled trial exists; heterogeneity precluded a single recommendation
Viva Questions
Viva Scenarios
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
"A 28-year-old male presents after punching a wall with a painful swollen thumb. X-rays show a Bennett's fracture with 2mm subluxation. How would you manage this patient?"
Key Discussion Points:
- Bennett's is a fracture-SUBLUXATION - not just a fracture
- Deforming force is APL pulling shaft dorsal/radial
- Volar fragment held by AOL (anterior oblique ligament)
- Greater than 1mm step is surgical indication
- K-wire options: MC1-trapezium (direct), MC1-MC2 (indirect)
- Must achieve anatomic reduction to prevent arthritis
- Post-traumatic arthritis occurs in 20-30% even with good reduction
"Describe the anatomy of the thumb CMC joint and explain why Bennett's fracture is inherently unstable."
Key Discussion Points:
- Thumb CMC is a saddle joint (biconcave-biconvex) allowing circumduction
- Key stabilizer is AOL (anterior oblique ligament) - strongest ligament
- AOL attaches to volar-ulnar MC1 base
- In Bennett's, AOL keeps volar fragment reduced to trapezium
- APL inserts on dorsal MC1 base - pulls shaft dorsal, radial, proximal
- Adductor pollicis pulls shaft ulnarly
- Result: shaft subluxates while volar fragment stays anatomic
- Instability from loss of bony buttress against APL pull
- Joint incongruity leads to post-traumatic arthritis
"You attempt closed reduction of a Bennett's fracture under fluoroscopy but cannot achieve anatomic reduction. What are your options and considerations?"
Key Discussion Points:
- Reasons for irreducibility: interposed soft tissue, fragment rotation, inadequate traction
- Open reduction through Wagner (volar-radial) approach
- Protect: radial artery (terminal branch), superficial radial nerve
- Fixation based on fragment size: screws if greater than 30%, K-wires if smaller
- Lag screw technique for compression across fracture
- Always consider supplemental MC1-trapezium wire for stability
- Arthroscopic-assisted reduction is alternative if available
- Goal remains less than 1mm articular step
MCQ Practice Points
MCQ Practice Points
Ligament Anatomy
Q: Which ligament keeps the volar-ulnar fragment of a Bennett's fracture reduced to the trapezium?
A: Anterior Oblique Ligament (AOL) - Also called the "beak ligament." This is the primary stabilizer of the thumb CMC joint and attaches to the volar-ulnar base of the first metacarpal. Because this ligament remains intact, the small triangular fragment stays in anatomic position.
Deforming Forces
Q: What is the main deforming force in a Bennett's fracture and in which direction does it displace the metacarpal shaft?
A: Abductor Pollicis Longus (APL) is the main deforming force. It pulls the metacarpal shaft dorsally, radially, and proximally. Secondary deforming forces include adductor pollicis and the extensor pollicis muscles.
Surgical Threshold
Q: What is the articular step-off threshold for surgical intervention in Bennett's fracture?
A: Greater than 1mm of articular step-off is the accepted threshold for surgical intervention. Studies have shown that articular incongruity of more than 1mm is associated with significantly higher rates of post-traumatic arthritis at long-term follow-up.
Radiographic View
Q: What is the Roberts view and why is it useful for evaluating Bennett's fractures?
A: The Roberts view is a true AP view of the thumb CMC joint obtained by placing the thumb flat on the cassette (hyperpronated) with the beam perpendicular to the metacarpal. It provides the best view of the CMC joint and accurately shows the articular step-off and subluxation.
Bennett vs Rolando
Q: What is the key difference between a Bennett's fracture and a Rolando fracture?
A: Bennett's fracture is a two-part intra-articular fracture-subluxation with a small volar-ulnar fragment. Rolando fracture is a comminuted (three-part or more) intra-articular fracture with a Y or T pattern. Rolando fractures have a worse prognosis due to greater articular destruction.
Fixation Method
Q: A patient has a Bennett's fracture with a fragment involving 10% of the articular surface. What is the preferred fixation method?
A: Percutaneous K-wire fixation is preferred for small fragments. K-wires from MC1 to trapezium (direct) and/or MC1 to MC2 (indirect) provide adequate stabilization. Screw fixation is not ideal for small fragments due to inadequate purchase and risk of fragmentation.
Guidelines, Registries & Global Practice
Guidelines, Registries & Global Practice
Bennett's fracture is a worldwide injury with a remarkably consistent demographic profile. The discussion below frames the global standard of care plus the regional nuances a candidate may be examined on, irrespective of board.
