Irreducible Ankle Fracture-Dislocation | Fibula Trapped Behind Tibia | Emergency Surgery
KEY FEATURES
Critical Must-Knows
- Definition: Rare fracture-dislocation where the distal fibula becomes entrapped behind the posterior tubercle of the distal tibia.
- Clinical Sign: Foot is severely externally rotated, often 'axilla sign' (pucker) over medial malleolus.
- X-ray Pitfall: Can look like a standard ankle fracture on AP; Lateral view is diagnostic (fibula behind tibia).
- Management: Usually irreducible by closed means. Requires urgent Open Reduction Internal Fixation (ORIF).
- Attempting forced closed reduction can cause additional iatrogenic fractures or soft tissue damage.
Clinical Pearls
- "Suspect Bosworth if closed reduction of an 'ankle fracture-dislocation' is impossible.
- "The 'Axilla Sign' is a medial skin pucker caused by severe deltoid ligament traction.
- "CT scan is critical if diagnosis is unclear or reduction fails.
- "Always assess the proximal fibula (Maisonneuve variant potential).
Critical Exam Points
Irreducibility
The defining feature is mechanical block to reduction. The fibula is locked behind the posterior tibial ridge (Volkmann's triangle). Repeated closed attempts cause harm.
Radiographic Clue
On the AP view, the tibia and fibula overlap excessively. On the Lateral view, the fibula is clearly visible posterior to the tibia (normally they overlap).
Compartment Syndrome
High energy + distorted anatomy + failed reduction attempts = high risk of compartment syndrome. Monitor pressures if delay to surgery.
Syndesmosis Injury
The interosseous membrane and syndesmotic ligaments are universally torn. Syndesmotic fixation is almost always required after reduction.
Quick Decision Guide - Ankle Dislocation
| Condition | Reduction | Management | Urgency |
|---|---|---|---|
| Standard Ankle Fracture-Dislocation | Usually reducible (Quigley maneuver) | Splint to Delayed ORIF (swelling dependent) | Urgent Reduction (ED) |
| Bosworth Fracture-Dislocation | **Impossible/Locking** sensation | **Urgent Open Reduction** (cannot wait) | **Emergency Surgery** |
TRAPBosworth Characteristics
| T | Tibial posterior tubercle blocks reduction |
| R | Rotation Severe external rotation mechanism |
| A | Axilla sign Medial skin pucker (pathognomonic) |
| P | Posterior Fibula trapped POSTERIOR to tibia |
| T | Tibial posterior tubercle blocks reduction | A | Axilla sign Medial skin pucker (pathognomonic) |
| R | Rotation Severe external rotation mechanism | P | Posterior Fibula trapped POSTERIOR to tibia |
Hook:The fibula is caught in a TRAP behind the tibia.
ROFSurgical Steps
| R | Reduce Open reduction (lever fibula back into notch) |
| O | ORIF Plate fibula fracture if present |
| F | Fix Fix Syndesmosis (screw/tightrope) |
| R | Reduce Open reduction (lever fibula back into notch) |
| O | ORIF Plate fibula fracture if present |
| F | Fix Fix Syndesmosis (screw/tightrope) |
Hook:ROF (Rough) reduction needed for Bosworth
SNAPComplications
| S | Stiffness Joint arthrosis common |
| N | Necrosis Skin edge necrosis |
| A | Arthritis Post-traumatic OA |
| P | Poor function If missed or delayed |
| S | Stiffness Joint arthrosis common | A | Arthritis Post-traumatic OA |
| N | Necrosis Skin edge necrosis | P | Poor function If missed or delayed |
Hook:The ankle SNAPs back badly if not fixed.
Overview and Epidemiology
Bosworth fracture-dislocation is a rare and severe ankle injury where a fragment of the distal fibula displaces posteriorly behind the posterior tubercle of the distal tibia and becomes entrapped. The fibula is "locked" in this position, making closed reduction impossible in almost all cases without specific maneuvers or open surgery.
