Mankin Principles | Approach Planning | Avoid Contamination | Tumor Center Collaboration
- All biopsies should be performed by the surgeon who will do the definitive resection or in consultation with tumor center
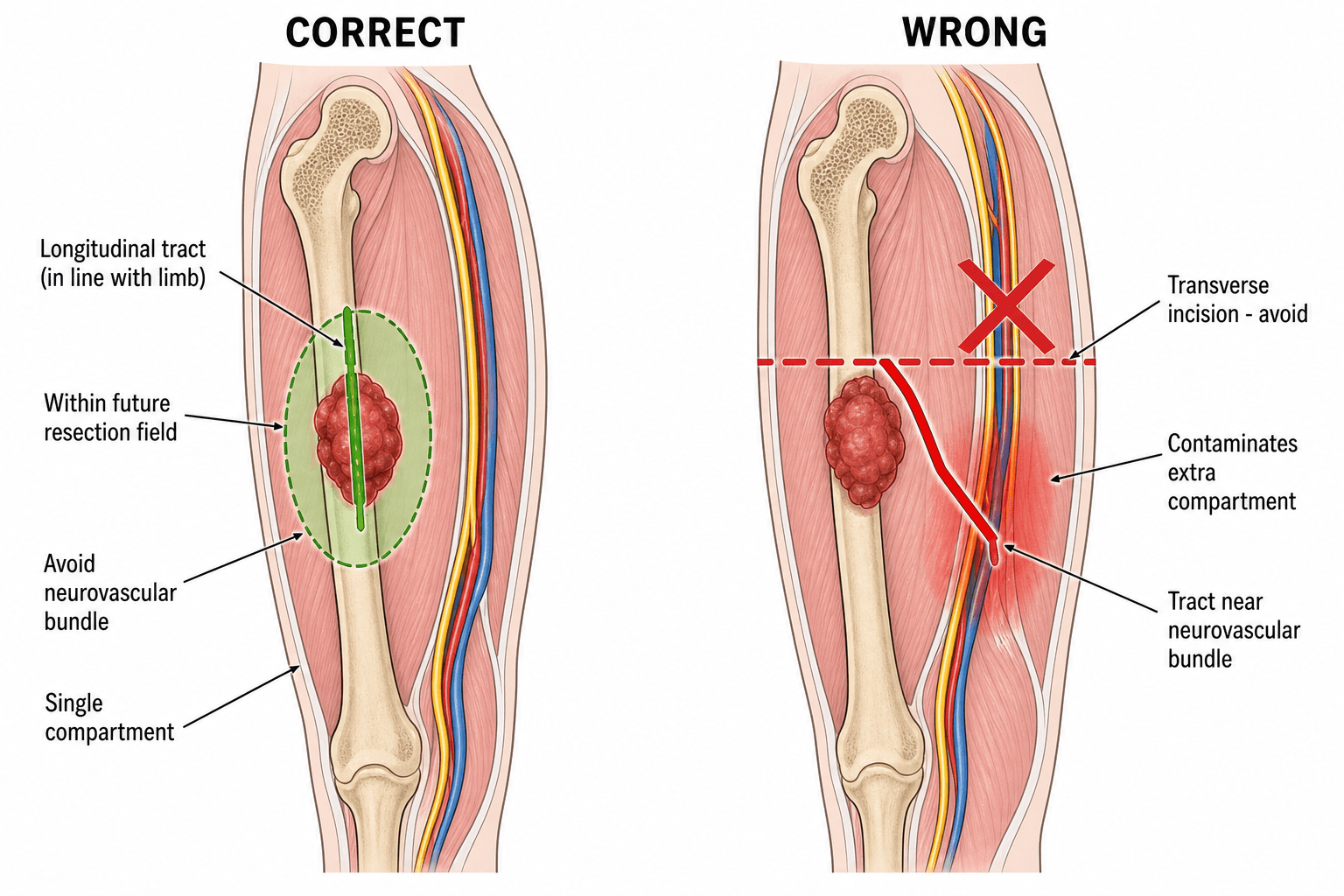
- Longitudinal incisions only - transverse incisions contaminate multiple compartments and may preclude limb salvage
- Biopsy tract must be in the planned resection field - entire tract including skin incision will be excised
- Minimize hematoma - use meticulous hemostasis, minimal tourniquet time, compression dressing, avoid drains if possible
- Never perform excisional biopsy for suspected sarcoma - violates oncologic principles and contaminates surrounding tissue
- “Mankin's series showed 18.2% major biopsy errors leading to altered treatment in 8.5% and unnecessary amputation in 4.5%
- “The three cardinal sins: wrong biopsy type, wrong approach, inadequate specimen handling
- “Image-guided core needle biopsy has 90% diagnostic accuracy with minimal complications
- “Always discuss suspected bone or soft tissue tumor with tumor center BEFORE biopsy
18.2% major errors in referral biopsies led to altered treatment (8.5%) and unnecessary amputations (4.5%). Recurring error themes: wrong biopsy type (e.g. excisional biopsy of a sarcoma), an inappropriate approach contaminating compartments, poor haemostasis causing tumour-laden haematoma, and inadequate or non-representative tissue.
NEVER use transverse incisions. Longitudinal incisions parallel to neurovascular bundle allow excision of entire tract en bloc. Transverse incisions contaminate multiple compartments, destroy tissue planes, and may necessitate amputation.
Every biopsy tract must be in the planned resection field. The entire tract including skin incision will be excised en bloc with tumor. Poorly planned biopsy can convert limb salvage to amputation.
Discuss all suspected sarcomas with tumor center BEFORE biopsy. Many biopsies should be performed at the treating center by the definitive surgeon. Inappropriate biopsy is the most common referral error.
Overview and Epidemiology
Biopsy is the definitive diagnostic procedure for suspected bone and soft tissue tumors. The technique and timing of biopsy are critical - improper biopsy can compromise subsequent treatment, increase morbidity, and even necessitate amputation in cases where limb salvage would otherwise be possible.
Mankin's 1982 study of 329 patients referred to a sarcoma centre after biopsy elsewhere revealed that 18.2% had major biopsy errors. These errors led to altered treatment in 8.5% of patients and unnecessary amputation in 4.5%, and were 2-12 times more frequent when the biopsy was performed at the referring institution rather than the treating centre. The recurring error categories were wrong biopsy type, an inappropriate approach, poor haemostasis causing haematoma, and inadequate or non-representative tissue. This study established the principle that biopsies should be performed by or in consultation with the surgeon who will perform the definitive resection.
