Bioabsorbable Materials
PGA, PLA, and PLLA Implants
Material Classes
Critical Must-Knows
- Definition: Synthetic polymers (Polyesters) that degrade in the body via Hydrolysis, eliminating the need for removal surgery
- Definition: Commonly used for interference screws, suture anchors, and pediatric fractures
- Mechanism: Degradation via Hydrolysis (uptake of water breaks ester bonds)
- Management: Used where metal removal would be obligatory or difficult
Clinical Pearls
- "Biocompatibility (Foreign body reaction is a risk)
- "Strength retention profile (Must last long enough for bone healing)
- "Risk of Foreign Body Reaction (Sterile abscess/cystic change) especially with PGA
- "Osteoconductive composites (added TCP/HA) help bone replacement
Clinical Imaging
Imaging Gallery

Exam Warning
Degradation Mechanism
Hydrolysis: It is NOT enzymatic. Water breaks ester bonds.
The 'Acid Dump' Risk
PGA (Rapid): Fast degradation releases acid spike → overwhems buffer → Sterile Abscess.
PLLA Profile
Hydrophobic: Very slow degradation (years). Less reaction, but foreign body remains.
Common Polymers
1. Polyglycolic Acid (PGA):
- Hydrophilic (loves water).
- Fast degradation: Loses strength in ~6 weeks. Absorbed by ~6 months.
- Problem: High rate of foreign body reaction (sterile abscess) due to "acid dump".
- Use: Rapidly healing tissues / Sutures (Vicryl is Polyglactin).
2. Poly-L-Lactic Acid (PLLA):
- Hydrophobic.
- Slow degradation: Retains strength for over 12 months. Absorbed over 3-5 years.
- Problem: Crystalline debris can cause late reactions.
- Use: ACL screws, Meniscal arrows.
3. Co-polymers (PLGA/PLDLA):
- Mixing L-Lactic and D-Lactic acids creates an Amorphous (non-crystalline) structure.
- Tunable degradation rate (intermediate).
4. Bio-Composites:
- Polymer + Bioceramic (TCP or Hydroxyapatite).
- Benefit: The ceramic buffers the acidic byproducts (alkaline) and promotes bone ingrowth.
At a Glance
Bioabsorbable materials are synthetic polyester polymers that degrade in vivo via hydrolysis, eliminating the need for removal surgery. PGA (polyglycolic acid) degrades rapidly (weeks-months) with 5-10% risk of sterile abscess from acid byproduct accumulation, while PLLA (poly-L-lactic acid) is hydrophobic with slow degradation (3-5 years). Common applications include ACL interference screws, meniscal arrows, and paediatric transphyseal pins. Bio-composites (polymer + TCP/hydroxyapatite) buffer acidic byproducts and promote osteoconduction. Key advantages include no stress shielding and MRI compatibility, but they are weaker than metal and carry risks of tunnel widening and brittle screw breakage during insertion.
G-L-Very SlowDegradation Speed
| P | PGA (Glycolic): Fast (weeks) |
| P | PLLA (Lactic): Slow (years) |
| P | PLGA: Variable |
| P | PGA (Glycolic): Fast (weeks) |
| P | PLLA (Lactic): Slow (years) |
| P | PLGA: Variable |
Hook:Glycolic Goes (Fast), Lactic Lasts (Slow)
SCRAPWhere Bioabsorbables Shine
| S | S — Suture anchors (shoulder/hip labrum) |
| C | C — Cruciate (ACL) interference screws |
| R | R — Repair of meniscus (arrows/darts) |
| A | A — All paediatric transphyseal pins |
| P | P — Plus small-fragment / malleolar fixation |
| S | S — Suture anchors (shoulder/hip labrum) | A | A — All paediatric transphyseal pins |
| C | C — Cruciate (ACL) interference screws | P | P — Plus small-fragment / malleolar fixation |
| R | R — Repair of meniscus (arrows/darts) |
Hook:You SCRAP the second operation
Degradation & Erosion Mechanism
Understanding the mechanism is the single most-tested concept in the basic-science viva. Degradation is non-enzymatic hydrolysis of ester bonds — water diffuses into the polymer and cleaves the backbone, progressively reducing molecular weight until fragments are small enough to be cleared by macrophages and metabolised via the Krebs cycle to CO₂ and water.
