Structured Bacterial Communities | Extracellular Matrix Protection | 1000x Antibiotic Resistance | Implant-Associated Infections
STAGES OF BIOFILM FORMATION
Critical Must-Knows
- Biofilm = structured bacterial community embedded in self-produced extracellular polymeric substance (EPS)
- 1000-fold increase in MIC compared to planktonic bacteria - explains antibiotic failure
- Persister cells (dormant, metabolically inactive) resist antibiotics that target dividing cells
- Implant removal essential for cure of mature biofilm infections - antibiotics alone fail
- DAIR (debridement, antibiotics, implant retention) only works for ACUTE infections (less than 3 weeks)
Clinical Pearls
- "Biofilm bacteria communicate via quorum sensing (autoinducer molecules)
- "EPS matrix is polysaccharide (80% water, 10-15% eDNA, proteins, polysaccharides)
- "Rifampicin penetrates biofilm better than other antibiotics (used in PJI treatment)
- "Sonication of explanted implants releases biofilm bacteria - improves culture yield by 20-30%
Clinical Imaging
Imaging Gallery




Critical Biofilm Exam Points
Biofilm Definition
Biofilm is a structured community of bacteria enclosed in self-produced extracellular polymeric substance (EPS) matrix, adherent to a surface. Fundamentally different from planktonic (free-floating) bacteria in physiology and antibiotic susceptibility.
1000x Antibiotic Resistance
Bacteria in biofilm are 1000-fold more resistant to antibiotics than planktonic bacteria. Not due to genetic resistance genes, but physical protection (EPS barrier) and metabolic dormancy (persister cells). This explains treatment failure despite in vitro susceptibility.
Implant Removal Necessary
Mature biofilm cannot be eradicated with antibiotics alone - physical removal of biofilm (implant exchange) essential for cure. DAIR only works if biofilm not yet established (less than 3 weeks, acute infections).
Persister Cells
Persister cells (0.1-1% of biofilm) are dormant, metabolically inactive bacteria resistant to all antibiotics. They survive treatment and cause relapse when conditions improve. Explains recurrence after stopping antibiotics.
BIOFILMBIOFILM - Stages and Characteristics
| B | Bacteria attach to surface Initial reversible adhesion (0-4 hours) |
| I | Irreversible attachment Bacterial adhesins bind tightly (4-24 hours) |
| O | Organize into microcolonies 3D structure begins to form |
| F | Form EPS matrix Extracellular polymeric substance secreted (polysaccharide shield) |
| I | Impenetrable to antibiotics 1000x increased MIC, persister cells dormant |
| L | Long-term persistence Chronic infection, requires implant removal for cure |
| M | Microenvironment created pH gradients, nutrient channels, anaerobic zones |
| B | Bacteria attach to surface Initial reversible adhesion (0-4 hours) | F | Form EPS matrix Extracellular polymeric substance secreted (polysaccharide shield) | M | Microenvironment created pH gradients, nutrient channels, anaerobic zones |
| I | Irreversible attachment Bacterial adhesins bind tightly (4-24 hours) | I | Impenetrable to antibiotics 1000x increased MIC, persister cells dormant | ||
| O | Organize into microcolonies 3D structure begins to form | L | Long-term persistence Chronic infection, requires implant removal for cure |
Hook:BIOFILM forms in stages and creates impenetrable antibiotic resistance
MATRIXMATRIX - Components of Biofilm EPS
| M | Microbes embedded Bacteria make up only 10-15% of biofilm volume |
| A | Adhesins for attachment Surface proteins bind to implant (fibronectin-binding, collagen-binding) |
| T | Teichoic acids (Staph) Cell wall components of gram-positive bacteria |
| R | Resistant to antibiotics Physical barrier, altered pH, persister cells |
| I | Intercellular polysaccharide PIA (polysaccharide intercellular adhesin) in S. epidermidis, encoded by ica genes |
| X | eXtracellular DNA (eDNA) 10-15% of matrix, provides structural support and antibiotic binding |
| M | Microbes embedded Bacteria make up only 10-15% of biofilm volume | T | Teichoic acids (Staph) Cell wall components of gram-positive bacteria | I | Intercellular polysaccharide PIA (polysaccharide intercellular adhesin) in S. epidermidis, encoded by ica genes |