Fundamental Principles
The core principles of tumor biopsy were established by Mankin and remain unchanged:
- Complete imaging workup first: Plain films, MRI, CT chest
- Multidisciplinary review: Radiology, pathology, oncology
- Tumor center consultation: Discuss plan before biopsy
- Definitive surgeon involvement: Ideally performs biopsy
- Image review: Understand anatomy, plan approach
- Appropriate biopsy type: Core needle for most lesions
- Longitudinal approach: Parallel to neurovascular structures
- Single compartment: Do not violate multiple planes
- Resection field: Entire tract must be excisable
- Meticulous hemostasis: Minimize hematoma formation
If you are not going to perform the definitive resection, do not perform the biopsy. Contact a tumor center first. An inappropriately placed biopsy can convert a limb salvage procedure to an amputation, increase surgical morbidity, or compromise oncologic outcome.
Oncologic Rationale
The biopsy tract becomes contaminated with tumor cells and must be excised en bloc with the tumor during definitive resection. Poor biopsy technique can:
- Seed tumor cells into surrounding tissue via hematoma
- Violate tissue planes making resection margins unclear
- Contaminate multiple compartments necessitating wider resection
- Compromise neurovascular structures precluding limb salvage
- Create skin bridges between biopsy and tumor requiring skin grafting
Clinical Presentation and Indications
Fine Needle Aspiration (FNA)
- Needle: 22-25 gauge
- Yield: Cells for cytology only
- Guidance: Palpation or image-guided
- Passes: Multiple (4-6 typical)
- Processing: Air-dried smears, alcohol-fixed
- Primary diagnosis: Generally insufficient
- Confirmatory role: Metastasis with known primary
- Limitations: No architecture, limited immunohistochemistry
- Accuracy: 60-80% sensitivity for sarcoma
- Inadequate rate: 10-20%
- Minimally invasive, office-based
- Multiple sites can be sampled
- Minimal contamination risk
- Quick turnaround for cytology
- Cannot assess architecture (critical for bone tumors)
- Limited tissue for immunohistochemistry and molecular studies
- High inadequate specimen rate
- Reader-dependent (requires expert cytopathologist)
FNA has a limited role in primary diagnosis of bone and soft tissue sarcomas because architectural assessment is essential for grading and subtyping. FNA is useful for: (1) confirming metastatic disease when primary cancer is known, (2) diagnosing lymphoma when combined with flow cytometry, and (3) initial triage in resource-limited settings. Core needle biopsy is superior for primary sarcoma diagnosis.
Core Needle Biopsy (CNB)
Core needle biopsy is the first-line biopsy technique for most suspected bone and soft tissue tumors.
- Soft Tissue
- 14-16 gauge
- Bone Lesion
- 11-13 gauge (larger for bone)
- Soft Tissue
- Ultrasound or CT
- Bone Lesion
- CT preferred (bone cortex visualization)
- Soft Tissue
- 3-5 cores minimum
- Bone Lesion
- 4-6 cores (bone harder to sample)
- Soft Tissue
- Local infiltration
- Bone Lesion
- Local plus conscious sedation often
- Soft Tissue
- Longitudinal trajectory
- Bone Lesion
- Through planned resection field
- High diagnostic accuracy: 85-95% for sarcoma
- Tissue architecture preserved: Allows histologic grading
- Sufficient for immunohistochemistry: Multiple cores provide tissue
- Minimal contamination: Small needle tract, easily excised
- Image-guided: Targets viable tumor, avoids necrosis
- Outpatient procedure: Lower morbidity than open biopsy
- Sampling error (small tissue volume)
- May be inadequate for heterogeneous tumors
- Requires expert musculoskeletal pathologist
- Cannot perform frozen section reliably
- May need repeat if non-diagnostic
CT guidance is preferred for bone lesions (visualizes cortex, guides through planned resection field). Ultrasound guidance is preferred for soft tissue masses (real-time visualization, no radiation, can avoid vessels). The radiologist performing the biopsy should communicate with the surgeon regarding planned approach and resection field.
A single core is insufficient for sarcoma diagnosis. Minimum 3-5 cores should be obtained to: (1) ensure representative sampling, (2) provide tissue for permanent sections, (3) allow immunohistochemistry if needed, (4) send fresh tissue for culture or molecular studies. Inadequate sampling is a common cause of non-diagnostic biopsy.
Incisional Biopsy
Open incisional biopsy involves a limited surgical incision to obtain a tissue sample without removing the entire lesion.
Indications for incisional over needle biopsy:
- Prior needle biopsy non-diagnostic (inadequate or inconclusive)
- Heterogeneous tumor: Large areas of necrosis, need larger sample
- Bone lesion requiring instrumentation: Hard cortex preventing needle access
- Surgeon preference: When definitive surgeon prefers to perform biopsy
- Suspected lymphoma: Need tissue architecture and fresh tissue for flow
Incisional Biopsy Technique
- Review all imaging with treating surgeon
- Mark incision site with patient awake (anatomic landmarks)
- Plan longitudinal incision in resection field
- Ensure entire tract can be excised en bloc
- Prepare for frozen section (confirm adequate tissue)
- Longitudinal skin incision, minimal length
- Dissect directly to lesion (do not create flaps)
- Single compartment approach
- Remove tissue block (1-2cm cube minimum)
- Sample viable tumor (periphery), avoid necrotic center
- Send fresh tissue for culture in sterile container
- Meticulous hemostasis (bipolar, bone wax)
- Irrigate wound thoroughly
- Layered closure (no dead space)
- Avoid drain if possible (if needed, exit through incision)
- Compression dressing for 48 hours
Drains should be avoided if at all possible in tumor biopsies. Drains create a tract that can disseminate tumor cells and must be excised en bloc with the tumor. If a drain is absolutely necessary (e.g., large cavity in bone after biopsy), it must exit through the biopsy incision (not a separate stab incision) so the entire tract can be resected.
Excisional Biopsy
Excisional biopsy involves removing the entire lesion with a margin of normal tissue.
- Small superficial lesion (less than 3cm) with low suspicion for sarcoma
- Subcutaneous lipoma typical appearance, mobile, soft
- Pedunculated lesion (e.g., presumed skin tag, neurofibroma)
- Patient preference for complete removal if benign likely
- Deep mass (below fascia) - unacceptable contamination risk
- Large mass (greater than 5cm) - violates oncologic principles
- Firm or fixed mass - suggests malignancy
- Imaging features of sarcoma - inappropriate marginal excision
- Bone lesion with aggressive features - requires staging and planning
Excisional biopsy of a suspected sarcoma is a major error. It results in: (1) tumor spillage into surrounding tissue, (2) loss of anatomic planes for definitive resection, (3) contamination of adjacent compartments, (4) need for much wider re-excision, and (5) potential conversion of limb salvage to amputation. Wrong choice of biopsy type was one of the leading error categories in Mankin's series.
