Primary-Quaternary Mechanisms | Zone of Injury | Damage Control | Reconstruction vs Amputation
- Secondary blast injury is the leading cause of extremity trauma (fragment penetration)
- Zone of injury extends well beyond visible wound margins — serial debridement is mandatory
- Damage control orthopaedics: external fixation first, definitive fixation once physiologically stable
- MESS score greater than 7 suggests likely amputation, but clinical judgement remains paramount
- Never close a blast wound primarily — delayed primary closure at 3-5 days
- “Blast = four mechanisms (primary-quaternary), secondary dominates extremity pathology
- “Zone A = permanent cavity, Zone B = temporary cavitation, Zone C = molecular wound
- “Serial debridement every 48-72 hours until clean and viable tissue only
- “MESS less than 7 does not guarantee salvage; MESS greater than 7 does not mandate amputation
Four mechanisms act simultaneously. Primary (overpressure) mainly affects gas-containing organs (lungs, bowel). Secondary (fragments) is the dominant mechanism for extremity wounds. Tertiary (body displacement) causes blunt and crush injuries. Quaternary covers burns, crush syndrome, and inhalation injury.
Three concentric zones surround every fragment wound. Zone A (permanent cavity), Zone B (temporary cavitation — muscle crushed then recoils, devascularised), Zone C (molecular injury — cells look viable but undergo necrosis over 24-72 hours). This is why serial debridement is mandatory.
Physiological derangement dictates timing. Damage control orthopaedics (DCO): external fixation, haemorrhage control, wound debridement. Convert to definitive fixation only when inflammatory response settles (typically 5-14 days). Early intramedullary nailing in polytrauma risks fat embolism and ARDS ("second hit").
MESS, LSI, and PSI scores guide but do not replace clinical judgement. MESS greater than 7 strongly suggests amputation. However, no scoring system has sufficient sensitivity to dictate salvage. Key factors: warm ischaemia time, nerve status, soft tissue envelope, patient physiology, and resource setting.
- Diagnosis
- Secondary blast injury, assess each wound for depth and neurovascular status
- Treatment
- Serial debridement, external fixation of fractures, delayed closure
- Key Pearl
- Zone of injury extends well beyond visible wound
- Diagnosis
- Tertiary blast + crush, assess MESS score and physiological reserve
- Treatment
- Damage control: ex-fix, haemorrhage control, ICU resuscitation
- Key Pearl
- Limb vs life — never sacrifice the patient for the limb
- Diagnosis
- High-energy blast amputation with extensive zone of injury
- Treatment
- Serial debridement of stump, revise amputation at definitive stage
- Key Pearl
- Preserve length and viable soft tissue whenever possible
PSTQBlast Injury Mechanisms
Hook:PSTQ = Primary overpressure, Secondary shrapnel, Tertiary thrown, Quaternary everything else!
ABCZone of Injury in Blast Wounds
Hook:ABC of blast wounds — Actual destruction, Bruised zone, Contusion (molecular injury) — explains why serial debridement is mandatory!
MESSMESS Score for Limb Salvage Decision
Hook:MESS greater than 7 = likely amputation, but clinical judgement is king — no score replaces senior decision-making!
Overview and Epidemiology
Blast injuries represent the most complex form of extremity trauma encountered in both military and civilian settings. The combination of multiple injury mechanisms (primary through quaternary), extensive zone of injury far exceeding visible wound margins, heavy bacterial contamination, and the physiological insult of polytrauma makes management uniquely challenging. Decisions around limb salvage versus amputation, the timing of definitive fracture management, and the approach to wound coverage require systematic application of evidence-based principles. These principles are examined across FRACS, FRCS, and ABOS formats.