Bulk erosion vs surface erosion — alpha-hydroxy polyesters (PLA, PGA) undergo bulk erosion: water penetrates faster than bonds break, so the whole implant hydrolyses simultaneously. Strength is lost throughout the cross-section before significant mass is lost, and trapped acidic monomers cannot escape — this autocatalysis is what drives the rapid late "acid dump". Surface-eroding polymers (polyanhydrides, not standard ortho polyesters) degrade from the outside in and retain core strength longer.
Two distinct timelines matter clinically:
- Strength-retention time — how long the implant holds load (must outlast bone/graft healing).
- Mass-loss / resorption time — how long until the implant disappears (much longer than strength loss).
For PLLA the gap is large: mechanical strength may be lost over months while the bulk material persists radiographically for 3-5 years or more, which is why late PLLA foreign-body reactions can present years after surgery.
Advantages and Disadvantages
Advantages:
- No removal surgery needed.
- No stress shielding (load transfers gradually as implant weakens).
- No MRI artifact.
- Radiolucent (can see fracture healing).
Disadvantages:
- Weaker than metal (cannot use for load bearing in adults).
- Sterile Abscess / Osteolysis: 5-10% rate.
- Screw breakage during insertion (Brittle).
- "Tunnel widening" in ACL surgery.
Clinical Relevance
Bioabsorbable implants are chosen for low-load indications where avoiding a second removal operation, eliminating MRI artefact, or allowing easy revision through the implant outweighs the lower mechanical strength.
Established applications:
- ACL/PCL reconstruction — interference screws for graft fixation (the most studied use).
- Suture anchors — shoulder and hip labral repair, rotator cuff repair.
- Meniscal repair — arrows, darts and screws (largely superseded by all-inside suture devices, but historically important).
- Paediatric fractures — transphyseal/epiphyseal fixation where crossing the physis with metal is undesirable; pins resorb and avoid hardware removal.
- Selected malleolar and small-fragment fractures — historically a major indication in the Helsinki series.
Where NOT to use them:
- Load-bearing diaphyseal or articular fixation in adults (insufficient strength).
- Situations where a sterile foreign-body reaction would be catastrophic without warning.
Evidence Base
Adverse tissue reactions — the landmark cohort (PGA vs PLA)
- 2528 patients with absorbable pins/rods/screws; clinically significant sterile foreign-body reaction in 108 (4.3%)
- Reaction rate 5.3% for PGA (107/2037) versus 0.2% for PLA (1/491) — over 20-fold higher with fast-degrading PGA
- PGA reactions appeared at a mean of 11 weeks; the single PLA reaction occurred 4.3 years after surgery
- Higher risk with poorly vascularised bone (scaphoid), quinone-dye additives, and high-surface-area implants (screws greater than pins)
- Severe reactions caused osteolytic lesions; four patients ultimately needed wrist/ankle arthrodesis
Bioabsorbable vs metallic interference screws — Cochrane review
- 12 trials (11 RCTs), 944 participants, hamstring or patellar-tendon grafts
- No clinically important difference in Lysholm or Tegner scores at 12, 24 or ≥60 months (very low-quality evidence)
- Greater treatment failure with bioabsorbable screws: 60/451 vs 29/434, RR 1.94 (95% CI 1.29-2.93) favouring metal
- All 16 intraoperative complications in the bioabsorbable group were implant breakage on insertion
- PLLA was the most common bioabsorbable material; metal screws were titanium
Overlapping meta-analyses — what is actually different
- Systematic review of 3 high-quality meta-analyses (1 Level I, 2 Level II) of metal vs bioabsorbable interference screws
- No difference in validated outcome scores, pivot-shift, KT arthrometry or loss of motion
- Bioabsorbable screws associated with prolonged knee effusion, increased femoral tunnel widening, and more screw breakage
- Concludes future work should focus on cost-effectiveness rather than further efficacy trials
RCT — identically shaped bioabsorbable vs titanium screw