Pathophysiology and Rationale
When Biopsy is Indicated
Not all bone and soft tissue lesions require biopsy. Many benign lesions can be diagnosed with certainty on imaging and clinical grounds.
- Biopsy Needed?
- No
- Rationale
- Pathognomonic imaging, age-appropriate, asymptomatic
- Biopsy Needed?
- No (unless atypical)
- Rationale
- Classic imaging and location, can treat empirically
- Biopsy Needed?
- No
- Rationale
- Classic appearance, no aggressive features
- Biopsy Needed?
- Yes
- Rationale
- High risk of malignancy, requires tissue diagnosis
- Biopsy Needed?
- Yes
- Rationale
- Permeative pattern, cortical destruction, soft tissue mass
- Biopsy Needed?
- Yes (after stabilization)
- Rationale
- Need diagnosis to guide adjuvant treatment
- Biopsy Needed?
- Maybe
- Rationale
- Biopsy if changes treatment or confirms diagnosis
Any soft tissue mass that is deep to fascia, larger than 5cm, or growing on serial imaging should be considered malignant until proven otherwise and requires biopsy. Superficial subcutaneous lipomas less than 5cm can usually be observed or excised without pre-operative biopsy. However, atypical features (firmness, fixation, rapid growth) mandate biopsy regardless of size.
Absolute Indications
Lesions Requiring Biopsy
- Aggressive imaging features (permeative, moth-eaten destruction)
- Age-inappropriate lesion (e.g., lytic femur lesion age 40)
- Soft tissue mass associated with bone lesion
- Pathological fracture through unknown lesion
- Rapid growth or symptom progression
- Atypical features not fitting benign diagnosis
- Any deep mass (below investing fascia)
- Superficial mass greater than 5cm
- Rapid growth on serial imaging
- Firm, fixed, or irregular mass
- Recurrent mass after prior excision
- Symptomatic (pain, paresthesia)
- Metastatic workup (establish diagnosis)
- Pre-operative planning (neoadjuvant therapy)
- Monitor treatment response (re-biopsy)
- Uncertain imaging despite full workup
- Infection vs tumor differential
Contraindications to Biopsy
Biopsy should be deferred or avoided in specific situations:
- Classic benign imaging: Pathognomonic appearance (e.g., fibrous cortical defect)
- Vascular lesions: Risk of hemorrhage (consider embolization first)
- Inadequate imaging: Complete MRI and staging studies first
- Infection suspected: Aspiration for culture, not biopsy
- Coagulopathy uncorrected: Bleeding risk too high
- Patient unfit for treatment: Diagnosis will not change management
Differential Diagnosis: Lesions That Mimic Sarcoma
A defining biopsy error is treating a benign or non-neoplastic mimic as a sarcoma (or vice versa). Recognising the differential before biopsy guides whether to biopsy, how, and where.
- Clue Favouring the Mimic
- Fever, raised inflammatory markers, sinus, adjacent septic focus
- Why It Matters for Biopsy
- Always send fresh tissue for culture; infection can both mimic and contaminate
- Clue Favouring the Mimic
- Trauma history, peripheral zonal ossification maturing over weeks
- Why It Matters for Biopsy
- Biopsy of immature myositis ossificans can be misread as osteosarcoma
- Clue Favouring the Mimic
- Soft, mobile, subcutaneous, fat signal on all MRI sequences
- Why It Matters for Biopsy
- Deep or septated fatty lesions may be atypical lipomatous tumour - needs proper biopsy
- Clue Favouring the Mimic
- Fluid-fluid levels, classic age and location
- Why It Matters for Biopsy
- Highly vascular - bleeding risk; primary aggressive lesion may underlie ABC
- Clue Favouring the Mimic
- Age over 40, known primary, multiple lesions
- Why It Matters for Biopsy
- May only need confirmatory biopsy; changes whole workup (look for primary first)
- Clue Favouring the Mimic
- Permeative bone with large soft-tissue mass, B symptoms
- Why It Matters for Biopsy
- Needs fresh tissue for flow cytometry; chemo/RT not surgery
- Clue Favouring the Mimic
- Epiphyseal lytic lesion, skeletally mature
- Why It Matters for Biopsy
- Locally aggressive but benign - biopsy still in resection field
Classification
Classification of Biopsy Types
- Technique
- 22-25 gauge needle, multiple passes
- Tissue Yield
- Cells only (cytology)
- Primary Indication
- Confirmatory role, metastatic disease
- Technique
- 11-16 gauge, image-guided
- Tissue Yield
- Tissue cores (histology)
- Primary Indication
- First-line for most lesions
- Technique
- Open surgical, partial removal
- Tissue Yield
- Tissue block (1-2cm cube)
- Primary Indication
- When needle inadequate
- Technique
- Complete lesion removal
- Tissue Yield
- Entire lesion with margin
- Primary Indication
- Only small superficial lesions under 3cm
- 14-16 gauge needles adequate
- Ultrasound guidance preferred
- 11-13 gauge for harder cortex
- CT guidance for accuracy
- 3-5 cores for soft tissue
- 4-6 cores for bone lesions
- Accounts for heterogeneous tumors
- Allows immunohistochemistry
- Provides tissue for molecular studies
Investigations and Imaging Guidance
The Longitudinal Incision Rule
The single most important principle in biopsy technique is the longitudinal incision.
- Longitudinal (Correct)
- Parallel to neurovascular bundle and long axis of limb
- Transverse (WRONG)
- Perpendicular to long axis, crosses compartments
- Longitudinal (Correct)
- Can extend proximally/distally for definitive resection
- Transverse (WRONG)
- Cannot be extended without creating skin flaps
- Longitudinal (Correct)
- Single compartment
- Transverse (WRONG)
- Multiple compartments contaminated
- Longitudinal (Correct)
- Entire tract excised en bloc with tumor
- Transverse (WRONG)
- May necessitate amputation or massive skin grafting
- Longitudinal (Correct)
- Confined to single compartment
- Transverse (WRONG)
- Spreads across multiple compartments
A transverse biopsy incision can convert a limb salvage to an amputation. Transverse incisions cross multiple tissue planes and compartments. During definitive resection, the entire contaminated area (including all crossed compartments) must be excised. This may require sacrifice of critical neurovascular structures or amputation. Examiners will fail candidates who suggest transverse biopsy incisions.