- Extremity involvement: 70-80 percent of all blast injuries affect the limbs
- Military: Improvised explosive devices (IEDs) are the dominant mechanism in modern conflict
- Civilian: Industrial explosions, terrorist attacks, and mining disasters
- Mortality: Determined by primary blast (pulmonary, visceral) and associated head/chest injury
- Morbidity: Extremity blast wounds are the leading cause of long-term disability in survivors
- Polytrauma: Blast injury rarely isolates to one limb — always assess for torso, head, and contralateral injury
- Contamination: Foreign material driven deep into tissues — soil, clothing, bone fragments
- Soft tissue loss: Massive, often underestimated on initial assessment
- Psychological: Post-traumatic stress disorder (PTSD) and chronic pain are nearly universal
- Rehabilitation: Protracted course — months to years of reconstructive surgery and therapy
Pathophysiology
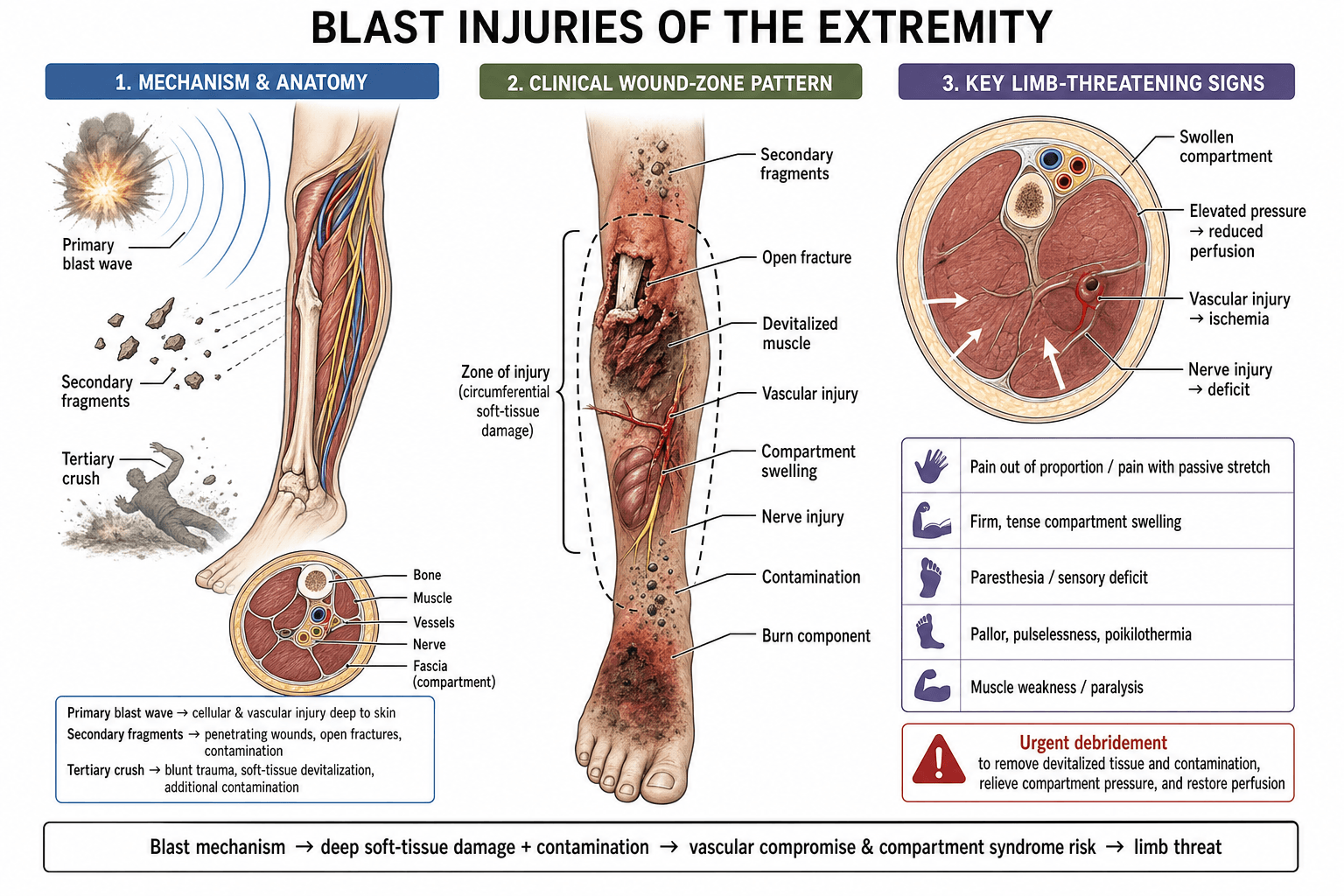
An explosion generates a supersonic overpressure wave (primary blast) followed by a blast wind. The overpressure wave causes barotrauma at air-tissue interfaces (lung, bowel, tympanic membrane). In the extremity, secondary blast (fragment penetration) dominates. Fragments are accelerated to high velocity and produce tissue destruction through three mechanisms: (1) direct laceration along the projectile path, (2) temporary cavitation as kinetic energy transfers to surrounding tissue, and (3) microscopic vascular injury at the cellular level that declares itself over 24-72 hours. This progressive necrosis is why no blast wound should be closed primarily and serial debridement every 48-72 hours is mandatory until all zones have declared themselves.
