Lumbosacral Transitional Vertebra | Castellvi Classification | Symptomatic LSTV
CASTELLVI CLASSIFICATION
Critical Must-Knows
- LSTV = Lumbosacral Transitional Vertebra - sacralization of L5 or lumbarization of S1
- Castellvi classification based on transverse process morphology (I-IV, a/b for unilateral/bilateral)
- Type II (pseudoarticulation) most associated with symptomatic Bertolotti syndrome
- Pain sources: anomalous articulation, contralateral facet, above-level disc degeneration
- Diagnosis: Ferguson view X-ray, CT for bony detail, MRI for disc assessment
Clinical Pearls
- "Named after Mario Bertolotti (1917) - Italian radiologist
- "May cause miscounting of vertebral levels - critical for surgical planning
- "Contralateral facet arthropathy common with unilateral LSTV
- "L4-L5 disc more commonly degenerates when L5 is sacralized (reduced motion at L5-S1)
Clinical Imaging
Imaging Gallery



Critical Bertolotti Syndrome Exam Points
Castellvi Classification
Type I: Dysplastic TP (≥19mm width). Type II: Incomplete fusion (pseudoarticulation). Type III: Complete fusion. Type IV: II on one side, III on other. Suffix a=unilateral, b=bilateral.
Pain Sources
Four pain generators: 1) Anomalous articulation itself (pseudoarthrosis), 2) Contralateral facet overload, 3) Above-level disc degeneration (especially L4-L5), 4) Extraforaminal nerve compression by enlarged TP.
Level Counting
Critical for surgery: LSTV can cause vertebral miscounting. Always use whole-spine imaging or identify C2 to count down. Operating on wrong level is a major medicolegal issue.
Treatment Approach
Injection first: Diagnostic/therapeutic injection into pseudoarticulation. Surgery: Resection of anomalous articulation, or fusion of L5-S1. Address above-level disc if symptomatic.
Castellvi Classification of LSTV
| Type | Description | Clinical Significance |
|---|---|---|
| Ia | Unilateral dysplastic TP (≥19mm) | Usually asymptomatic |
| Ib | Bilateral dysplastic TP | Usually asymptomatic |
| IIa | Unilateral pseudoarticulation | Most commonly symptomatic |
| IIb | Bilateral pseudoarticulation | Symptomatic, both sides may hurt |
| IIIa | Unilateral complete fusion | Contralateral facet/disc issues |
| IIIb | Bilateral complete fusion | Above-level disc disease |
| IV | IIa on one side, IIIa on other | Complex - address pseudoarthrosis side |
LSTV - CLSTV - Classification Types
| L | Large TP (Type I) Dysplastic transverse process ≥19mm |
| S | Semi-fused (Type II) Pseudoarticulation - incomplete fusion |
| T | Totally fused (Type III) Complete bony fusion to sacrum |
| V | Variable (Type IV) Type II one side, Type III other |
| L | Large TP (Type I) Dysplastic transverse process ≥19mm | T | Totally fused (Type III) Complete bony fusion to sacrum |
| S | Semi-fused (Type II) Pseudoarticulation - incomplete fusion | V | Variable (Type IV) Type II one side, Type III other |
Hook:LSTV types progress from Large to Semi to Total fusion, Variable is mixed
PAIN - SPAIN - Sources of Bertolotti Pain
| P | Pseudoarticulation Anomalous joint itself degenerates |
| A | Arthrosis (contralateral facet) Overload of facet opposite to LSTV |
| I | Intervertebral disc (above) L4-L5 disc degenerates faster |
| N | Nerve (extraforaminal) L5 nerve compressed by enlarged TP |
| P | Pseudoarticulation Anomalous joint itself degenerates | I | Intervertebral disc (above) L4-L5 disc degenerates faster |
| A | Arthrosis (contralateral facet) Overload of facet opposite to LSTV | N | Nerve (extraforaminal) L5 nerve compressed by enlarged TP |
Hook:PAIN sources help target treatment - identify the pain generator
COUNT - LCOUNT - Level Identification
| C | Cervical start Count from C2 down on whole-spine imaging |
| O | Occiput to sacrum Use full spine scout |
| U | Use ribs T12 has free-floating ribs |
| N | Note iliac crests L4 at level of iliac crests |
| T | Transitional findings Document clearly in operative plan |
| C | Cervical start Count from C2 down on whole-spine imaging | N | Note iliac crests L4 at level of iliac crests |
| O | Occiput to sacrum Use full spine scout | T | Transitional findings Document clearly in operative plan |
| U | Use ribs T12 has free-floating ribs |
Hook:COUNT carefully to avoid wrong-level surgery
Overview and Epidemiology
Bertolotti Syndrome refers to symptomatic low back pain caused by a lumbosacral transitional vertebra (LSTV). Named after Mario Bertolotti, an Italian radiologist who described the condition in 1917.