Anatomic Approach Principles
- Deltopectoral approach (anterior access)
- Posterior approach through deltoid (posterior tumors)
- Longitudinal over tumor in line with definitive incision
- Avoid crossing antecubital fossa
- Longitudinal dorsal or volar
- Midaxial for digit lesions
- Anterolateral (vastus lateralis interval)
- Medial (direct to adductors)
- Posterior (through hamstrings)
- Anteromedial (medial to tibial crest)
- Posterolateral (between peronei and gastrocnemius)
- Dorsal longitudinal most common
Specific Technical Considerations
Soft Tissue Mass Biopsy Technique
- Review MRI in axial cuts (identify safest trajectory)
- Mark skin incision with patient awake (muscle relaxation changes anatomy)
- Identify neurovascular structures to avoid
- Plan incision to be within resection field
- Directly over mass (shortest distance to tumor)
- Longitudinal orientation
- Avoid neurovascular bundles (approach between muscles)
- Consider extensile approach for definitive surgery
- Do NOT raise skin flaps (increases contamination)
- Dissect between muscles to reach mass
- Stay in single compartment
- Avoid opening neurovascular sheath
- Sample periphery of mass (avoid necrotic center)
- Minimum 1cm cube of tissue
- Send fresh specimen for culture (rule out infection)
- Obtain hemostasis before closing
- Layered closure (no dead space)
- No drain (or drain through incision if essential)
- Compression dressing
This approach ensures minimal contamination and preserves limb salvage options.
Does the Needle Tract Need to Be Excised? (Tract Seeding)
The principle stated throughout this topic - that the entire biopsy tract is excised en bloc with the tumour - was defined for open biopsy. Core needle biopsy (the first-line technique) raises a distinct, examinable nuance, because a percutaneous needle leaves a far smaller tract.
- Tract seeding is real but rare. Tumour cells can implant along any biopsy tract, but with modern percutaneous core needle biopsy the seeding rate is very low.
- Open versus needle tract. The open-biopsy tract is always excised (skin, subcutaneous tissue and the deep tract together). For a percutaneous core-needle tract, routine excision is debated - many sarcoma centres do not formally resect every needle tract, particularly for deep lesions where the tract cannot be reliably identified, while others excise it when it is superficial and easily incorporated into the resection.
- The practical compromise. Keep the needle tract within the future resection field, use a single coaxial tract (multiple cores through one cannula, not several separate punctures), and mark or tattoo the skin entry so the resecting surgeon can identify and, if chosen, excise it - preserving the option to remove the tract without mandating it for every percutaneous biopsy.
The "excise the whole tract" rule was written for open biopsy. Needle-tract seeding after core biopsy is uncommon and routine excision of a percutaneous tract is debated - but you still plan the needle path within the resection field, single coaxial tract, entry marked so the resecting surgeon retains the choice to excise it. A carelessly placed needle tract outside the resection field is the same error as a badly placed open-biopsy incision.
Management - Biopsy Technique
Communication with Pathologist
Essential information for pathologist:
- Patient age and relevant history
- Location and size of lesion (anatomic compartment)
- Imaging findings and differential diagnosis
- Clinical question (primary tumor? metastasis? infection?)
- Fresh tissue sent separately for culture
- Request for frozen section if applicable
Call the pathologist before the biopsy to discuss the case. Provide imaging and clinical context. This allows the pathologist to: (1) prepare appropriate fixatives and stains, (2) plan for ancillary studies (immunohistochemistry, molecular), (3) have frozen section capability if needed, (4) optimize specimen handling. Poor communication with pathology is a common cause of non-diagnostic biopsies.
Specimen Processing
From Biopsy to Diagnosis
- Send portion in sterile container (not formalin) for culture
- Touch prep cytology can be done on fresh tissue
- Frozen section if requested (limited role in sarcoma)
- Photograph specimen if desired
- Minimize time to pathology (tissue degradation)
- Majority of tissue in 10% formalin for permanent sections
- Fixation time 24-48 hours before processing
- Decalcification if bone (EDTA preferred over acid)
- Embedding in paraffin blocks
- Sectioning at 4-5 microns thickness
- H&E staining: Standard hematoxylin and eosin
- Immunohistochemistry: Panel based on differential
- Special stains: As needed (trichrome, reticulin)
- Molecular studies: FISH, PCR, NGS if indicated
- Expert musculoskeletal pathologist review
- Diagnosis with grading if malignant
- Immunohistochemistry results
- Molecular findings if performed
- Comment on adequacy and differential
- Recommendations for further testing if needed
Frozen Section Limitations
- Cannot reliably diagnose sarcoma subtype (architecture disrupted by freezing)
- Cannot grade sarcoma (cellular detail lost)
- Risk of using up tissue (small biopsies may be exhausted)
- Delaying definitive diagnosis (frozen is preliminary only)
- Confirm adequate tissue obtained (vs adipose, muscle, necrosis)
- Rule out infection (gram stain on frozen)
- Confirm diagnostic material in difficult-to-access lesions (spine, pelvis)
- Triage tissue for ancillary studies (flow cytometry for lymphoma)
Do NOT rely on frozen section for definitive sarcoma diagnosis or grading. The architectural details and cellular morphology required for sarcoma diagnosis are lost in frozen sections. Frozen section should only confirm that diagnostic tissue has been obtained, not provide the final diagnosis. Permanent sections with immunohistochemistry are essential.