- Physics
- Spalling, implosion, inertia differential at gas-tissue interfaces
- Extremity Manifestation
- Limb compartment syndrome from blast wave; rare isolated extremity primary blast
- Priority
- Assess lungs and GI first — life-threatening
- Physics
- Projectiles (metal, glass, bone, debris) accelerated by blast wind
- Extremity Manifestation
- Multiple penetrating wounds, fractures, vascular and nerve injury, contamination
- Priority
- Dominant mechanism for extremity — multiple wounds expected
- Physics
- Whole-body acceleration/deceleration, structural collapse
- Extremity Manifestation
- Blunt fractures, crush injury, traumatic amputation, degloving
- Priority
- High-energy blunt trauma — ATLS approach
- Physics
- Burns, toxic inhalation, crush syndrome, radiation
- Extremity Manifestation
- Burns overlying fractures, rhabdomyolysis, compartment syndrome from crush
- Priority
- Multidisciplinary management essential
Zone A (Permanent cavity): Tissue directly crushed and destroyed by projectile passage. Irreversibly necrotic.
Zone B (Temporary cavitation): Tissue stretched by radial energy transfer, then recoils. Muscle appears viable but is devascularised. Declares over 24-72 hours.
Zone C (Molecular wound): Cells at the periphery appear viable on initial inspection but undergo apoptosis and necrosis due to microvascular thrombosis and cellular membrane disruption.
Clinical implication: What looks viable at first debridement may not be viable at 48-72 hours.
First look: Remove obvious necrosis, foreign material, and contaminants
48-72 hours: Zone C declares itself — more tissue may need excision
Repeat every 48-72 hours: Until the wound is clean with only clearly viable tissue
Closure: Only when wound is clean, granulating, and no further necrosis — typically 3-5 days minimum (delayed primary closure) or 5-7 days (secondary closure)
Never: Close a blast wound at index operation
Classification and Types
Classification by Blast Mechanism
- Typical Extremity Injury
- Compartment syndrome, vacuum phenomenon
- Contamination Level
- Low (no external wound)
- Key Management Difference
- Decompress compartments, monitor for pulmonary blast lung
- Typical Extremity Injury
- Multiple small penetrating wounds, often without fracture
- Contamination Level
- High (environmental debris embedded)
- Key Management Difference
- Explore tract, serial debridement, foreign body retrieval
- Typical Extremity Injury
- Devastating soft tissue destruction, comminuted fractures, vascular injury
- Contamination Level
- Very high (deep contamination)
- Key Management Difference
- Damage control, external fixation, vascular shunt or repair
- Typical Extremity Injury
- Closed or open fractures, traumatic amputation, degloving
- Contamination Level
- Moderate to high
- Key Management Difference
- ATLS resuscitation, mangled extremity assessment
- Typical Extremity Injury
- Burns overlying fracture, rhabdomyolysis, compartment syndrome
- Contamination Level
- Variable
- Key Management Difference
- Burn excision, fasciotomy, renal protection for crush syndrome
In real-world blast events, multiple mechanisms operate simultaneously — always assume a mixed pattern.
Clinical Assessment
- Airway with C-spine: Blast can cause airway burns, foreign body aspiration
- Breathing: Primary blast lung — look for haemoptysis, hypoxia, bilateral infiltrates
- Circulation: Haemorrhage control — tourniquet if active extremity bleeding, then direct pressure and tranexamic acid
- Disability: Head injury and spinal clearance — tertiary blast can cause traumatic brain injury
- Exposure: Full exposure for all wounds — blast produces multiple entry and exit sites
- Vascular: Palpable pulses distal to injury? Doppler if not palpable. ABI less than 0.9 suggests vascular injury
- Neurological: Document motor and sensory function of every major nerve — deficit changes management
- Compartment: Tense compartment, pain out of proportion, passive stretch pain — measure compartment pressures
- Wound: Document location, size, depth, contamination, visible bone/tendon/nerve. Do NOT explore in emergency department
- Fractures: Stabilise with splint or temporary external fixation. Document Gustilo-Anderson type
Probing, exploring, or attempting to close blast wounds in the emergency department risks further contamination, worsening haemorrhage, and missing deep-seated foreign material. Wound management belongs in the operating theatre under tourniquet control with adequate lighting and instrumentation. Emergency department management is limited to haemorrhage control (tourniquet, pressure dressing), splinting, antibiotics, tetanus prophylaxis, and urgent transfer to theatre.