| A | Adhesins for attachment Surface proteins bind to implant (fibronectin-binding, collagen-binding) | R | Resistant to antibiotics Physical barrier, altered pH, persister cells | X | eXtracellular DNA (eDNA) 10-15% of matrix, provides structural support and antibiotic binding |
Hook:The MATRIX protects bacteria and makes them antibiotic-resistant
PERSISTPERSIST - Why Biofilm Bacteria Survive Antibiotics
| P | Physical barrier (EPS) Matrix blocks antibiotic penetration |
| E | Enzymes degrade antibiotics Beta-lactamases, aminoglycoside-modifying enzymes concentrated in biofilm |
| R | Reduced metabolic activity Dormant bacteria not targeted by antibiotics (target dividing cells) |
| S | Slow growth rate Nutrient limitation in biofilm depths slows division |
| I | Impaired antibiotic binding eDNA and matrix components bind antibiotics |
| S | Small persister cell population 0.1-1% of bacteria are dormant persisters resistant to all antibiotics |
| T | Tolerance not resistance Phenotypic tolerance (reversible) not genetic resistance (permanent) |
| P | Physical barrier (EPS) Matrix blocks antibiotic penetration | S | Slow growth rate Nutrient limitation in biofilm depths slows division | T | Tolerance not resistance Phenotypic tolerance (reversible) not genetic resistance (permanent) |
| E | Enzymes degrade antibiotics Beta-lactamases, aminoglycoside-modifying enzymes concentrated in biofilm | I | Impaired antibiotic binding eDNA and matrix components bind antibiotics | ||
| R | Reduced metabolic activity Dormant bacteria not targeted by antibiotics (target dividing cells) | S | Small persister cell population 0.1-1% of bacteria are dormant persisters resistant to all antibiotics |
Hook:PERSIST explains why biofilm bacteria survive despite antibiotic susceptibility in vitro
Overview
Biofilm is a structured community of bacterial cells enclosed in a self-produced extracellular polymeric substance (EPS) matrix and adherent to an inert or living surface.
Historical context: Biofilms were first described by van Leeuwenhoek in 1684 observing "animalcules" on teeth. The modern concept of biofilm was established by Costerton in the 1970s-1980s, revolutionizing understanding of bacterial persistence and chronic infections.
Why biofilm matters clinically:
Prosthetic Joint Infections
Biofilm formation on implants explains why PJI cannot be cured with antibiotics alone. Mature biofilm requires implant removal for eradication. DAIR only effective if biofilm not yet established (acute infections less than 3 weeks).
Chronic Osteomyelitis
Biofilm on sequestrum (dead bone) and necrotic tissue protects bacteria from antibiotics and immune system. Explains need for surgical debridement of all necrotic material in addition to prolonged antibiotics.
Biofilm vs Planktonic Bacteria
Planktonic bacteria (free-floating) are what we test in microbiology lab (in vitro susceptibility). Biofilm bacteria are fundamentally different: 1000x higher MIC, metabolically dormant, physically protected. In vitro susceptibility does NOT predict in vivo efficacy for biofilm infections. This explains "antibiotic failure" despite sensitive organism.
Stages of Biofilm Formation

Biofilm Development Timeline
Initial contact between planktonic bacteria and surface (implant, bone). Mediated by weak van der Waals forces, electrostatic interactions, and hydrophobic effects. Bacteria are still susceptible to antibiotics and mechanical forces (irrigation). This is a critical window for prevention - antibiotic prophylaxis effective at this stage.
Bacterial adhesins (surface proteins) bind tightly to host proteins (fibronectin, collagen, fibrinogen) adsorbed on implant. Bacteria begin producing extracellular polymeric substance (EPS). Attachment becomes permanent. Early debridement and antibiotics may still be effective.
Bacteria proliferate and organize into microcolonies (clusters). EPS production increases, forming protective matrix. 3D architecture begins to develop with water channels for nutrient flow. Antibiotic penetration starts to diminish.
Mature biofilm with complex 3D structure. EPS matrix fully developed (80% water, 10-15% polysaccharides/eDNA/proteins). Persister cells present (dormant, antibiotic-resistant). Quorum sensing coordinates bacterial behavior. Antibiotics largely ineffective - implant removal necessary.