Ancillary Studies
Modern sarcoma diagnosis often requires studies beyond standard H&E microscopy:
- Indications
- Subtype sarcoma, confirm diagnosis
- Examples
- Desmin (muscle), S100 (nerve), CD34 (vascular), keratin (epithelial)
- Indications
- Diagnostic translocations
- Examples
- EWSR1 (Ewing), SYT-SSX (synovial), MDM2 (liposarcoma)
- Indications
- Lymphoma diagnosis
- Examples
- B-cell vs T-cell markers, clonality assessment
- Indications
- Rule out infection
- Examples
- Bacterial, fungal, mycobacterial cultures from fresh tissue
- Indications
- Poorly differentiated tumors
- Examples
- Rare, for ultrastructural features (seldom needed now)
Surgical Technique
Core Needle Biopsy Technique
Step-by-Step Core Needle Biopsy
- Review all imaging with radiologist
- Plan trajectory through resection field
- Mark skin entry point
- Confirm pathology availability
- Obtain informed consent
- Position for optimal access (prone/supine/lateral)
- Ensure patient comfort (sedation if needed)
- Sterile prep and drape
- Local anesthesia to skin and tract
- Small skin nick with scalpel
- Insert coaxial guiding cannula
- Advance under image guidance
- Confirm position within lesion
- Avoid necrotic center
- Insert biopsy needle through coaxial
- Fire needle to obtain core
- Remove and inspect core
- Repeat for 4-6 cores minimum
- Confirm adequate tissue obtained
- Remove coaxial cannula
- Apply pressure for hemostasis
- Post-procedure imaging (assess complications)
- Compression dressing
- Steri-strips to skin (no sutures usually needed)
- 11-16 gauge biopsy needle
- Coaxial guiding cannula
- Specimen containers (formalin and sterile)
- CT scanner or ultrasound
- Sterile probe covers if ultrasound
- Target lesion periphery (viable tissue)
- Avoid cystic/necrotic areas
- Multiple cores through single tract
- Rotate needle between passes
- Meticulous hemostasis
- Avoid major neurovascular structures
Complications and Biopsy Errors
Mankin's Classification of Errors
Mankin identified major biopsy errors in 18.2% of referral cases. These errors fall into recurring categories:
- Mechanism
- Excisional biopsy of a suspected sarcoma
- Consequence
- Tumour spillage, loss of planes, wider re-excision
- Prevention
- Use core needle or incisional biopsy for suspected sarcoma
- Mechanism
- Transverse incision crossing compartments
- Consequence
- Multi-compartment contamination, salvage compromised
- Prevention
- Longitudinal incision, single compartment, resection field
- Mechanism
- Haematoma seeds tumour cells along tissue planes
- Consequence
- Field contamination beyond the tract
- Prevention
- Meticulous technique, avoid tourniquet release bleed, no drain
- Mechanism
- Insufficient or non-representative sample
- Consequence
- Non-diagnostic specimen, repeat biopsy, delay
- Prevention
- Adequate sample size, avoid necrosis, frozen confirmation
Mankin's series showed that major biopsy errors led to:
- Altered treatment in 8.5% of patients (wider resection needed)
- Unnecessary amputation in 4.5% (contamination precluded salvage)
- Increased morbidity (re-operation, skin grafting, flap coverage)
- Delayed definitive treatment (waiting for wound healing)
- Tumor progression during delay
These catastrophic outcomes emphasize why tumor biopsies should be performed at specialized centers by surgeons with oncologic training.
Specific Complications
- Most common early complication
- Spreads tumor cells to surrounding tissue
- Prevention: meticulous hemostasis, compression dressing
- Mimics tumor progression
- Delays definitive treatment
- Prevention: sterile technique, prophylactic antibiotics
- Through cortical window in bone biopsy
- Prevention: small window, avoid stress risers, consider prophylactic fixation
- Along biopsy tract (requires wide excision of tract)
- Into adjacent compartment (may preclude salvage)
- Prevention: proper technique, en bloc excision of tract
- Inadequate tissue or sampling error
- Requires repeat biopsy
- Prevention: adequate sample, image guidance, pathologist communication
- Wider resection needed due to contamination
- Amputation instead of salvage
- Prevention: proper planning and execution
Case Example: Biopsy Error Cascade
A 25-year-old presents with a 8cm firm thigh mass. A general surgeon performs an excisional biopsy through a transverse incision (thinking it is a benign cyst). Pathology returns as high-grade undifferentiated pleomorphic sarcoma.
- Transverse incision violated anterior and posterior compartments
- Tumor was "shelled out" (not excised with margin)
- Hematoma tracked into both compartments
- Femoral vessels and sciatic nerve now in contaminated field
- Wide re-excision would require sacrifice of these structures
- Patient counseled for above-knee amputation
- Pre-operative MRI staging
- Core needle biopsy or incisional biopsy
- Longitudinal incision in planned resection field
- Wide resection with negative margins
- Limb salvage achieved
This case illustrates how a single poor decision (excisional biopsy, transverse incision) can convert limb salvage to amputation.
The Unplanned ("Whoops") Excision
A specific and common referral disaster is the unplanned excision - inadvertent marginal or intralesional removal of an unsuspected sarcoma by a non-specialist who assumed the mass was benign (a "whoops procedure"). It is the surgical analogue of the biopsy errors above, and is the scenario behind this topic's residual-disease (Noria) data and the "referral after inappropriate biopsy" theme.
- Why it matters. The tumour has been shelled out without a margin, the whole surgical bed (and any drain sites and haematoma) is contaminated, and tissue planes are destroyed - exactly the situation Mankin warned against.
- Residual disease is common and unpredictable. After an unplanned excision with apparently "negative" margins and no gross residual on examination or imaging, planned re-excision still finds residual sarcoma in roughly a third of cases (Noria), and this cannot be predicted by tumour size, grade or the interval since surgery - so a clear scan does not mean clear tissue.
- Management. Restage (MRI of the operative bed plus CT chest), discuss at the sarcoma MDT, and perform a planned wide re-excision of the entire previous surgical field - scar, drain tracts and contaminated tissue en bloc - rather than assuming the lesion is gone. Adjuvant or neoadjuvant radiotherapy is frequently added given the contaminated field. Re-excision is often still margin-positive and local recurrence is higher than for primarily and correctly resected tumours.
After an unplanned ("whoops") excision of a sarcoma, around a third of patients have residual tumour at planned re-excision despite no visible residual on imaging, and this is not predictable from size or grade. Do NOT simply observe - restage, refer to the sarcoma MDT, and perform a planned wide re-excision of the entire previous surgical bed (often with adjuvant radiotherapy).