Historical Background: First described by David Bosworth in 1947 (J Bone Joint Surg Am). He identified the fibula becoming trapped behind the "posterior tibial ridge" (posterior tubercle), and crucially attributed irreducibility to this bony block rather than to the soft-tissue interposition that had previously been blamed. Understanding the entity is critical because persistent forceful closed reduction attempts can cause iatrogenic fracture, massive swelling and compartment syndrome.
Epidemiology:
- Incidence: Rare; estimated at under 2% of ankle fractures, with roughly 175 cases described in the world literature.
- Demographics: Predominantly young to middle-aged adults from high-energy trauma (sport, falls, motor-vehicle crashes); the morphology is age-dependent (see Classification).
- Pathognomonic Mechanism: Severe external rotation of the supinated foot, with the tibia driven anteriorly relative to the fibula.
- Association: Usually associated with a fibular fracture (most often Weber B), and a posterior malleolar fracture is present in roughly 70% of cases; "pure" dislocations without fibular fracture occur, classically in younger, more elastic patients.
Why is it Critical?
- Irreducible: It will NOT reduce with standard traction.
- Skin Risk: The skin over the medial malleolus is tented (Axilla sign) and the skin over the posterior fibula is compressed. Necrosis occurs rapidly.
- Compartment Syndrome: The distortion of the deep posterior compartment can lead to ischemia. Pathophysiology:
- Mechanism: Severe External Rotation of the supinated foot.
- Sequence: The fibula rotates externally, snaps out of the incisura fibularis, moves posteriorly, and gets locked behind the posterior ridge of the tibia.
- Ligaments: The anterior inferior tibiofibular ligament (AITFL) is intact or avulsed (Tillaux-Chaput), acting as a hinge. The interosseous membrane is torn.
Anatomy
The Key Anatomic Checkpoint: The Incisura Fibularis. The distal tibia has a concave notch laterally (incisura) where the fibula sits. The posterior tubercle (Volkmann's triangle border) forms a buttress. In Bosworth injuries, the fibula jumps this buttress.
Detailed Osteology:
- Distal Tibia: The Lateral surface forms the incisura fibularis. It is bounded anteriorly by the anterior tubercle (Chaput) and posteriorly by the larger posterior tubercle (Volkmann).
- Distal Fibula: Fits into the incisura. It serves as the attachment for the syndesmotic ligaments (AITFL anteriorly, PITFL posteriorly, IOM medially).
- The Trap: The posterior tubercle acts as a "cam". Once the fibula rotates past it, the elastic recoil of the interosseous membrane snaps it medially against the posterior cortex of the tibia, locking it in place.
Pathomechanics of Entrapment: The entrapment occurs because the fibula is levered out of the incisura. The force vector is external rotation. The fibula acts as a lever arm.
- Stage 1 - Ligament Failure: AITFL rupture or avulsion (Tillaux-Chaput or Wagstaffe). This releases the anterior constraint.
- Stage 2 - Translation: Fibula rotates externally and translates posteriorly out of the groove.
- Stage 3 - Crossing the Equator: The equator of the fibula passes the posterior colliculus of the tibia.
- Stage 4 - The Lock: Elastic recoil of the soft tissues (or remaining interosseous membrane fibers superiorly) pulls the fibula tightly against the posterior cortex of the tibia.
- Stage 5 - Irreducibility: The fibula is now "locked". The posterior tubercle prevents it from sliding forward. Traction alone simply tightens the IOM against the bone. Reducing it requires overcoming this posterior ridge by "unhooking" it laterally.
Ligamentous Structures:
- Anterior Inferior Tibiofibular Ligament (AITFL): Always torn or avulsed. This is the first restraint to fail.
- Posterior Inferior Tibiofibular Ligament (PITFL): Often intact, attached to the posterior malleolus, pulling it off (Volkmann fracture) or torn. If intact, it contributes to the posterior tethering.
- Interosseous Membrane (IOM): Extensive tearing proximally, depending on the level of the fibular fracture (Maisonneuve variant). The level of the IOM tear often determines the level of the fibular fracture.
- Deltoid Ligament: Universally injured (either tear or medial malleolus fracture) allowing the talus to shift laterally and externally rotate.
- Lateral Ligament Complex (ATFL/CFL): Usually intact, as the fibula moves with the talus.