Definition:
A lumbosacral transitional vertebra is a congenital anomaly where the lowest lumbar vertebra (usually L5) has features of a sacral vertebra (sacralization), or the first sacral segment has features of a lumbar vertebra (lumbarization).
Epidemiology:
| Factor | Details |
|---|---|
| LSTV Prevalence | 4-35% (varies by population and definition) |
| Symptomatic rate | Only minority of LSTV are symptomatic |
| Age of presentation | Usually 20s-30s (younger than typical LBP) |
| Gender | No clear predominance |
Key Concept:
Not all LSTVs cause symptoms. Bertolotti syndrome specifically refers to symptomatic LSTV. The challenge is determining whether the LSTV is the pain generator in a patient with low back pain.
Sacralization vs Lumbarization
Sacralization = L5 takes on sacral characteristics (more common). Lumbarization = S1 takes on lumbar characteristics. Both can cause Bertolotti syndrome. The distinction is less important clinically than identifying whether the transition is symptomatic.
Anatomy of Lumbosacral Transition
Normal Lumbosacral Anatomy
L5 Vertebra:
- Largest vertebral body
- Short, broad transverse processes
- Wide intervertebral foramen
- Articulates with S1 via disc and facets
Sacral Ala:
- Lateral wing of S1
- Provides surface for SI joint
- Normal gap between L5 TP and sacral ala
LSTV Morphology
Type I - Dysplastic Transverse Process:
The transverse process is enlarged (≥19mm craniocaudal width) but does not articulate with the sacrum. This is considered a forme fruste of transitional vertebra.
Type II - Pseudoarticulation:
The enlarged transverse process forms a diarthrodial (synovial) joint with the sacral ala. This joint can develop degenerative changes similar to other synovial joints.
| Feature | Description |
|---|---|
| Joint space | Present between TP and sacrum |
| Cartilage | Articular cartilage present |
| Degeneration | Osteoarthritis can develop |
| Motion | Limited motion possible |
Type III - Complete Fusion:
The transverse process is completely fused to the sacral ala. No motion exists at this segment, concentrating stress at the level above.
Type IV - Mixed:
One side has pseudoarticulation (Type II), the other has complete fusion (Type III). This creates asymmetric biomechanics.
Biomechanical Implications
Motion Segment Changes:
When L5 is partially or completely incorporated into the sacrum, the L4-L5 disc becomes the functional lumbosacral junction. This disc experiences increased stress and is prone to early degeneration.
| Normal Spine | LSTV (Sacralized L5) |
|---|---|
| L5-S1 is lumbosacral junction | L4-L5 becomes functional junction |
| 5 mobile lumbar segments | 4 mobile lumbar segments |
| Load distributed normally | Concentrated at L4-L5 |
Contralateral Stress:
With unilateral LSTV (types a), the contralateral facet joint bears increased load due to asymmetric stiffness. This leads to contralateral facet arthropathy.
Pathophysiology
Embryology
Development:
LSTVs result from errors in vertebral segmentation during embryonic development. The HOX genes control segmentation of the axial skeleton. Mutations or variations in HOX gene expression can lead to transitional morphology.