- Purpose
- Fracture pattern, foreign bodies, vascular gas pattern
- Key Findings
- Comminution, radiopaque fragments, soft tissue gas
- Action Threshold
- Any fracture in blast = open until proven otherwise
- Purpose
- Vascular injury assessment in proximity wounds
- Key Findings
- Pseudoaneurysm, intimal flap, occlusion, active extravasation
- Action Threshold
- Hard signs = straight to theatre; soft signs = CTA
- Purpose
- Tissue perfusion and shock severity
- Key Findings
- Metabolic acidosis, elevated lactate
- Action Threshold
- Lactate greater than 4 mmol/L suggests under-resuscitation
- Purpose
- Rhabdomyolysis / crush syndrome screening
- Key Findings
- CK rising, dark urine, myoglobinuria
- Action Threshold
- CK greater than 5000 U/L = high risk of renal failure; aggressive IV fluids
- Purpose
- Confirm suspected compartment syndrome
- Key Findings
- Delta pressure less than 30 mmHg (diastolic minus compartment pressure)
- Action Threshold
- Delta pressure less than 30 = emergency fasciotomy
In the acute blast setting, a pre-hospital tourniquet is life-saving for haemorrhage control. In the emergency department, do not remove a functioning tourniquet until the patient is in the operating theatre with vascular surgical capability available. Premature removal can cause exsanguination from a previously contained vascular injury. Document tourniquet time — ischaemia beyond 6 hours (especially in a warm limb) substantially reduces limb salvage potential.
A limb tourniquet works only on a limb - but the highest-mortality blast bleeding is junctional, where the limb meets the torso and a tourniquet cannot be applied.
Junctional haemorrhage (groin/proximal thigh, buttock, perineum, axilla):
- A standard limb tourniquet will not control it. Use a junctional tourniquet device, aggressive wound packing with a haemostatic (e.g. kaolin-impregnated) dressing and direct pressure, and a pelvic binder for pelvic-source bleeding.
- For ongoing non-compressible pelvic/junctional haemorrhage, consider REBOA (resuscitative endovascular balloon occlusion of the aorta, Zone III) as a temporising bridge to surgical packing or angioembolisation.
The dismounted complex blast injury (DCBI) - the characteristic modern IED pattern in the soldier on foot:
- Bilateral lower-limb traumatic amputations PLUS pelvic ring disruption and perineal/genitourinary/rectal injury (the "blast pelvis") - a triad with very high mortality from exsanguination and heavy pelvic/perineal contamination.
- Management is combined-team: aggressive haemorrhage control (binder, packing, junctional tourniquet, REBOA), massive transfusion, serial debridement of the perineal wound, faecal diversion (defunctioning colostomy) for rectal/perineal contamination, and urology input for genitourinary injury - on top of the bilateral amputation/stump management.
Exam point: junctional haemorrhage (groin/perineum/axilla) is not controllable by a limb tourniquet - use a junctional tourniquet, haemostatic wound packing, pelvic binder, and REBOA (Zone III); recognise the dismounted complex blast injury triad (bilateral lower-limb amputation + pelvic ring + perineal/GU/rectal injury), which needs combined haemorrhage control, faecal diversion for perineal contamination, and multidisciplinary care.
Investigations
Imaging and Investigation Protocol
Views: AP and lateral of the injured extremity, including joint above and joint below
Look for: Fracture pattern (comminution suggests high energy), radiopaque foreign bodies, soft tissue gas (raises concern for gas gangrene), vascular gas pattern, bone loss
Clinical correlation: Any fracture in the setting of a blast wound is considered open until proven otherwise. Radiographs underestimate soft tissue injury severity.
Indication: Blast wound in proximity to major vessels, absent or diminished distal pulses, ABI less than 0.9
Findings: Pseudoaneurysm, intimal flap, complete occlusion, active extravasation
Decision: Hard signs of vascular injury (pulsatile bleeding, expanding haematoma, absent pulse, distal ischaemia) = proceed directly to operative exploration without CTA. Soft signs = CTA to localise injury.
Bloods: FBC, coagulation profile, cross-match (minimum 4 units), group and save
Metabolic panel: Urea, creatinine, electrolytes, lactate (greater than 4 mmol/L suggests under-resuscitation)
Muscle markers: Serum CK (greater than 5000 U/L suggests significant rhabdomyolysis and risk of acute kidney injury)
ABG: Assess for acidosis (blast lung), CO poisoning (inhalation), and base deficit
Technique: Stryker needle or slit catheter, measure delta pressure (diastolic BP minus compartment pressure)
Threshold: Delta pressure less than 30 mmHg = compartment syndrome = emergency fasciotomy
Clinical trigger: Tense compartment, pain out of proportion, pain on passive stretch. In blast injuries, a high index of suspicion is warranted — consider prophylactic fasciotomy for high-energy injuries.
In blast injuries, do not delay operative management for imaging if the patient has hard signs of vascular injury or haemodynamic instability. Plain radiographs in the emergency department are sufficient to plan initial damage control surgery. CT angiography is reserved for haemodynamically stable patients with soft signs of vascular injury. The investigation that matters most is the serial examination — reassess the limb every 2-4 hours for vascular status, compartment tightness, and neurological change.
Management Algorithm
Damage Control Orthopaedics (DCO)
Goal: Control haemorrhage, stabilise fractures temporarily, control infection source, and get the patient to ICU alive. Definitive management is deferred until physiological stability is achieved.