- 100 patients randomised to bioabsorbable or titanium interference screws, hamstring autograft ACL reconstruction
- Identical screw geometry isolated the material variable
- No difference in Lysholm or IKDC scores at any time point to 2 years
- Tibial tunnel widths equal; slightly more femoral tunnel widening with bioabsorbable screws
Bio-composite (PLLA/PGA/β-TCP) degradation and osteoconduction
- 13 patients with BPTB ACL reconstruction fixed by PLLA/PGA/β-TCP biocomposite screws, CT at mean 38 months
- No screw remnant present at 3 years — complete degradation, replaced by calcified non-trabecular material
- Osteoconductivity present in 21/26 tunnels (81%), complete (type 4) ossification in 5/26 (19%)
- Screw-site density (≈157-159 HU) matched native cancellous bone (≈140-146 HU)
Large single-centre series — clinical track record
- 3200 patients managed with self-reinforced absorbable polyester implants since 1984 (Helsinki series)
- Uneventful postoperative course in over 90%; wound infection 4%, fixation failure 4%
- Non-infectious foreign-body reaction at 2-3 months in ~2% of recent PGA cases, none with PLA
- Most common indication was the displaced malleolar fracture; transphyseal pins used in children
- Implant-removal operations avoided, giving financial and psychological advantages
Foundational textbook — biomaterials principles
- Bioabsorbable polymers are alpha-hydroxy polyesters degraded by non-enzymatic hydrolysis
- Degradation order (fastest to slowest): PGA greater than PDLLA (amorphous) greater than PLLA (crystalline)
- Copolymer (PLGA) degradation is tunable by lactide:glycolide ratio
- Composites with TCP/HA buffer acid byproducts and add osteoconduction
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Controversies & Areas of Uncertainty
- Do bioabsorbable screws offer any real clinical advantage over metal? High-level evidence (Cochrane and overlapping meta-analyses) shows equivalent functional outcomes but higher treatment-failure and intraoperative-breakage rates for bioabsorbable interference screws. The argued benefits — easier revision, no MRI artefact, no removal surgery — are largely theoretical or device-specific rather than proven in outcome scores.
- "Tunnel widening" — does it matter? Bioabsorbable (especially pure-polymer) screws are associated with more femoral tunnel widening and prolonged effusion, but whether this translates into worse long-term stability or harder revision is unresolved.
- Are composites the answer? Bio-composites (polymer + β-TCP/HA) demonstrably degrade more completely and promote osteoconduction, but high-quality comparative RCTs showing they reduce clinically important complications versus pure polymers (and justify higher cost) are limited.
- PLLA's slow resorption — benefit or liability? Prolonged strength retention is useful, but bulk PLLA can persist for years and cause late foreign-body reactions, so "absorbable" does not mean "gone".
- Cost-effectiveness is now the key research question — efficacy is broadly settled, so future trials should weigh device cost against the avoided-removal-surgery and adverse-event profiles.
Complications
Polymer Types — Differential Comparison
Bioabsorbable vs Metal Interference Screws
MCQ Practice Points
Clinical Pearl
Q: What are the main types of bioabsorbable polymers used in orthopaedics?
A: (1) PLA (Poly-lactic acid): Most common, slow degradation (2-4 years), good strength. (2) PGA (Poly-glycolic acid): Fast degradation (6-12 months), high crystallinity, historic first-generation. (3) PLLA: L-isomer of PLA, slower degradation than racemic PDLLA. (4) Copolymers (PLGA): Tunable degradation by varying LA:GA ratio. All degrade via hydrolysis to lactic/glycolic acid.
Clinical Pearl
Q: What is the mechanism of bioabsorbable polymer degradation?
A: Bulk hydrolysis of ester bonds by water. Polymers absorb water, autocatalytic degradation occurs (acidic byproducts accelerate breakdown), molecular weight decreases, mechanical strength lost, fragments phagocytosed by macrophages. Final products (lactic acid, glycolic acid) enter Krebs cycle and are excreted as CO₂ and H₂O. Not enzymatic degradation.