Pain Mechanisms
Four Pain Generators:
Anomalous Articulation Pain
Mechanism: The pseudoarticulation between the enlarged transverse process and sacral ala is a true diarthrodial joint with articular cartilage. Over time, this joint develops degenerative changes.
Characteristics:
- Located at L5-sacrum junction
- Mechanical pain with loading
- May have inflammatory component
Diagnosis:
- Tenderness over pseudoarticulation
- Diagnostic injection provides relief
- CT shows joint degeneration
This is the primary pain generator in Type II LSTV and the target for injection or surgical treatment.
Natural History
Many LSTVs are asymptomatic and discovered incidentally. Symptomatic patients typically present in their 20s-30s, earlier than typical degenerative low back pain. The condition may wax and wane, with some patients having prolonged symptom-free periods.
Classification
Castellvi Classification (1984)
The Castellvi classification, described in 1984, remains the standard system for classifying LSTVs based on the morphology of the transverse process and its relationship to the sacrum.
| Type | Description | Subtype |
|---|---|---|
| I | Dysplastic TP ≥19mm width | a = unilateral, b = bilateral |
| II | Pseudoarticulation (incomplete fusion) | a = unilateral, b = bilateral |
| III | Complete osseous fusion | a = unilateral, b = bilateral |
| IV | Type II on one side, Type III on other | - |
Clinical Correlation
Dysplastic Transverse Process
Morphology: Enlarged transverse process measuring ≥19mm in craniocaudal dimension, but no articulation or fusion with the sacrum. Subtype Ia is unilateral, Ib is bilateral.
Clinical Significance: Usually asymptomatic and often an incidental finding on imaging. May be a predisposing factor for low back pain in some patients but generally considered a "forme fruste" (incomplete form) without clinical significance.
Management: Observation and reassurance. If symptomatic, consider other pain generators before attributing symptoms to Type I LSTV.
Level Identification
Critical Importance:
LSTV can cause confusion in vertebral counting. A sacralized L5 may be counted as S1, leading to wrong-level surgery.
Methods to Identify Correct Level:
- Whole-spine imaging - Count from C2 down
- Identify T12 - Last rib-bearing vertebra
- Iliac crest reference - Usually at L4 body
- Rib counting on CT - Count from T1 down
- Document clearly - Pre-operative planning essential
Wrong-Level Surgery Risk
LSTV is a common cause of wrong-level spinal surgery. Always use multiple methods to confirm vertebral level. Document the transitional anatomy in operative reports. Consider intraoperative confirmation with imaging.
Clinical Presentation
History
Pain Characteristics:
| Feature | Bertolotti Pattern |
|---|---|
| Location | Low back, may lateralize to side of LSTV |
| Character | Deep, aching, mechanical |
| Aggravating | Extension, rotation, prolonged standing |
| Age onset | Often 20s-30s (younger than typical DDD) |
| Radiation | May have L5 radicular symptoms if nerve compressed |
Important History Points:
- Duration and onset (often chronic, insidious)
- Previous imaging showing LSTV
- Failed treatments
- Radicular symptoms (suggests nerve involvement)
- Presence of leg symptoms (disc vs LSTV)
Physical Examination
Inspection:
- May have mild scoliosis (especially unilateral LSTV)
- Normal lumbar lordosis usually
Palpation:
- Tenderness over pseudoarticulation (lateral to midline)
- May be difficult to differentiate from SI joint tenderness
- Contralateral facet tenderness if overloaded
Range of Motion:
- Extension often painful
- Rotation to affected side may reproduce pain
- Flexion usually less painful
Neurological Examination:
- Usually normal
- If L5 radiculopathy: weak ankle dorsiflexion, altered sensation L5 dermatome
- Check for extraforaminal compression signs
Special Tests:
| Test | Technique | Significance |
|---|---|---|
| Single leg extension | Extension on one leg | Reproduces pain on affected side |
| FABER test | May be positive | Overlaps with SI joint testing |
| Straight leg raise | Usually negative | Positive suggests disc herniation |
Red Flags
Rule out serious pathology. Bertolotti syndrome should be mechanical pain without red flags.