Neurovascular Anatomy at Risk:
- Posterior Structures: The neurovascular bundle (Posterior Tibial Artery/Nerve) runs just medial to the Achilles tendon but lateral to the medial malleolus. In a severe posterior dislocation, the bundle can be tented or stretched over the posterior aspect of the tibia.
- Anterior Structures: The Superficial Peroneal Nerve (SPN) runs anteriorly in the subcutaneous tissue. It is at risk during the lateral approach if not identified and retracted.
- Posterior Approach Risks: The Sural Nerve runs with the small saphenous vein posterior to the peroneal tendons. It must be identified and protected during the posterolateral approach.
Classification
There is no universally accepted classification, but they are described by the level of the fibular fracture:
- Proximal Fracture (Maisonneuve-type): Fibula trapped distally, fracture is proximal. Harder to diagnose.
- Shaft Fracture: Spiral fracture of the shaft; distal fragment trapped.
- No Fracture (Pure Dislocation): Rare. Only ligamentous disruption.
Note: The key feature is the DISLOCATION, not the fracture pattern. Relevance: The level of the fracture often dictates the integrity of the proximal IOM.
- High Fracture: Extensive IOM tear.
- Low Fracture: IOM may be intact proximally (but still torn at the incisura).
Clinical Assessment
History:
- High-energy twisting injury (sports, fall).
- Patient reports inability to stand, severe pain.
- "The ankle looks twisted around backward."
Physical Exam:
- Deformity: Foot is in severe external rotation relative to the leg.
- Axilla Sign: A skin dimple/pucker over the medial malleolus (resembling an axilla). This is due to the tibia buttonholing through the capsule or severe deltoid tethering.
- Neurovascular: Check dorsalis pedis/posterior tibial pulses. Tibial nerve stretch injury is possible and should be documented carefully.
- Swelling: Rapid and massive soft tissue swelling occurs due to the violent nature of the injury and significant tearing of the IOM. This further compromises the skin.
- Skin: Look for tenting posteriorly (fibula) or medially (tibia). Skin necrosis is a major risk.
- Tenderness: Diffuse tenderness, maximal over the syndesmosis and posterior fibula.
- Gait: Patient is unable to bear weight and unable to hop.
Pre-Hospital Care:
- Analgesia: Assessment of pain score. Methoxyflurane or IV opioids.
- Deformity Check: Document neurovascular status BEFORE and AFTER any movement.
- Splintage: Don't forcefully reduce on the field. Apply a pillow splint in the position of deformity (which is usually significant external rotation) to support the limb. Attempting to force the ankle into a standard backslab without disengaging the lock is dangerous and futile.
- Transport: Urgent transport to a center capable of surgical intervention. This is a time-critical ischemia injury for the skin.
- Documentation: Clearly document "Non-reducible deformity" to alert ED staff immediately upon arrival.
Emergency Department Assessment:
- Triad of Signs:
- Severe external rotation of foot (often 90 degrees).
- Impossible closed reduction.
- "Axilla Sign" (medial skin pucker).
- Reduction Attempt:
- Typical Quigley maneuver (lift toe, internally rotate) feels locked.
- Elastic resistance ("bouts back") when trying to internally rotate.
- STOP if this sensation is felt. Repeated attempts damage the articular surface of the posterior tibia.
Differential Diagnosis:
Differentiating Bosworth from Mimics
| Condition | Reducibility | Discriminating Feature | Key Imaging |
|---|---|---|---|
| Bosworth fracture-dislocation | Irreducible / 'locked' | Severe external rotation + axilla sign; fibula posterior to tibia | Lateral: posterior tibiofibular dissociation; CT confirms entrapment |
| Standard ankle fracture-dislocation (SER) | Usually reducible (Quigley) | Reduces with traction/internal rotation; no bony block | Mortise restored after reduction |
| Pilon fracture | Variable | High-energy axial load, articular comminution, not a pure dislocation | CT shows plafond impaction/comminution |
| Subtalar dislocation | Often reducible closed | Foot deformity but tibiotalar mortise intact | AP: intact ankle mortise; talus displaced at subtalar joint |
| Total talar (pan-talar) dislocation / extrusion | Surgical emergency | Talus extruded, usually open, dramatic deformity | Talus displaced out of all articulations |
Investigations
X-rays (Trauma Series):
- AP View:
- "Cortical Overlap Sign": The proximal cortex of the distal fibula fragment overlaps with the lateral cortex of the distal tibia. The overlap is significantly greater than the normal tibiofibular overlap (greater than 6mm).