Bacteria detach from biofilm edges (planktonic dispersal) to colonize new sites. Triggers acute symptoms (bacteremia, sepsis). Dispersal can be triggered by nutrient depletion, quorum sensing signals, or external stress. Explains acute exacerbations of chronic infections.
Critical Time Window
First 24-48 hours post-implantation are critical. If bacteria attach and begin biofilm formation, chronic infection likely. Antibiotic prophylaxis most effective if given before incision (within 60 minutes) to prevent initial attachment. After 48 hours, biofilm maturation makes eradication difficult without implant removal.
DAIR Window
DAIR (debridement, antibiotics, implant retention) only successful if performed within 3 weeks of symptom onset for acute infections. After 3 weeks, mature biofilm established and implant removal required. Success rate of DAIR: 50-70% if acute (less than 3 weeks), less than 20% if chronic (greater than 3 weeks).
Biofilm Structure and Composition
Extracellular Polymeric Substance (EPS) Matrix
Composition (by weight):
- Water: 80-90% of biofilm volume
- Polysaccharides: 40-50% of dry weight (structural backbone)
- eDNA (extracellular DNA): 10-20% of dry weight
- Proteins: 20-30% of dry weight (enzymes, adhesins)
- Lipids: 5-10% of dry weight
- Bacterial cells: Only 10-15% of biofilm volume
Polysaccharides:
- PIA (polysaccharide intercellular adhesin): S. epidermidis, encoded by ica genes
- PNAG (poly-N-acetylglucosamine): Staphylococcus species
- Alginate: Pseudomonas aeruginosa
- Pel and Psl: Pseudomonas aeruginosa
- Functions: Structural scaffold, adhesion, protection from desiccation and immune cells
Extracellular DNA (eDNA):
- Released from lysed bacteria or actively secreted
- Provides structural support (scaffolding)
- Binds cationic antibiotics (aminoglycosides, polymyxins) - reduces penetration
- Contains antibiotic resistance genes (horizontal gene transfer within biofilm)
- DNase treatment can disrupt young biofilms (research application)
Proteins:
- Adhesins: Bind to host proteins and implant surfaces
- Enzymes: Beta-lactamases, proteases, nucleases
- Amyloid fibrils: Structural support (Staphylococcus, E. coli)
ica Genes in Staphylococcus
ica operon (icaADBC) in S. epidermidis encodes enzymes for PIA synthesis. Bacteria lacking ica genes cannot form biofilm and are less virulent in prosthetic infections. icaA and icaD are essential genes. Biofilm-negative strains exist but are uncommon clinical isolates.
The EPS matrix is the key protective element of biofilm.
Mechanisms of Antibiotic Resistance in Biofilm
Biofilm bacteria are 1000-fold more resistant to antibiotics through multiple mechanisms:
Biofilm Antibiotic Resistance Mechanisms
| Mechanism | Description | Effect | Clinical Implication |
|---|---|---|---|
| EPS barrier | Matrix blocks antibiotic diffusion | Reduced penetration to depths | Outer bacteria killed, inner survive |
| eDNA binding | eDNA binds cationic antibiotics | Aminoglycosides, polymyxins sequestered | Higher doses cannot overcome |
| pH gradients | Acidic microenvironments (pH 5-6) | Many antibiotics less active at low pH | Fluoroquinolones, aminoglycosides impaired |
| Enzyme degradation | Beta-lactamases concentrated in biofilm | Penicillins, cephalosporins destroyed | Even susceptible strains protected |
| Slow growth rate | Nutrient limitation slows division | Antibiotics target dividing cells | Dormant bacteria not killed |
| Persister cells | 0.1-1% dormant, non-growing | Tolerant to ALL antibiotics | Cause relapse, require removal |
| Altered gene expression | Biofilm-specific genes upregulated | Efflux pumps, stress responses | Phenotypic resistance |
Tolerance vs Resistance
Antibiotic tolerance (biofilm) is phenotypic and reversible - bacteria are genetically susceptible but protected by biofilm environment. Antibiotic resistance is genetic (genes like mecA, vanA) and permanent. Biofilm bacteria are TOLERANT not resistant - in vitro testing shows susceptibility, but in vivo treatment fails due to tolerance. This is why implant removal necessary.
Why antibiotics fail in biofilm infections:
Physical Barriers
EPS matrix, eDNA binding, and altered pH create physical and chemical barriers preventing antibiotics from reaching bacteria at MIC concentrations. Even high-dose IV antibiotics cannot penetrate to biofilm depths.