Investigations
Imaging Protocol
X-ray (First Line):
| View | Purpose |
|---|---|
| AP Lumbar | Shows TP morphology, may see LSTV |
| Lateral | Disc heights, overall alignment |
| Ferguson view | Angled AP view (30-35°) - best for LSTV |
| Oblique | Facet joints, pars interarticularis |
The Ferguson view (AP with 30-35° cephalad tilt) provides the best visualization of the lumbosacral junction and LSTV.
CT Scan:
Best modality for bony detail of LSTV.
| Assessment | CT Findings |
|---|---|
| Castellvi type | Precisely defines type I-IV |
| Pseudoarthrosis | Joint space, sclerosis, cysts |
| Fusion | Complete vs incomplete |
| Nerve foramina | Extraforaminal stenosis |
MRI:
| Assessment | MRI Findings |
|---|---|
| Disc pathology | Degeneration, herniation at L4-L5 |
| Bone marrow edema | Active inflammation at pseudoarthrosis |
| Nerve root | Compression, inflammation |
| Facet joints | Effusion, degeneration |
Diagnostic Injection
Pseudoarthrosis Injection:
This is both diagnostic and therapeutic. Response to injection helps confirm LSTV as pain source.
Technique:
- CT or fluoroscopic guidance
- Needle into pseudoarticulation
- Inject local anesthetic and steroid
Interpretation:
- Greater than 50% relief = positive (LSTV is pain source)
- Partial relief = may have multiple pain generators
- No relief = consider other diagnosis
Other Injections:
- Facet injection (contralateral side) if facet suspected
- Selective nerve root block if radiculopathy
Laboratory Studies
Not typically required. If concern for inflammatory arthropathy, check:
- ESR, CRP
- HLA-B27 (spondyloarthropathy)
Management
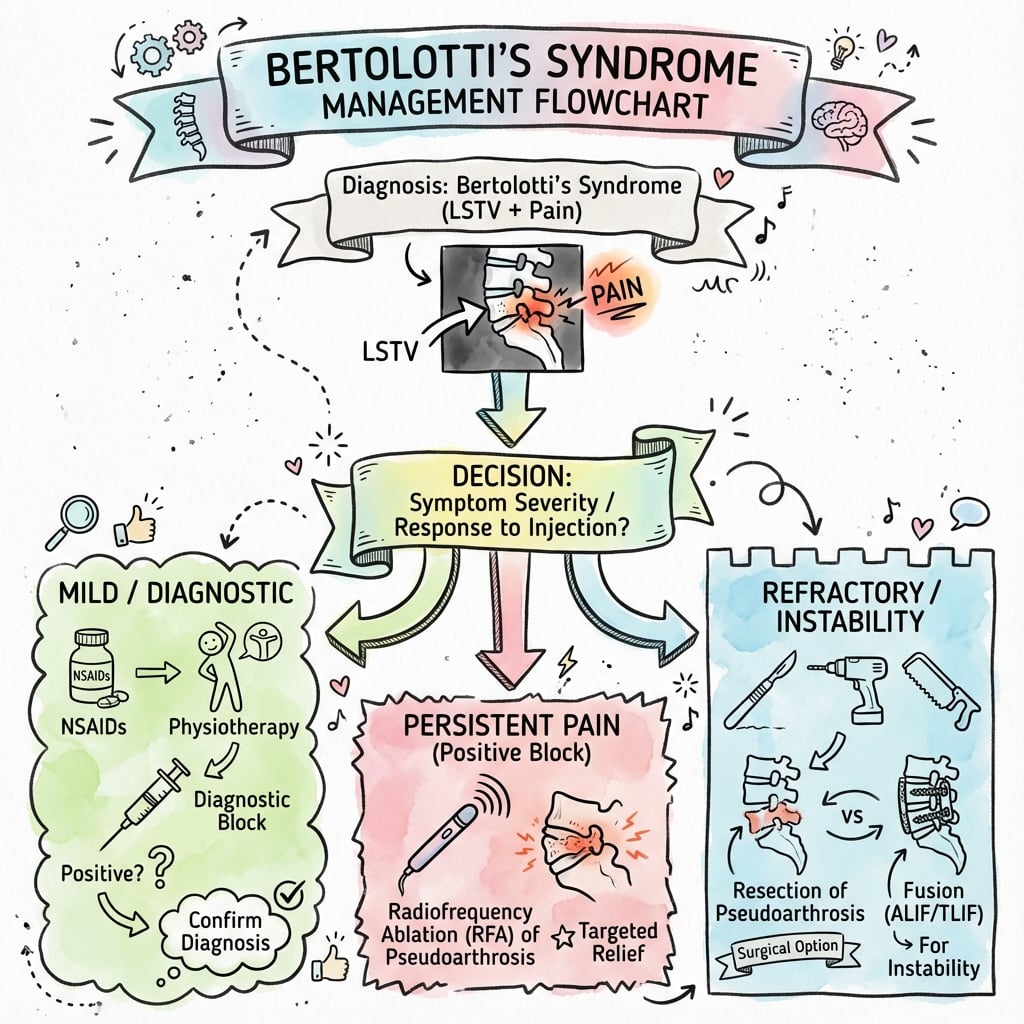
Treatment Algorithm
Conservative Management (First Line):
| Intervention | Details |
|---|---|
| Activity modification | Avoid aggravating positions |
| NSAIDs | First-line pharmacotherapy |
| Physical therapy | Core strengthening, flexibility |
| Weight management | Reduce spinal loading |
Duration: Trial of 6-12 weeks before interventional treatment.
Injection Therapy:
Indications:
- Failed conservative management
- Diagnostic confirmation
- Therapeutic trial
Options:
- Pseudoarthrosis injection (primary target in Type II)