Postoperative Care
Post-Biopsy Care Protocol
Post-Biopsy Care Timeline
- Compression dressing maintained
- Monitor for bleeding/hematoma
- Ice for comfort if needed
- Analgesia (simple analgesics usually sufficient)
- Keep wound clean and dry
- Remove compression dressing at 48 hours
- Inspect wound for complications
- Light dressing over puncture site
- Resume normal activities as tolerated
- No heavy lifting or impact activities
- Await pathology results (5-10 days)
- Review wound at 7-10 days
- Remove sutures if open biopsy (10-14 days)
- Multidisciplinary team review when results available
- Plan definitive treatment
Patient instructions:
- Keep dressing clean and dry for 48 hours
- May shower after 48 hours (pat dry)
- No soaking (bath, swimming) for 2 weeks
- Watch for signs of infection (redness, swelling, discharge)
- Contact clinic if concerns arise
- Resume normal activities next day
- Avoid strenuous exercise for 48-72 hours
- No restrictions on weight-bearing
- Limit activity for 1 week
- Consider protected weight-bearing if bone biopsy
- Avoid impact activities until wound healed
Outcomes
Biopsy Outcomes Overview
- Overall: 85-95% for sarcomas
- Sensitivity: 89-96%
- Specificity: 97-100%
- NPV: 85-92%
- Overall: 3-5%
- Hematoma: 2-3% (mostly minor)
- Infection: less than 1%
- Major complications: less than 0.5%
- Higher tissue yield improves diagnosis
- Near 100% when adequate tissue obtained
- May be required after non-diagnostic needle
- Higher than needle biopsy
- Hematoma: 5-10%
- Wound complications: 2-5%
- Tumor seeding risk higher
- Longer recovery time
Mankin: The Hazards of Biopsy (Landmark Study)
- 329 patients with primary bone or soft tissue sarcoma referred to a sarcoma centre after biopsy elsewhere were analysed
- Major errors in diagnosis, technique or complications occurred in 18.2% of patients
- The biopsy adversely altered the treatment plan in 8.5% of patients
- Unnecessary amputation was attributed to the biopsy in 4.5% of patients
- Problems were 2-12 times more frequent when biopsy was done at the referring institution rather than the treating centre
- Established the principle that biopsy should be performed by, or in consultation with, the surgeon who will undertake the definitive resection
The Hazards of the Biopsy, Revisited (MSTS)
- Repeat multi-institutional Musculoskeletal Tumor Society study of 597 patients (25 surgeons, 21 institutions)
- Diagnostic error rate for the whole series was 17.8% - essentially unchanged from the 1982 study
- A biopsy-related problem forced a different or more complex operation, or adjuvant radiation/chemotherapy, in 19.3% (versus 18% in 1982)
- A change in outcome (disability, loss of function, local recurrence or death) attributable to the biopsy occurred in 10.1% (versus 8.5% in 1982)
- 18 patients underwent an unnecessary amputation because of the biopsy
- Errors, complications and outcome changes were 2-12 times greater when biopsy was done at a referring institution rather than a treatment centre (p less than 0.001)
CT-Guided Biopsy Accuracy in Musculoskeletal Lesions
- 359 CT-guided biopsies of musculoskeletal lesions analysed against final diagnosis
- Overall diagnostic accuracy was 71% across all techniques and sites
- Core biopsy outperformed fine needle aspiration (74% versus 63%)
- Pelvic lesions had higher accuracy (81%) than non-pelvic sites (68%); spine lesions were lowest (61%)
- Infectious lesions had the lowest yield (50%)
- Concluded CT-guided biopsy remains a safe, logical first diagnostic step despite site-dependent yield
Percutaneous Needle Biopsy is Safe and Recommended
- 185 biopsy procedures on 161 musculoskeletal masses suspected of being sarcoma in 155 patients
- Only 7.4% of masses required open biopsy; a single percutaneous biopsy was adequate in 88.2%
- Complication rate 1.1% and major diagnostic-error rate 1.1%; no unnecessary amputations
- Positive predictive value 100%, sensitivity 81.8%, specificity 100%
- Accuracy for benign versus malignant 92.4%, for exact grade 88.6%, for exact pathology 72.7%
- Open biopsy added little when preceded by an adequate needle biopsy
Core Needle versus Open Biopsy: Accuracy and Cost
- Prospective study of 62 outpatient core needle biopsies for soft tissue mass or bone tumour with soft-tissue extension
- Core needle biopsy diagnostic accuracy was 84% (52/62); all errors involved soft-tissue tumours
- Contemporary open biopsy by the same surgeon achieved 96% accuracy
- Hospital charges were markedly lower for needle biopsy ($1106) than open biopsy ($7234)
- 13% of needle biopsies yielded no neoplastic tissue (non-diagnostic)
- Recommended treating equivocal/non-diagnostic needle results as if no biopsy had been done
Core Needle versus Open Biopsy for Bone and Soft Tissue Sarcoma
- Retrospective comparison of percutaneous core needle versus open biopsy in 77 patients with suspected primary sarcoma
- Overall diagnostic accuracy 92.9% for core needle biopsy versus 98.0% for open biopsy (no significant difference)
- For bone tumours core needle biopsy reached 100% accuracy, comparable to open biopsy
- For soft tissue tumours core needle biopsy was moderately inferior to open biopsy (84.6% versus 100%, not significant)
- A specific diagnosis was obtained in 84.2% (core) versus 93.9% (open)
- Concluded core needle biopsy is safe and cost-effective for bone, but should be selected carefully for soft-tissue masses
Guidelines, Registries & Global Practice
Global Epidemiology and Centralisation
Soft tissue sarcomas account for roughly 1% of adult malignancies and primary bone sarcomas for around 0.2%, with combined incidences in the region of 4-5 and 0.8-1 per 100,000 per year respectively across high-income registries - both are rare cancers for which centralised, multidisciplinary care is the international standard (ESMO-EURACAN-GENTURIS soft tissue/visceral sarcoma and bone sarcoma guidelines, Ann Oncol 2021). Across all major frameworks the consistent message is identical to Mankin's: biopsy should be planned and ideally performed at, or in agreement with, the sarcoma reference centre that will deliver definitive treatment.
Side-by-Side Guideline Positions on Biopsy
- Biopsy recommendation
- Image-guided core needle biopsy is the standard; excisional biopsy of a suspected sarcoma is discouraged
- Referral position
- Diagnosis and biopsy planning at a sarcoma reference centre / network
- Evidence basis
- Expert consensus guideline (Ann Oncol 2021)
- Biopsy recommendation
- Core needle biopsy at the specialist centre after MRI; planned by the surgeon who will resect
- Referral position
- Refer any suspected sarcoma to a diagnostic clinic before biopsy
- Evidence basis
- NICE improving-outcomes guidance + BSG/BOA standards
- Biopsy recommendation
- Core needle (or image-guided) biopsy preferred; incisional if inadequate; avoid excisional for deep/large lesions
- Referral position
- Evaluation/biopsy at a sarcoma centre with experienced MDT
- Evidence basis
- NCCN category 2A consensus guideline
- Biopsy recommendation
- Percutaneous core needle first-line, open biopsy by treating surgeon if needed
- Referral position
- Early referral to a sarcoma service, ideally before biopsy
- Evidence basis
- Optimal care pathway / national consensus
ESMO, NICE/BOA, NCCN and Cancer Australia differ in formatting but agree on the substance: complete cross-sectional imaging first, image-guided core needle biopsy as first-line, no excisional biopsy of a suspected deep/large lesion, and biopsy planned by (or with) the resecting surgeon at a specialist centre. This convergence is itself an examinable point.
Practice Variation and Registries
Real-world practice still diverges from guideline ideals. Population and centre-based series consistently show that a substantial minority of sarcomas are still subjected to an unplanned ("whoops") excision before referral, and that biopsy performed outside a sarcoma centre carries 2-12 times the error/complication rate (Mankin, J Bone Joint Surg Am 1982 and 1996). National sarcoma registries and reference-centre networks (for example UK and European networks, and the Australian sarcoma services) are used to audit unplanned-excision rates, time-to-specialist-review and diagnostic accuracy as quality indicators.