- Joint Space: The medial clear space is often widened due to deltoid rupture.
- Deception: It may look like a "well-reduced" ankle fracture if not scrutinized, but the patient has severe pain and deformity.
- Lateral View:
- "The Diagnostic View": This is the single most important film.
- Posterior Displacement: The distal fibula is seen completely posterior to the tibia. (Normally, the fibula superimposes on the posterior third of the tibia).
- Empty Notch: The tibial incisura is empty.
- Double Shadow: If the fibula is fractured, the proximal shaft may be seen in normal position while the distal fragment is posterior.
CT Scan:
- Indication: Often obtained after failed reduction or if the diagnosis is suspected but X-rays are equivocal. Recommended for surgical planning in all cases if resources allow.
- Bone Window Findings:
- Shows the "fibular head locked behind tibial plume".
- Identifies associated marginal fractures (Volkmann, Chaput).
- Assesses the size of the posterior malleolus fragment (important for fixation).
- 3D Reconstruction:
- Extremely useful for understanding the rotational deformity and planning the "unhooking" maneuver.
- Soft Tissue Window:
- Can show entrapment of the FHL or Peroneus Brevis tendons, which may block reduction.


Management Algorithm
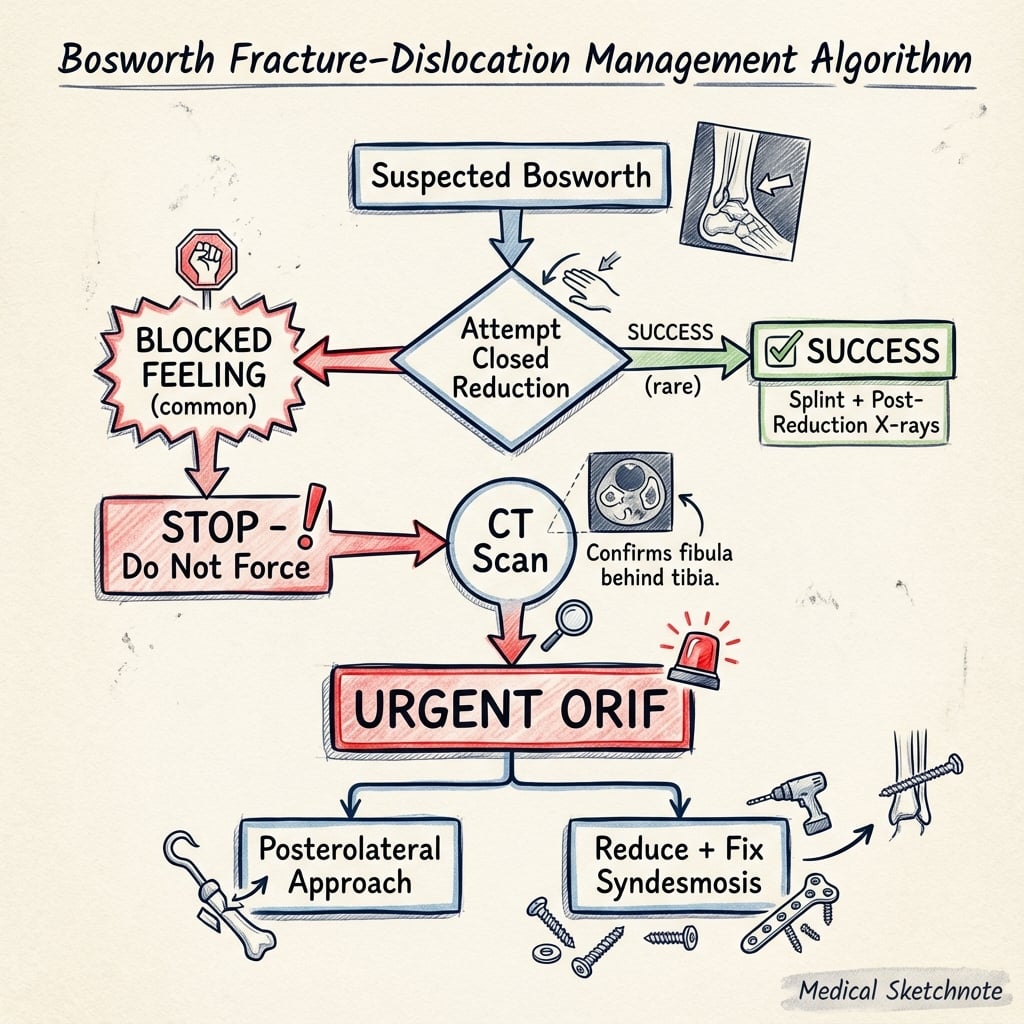
It is crucial to recognize this early.