Clinical Pearl
Q: What are the clinical applications of bioabsorbable implants in orthopaedics?
A: (1) Suture anchors: Shoulder, hip labral repairs. (2) Interference screws: ACL reconstruction (tibial fixation). (3) Meniscal arrows/darts: Meniscal repair. (4) Pediatric fractures: Avoid growth plate crossing with metal. Advantages: No second surgery for removal, no stress shielding. Not suitable for load-bearing cortical fixation.
Clinical Pearl
Q: What are the complications specific to bioabsorbable implants?
A: (1) Sterile osteolysis: Acidic degradation products cause foreign body reaction, cyst formation. (2) Inflammatory reaction: Crystalline degradation particles. (3) Premature mechanical failure: Loss of strength before healing complete. (4) Incomplete resorption: Residual material detectable years later. (5) MRI artifact: Some products create signal void for extended period.
Clinical Pearl
Q: Why did early bioabsorbable implants (PGA) cause high rates of sterile abscess formation?
A: Pure PGA degrades rapidly (3-6 months), releasing high concentrations of glycolic acid in a short period. This acidic environment causes: (1) pH drop, (2) Intense foreign body reaction, (3) Sterile fluid collection/sinus formation. Modern implants use slower-degrading PLA or copolymers (PLGA 85:15) with more gradual acid release, reducing inflammatory response.
Guidelines, Registries & Global Practice
Global Epidemiology & Practice Variation
Bioabsorbable implants are a global market that continues to expand, with the dominant indications being ACL/soft-tissue fixation, suture anchors, meniscal repair devices, and paediatric transphyseal/epiphyseal fixation. Practice converges worldwide on a few principles:
- First-generation pure PGA is now largely historical because of sterile foreign-body reaction rates of roughly 4-5% (and higher in poorly vascularised bone).
- PLLA and PLGA copolymers replaced PGA for slower, cleaner degradation.
- Bio-composites (polymer + β-TCP / hydroxyapatite) are now the default choice for interference screws and many anchors in well-resourced settings because they buffer acid and promote bony replacement of the implant track.