Damage Control Sequence
ATLS protocol: Airway, breathing, circulation
Haemorrhage control: Tourniquet to wound, tranexamic acid (within 3 hours of injury), blood products per massive transfusion protocol
Antibiotics: First-generation cephalosporin (or clindamycin if penicillin-allergic) plus aminoglycoside for gross contamination. Start immediately — do not wait for theatre
Tetanus: Tetanus prophylaxis as per guidelines
Wound debridement: Excise Zone A and clearly necrotic Zone B tissue. Irrigate copiously (minimum 6-9 litres pulsed lavage). Remove all accessible foreign material
Fracture stabilisation: External fixation spanning the zone of injury. Do NOT use internal fixation through a blast wound at index operation — infection risk is unacceptably high
Vascular management: Shunt if ischaemic limb with vascular injury (temporary intravascular shunt). Definitive repair can be done at a later stage when the patient is stable
Fasciotomy: Prophylactic four-compartment fasciotomy for any high-energy blast wound of the leg. Do not close fasciotomy primarily
Correct coagulopathy, acidosis, hypothermia (the lethal triad)
Monitor: Lactate clearance, urine output, compartment pressures if fasciotomy not performed
Plan: Return to theatre at 48-72 hours for second-look debridement
Re-assess all tissue viability: Zone C has now declared — more necrosis may be evident
Repeat debridement: Until wound is clean, granulating, and no further necrosis
Culture: Send tissue for microbiology at each debridement
Decision point: Once wound clean, plan definitive skeletal fixation and soft tissue coverage
Early Total Care (ETC) = definitive internal fixation within 24 hours. Appropriate for isolated fractures in stable patients. Damage Control Orthopaedics (DCO) = external fixation now, convert to definitive fixation later. Required for polytrauma, blast injury, or any patient with physiological derangement (ISS greater than 15, lactate greater than 2.5, coagulopathy). The "second hit" theory: major surgery on an inflamed patient triggers a systemic inflammatory cascade that worsens outcomes (ARDS, MOF). DCO minimises the surgical inflammatory hit.
Complications
- Incidence
- 20-40 percent in severe blast wounds
- Risk Factors
- Contamination burden, delay to debridement, open fractures, foreign bodies
- Management
- Serial debridement, targeted IV antibiotics, antibiotic beads, NPWT
- Incidence
- Rare but life-threatening when it occurs
- Risk Factors
- Devitalised muscle left in wound, delay to debridement, soil contamination
- Management
- Emergent radical debridement or amputation, IV penicillin + clindamycin, hyperbaric oxygen (adjunct)
- Incidence
- Up to 20 percent in high-energy blast limb injuries
- Risk Factors
- Crush component, reperfusion after vascular repair, tight dressings
- Management
- Emergency fasciotomy — prophylactic in high-energy injuries
- Incidence
- 10-30 percent in blast-related open fractures
- Risk Factors
- Gustilo IIIB/C fractures, infection, segmental bone loss, poor soft tissue envelope
- Management
- Bone grafting, Masquelet technique, Ilizarov bone transport
- Incidence
- Up to 60 percent in blast-related amputations (military data)
- Risk Factors
- High-energy injury, amputation through zone of injury, brain injury
- Management
- Prophylaxis with NSAIDs or radiation; excision if functional impairment
- Incidence
- Common after tertiary blast with prolonged entrapment
- Risk Factors
- Crush duration, muscle mass involved, delay to extrication
- Management
- Aggressive IV fluids (target urine output greater than 200 mL/hour), mannitol, bicarbonate, monitor CK and renal function
Clostridial myonecrosis (gas gangrene) is the most feared complication of blast wound contamination. Presentation: rapidly progressive severe pain out of proportion, bronze/grey discolouration of skin, crepitus, foul-smelling serosanguinous discharge, and systemic toxicity (tachycardia, fever, altered mental status). Treatment is emergent radical surgical debridement or amputation — do not wait for cultures. IV penicillin G and clindamycin are first-line antibiotics. Hyperbaric oxygen is an adjunct, not a substitute for surgery. Mortality approaches 100 percent without urgent surgical intervention.
The 4 Cs section warns that retained dead muscle drives invasive fungal infection, but this devastating, blast-specific entity deserves to be recognised in its own right - it is a major cause of late amputation and death after high-energy soil-contaminated blast wounds.
- Who and what: classically the soil-contaminated dismounted (on-foot) blast injury, infected by Mucorales (Rhizopus, Mucor, Lichtheimia) and also Aspergillus and Fusarium. The Mucorales are angioinvasive, thrombosing vessels and producing rapidly spreading necrosis.