1. Attempt Closed Reduction (ED/Sedation):
- Technique: Traction + External Rotation (to unlock) + Anterior translation of fibula + Internal Rotation.
- Outcome: Rarely works.
- Warning: Do not use excessive force.
2. Surgical Management (Standard of Care):
- Urgent Open Reduction.
- Sooner is better to prevent skin necrosis.
Surgical Technique
Step-by-Step Surgical Technique
1. Patient Setup and Positioning:
- Position: Lateral decubitus position is preferred for the posterolateral approach. A beanbag is used to stabilize the patient.
- Alternate: Supine position with a sandbag under the ipsilateral hip (bump) allows for easier access to the medial side if needed, but posterolateral access is slightly more difficult.
- Tourniquet: Applied to the thigh.
- Imaging: C-arm positioned from the opposite side.
2. Approach (Posterolateral):
- Incision: Longitudinal incision midway between the posterior border of the fibula and the lateral border of the Achilles tendon.
- Superficial Dissection: Identify and protect the Sural Nerve and short saphenous vein (typically in the posterior flap).
- Deep Dissection: Incise the deep fascia. Find the interval between the Peroneus Brevis (lateral) and Flexor Hallucis Longus (medial).
- Exposure: Retract peroneal tendons anteriorly/laterally and FHL posteriorly/medially. This exposes the posterior aspect of the distal tibia and fibula.
3. Reduction Maneuver:
- Assessment: Inspect the pathology. The distal fibula will be seen trapped behind the posterior colliculus of the tibia.
- Soft Tissue Clearance: Careful removal of interposed periosteum or torn labrum from the incisura.
- Reduction: A bone hook is placed around the fibula. Apply lateral and anterior traction to "pry" the fibula back into the incisura notch.
- Assist: An assistant should internally rotate the foot simultaneously.
- Confirmation: A palpable and audible "clunk" is often felt as it reduces. Verify reduction fluoroscopically (the fibula should be centered in the notch on lateral view).
4. Fixation Strategy:
- Fibula Fracture: Perform standard ORIF. Use a 1/3 tubular plate or anatomical locking plate. If the fracture is high (Maisonneuve), it may not need plating if the syndesmosis is stabilized.
- Syndesmosis: This is the critical step. The IOM is torn. Assess stability with the Cotton (hook) test.
- Syndesmosis Fixation: Place 1 or 2 syndesmotic screws (3.5mm or 4.5mm) or suture button devices (TightRope).
- Trajectory: Aim from fibula to tibia, parallel to the joint, about 2-3 cm proximal to the joint line. Angle 30 degrees anteriorly to match the transmalleolar axis.
5. Closure:
- Washout: Thorough irrigation.
- Layered Closure: Repair the deep fascia if possible (carefully, do not constrict). Subcutaneous and skin closure.
- Dressing: Bulky dressing and posterior slab (backslab) in neutral dorsiflexion.
Critical Note: Ensure the fibula is length-restored and fully seated in the incisura before fixation.