Metabolic Dormancy
Persister cells and slow-growing bacteria in nutrient-limited zones are metabolically inactive. Antibiotics target active processes (cell wall synthesis, protein synthesis, DNA replication) - dormant cells are untouched.
Clinical Implications in Orthopaedics
Biofilm in Prosthetic Joint Infections
Biofilm formation on implants:
- Bacteria attach within hours of contamination (intraoperative or hematogenous)
- Mature biofilm established by 48-72 hours
- Coagulase-negative Staphylococci (S. epidermidis) are master biofilm formers
- Biofilm provides sanctuary from antibiotics and immune cells
Treatment strategies based on biofilm maturity:
Acute infection (less than 3 weeks symptoms, less than 3 months post-op):
- Biofilm not yet mature or well-established
- DAIR (debridement, antibiotics, implant retention) possible
- Success rate: 50-70% if treated early
- Requires aggressive debridement, implant exchange of modular parts, biofilm-active antibiotics (rifampicin)
Chronic infection (greater than 3 weeks symptoms):
- Mature biofilm established
- Implant removal mandatory for cure
- Two-stage exchange: Remove implant + antibiotic spacer, then reimplantation after 6-12 weeks
- Suppressive antibiotics without removal: Temporary symptom control but eventual failure
Treatment Options by Infection Timing
| Scenario | Biofilm Status | Treatment | Success Rate |
|---|---|---|---|
| Acute (less than 3 weeks) | Immature biofilm | DAIR + antibiotics + rifampicin | 50-70% |
| Chronic (greater than 3 weeks) | Mature biofilm | Two-stage exchange | 80-90% |
| Chronic (suppression) | Mature biofilm | Antibiotics alone (no surgery) | less than 20% (eventual failure) |
Biofilm-active antibiotics:
- Rifampicin: Best biofilm penetration, NEVER monotherapy (rapid resistance)
- Fluoroquinolones: Moderate penetration, bactericidal
- Linezolid: Good penetration, oral bioavailability
- Daptomycin: Biofilm activity against Staphylococcus
- Avoid: Vancomycin (poor biofilm penetration despite IV use)
Rifampicin in PJI
Rifampicin is the most biofilm-penetrating antibiotic for Staphylococcus. Used in PJI treatment (300-450mg PO twice daily) in combination (NEVER alone - resistance develops in 48 hours). Added after 2-5 days of primary antibiotic (if susceptible). Effective for both DAIR and suppression protocols.
Evidence Base
Bacterial Biofilms: A Common Cause of Persistent Infections
- Landmark review defining biofilms as sessile bacterial communities in a self-synthesised hydrated polymeric matrix on surfaces
- Inherent antimicrobial resistance of biofilm communities is the root of many persistent and chronic bacterial infections
- Biofilm bacteria show differentiated, structured community behaviour distinct from planktonic cells
- Identified genetic and molecular community behaviour (including quorum sensing) as potential therapeutic targets
Sonication of Removed Hip and Knee Prostheses for Diagnosis of Infection
- Prospective study of 331 patients (79 with PJI); sonicate-fluid culture sensitivity 78.5% vs 60.8% for periprosthetic tissue (P less than 0.001)
- Specificity comparable: 98.8% (sonicate) vs 99.2% (tissue) - dislodging biofilm bacteria did not increase false positives
- Greatest gain in patients on antimicrobials within 14 days before surgery: 75.0% vs 45.0% sensitivity
- 14 PJI cases detected by sonicate culture that were missed by tissue culture alone
Role of Rifampin for Treatment of Orthopaedic Implant-Related Staphylococcal Infections (FBI Study)
- Randomised, double-blind, placebo-controlled trial; 33 patients with staphylococcal infection of stable orthopaedic implants and short symptom duration (0-21 days)
- After debridement and implant retention, cure in 12/12 (100%) with ciprofloxacin-rifampin vs 7/12 (58%) with ciprofloxacin-placebo among completers (P = 0.02)
- Rifampin combinations cured infection without device removal in tolerant, compliant patients
- Rifampin penetrates biofilm and is active against adherent/slow-growing staphylococci, but must never be given as monotherapy (rapid resistance)
Diagnosis and Management of Prosthetic Joint Infection: IDSA Clinical Practice Guidelines
- Debridement and implant retention (DAIR) is an option only for well-fixed prostheses with short symptom duration (within ~3 weeks) and a susceptible organism
- Biofilm-active rifampin-based combinations recommended for staphylococcal PJI managed with retention