- The cardinal clue: the wound shows recurrent, progressive tissue necrosis at the margins that keeps "advancing" despite adequate serial debridement and broad-spectrum antibiotics - a wound that will not turn the corner should raise immediate suspicion.
- Diagnosis: frozen-section histology and fungal culture of debrided tissue - broad, ribbon-like, non-septate hyphae indicate Mucorales.
- Management is dual: aggressive, frequent (often daily) wide surgical debridement back to bleeding tissue - frequently forcing more proximal amputation or stump revision - plus systemic antifungals, typically liposomal amphotericin B (for Mucorales) combined with a broad-spectrum azole (voriconazole or posaconazole) to cover Aspergillus/Fusarium.
- Outcome: high morbidity and mortality, and a major driver of higher final amputation levels.
Exam point: a blast wound with recurrent advancing necrosis despite proper serial debridement and antibiotics is invasive fungal infection (commonly angioinvasive Mucorales) until proven otherwise - confirm with tissue histology/culture (non-septate hyphae) and treat with repeated radical debridement (often more proximal amputation) plus liposomal amphotericin B and a broad-spectrum azole.
Outcomes and Prognosis
- Management
- Wound care, observation, antibiotics
- Expected Outcome
- Near 100 percent recovery of limb function
- Return to Function
- Days to weeks
- Management
- Serial debridement, external fixation, delayed closure
- Expected Outcome
- 80-90 percent limb salvage, functional outcome variable
- Return to Function
- Months — depends on fracture healing and soft tissue recovery
- Management
- Prolonged reconstruction: serial debridement, vascular repair, flap coverage, bone grafting
- Expected Outcome
- 50-70 percent achieve functional limb salvage; 30-50 percent eventual amputation
- Return to Function
- 12-24 months of reconstructive surgery and rehabilitation
- Management
- Stump revision, early prosthetic fitting, rehabilitation
- Expected Outcome
- Good function with modern prosthesis; phantom limb pain common
- Return to Function
- 6-12 months to independent mobility with prosthesis
Best prognosis: Low-energy fragments without fracture or vascular injury, early debridement, adequate soft tissue envelope, young and fit patient
Poor prognosis: High-energy blast with massive soft tissue loss, vascular injury with prolonged warm ischaemia, polytrauma with high ISS, delayed presentation, infection requiring multiple debridements
The LEAP study (Lower Extremity Assessment Project) showed that at 2 and 7 years, outcomes after limb salvage and amputation were broadly similar for quality of life — the critical message is that a good amputation may be preferable to a poor salvage.
Guidelines, Registries & Global Practice
- Military: Blast injury is the dominant mechanism in modern asymmetric warfare (IEDs account for the majority of casualties in Iraq and Afghanistan conflicts)
- Civilian: Industrial explosions, terrorist attacks, and mining disasters produce similar injury patterns
- Extremity dominance: 70-80 percent of surviving blast casualties have extremity wounds
- Resource disparity: Military medical systems in developed nations have advanced trauma chains; civilian blast management varies enormously by region
- High-resource: CT angiography, NPWT, free flap reconstruction, modular prostheses, multidisciplinary rehabilitation teams
- Limited-resource: Plain radiographs, saline dressings, skin grafting, basic external fixation, locally fabricated prostheses
- Universal principle: Serial debridement and delayed closure require no advanced technology — they are the standard everywhere
- Tourniquet use: Now universally accepted as first-line haemorrhage control in blast injury, regardless of resource setting
- Wound Management
- Irrigation and debridement, never close primarily, serial debridement every 48-72 hours
- Fracture Strategy
- Damage control: external fixation first; convert to definitive fixation at 5-14 days when physiologically stable
- Amputation Guidance
- No absolute indication — use MESS as adjunct, clinical judgement is paramount
- Wound Management
- BOAST 4: open fractures require urgent debridement (within 6 hours for high-grade), NPWT as standard
- Fracture Strategy
- DCO for polytrauma; ETC acceptable for isolated open fractures in stable patients
- Amputation Guidance
- Discuss at MDT before primary amputation; document decision-making clearly
- Wound Management
- Combat wound management principles: serial debridement, NPWT, delayed primary closure
- Fracture Strategy
- External fixation at forward surgical teams; convert at Role 3/4 facility
- Amputation Guidance
- MESS greater than 7 guides discussion; LEAP data supports functional equivalence of salvage and amputation
- Wound Management
- Minimum standard: wound excision, irrigation, delayed closure, no internal fixation through contaminated wounds
- Fracture Strategy
- External fixation or non-operative if no surgical capability; plaster and traction acceptable
- Amputation Guidance
- Functional amputation well performed is preferable to failed salvage with limited resources
Joint replacement registries (NJR, AJRR, AOANJRR) do not directly track blast outcomes. The primary evidence base comes from the Joint Theatre Trauma Registry (JTTR) for military data, the LEAP study for civilian severe limb trauma, and individual institutional series. The absence of a dedicated blast extremity registry means that most recommendations are Level 3-4 evidence, derived from expert consensus and observational data.