- Contralateral facet injection (if facet pain suspected)
- Selective nerve root block (if radiculopathy)
Surgical Management
Indications:
- Failed conservative and injection therapy
- Confirmed LSTV as pain source (positive diagnostic injection)
- Significant functional impairment
Surgical Options:
Anomalous Articulation Resection
Concept: Remove the enlarged transverse process and pseudoarthrosis, eliminating the pain generator while preserving motion.
Technique:
- Posterior or posterolateral approach
- Identify the enlarged transverse process
- Resect TP and pseudoarticulation
- Decompress L5 nerve if compressed
- No fusion required
Advantages:
- Motion-preserving
- Addresses primary pathology
- Less morbidity than fusion
Outcomes: 70-85% good to excellent results reported in appropriate patients with positive diagnostic injection.
Surgical Selection
For Type II LSTV with positive pseudoarthrosis injection, resection of the anomalous articulation is the preferred first-line surgical treatment. Fusion is reserved for failed resection, Type III with disc disease, or when instability is present.
Complications
Conservative/Injection Complications
Injection-Related:
- Infection (rare)
- Bleeding
- Nerve injury
- Steroid side effects
Surgical Complications
Resection:
- L5 nerve injury (proximity to pseudoarthrosis)
- Incomplete resection (recurrent pain)
- Instability (rare if technique appropriate)
- Wound complications
Fusion:
- Pseudarthrosis
- Hardware failure
- Adjacent segment disease
- Nerve injury
- Infection
Wrong-Level Surgery
This is a particular risk with LSTV due to difficulty in level counting.
Prevention:
- Whole-spine imaging pre-operatively
- Multiple methods to confirm level
- Intraoperative imaging confirmation
- Clear documentation of transitional anatomy
Differential Diagnosis
Bertolotti syndrome is a diagnosis of attribution: an LSTV is present in a substantial minority of the population, so the key task is distinguishing LSTV-driven pain from overlapping causes of mechanical low back and buttock pain. A positive diagnostic injection into the pseudoarticulation is the single most useful discriminator.