- Two-stage (or one-stage) exchange recommended where mature biofilm or implant loosening is present
- Sinus tract, prolonged symptoms, or unstable implant are contraindications to retention
Persister Cells, Dormancy and Infectious Disease
- Seminal review linking latent infection, biofilm multidrug tolerance and unculturable organisms to a shared dormant (non-dividing) bacterial state
- Persisters are a small, phenotypically tolerant subpopulation - not genetic mutants - that survive bactericidal antibiotics
- Toxin-antitoxin modules and a shift to dormancy underpin persister formation and antibiotic tolerance
- Biofilm protects persisters from immune clearance, allowing relapse once antibiotics stop
Antibiotic Resistance of Bacteria in Biofilms
- Review establishing that biofilm antimicrobial tolerance arises from multicellular strategies, not classic plasmid/transposon/mutation resistance
- Mechanisms include restricted matrix penetration, altered microenvironment/slow growth, and a persister subpopulation
- Biofilm tolerance contributes directly to the chronicity of device-associated infection
- Frames biofilm dispersal and matrix disruption as potential adjunctive therapeutic targets
Biofilm Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Define Biofilm and Antibiotic Resistance (~3 min)
"What is a biofilm and why are bacteria in biofilm resistant to antibiotics?"
Scenario 2: Biofilm in PJI Treatment (~4 min)
"How does biofilm formation influence your treatment strategy for prosthetic joint infection, particularly the decision between DAIR and two-stage exchange?"
Scenario 3: Persister Cells and Treatment Failure (~3 min)
"A patient with a Staphylococcus aureus prosthetic joint infection has had repeated courses of culture-directed intravenous antibiotics. Each time, symptoms settle and inflammatory markers normalise, but the infection recurs weeks after antibiotics stop. The organism remains fully susceptible on every culture. How do you explain this to the patient and what is your definitive plan?"
Guidelines, Registries & Global Practice
Biofilm science underpins implant-infection management worldwide, but recommendations and resources differ by setting. Below is a global, society-neutral synthesis - not the practice of any single country.
Global Epidemiology
- PJI incidence: approximately 1-2% after primary hip and knee arthroplasty, rising to 3-5% or more after revision surgery (population-dependent).
- Dominant organisms: staphylococci (S. aureus and coagulase-negative staphylococci, especially S. epidermidis) cause the majority of biofilm-related PJI; Cutibacterium acnes predominates in shoulder arthroplasty; gram-negatives and polymicrobial infection are more common in early post-operative and immunocompromised cases.
- Burden: as global arthroplasty volume grows, the absolute number of biofilm-associated revisions is projected to rise substantially, making prevention and early diagnosis a worldwide priority.
Side-by-Side Guidance
Major Society / Consensus Guidance on Biofilm-Related Implant Infection
| Body | Implant retention (DAIR) | Biofilm-active therapy | Diagnosis emphasis |
|---|---|---|---|
| IDSA (US) | Acute, stable, susceptible organism, short symptoms | Rifampin combination for staphylococci | Multiple cultures; defined PJI criteria |
| EBJIS (Europe) | Similar acute window; structured definition | Rifampin combination; agent by organism | Sonication, synovial markers, definition tiers |
| ICM Consensus | Time-dependent; favours exchange once chronic | Biofilm-active agents endorsed | Synovial WBC, alpha-defensin, culture protocol |
| AAOS / BOA-BOAST | Early referral, source control, MDT pathway | Specialist-directed prolonged therapy | Aspiration before antibiotics; MDT diagnosis |
Registry & Surveillance Signals
- Arthroplasty registries (e.g. NJR, AOANJRR, SHAR, NZJR, AJRR) consistently identify infection as a leading cause of early revision, and track antibiotic-loaded cement use and bearing/fixation choices that influence infection-related revision.
- Registries inform - but do not replace - the biofilm-based decision rule: maturity of biofilm (largely time-driven) determines whether retention or exchange is appropriate.
High- vs Limited-Resource Practice Variation
High-Resource Settings
Routine sonication, synovial biomarkers (alpha-defensin, leucocyte esterase), extended and molecular cultures, two-stage exchange with antibiotic spacers, and infectious-disease/MDT input are widely available.