Complications
Major Complications
1. Skin Necrosis and Wound Issues
- Incidence: Disproportionately high for a malleolar injury, especially with delayed reduction and repeated closed attempts.
- Mechanism: The entrapped fibula tents the posterior skin, causing pressure necrosis. Alternatively, the "axilla sign" medially causes skin compromise due to extreme tension.
- Risk Factors: Time to reduction greater than 24 hours, older age, smoking, diabetes.
- Prevention: Urgent reduction (within hours). Handle soft tissues gently. Avoid "searching" for the nerve in compromised skin.
- Management: Debridement, negative pressure wound therapy (VAC), or flap coverage (sural flap/free flap) if defect is large.
2. Compartment Syndrome
- Risk: Far higher than in ordinary malleolar fractures (calculated prevalence around 5.4% across reported Bosworth cases; Bartoníček et al, 2021). Severe dislocation, repeated closed reduction attempts and a long interval to surgery are the key risk factors. The deep posterior compartment is most at risk.
- Mechanism: Bleeding + edema from the torn IOM and muscles.
- Signs: Pain out of proportion, pain with passive toe stretch (especially great toe), tense compartments, paresthesia.
- Action: High index of suspicion. Emergent 4-compartment fasciotomy if pressures are elevated (greater than 30 mmHg or delta pressure less than 30 mmHg).
- Sequelae: Claw toes, sensory loss, weakness.
3. Post-Traumatic Osteoarthritis
- Mechanism: Chondral damage occurs as the fibula "grinds" across the posterior tibia during dislocation and reduction. Some degree of cartilage scuffing is common.
- Prevalence: Higher than after standard ankle fractures; persistent pain, restricted motion and degenerative change are commonly reported, although large long-term series are lacking (Bartoníček, Rammelt, Tuček, 2024).
- Symptoms: Chronic pain, stiffness, weather-related ache, swelling.
- Treatment: Non-operative (bracing, injections) initially. Ankle arthrodesis or Total Ankle Arthroplasty (TAA) for end-stage disease.
4. Neurovascular Injury
- Posterior Tibial Nerve: Can be stretched around the tibia or injured during reduction. Leads to paresthesia in the sole of the foot.
- Sural Nerve: At risk during the posterolateral approach (crossing the incision). Numbness in lateral foot.
- Superficial Peroneal Nerve: At risk during lateral approach. Numbness in dorsum of foot.
- Management: Careful dissection and protection. Document deficits pre-op if possible.
5. Missed Diagnosis
- Problem: Often mistaken for a "bad sprain" or simple fracture if only AP X-ray is seen. The "Cortical Overlap" is subtle.
- Consequence: Delayed treatment leads to irreducible contractures, severe arthritis, and "Chronic Bosworth Injury" which is very difficult to treat (often requires fusion).
- Pearl: The "Lateral View" rule: You must see the fibula centered in the tibia. If it's behind, it's out.
Special Populations and Chronic Cases
The "Neglected" Bosworth:
- Definition: Cases presenting or diagnosed after 3-4 weeks.
- Problem: Significant soft tissue contracture (triceps surae), formation of distinct facet on posterior tibia (false articulation), and extensive osteopenia.
- Management:
- Open Reduction: Extensive release required. Often need to lengthen Achilles tendon.
- Osteotomy: Removal of the posterior tibial tubercle (buttress) to allow the fibula to slide forward.
- Arthrodesis: In cases greater than 6 weeks with cartilage destruction, primary fusion may be the better option to avoid painful stiffness.
Pediatric Bosworth:
- Rare: Even rarer than in adults.
- Variant: Often involves a Salter-Harris type separation of the distal fibular physis.
- Trap: The distal fibular epiphysis may be trapped behind the tibia while the metaphysis looks aligned (if separated).
- Treatment: Gentle reduction under anesthesia. If closed reduction fails (common due to periosteal entrapment), open reduction is required. Fixation with smooth K-wires is preferred to avoid growth arrest, crossing the physis only if necessary, and removing them early (3-4 weeks).
Geriatric Considerations:
- Bone Quality: Porotic bone makes the "locking" mechanism less secure, but associated fractures (posterior malleolus) are more comminuted. The posterior wall may be crushed, making the lock less distinct but the joint more unstable.