Regional Access Notes
Reference-centre models operate worldwide, each providing multidisciplinary sarcoma clinics, limb-salvage expertise and trial access, with telehealth review for regional and rural patients. Examples include specialist sarcoma units in the UK (BSG/NICE designated centres), EURACAN reference networks in Europe, NCCN-aligned sarcoma centres in North America, and Australian sarcoma services (e.g. Peter MacCallum Cancer Centre, Chris O'Brien Lifehouse, Princess Alexandra Hospital and Royal Adelaide Hospital). Across systems, the rate-limiting step for good outcomes is the same: getting the patient to an expert MDT before the first biopsy.
MCQ Practice Points
Q: What percentage of patients in Mankin's series had major biopsy errors?
A: 18.2% had major errors, leading to altered treatment in 8.5% and unnecessary amputation in 4.5%. Error categories: wrong biopsy type, wrong approach, poor haemostasis, and inadequate tissue. Errors were 2-12 times more frequent at referring institutions than at the treating centre. The conclusion was that biopsies should be performed by the definitive surgeon.
Q: What is the diagnostic accuracy of image-guided core needle biopsy for musculoskeletal tumors?
A: 85-95% diagnostic accuracy with under 5% complication rate. This is higher than FNA (60-80%). Requires minimum 3-5 cores. Image guidance (CT or ultrasound) is preferred. It is the first-line technique for most musculoskeletal tumors.
Q: A general surgeon performs a biopsy for a suspected thigh sarcoma. Which represents a major error?
A: A transverse incision (NEVER acceptable). Must use longitudinal incision parallel to neurovascular bundle, in planned resection field, so entire tract can be excised en bloc. Transverse incisions contaminate multiple compartments and may necessitate amputation.
Q: A 60-year-old presents with a 7cm deep soft tissue mass. What is the most appropriate initial biopsy?
A: Core needle biopsy (image-guided). This is first-line for most lesions with 85-95% accuracy. Excisional biopsy would be a major error for a large deep mass (suspected sarcoma). Incisional biopsy is reserved for cases where needle is inadequate.
This section provides exam-focused practice points.
At a Glance
Biopsy technique in orthopaedic oncology is critical—Mankin's series showed 18.2% major errors in referral biopsies leading to altered treatment in 8.5% and unnecessary amputation in 4.5%. Cardinal principles: all biopsies should be performed by the definitive resection surgeon or in consultation with a tumor center; use longitudinal incisions only (transverse incisions contaminate multiple compartments); the biopsy tract must be in the planned resection field (will be excised en bloc); and minimize hematoma with meticulous hemostasis. Core needle biopsy (11-14 gauge) is first-line with 90% diagnostic accuracy. Never perform excisional biopsy for suspected sarcoma—this violates oncologic principles. Discuss all suspected bone/soft tissue tumors with a tumor center BEFORE biopsy.
MANKINMankin Biopsy Principles
Hook:MANKIN's principles prevent the catastrophic errors that led to his landmark 1982 study on biopsy complications
RESECTBiopsy Approach Planning
Hook:RESECT reminds you that the biopsy tract will be RESECTed with the tumor - plan accordingly!
FRESHSpecimen Handling
Hook:Send FRESH tissue - proper specimen handling is essential for accurate diagnosis
BIOPSYIndications for Biopsy
Hook:When do you need a BIOPSY? These indications guide decision-making
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“What are the indications for open incisional biopsy over core needle biopsy?”
“You are performing an open biopsy of a proximal tibia lesion suspected to be osteosarcoma. Walk me through your surgical approach.”
“What is the reported diagnostic accuracy of core needle biopsy for musculoskeletal tumors, and what factors influence this?”
Mankin's Biopsy Errors (MUST KNOW)
- **18.2% major errors** in referral biopsies
- **8.5% altered treatment**, 4.5% unnecessary amputation
- Error types: wrong biopsy type, wrong approach, poor haemostasis, inadequate tissue
- Conclusion: **biopsy by definitive surgeon** or tumor center
Cardinal Biopsy Principles
- **Longitudinal incision ONLY** - transverse is never acceptable
- **Single compartment** approach - do not violate multiple planes
- **Resection field trajectory** - entire tract excised en bloc
- **Meticulous hemostasis** - hematoma spreads tumor cells
- **No drains** (or drain exits through incision)
- **Tumor center consultation** before biopsy
Biopsy Type Selection
- **Core needle**: First-line, 85-95% accuracy, 4-6 cores minimum
- **Incisional open**: If needle inadequate, longitudinal approach
- **Excisional**: ONLY small superficial under 3cm low suspicion
- **FNA**: Limited role, confirmatory only (60-80% accuracy)
- **NEVER** excise suspected sarcoma - major error
Image Guidance
- **CT-guided**: Bone lesions, deep masses, 3D planning
- **Ultrasound-guided**: Superficial soft tissue, real-time, Doppler
- **Fluoroscopy**: Limited role, spine transpedicular approach
- Communicate with radiologist about resection field
Specimen Handling
- **Fresh tissue** in sterile container for culture (not formalin)
- **Minimum 1cm cube** or 3-5 cores for diagnosis
- **Frozen section**: Confirm adequacy only (cannot diagnose sarcoma)
- **Permanent H&E**: Standard diagnosis
- **Immunohistochemistry**: Subtype sarcoma
- **Molecular studies**: FISH, PCR if indicated
Indications for Biopsy
- Deep soft tissue mass (below fascia)
- Superficial mass over 5cm or growing
- Bone lesion with aggressive features
- Age-inappropriate lesion
- Pathological fracture through lesion
- Atypical imaging not fitting benign diagnosis
Specific Approaches
- **Distal femur**: Anteromedial longitudinal (vastus medialis)
- **Posterior thigh**: Posterior longitudinal (hamstring interval)
- **Proximal tibia**: Anteromedial (pes anserinus)
- **Pelvis**: CT-guided safer than open (complex anatomy)
- **Spine**: Transpedicular CT-guided or posterior open
Common Exam Scenarios
- **Referral after inappropriate biopsy**: Assess contamination, plan salvage
- **Plan biopsy for suspected osteosarcoma**: Staging first, tumor center discussion, longitudinal approach
- **Deep soft tissue mass**: Image-guided core needle first-line
- **Transverse incision complication**: Multi-compartment contamination, amputation risk
Evidence Base and Literature
CT-Guided Core Biopsy
- Bone visualization: See cortex, plan trajectory
- Avoidance of critical structures: 3D planning
- Confirmation of placement: Real-time imaging
- Deep lesions accessible: Pelvis, spine, retroperitoneum
- Reproducible approach: Coordinates documented
- Patient positioning (prone, supine, lateral based on approach)
- Scout CT to plan trajectory
- Skin prep and local anesthesia
- Small nick incision with scalpel
- Coaxial needle placement under CT guidance
- Confirm position on CT
- Multiple cores through coaxial needle (4-6 cores)
- Post-biopsy CT to assess for complications
- Compression dressing
A coaxial needle system uses an outer guiding cannula through which the biopsy needle passes. This allows multiple cores through a single tract, reducing contamination and improving patient comfort. The guiding cannula is positioned under CT, then multiple cores are obtained without removing the guide. This is the standard technique for percutaneous bone biopsy.