Limited-Resource Settings
Diagnosis often relies on clinical assessment, plain radiographs, aspiration and tissue culture. Emphasis falls on prevention (prophylaxis timing, theatre discipline), early debridement, and single-stage or excision arthroplasty where staged revision or spacers are not feasible.
Controversies & Areas of Uncertainty
DAIR time threshold
The 3-4 week "acute" window is pragmatic, not absolute. Biofilm maturity is a continuum, and outcomes also depend on organism, host, and implant stability rather than time alone.
One- vs two-stage exchange
Single-stage revision shows comparable success to two-stage in selected patients in several series, challenging two-stage as a universal gold standard - but evidence remains heterogeneous.
Anti-biofilm technologies
Quorum-sensing inhibitors, dispersal agents, bacteriophage therapy, and antibiotic/silver-coated surfaces are promising but largely lack high-level clinical trial evidence.
Chronic suppression
The durability and antimicrobial-stewardship implications of long-term suppressive therapy without implant removal remain debated, especially with persister-driven relapse.
Management Algorithm
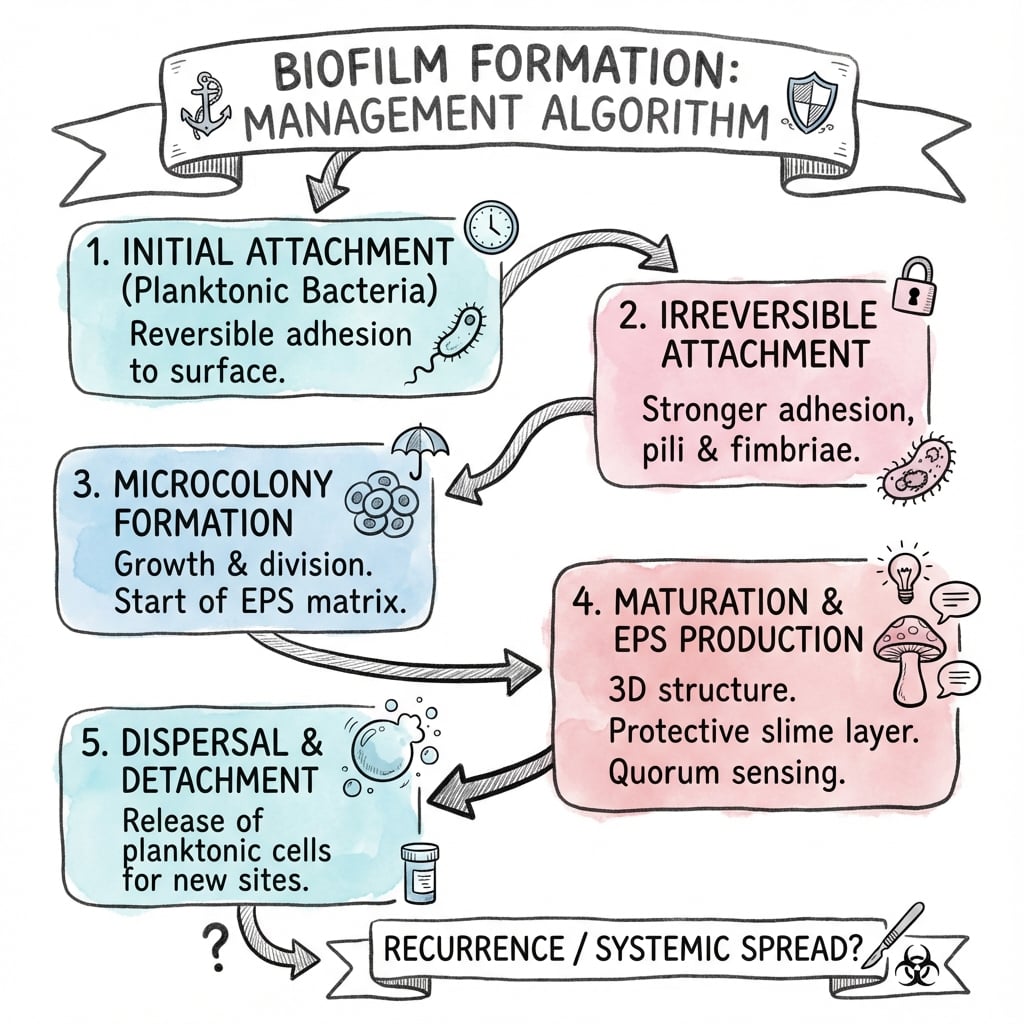
BIOFILM FORMATION
Clinical summary
Core Definition
- •Biofilm = structured bacterial community in EPS matrix adherent to surface
- •Costerton 1970s-1980s established modern biofilm concept
- •80% of chronic infections involve biofilm (implants, osteomyelitis)
- •Fundamentally different from planktonic (free-floating) bacteria
Biofilm Formation Stages
- •Stage 1 (0-4h): Reversible attachment, antibiotics still effective
- •Stage 2 (4-24h): Irreversible attachment via adhesins, EPS begins
- •Stage 3 (24-48h): Microcolony formation, 3D structure develops
- •Stage 4 (48h+): Mature biofilm, persister cells, antibiotic resistance
- •Critical window: First 24-48h before irreversible biofilm established
EPS Matrix Composition
- •80-90% water, 10-15% bacterial cells (by volume)
- •Dry weight: 40-50% polysaccharides, 10-20% eDNA, 20-30% proteins
- •Polysaccharides: PIA in S. epidermidis (ica genes), alginate in Pseudomonas
- •eDNA: Structural support, binds cationic antibiotics, gene transfer
Antibiotic Resistance Mechanisms
- •1000-fold increased MIC compared to planktonic bacteria
- •EPS barrier: Blocks antibiotic penetration to depths
- •eDNA binding: Sequesters aminoglycosides, polymyxins