High- vs limited-resource settings:
- High-resource centres favour bio-composite or all-suture anchors and accept the higher per-unit cost for the avoided-removal-surgery and MRI-compatibility benefits.
- In limited-resource settings, reusable metal (titanium/stainless steel) implants remain standard for cost reasons; the theoretical advantage of avoiding a removal operation is offset by the device cost, and metal is robust and cheap.
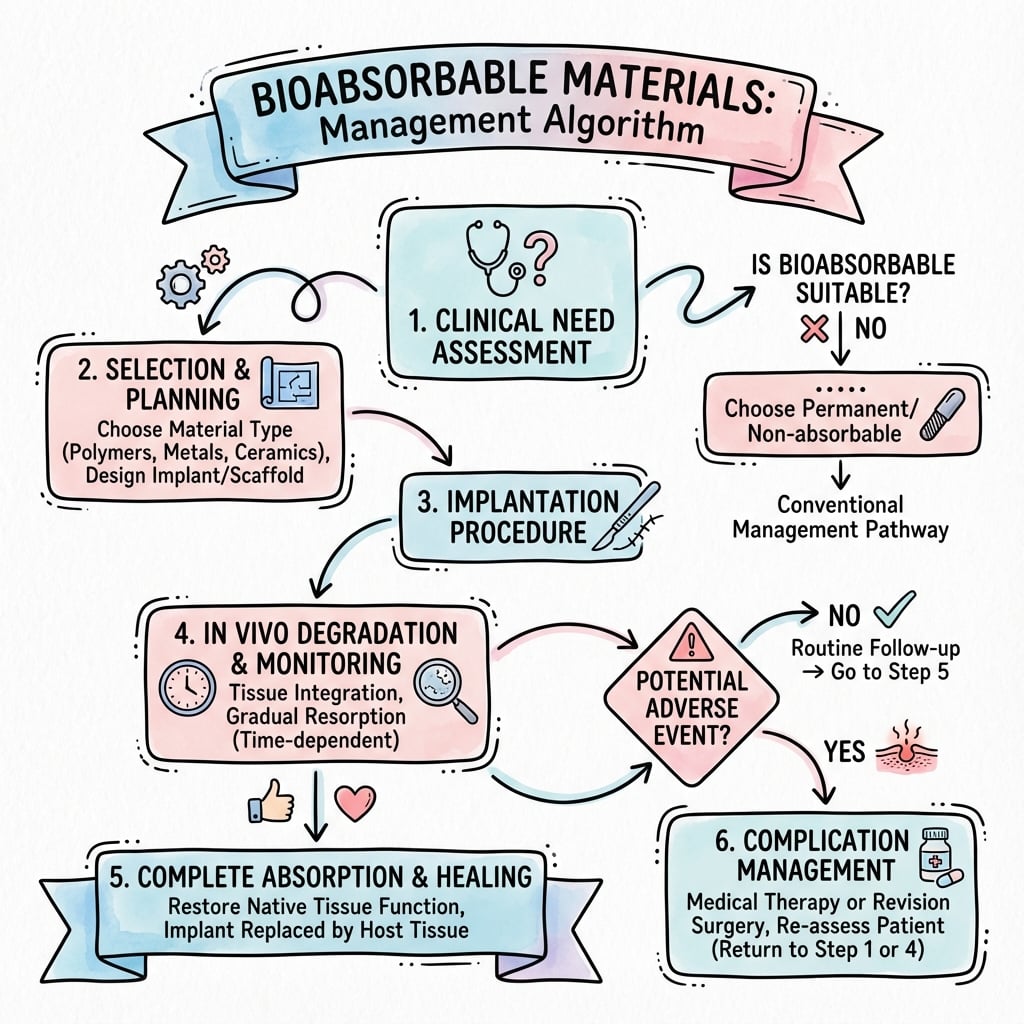
Management Algorithm
References
- Böstman OM, Pihlajamäki HK. Adverse tissue reactions to bioabsorbable fixation devices. Clin Orthop Relat Res. 2000;(371):216-27. PMID 10693569.
- Debieux P, Franciozi CES, Lenza M, et al. Bioabsorbable versus metallic interference screws for graft fixation in anterior cruciate ligament reconstruction. Cochrane Database Syst Rev. 2016;7:CD009772. DOI
- Mascarenhas R, Saltzman BM, Sayegh ET, et al. Bioabsorbable versus metallic interference screws in ACL reconstruction: a systematic review of overlapping meta-analyses. Arthroscopy. 2015;31(3):561-8. DOI
- Myers P, Logan M, Stokes A, Boyd K, Watts M. Bioabsorbable versus titanium interference screws with hamstring autograft in ACL reconstruction: a prospective randomized trial with 2-year follow-up. Arthroscopy. 2008;24(7):817-23. DOI
- Barber FA, Dockery WD, Hrnack SA. Long-term degradation of a poly-lactide co-glycolide/β-tricalcium phosphate biocomposite interference screw. Arthroscopy. 2011;27(5):637-43. DOI
- Rokkanen PU, Böstman O, Hirvensalo E, et al. Bioabsorbable fixation in orthopaedic surgery and traumatology. Biomaterials. 2000;21(24):2607-13. DOI
- Ambrose CG, Clanton TO. Bioabsorbable implants: review of clinical experience in orthopedic surgery. Ann Biomed Eng. 2004;32(1):171-7. DOI
Evidence verified against PubMed. Per PubMed attribution requirements, DOIs are linked above where available.
Bioabsorbable Quick Facts
Clinical summary
Science
- •Polyesters (PLLA, PGA)
- •Degradation: Hydrolysis
- •Byproducts: Acid + Water + CO2
Comparison
- •PGA: Hydrophilic, Fast, Reactive
- •PLLA: Hydrophobic, Slow, Inert
- •PLGA: Tunable