Ultrasound-Guided Core Biopsy
- Real-time visualization: See needle advancing in real-time
- No radiation: Safe for multiple passes
- Vascular avoidance: Doppler identifies vessels
- Soft tissue detail: Excellent for superficial masses
- Portable: Can be done in clinic or OR
- Identify lesion and vasculature on Doppler ultrasound
- Plan trajectory avoiding vessels
- Mark entry site
- Sterile prep and local anesthesia
- Visualize needle entry and advancement in real-time
- Multiple cores (3-5 minimum)
- Confirm hemostasis on ultrasound
- Compression dressing
- Superficial soft tissue masses
- Vascular lesions (can avoid vessels)
- Pediatric patients (no radiation)
- Lesions near neurovascular bundles (real-time avoidance)
Fluoroscopy-Guided Biopsy
Limited role in musculoskeletal oncology:
- Primarily for spine lesions (transpedicular approach)
- Real-time guidance for needle placement
- Lower radiation than CT
- 2D imaging only (less accurate than CT 3D)
Collaboration with Tumor Centers
All suspected sarcomas should be discussed with a tumor center before biopsy. Referral is indicated for suspected bone sarcoma, soft tissue mass greater than 5cm or deep to fascia, imaging features of malignancy, failed primary treatment, complex anatomy (spine, pelvis), and metastatic disease staging.
The optimal referral is BEFORE biopsy. Many tumor centers prefer to perform the biopsy themselves. Referral after an inappropriate biopsy results in delayed treatment, increased morbidity, and potentially worse outcomes.
Tumor centers provide access to multidisciplinary tumor boards including orthopaedic oncologist, musculoskeletal radiologist and pathologist, medical oncologist, radiation oncologist, and plastic surgeon. Benefits include expert consensus, coordinated treatment planning, protocol-based therapy, access to clinical trials, and improved outcomes.
References
-
Mankin HJ, Lange TA, Spanier SS. The hazards of biopsy in patients with malignant primary bone and soft-tissue tumors. J Bone Joint Surg Am. 1982;64(8):1121-1127.
-
Hau A, Kim I, Kattapuram S, et al. Accuracy of CT-guided biopsies in 359 patients with musculoskeletal lesions. Skeletal Radiol. 2002;31(6):349-353.
-
Welker JA, Henshaw RM, Jelinek J, et al. The percutaneous needle biopsy is safe and recommended in the diagnosis of musculoskeletal masses. Cancer. 2000;89(12):2677-2686.
-
Noria S, Davis A, Kandel R, et al. Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am. 1996;78(5):650-655.
-
Skrzynski MC, Biermann JS, Montag A, Simon MA. Diagnostic accuracy and charge-savings of outpatient core needle biopsy compared with open biopsy of musculoskeletal tumors. J Bone Joint Surg Am. 1996;78(5):644-649.
-
Dupuy DE, Rosenberg AE, Punyaratabandhu T, et al. Accuracy of CT-guided needle biopsy of musculoskeletal neoplasms. AJR Am J Roentgenol. 1998;171(3):759-762.
-
Fraser-Hill MA, Renfrew DL, Hilsenrath PE. Percutaneous needle biopsy of musculoskeletal lesions. 2. Cost-effectiveness. AJR Am J Roentgenol. 1992;158(4):813-818.
-
Heslin MJ, Lewis JJ, Woodruff JM, Brennan MF. Core needle biopsy for diagnosis of extremity soft tissue sarcoma. Ann Surg Oncol. 1997;4(5):425-431.
-
Pohlig F, Kirchhoff C, Lenze U, et al. Percutaneous core needle biopsy versus open biopsy in diagnostics of bone and soft tissue sarcoma: a retrospective study. Eur J Med Res. 2012;17:29.
-
Ray-Coquard I, Montesco MC, Coindre JM, et al. Sarcoma: concordance between initial diagnosis and centralized expert review in a population-based study within three European regions. Ann Oncol. 2012;23(9):2442-2449.
-
Mitsuyoshi G, Naito N, Kawai A, et al. Accurate diagnosis of musculoskeletal lesions by core needle biopsy. J Surg Oncol. 2006;94(1):21-27.
-
Strauss DC, Qureshi YA, Hayes AJ, et al. The role of core needle biopsy in the diagnosis of suspected soft tissue tumours. J Surg Oncol. 2010;102(5):523-529.
-
Domanski HA, Akerman M, Carlén B, et al. Core-needle biopsy performed by the cytopathologist: a technique to complement fine-needle aspiration of soft tissue and bone lesions. Cancer. 2005;105(4):229-239.
-
Adams SC, Potter BK, Pitcher DJ, Temple HT. Office-based core needle biopsy of bone and soft tissue malignancies: an accurate alternative to open biopsy with infrequent complications. Clin Orthop Relat Res. 2010;468(10):2774-2780.
-
Åkerman M, Domanski HA. The cytology of soft tissue tumours. Monogr Clin Cytol. 2003;16:1-116.
-
Mankin HJ, Mankin CJ, Simon MA. The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am. 1996;78(5):656-663. PMID: 8642021.
-
Gronchi A, Miah AB, Dei Tos AP, et al. Soft tissue and visceral sarcomas: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2021;32(11):1348-1365. PMID: 34303806.
-
Strauss SJ, Frezza AM, Abecassis N, et al. Bone sarcomas: ESMO-EURACAN-GENTURIS-ERN PaedCan Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2021;32(12):1520-1536. PMID: 34500044.
Key Regional References
-
Australia and New Zealand Sarcoma Association (ANZSA). Guidelines for the management of soft tissue sarcoma. Available at: www.anzsa.org.au
-
Cancer Australia. Optimal care pathway for people with sarcoma. Canberra: Cancer Australia, 2016.
-
Victorian Comprehensive Cancer Centre. Sarcoma service referral guidelines. Melbourne: Peter MacCallum Cancer Centre, 2020.
Suggested Reading
- Enneking WF. Musculoskeletal Tumor Surgery, Volume 1. Churchill Livingstone; 1983. [Classic text on biopsy principles]
- Simon MA, Springfield D. Surgery for Bone and Soft-Tissue Tumors. Lippincott-Raven; 1998. [Comprehensive operative techniques]
- Grimer RJ, Carter SR, Pynsent PB. The cost-effectiveness of limb salvage for bone tumours. J Bone Joint Surg Br. 1997;79(4):558-561.