Global Epidemiology
Hand fractures are among the most common skeletal injuries. In a population-based study of approximately 4 million people, the annual incidence of hand fracture was around 36 per 10,000, of which roughly 42% involved the metacarpals, with a male-to-female relative risk of about 2:1 and a peak in young men aged 15–40 years. [PMID 16945705]
| Feature | Typical pattern |
|---|---|
| Most common thumb metacarpal base fracture | Bennett's (~80% of base fractures) |
| Peak demographic | Young men, 15–40 years |
| Classic mechanisms | Axial load on partially flexed thumb (punch), fall, contact and ball sports |
| Functional stake | Thumb CMC contributes substantially to overall hand function |
Major Guidance & Society Positions (Side by Side)
| Source / Region | Position on Bennett's Fracture | Evidence Level |
|---|---|---|
| AO Foundation (global) | Anatomical reduction of the articular surface and stable fixation; CRPP for most, ORIF (lag screw) for larger or irreducible fragments | Expert consensus / Level IV-V |
| BOA / BSSH (UK) | Displaced intra-articular thumb base fractures are unstable and warrant reduction and fixation; refer to hand/trauma service | Consensus, low-level evidence |
| AAOS / ASSH (US) | Operative stabilisation for displaced fracture-subluxation; CRPP and ORIF both acceptable | Consensus, retrospective evidence |
| Systematic reviews (Daher 2023, Goru 2022) | No RCT exists; ORIF may give modest strength/alignment gains with more complications; no single best treatment | Level III (pooled retrospective) |
The Honest Evidence Position
There is no randomised controlled trial in Bennett's fracture. Guidance from the AO Foundation, BOA/BSSH and AAOS/ASSH is broadly concordant — reduce the joint, fix it stably — but rests on retrospective cohorts and two systematic reviews. The historical teaching that under-1 mm reduction prevents arthritis (Kjaer-Petersen, Thurston) is challenged by series showing no clear reduction–arthritis correlation (Leclère). State the controversy explicitly in a viva. [PMID 2307882] [PMID 8297298] [PMID 22438128]
Registry & Practice-Trend Evidence
Bennett's fractures are not tracked by joint-replacement registries (which cover arthroplasty), so evidence derives from national fracture cohorts and administrative datasets rather than implant registries. Population-level analyses report a clear secular trend away from closed reduction toward open reduction and internal fixation of metacarpal and phalangeal fractures over the past two decades, reflecting wider availability of fine fragment fixation and hand-surgery expertise. [PMID 35785509]
Global Practice Variation
- High-resource settings: ready access to fluoroscopy, fine K-wires/screws and arthroscopy; increasing use of ORIF and arthroscopic-assisted reduction.
- Limited-resource settings: closed reduction and percutaneous K-wiring predominate — low cost, widely available, and supported by evidence that technique matters less than reduction quality (Thurston). [PMID 8297298]
- Athletes / manual workers: lower threshold for stable internal fixation to allow earlier protected mobilisation and predictable return to work or sport.
- Elderly / low-demand patients: a degree of residual displacement may be accepted, balancing arthritis risk against surgical morbidity.
Exam Cheat Sheet
Exam Day Cheat Sheet
Bennett's Fractures - Key Points
Clinical summary
Definition
- •Intra-articular fracture-SUBLUXATION of thumb MC base
- •Two-part: volar-ulnar fragment + subluxated shaft
- •NOT the same as Rolando (which is comminuted)
- •Instability defined by dorsal/radial shaft migration
Key Anatomy
- •AOL (anterior oblique ligament) = primary stabilizer
- •AOL keeps volar fragment attached to trapezium
- •APL = main deforming force (pulls dorsal/radial/proximal)
- •Thumb CMC = saddle joint (40% of hand function)
Surgical Indications
- •Articular step greater than 1mm
- •Subluxation that cannot be reduced closed
- •Unstable after closed reduction
- •Rotational malalignment (rare but possible)
Fixation Options
- •K-wire MC1 to trapezium (most common)
- •K-wire MC1 to MC2 (indirect)
- •Lag screw (if fragment large enough)
- •ORIF via Wagner approach if closed fails
Complications
- •Post-traumatic arthritis (20-30%)
- •Malreduction
- •Stiffness
- •Pin site infection
Quick Reference: Key Numbers
| Parameter | Value |
|---|---|
| Articular step threshold | greater than 1mm = surgery |
| CMC contribution to hand function | 40% |
| Thumb spica duration | 4-6 weeks |
| K-wire removal | 4-6 weeks |
| Arthritis rate (anatomic reduction) | 20% |
| Arthritis rate (non-anatomic) | 50%+ |
| Return to full activity | 10-12 weeks |