Differentiating Bertolotti Syndrome from Mimics
| Condition | Typical Pattern | Key Discriminator |
|---|---|---|
| Bertolotti (symptomatic LSTV) | Young adult, paramedian pain over pseudoarticulation, worse on extension/ipsilateral bending | Pseudoarticulation injection gives over 50% relief; CT confirms Castellvi II/IV |
| Sacroiliac joint dysfunction | Pain below L5, FABER/thigh-thrust positive, overlapping territory | SI-joint block (not pseudoarticulation block) relieves pain |
| Facet (zygapophyseal) arthropathy | Older patient, extension-rotation pain, paramedian | Medial branch block / facet injection relieves; degenerate facets on CT |
| Discogenic / above-level disc disease | Flexion- and sitting-aggravated axial pain | Concordant discography or HIZ/Modic at L4-L5 on MRI |
| L5 radiculopathy (extraforaminal) | Dorsiflexion weakness, L5 dermatomal symptoms, often negative SLR | CT/MRI shows enlarged TP narrowing the far-lateral zone; selective L5 block |
| Axial spondyloarthritis | Inflammatory back pain, morning stiffness, raised CRP, HLA-B27 | Sacroiliitis on MRI/radiograph; note LSTV co-exists more often in axSpA |
LSTV and Sacroiliitis Overlap
LSTV is more frequent in patients with inflammatory back pain who turn out to have axial spondyloarthritis, and its pain territory overlaps the SI joint. Do not anchor on the LSTV: screen for inflammatory features and image the SI joints before attributing all pain to the pseudoarticulation.
Controversies & Areas of Uncertainty
Is LSTV truly a pain generator?
The causal link between LSTV and low back pain remains debated. Prevalence in asymptomatic and symptomatic populations is similar, so an LSTV seen on imaging is frequently incidental. Attribution requires concordant tenderness, imaging change at the pseudoarticulation, and a positive diagnostic block.
Resection versus fusion
No randomised trial compares pseudoarthrectomy with fusion. Biomechanical and cohort data favour motion-preserving resection when superior levels are stable, reserving fusion for above-level instability or established adjacent-segment disc disease. Practice varies widely between surgeons.
Injection durability
Pseudoarticulation injections reliably produce short-term relief and are valuable diagnostically, but the duration of therapeutic benefit is inconsistent and not well defined by long-term data. A good response predicts surgical success better than it predicts lasting relief from injection alone.
Classification limits
The Castellvi system describes morphology, not symptoms, and inter-observer agreement on plain radiographs is only moderate. It does not capture extraforaminal nerve compression or contralateral facet load, so it should guide rather than dictate management.
Evidence Base
Original Description
- First description of low back pain associated with lumbosacral transitional vertebra
- Recognized that anomalous anatomy could be symptomatic
- Established the eponymous syndrome
Castellvi Classification (landmark)
- 200 consecutive patients with myelographically proven disc herniation reviewed; 60 met criteria for LSTV
- Defined the four-type radiographic classification (Types I-IV) still in universal use
- Type II LSTV showed disc herniation at the transition level and excess herniations at the level just above
- Types III and IV showed no herniation at the transitional level itself
LSTV and Above-Level Disc Degeneration
- 52 patients on MRI: discs immediately above the LSTV were significantly more degenerate; the disc between transitional vertebra and sacrum was significantly less degenerate
- 70-cadaver study: iliolumbar ligament at the level above the LSTV was thinner and weaker
- Proposed weak iliolumbar ligament leads to instability and accelerated degeneration above the transition
LSTV: Classification, Imaging & Clinical Relevance (review)
- Comprehensive review of LSTV imaging, numbering and the genesis of LSTV-related low back pain
- Pain may arise from the level above the transition, the contralateral facet (when unilateral), or the anomalous articulation
- Emphasises whole-spine imaging and geometric landmarks to avoid wrong-level surgery
Prevalence of LSTV in the General Population
- 211 evaluable abdominal radiographs: 75 (35.6%) had an LSTV using strict Castellvi criteria
- Castellvi Type Ia was the most common variant (14.7%)
- 6.6% had six lumbar (non-ribbed) vertebrae, underscoring numbering pitfalls
Treatment Patterns & Pseudoarthrectomy Outcomes
- Retrospective cohort of 67 patients with LSTV over 10 years; 33% had an LSTV not identified by their provider
- Pseudoarticulation injection gave significantly greater immediate relief than any other injection type