Record in every blast extremity injury:
- Mechanism classification (primary / secondary / tertiary / quaternary)
- Vascular status before and after intervention, with times (tourniquet time, ischaemia time)
- Neurological status of all major nerves documented before any surgical intervention
- MESS score with individual component scores
- Number and timing of each debridement
- Tissue viability findings at each debridement
- Decision-making for limb salvage versus amputation — including MDT discussion when possible
Missed or poorly documented blast wound assessment is a significant medico-legal risk worldwide. The key is serial assessment and clear documentation of evolving findings.
Controversies & Areas of Uncertainty
The optimal window for converting external fixation to definitive intramedullary nailing or plating is debated. Early conversion (5-7 days) risks operating in an inflamed wound bed; delayed conversion (greater than 14 days) increases pin-site infection and colonisation risk. Most guidance favours 7-14 days when inflammatory markers are settling, but there is no RCT-defined optimal timing.
Negative pressure wound therapy is now standard in high-resource settings for blast wounds between debridements, but robust RCT evidence demonstrating superiority over regular saline dressings in blast-specific injuries is limited. NPWT appears to reduce debridement frequency and promote granulation, but the absolute benefit remains uncertain.
Some military protocols recommend prophylactic four-compartment fasciotomy for all high-energy blast injuries of the leg, regardless of compartment pressure. Others advocate selective fasciotomy based on clinical assessment and pressure measurement. No RCT exists; practice is centre-dependent.
Through-knee amputation preserves superior gait biomechanics and energy efficiency compared to trans-femoral, but carries higher wound complication rates. In blast injuries where the zone of injury often extends proximal to the knee, the decision between through-knee revision and trans-femoral amputation must balance functional outcome against wound healing risk.
MCQ Practice Points
Q: Which blast injury mechanism is the most common cause of extremity trauma? A: Secondary blast injury (fragment penetration). Fragments (metal, glass, debris) accelerated by the blast wind are the dominant mechanism for extremity wounds. Primary blast (overpressure) primarily affects gas-containing organs (lungs, bowel, middle ear). Tertiary blast (body displacement) causes blunt injuries. Understanding the mechanism hierarchy is essential for anticipating associated injuries.
Q: What are the three zones of injury in a blast wound, and why does Zone C mandate serial debridement? A: Zone A = permanent cavity (tissue directly destroyed). Zone B = temporary cavitation (tissue crushed and devascularised but may appear viable initially). Zone C = molecular wound (cells appear viable but undergo necrosis over 24-72 hours due to microvascular thrombosis). Zone C mandates serial debridement because tissue that looks viable at the first operation may be necrotic by 48-72 hours. A single debridement misses this evolving necrosis, leading to infection and gas gangrene.
Q: What are the 4 Cs of muscle viability assessment during debridement? A: Colour (red and healthy, not pale or brown-grey), Consistency (firm, not mushy), Capacity to bleed (bright red bleeding when cut, not dark ooze), Contractility (contracts when pinched or stimulated with diathermy). Any muscle failing these criteria must be excised. Leaving devascularised muscle is the primary driver of gas gangrene and invasive fungal infection in blast wounds.
Q: What is the "second hit" theory, and how does it influence fracture management in blast polytrauma? A: The second hit theory proposes that major surgical intervention (such as intramedullary nailing) during the peak systemic inflammatory response to trauma worsens outcomes by triggering a secondary inflammatory cascade, increasing the risk of ARDS and multi-organ failure. This is the rationale for damage control orthopaedics (DCO): use external fixation for immediate skeletal stabilisation, and defer definitive internal fixation until the inflammatory response has settled (typically 5-14 days), as guided by lactate, CRP, and clinical parameters.
Q: A patient has a Gustilo IIIC open tibial fracture with absent pulses, sustained hypotension, and a high-energy blast mechanism. What is the approximate MESS score, and what does it imply? A: MESS approximately 11-12 (mechanism: high-energy = 3; ischaemia: absent pulses = 3; shock: sustained hypotension = 3; skeletal/soft tissue: Gustilo IIIC = 4). A MESS greater than 7 strongly predicts that limb salvage will have a poor outcome, but it does not mandate amputation — clinical judgement, patient factors, and resource setting all contribute to the final decision. No scoring system has sufficient sensitivity to be used in isolation.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old soldier sustains an IED blast injury to the right lower leg. He has multiple fragment wounds, a Gustilo IIIB open tibial fracture, absent dorsalis pedis pulse, and a tourniquet in situ applied 90 minutes ago in the field. He is haemodynamically stable after initial resuscitation. Discuss your management.”