- •pH gradients: Acidic zones (pH 5-6) reduce antibiotic activity
- •Slow growth: Dormant bacteria not killed (antibiotics target division)
- •Persister cells: 0.1-1% of biofilm, tolerant to ALL antibiotics
- •Phenotypic tolerance (reversible) NOT genetic resistance
Persister Cells (Critical Concept)
- •Dormant, non-growing bacteria (0.1-1% of biofilm)
- •Tolerant to ALL antibiotics (not genetic resistance)
- •Survive treatment, cause relapse when antibiotics stopped
- •Located in nutrient-limited deep zones of biofilm
- •Explain chronic relapsing infections despite susceptible organism
- •Cannot be killed by antibiotics - require physical removal (implant exchange)
Clinical Implications - PJI
- •Acute (less than 3 weeks): DAIR possible (50-70% success)
- •Chronic (greater than 3 weeks): Implant removal required (mature biofilm)
- •Two-stage exchange: 80-90% success (gold standard for chronic)
- •Suppression without removal: Less than 20% success (eventual failure)
- •Biofilm-active antibiotics: Rifampicin (best), fluoroquinolones, linezolid
- •Rifampicin: NEVER monotherapy (resistance in 48h), always combine
Diagnostic Techniques
- •5-7 tissue samples (MSIS criteria), ≥2 positive same organism = infected
- •Sonication of explanted implant: Increases yield 20-30% (greater than 50 CFU/mL = infected)
- •Extended incubation: 7-14 days for slow-growing biofilm bacteria
- •16S rRNA PCR: Culture-independent, detects bacteria in culture-negative
- •Culture-negative rate: 10-30% (prior antibiotics, dormant bacteria, biofilm)
Prevention Strategies
- •Antibiotic prophylaxis: Within 60 minutes before incision (optimal 30 min)
- •Prevents initial attachment (Stage 1), given BEFORE contamination
- •Cefazolin 2g IV standard, redose if surgery greater than 4 hours
- •Patient optimization: HbA1c less than 7.5%, smoking cessation, BMI less than 40
- •Surgical technique: Minimize time, gentle handling, copious irrigation
- •Antibiotic cement, silver coatings (research/emerging)
Key Numbers and Thresholds
- •1000x: Increased MIC in biofilm vs planktonic
- •24-48h: Irreversible biofilm attachment established
- •3 weeks: Threshold for acute vs chronic PJI (DAIR vs exchange)
- •0.1-1%: Persister cell frequency in biofilm
- •50 CFU/mL: Sonication fluid threshold for infection (Trampuz)
- •50-70%: DAIR success if acute (less than 3 weeks)
- •80-90%: Two-stage exchange success for chronic PJI