- Patients responding to pseudoarticulation injection who underwent pseudoarthrectomy had more durable relief than those who continued injections alone
Biomechanics: Resection vs Fusion
- Cadaveric/3D-printed Bertolotti model (7 spines): LSTV significantly reduced L5-S1 motion, especially lateral bending and axial rotation
- Ipsilateral lateral bending with axial rotation generated the greatest force across the pseudoarticulation
- L4-S1 and L5-S1 fusion increased adjacent-segment motion versus LSTV alone, favouring joint resection when superior levels are stable
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Young Adult with Low Back Pain and LSTV
"A 28-year-old office worker presents with 18-month history of left-sided low back pain. Pain is worse with prolonged standing and extension. Examination shows tenderness lateral to the midline at L5 level on the left. X-ray shows an enlarged left L5 transverse process articulating with the sacral ala."
Surgical Planning for Bertolotti Syndrome
"The same patient has failed 6 months of conservative management including physical therapy. Diagnostic injection into the left pseudoarticulation provided 85% pain relief for 3 weeks. CT confirms Type IIa LSTV with degenerative changes at the pseudoarthrosis. MRI shows mild L4-L5 disc degeneration but no herniation."
LSTV with Level Counting Challenge
"A 45-year-old woman is scheduled for L4-L5 discectomy for disc herniation. Preoperative MRI shows disc herniation at the lowest mobile disc level. However, her lumbar spine X-ray shows 6 lumbar-type vertebrae with the lowest one having an enlarged left transverse process articulating with the sacrum."
BERTOLOTTI SYNDROME (LSTV)
Clinical summary
Definition
- •LSTV = Lumbosacral Transitional Vertebra
- •Sacralization of L5 or lumbarization of S1
- •Bertolotti syndrome = symptomatic LSTV
- •Named after Mario Bertolotti (1917)
Castellvi Classification
- •Type I: Dysplastic TP (≥19mm) - no articulation
- •Type II: Pseudoarticulation - MOST SYMPTOMATIC
- •Type III: Complete fusion to sacrum
- •Type IV: Type II + Type III (mixed)
- •Suffix a = unilateral, b = bilateral
Pain Sources (PAIN)
- •P = Pseudoarticulation (anomalous joint)
- •A = Arthrosis (contralateral facet)
- •I = Intervertebral disc (above level)
- •N = Nerve (extraforaminal L5 compression)
Diagnosis
- •Ferguson view X-ray (30-35° cephalad)
- •CT for bony detail and Castellvi typing
- •MRI for disc and soft tissue
- •Diagnostic injection confirms pain source
Treatment
- •Conservative first: PT, NSAIDs, activity modification
- •Injection: Pseudoarticulation (diagnostic/therapeutic)
- •Surgery: Resection for Type II, Fusion if disc disease
- •Must have positive diagnostic injection before surgery
Critical Points
- •Level counting essential - risk of wrong-level surgery
- •Count from C2 on whole-spine imaging
- •Document transitional anatomy clearly
- •Young patient presentation typical (20s-30s)
Guidelines, Registries & Global Practice
Global epidemiology:
| Measure | Figure | Source population |
|---|---|---|
| LSTV prevalence (strict criteria) | ~4-36% | Varies with definition and imaging method |
| General-population radiographic series | 18.9% positive (sacralization 17.2%, lumbarization 1.7%) | Turkish cohort, 3607 abdominal films |
| US general-population series | 35.6% positive; 6.6% had six lumbar vertebrae | US KUB radiographs |
| LSTV in suspected axial spondyloarthritis | 29.1% | European inflammatory back pain cohort |
Guideline landscape (side by side):
There is no condition-specific society guideline dedicated to Bertolotti syndrome. Management is governed by general low back pain and wrong-level-surgery guidance, which differs by region:
| Body | Position relevant to LSTV / low back pain |
|---|---|
| NICE (UK, NG59) | Non-specific low back pain managed without routine imaging; reserve MRI for when a specific cause is suspected or surgery is considered — relevant to avoiding over-attribution to incidental LSTV |
| AAOS / NASS (US) | Emphasise correlation of imaging with symptoms and image-guided diagnostic blocks before intervention |
| WHO Surgical Safety Checklist / national patient-safety bodies | Mandatory site and level verification — the core defence against LSTV-related wrong-level surgery |
| Spine society consensus | Whole-spine imaging and consistent numbering recommended whenever LSTV is present and surgery is planned |
Registry note:
No arthroplasty/implant registry tracks Bertolotti procedures specifically, as resection is non-instrumented and fusion volumes are low. Wrong-level spinal surgery is, however, captured by national patient-safety/never-event reporting systems in several countries, where transitional anatomy is a recurrent contributing factor.