“A 32-year-old civilian presents after an industrial boiler explosion. She has a mangled right lower extremity with a Gustilo IIIC open tibial fracture, complete tibial nerve disruption, 10 cm of segmental bone loss, and a warm ischaemia time of 7 hours. She is haemodynamically stable after resuscitation. Her MESS score is 9. How do you decide between limb salvage and amputation?”
Mechanisms (PSTQ)
- Primary = overpressure barotrauma (lungs, bowel, tympanic membrane — not primarily extremity)
- Secondary = fragment penetration — dominant mechanism for extremity wounds
- Tertiary = victim thrown by blast wind — blunt fractures, crush, traumatic amputation
- Quaternary = burns, crush syndrome, inhalation, psychological trauma
Zone of Injury
- Zone A = permanent cavity — tissue directly destroyed, irreversibly necrotic
- Zone B = temporary cavitation — devascularised muscle, may appear viable
- Zone C = molecular wound — cells necrose over 24-72 hours despite appearing viable
- Clinical implication: serial debridement every 48-72 hours is mandatory
Damage Control Orthopaedics
- External fixation at index operation — never internal fixation through a blast wound
- Temporary vascular shunt for ischaemic limbs — definitive repair when wound clean
- Prophylactic fasciotomy for high-energy leg blast injuries
- Convert to definitive fixation at 5-14 days when physiologically stable and wound clean
Wound Management Rules
- Never close a blast wound primarily — delayed primary closure at 3-5 days minimum
- Serial debridement every 48-72 hours using the 4 Cs of muscle viability
- NPWT between debridements to reduce oedema and promote granulation
- Soft tissue coverage (flap or graft) once wound definitively clean
Amputation Decision
- MESS greater than 7 suggests amputation but does not mandate it
- Warm ischaemia greater than 6 hours is the most important single poor prognostic factor
- Complete tibial nerve injury = insensate foot = poor functional outcome regardless of salvage
- LEAP study: quality of life at 2 years is similar for amputation versus limb salvage
- Preserve maximum stump length — through-knee is preferable to trans-femoral when feasible
Complications to Anticipate
- Infection: 20-40 percent deep infection in severe blast wounds — serial debridement prevents
- Gas gangrene: emergent radical debridement/amputation + IV penicillin and clindamycin
- Heterotopic ossification: up to 60 percent after blast amputation — consider NSAID prophylaxis
- Crush syndrome: aggressive IV fluids, monitor CK, target urine output greater than 200 mL/hour
Evidence Base and Key Trials
Factors influencing the decision to amputate or reconstruct after high-energy lower extremity trauma (LEAP Study)
- Prospective multicentre cohort of 601 patients with severe lower extremity trauma (including blast-type injuries)
- At 2 years, no significant difference in Sickness Impact Profile scores between limb salvage and amputation groups
- Patients who underwent amputation had faster return to function but more phantom limb pain
- Limb salvage patients had more reoperations (mean 5.3 vs 2.3) and longer hospitalisation
The timing of fracture treatment in polytrauma patients: relevance of damage control orthopedic surgery
- Review of damage control orthopaedics (DCO) versus early total care (ETC) in polytrauma
- Patients with ISS greater than 15 and elevated inflammatory markers had worse outcomes with early intramedullary nailing (second hit phenomenon)
- DCO with external fixation followed by conversion to definitive fixation at 5-14 days reduced ARDS incidence
- Lactate and IL-6 levels can guide timing of conversion to definitive fixation
Extremity war injuries: challenges in definitive reconstruction
- Review of extremity wound management principles from military conflicts (Iraq and Afghanistan)
- Serial debridement at 48-72 hour intervals was the standard of care for all combat blast wounds
- Negative pressure wound therapy reduced need for repeat debridement and improved granulation
- No blast wound should be closed primarily — delayed closure at minimum 3-5 days
Limb salvage versus amputation: preliminary results of the Mangled Extremity Severity Score
- Evaluation of MESS scoring reliability and predictive value in severe lower extremity trauma
- MESS greater than 7 had high specificity for predicting amputation but poor sensitivity
- Significant inter-observer variability in scoring individual components
- Authors concluded MESS should be an adjunct to clinical judgement, not a decision rule
Heterotopic ossification following traumatic and combat-related amputations: prevalence, risk factors, and preliminary results of excision
- 62 percent incidence of heterotopic ossification (HO) in combat-related amputations
- HO was more common when amputation was performed through the zone of injury
- Excision of symptomatic HO improved prosthetic fitting and comfort
- Prophylactic NSAIDs and local radiation reduced HO incidence but are not standard in acute blast care