High- vs limited-resource practice variation:
- Well-resourced settings: CT and MRI are routine; CT- or fluoroscopy-guided diagnostic injections and image-navigated minimally invasive pseudoarthrectomy are available; multidisciplinary review for complex level identification.
- Limited-resource settings: Diagnosis often rests on plain radiographs (Ferguson view) and clinical correlation; diagnostic injection access may be limited; treatment is predominantly conservative, with surgery reserved for clearly refractory, well-localised cases.
Wrong-level surgery — universal principle:
Prevention of wrong-level surgery is a global surgical-safety priority. Multiple level confirmations (whole-spine imaging, intraoperative imaging with a marker, consistent documented nomenclature) are required wherever transitional anatomy is present, irrespective of health system.
References
- Bertolotti M. Contributo alla conoscenza dei vizi di differenzazione regionale del rachide con speciale riguardo all'assimilazione sacrale della V. lombare. Radiol Med. 1917;4:113-44.
- Castellvi AE, Goldstein LA, Chan DP. Lumbosacral transitional vertebrae and their relationship with lumbar extradural defects. Spine (Phila Pa 1976). 1984;9(5):493-5. PMID 6495013. doi:10.1097/00007632-198407000-00014
- Aihara T, Takahashi K, Ogasawara A, et al. Intervertebral disc degeneration associated with lumbosacral transitional vertebrae: a clinical and anatomical study. J Bone Joint Surg Br. 2005;87(5):687-91. PMID 15855373. doi:10.1302/0301-620X.87B5.15727
- Konin GP, Walz DM. Lumbosacral transitional vertebrae: classification, imaging findings, and clinical relevance. AJNR Am J Neuroradiol. 2010;31(10):1778-86. PMID 20203111. doi:10.3174/ajnr.A2036
- Jancuska JM, Spivak JM, Bendo JA. A review of symptomatic lumbosacral transitional vertebrae: Bertolotti's syndrome. Int J Spine Surg. 2015;9:42. PMID 26484005. doi:10.14444/2042
- Apazidis A, Ricart PA, Diefenbach CM, Spivak JM. The prevalence of transitional vertebrae in the lumbar spine. Spine J. 2011;11(9):858-62. PMID 21951610. doi:10.1016/j.spinee.2011.08.005
- McGrath KA, Rabah NM, Steinmetz MP. Identifying treatment patterns in patients with Bertolotti syndrome: an elusive cause of chronic low back pain. Spine J. 2021;21(9):1497-1503. PMID 34010681. doi:10.1016/j.spinee.2021.05.008
- Golubovsky JL, Colbrunn RW, Klatte RS, et al. Development of a novel in vitro cadaveric model for analysis of biomechanics and surgical treatment of Bertolotti syndrome. Spine J. 2020;20(4):638-656. PMID 31669612. doi:10.1016/j.spinee.2019.10.011