- Skin Risk: Extreme risk of sloughing. Minimally invasive techniques should be used if possible.
- Fixation: Augment with locking plates (distal fibula LCP) or fibular nail if soft tissue allows. Primary fusion nail (hindfoot nail) is a salvage option for non-reconstructable locking injuries with poor skin.
Postoperative Care
Immediate Post-Op (0-2 Weeks):
- Immobilization: Backslab or bulky dressing applied in the operating room. Foot is held in neutral dorsiflexion to prevent equinus contracture.
- Elevation: Strict elevation (toes above nose) for 48-72 hours to minimize swelling and reduce wound complications.
- DVT Prophylaxis: Chemical prophylaxis (LMWH, Xarelto) is standard due to NWB status and trauma risk.
- Weight Bearing: Strict Non-Weight Bearing (NWB).
- Wound Check: Review at 2 weeks. Suture removal if healed. Check for marginal necrosis especially at the corners of the incision.
Early Rehab (2-6 Weeks):
- Immobilization: Transition to a removable CAM boot (Moon boot) once wounds are healed.
- ROM Exercises: Gentle active dorsiflexion/plantarflexion out of boot 3-4 times daily. Avoid inversion/eversion to protect ligaments and syndesmosis.
- Muscle Activation: Isometric calf, quad, and gluteal exercises.
- Weight Bearing: Remain NWB generally. Some protocols allow touch-down weight bearing (TDWB) if fixation is rigid, but caution is advised due to syndesmotic injury.
Progressive Loading (6-12 Weeks):
- X-ray Check: Confirm callus formation and maintenance of reduction. Ensure no diastasis of syndesmosis.
- Weight Bearing: Progress to partial weight bearing (PWB) then full weight bearing (FWB) in boot over 2-3 weeks.
- Proprioception: Begin wobble board and balance training once FWB.
- Strength: Theraband resistance exercises for peroneal and tibialis posterior strengthening.
Long Term (3+ Months):
- Hardware Removal:
- Syndesmosis Screws: Traditionally removed at 12-16 weeks before full sport return to prevent breakage. Current trend is to leave them unless symptomatic or removing due to breakage risk in athletes.
- Suture Buttons: Do not need removal.
- Return to Sport: Impact activities (jogging) at 4-6 months. Cutting sports (football/rugby) at 6-9 months pending functional testing (single leg hop).
- Work: Return to sedentary work at 2-3 weeks; manual labor at 4-6 months.
Outcomes/Prognosis
General Prognosis: Bosworth fractures historically have poorer outcomes than standard ankle fractures due to the severity of soft tissue injury and chondral damage. However, early recognition and anatomical reduction can yield good results.
Factors Influencing Outcome:
- Time to Reduction: The most critical modifiable factor. Delay and repeated closed attempts correlate with skin necrosis, compartment syndrome and worse function.
- Cartilage Damage: The "grinding" of the fibula against the posterior tibia causes osteochondral defects (OCDs) which predispose to arthritis.
- Syndesmosis and Posterior Malleolus Reduction: Malreduction of the syndesmosis or a large posterior malleolar fragment leads to accelerated joint degeneration; postoperative CT is recommended to confirm reduction.
Long-Term Complications:
- Post-Traumatic Osteoarthritis: More frequent than after ordinary ankle fractures; precise long-term rates are uncertain because large series are lacking.
- Chronic Pain / Stiffness: Reduced range of motion, particularly dorsiflexion, is commonly reported even in surgically treated patients.
- Hardware Issues: Prominent plates laterally may require removal.
Evidence
Original Description of the Lesion
- First description of fixed posterior displacement of the fibula behind the tibia.
- Identified the bony 'locking' mechanism behind the posterior tibial tubercle as the cause of irreducibility, rather than soft-tissue interposition.
- Concluded that closed traction and rotation fail, and open reduction is required.
The Bosworth Lesion: Series and Literature Analysis
- Six operatively/conservatively treated cases plus analysis of 54 cases from the literature.
- The one patient treated by closed reduction and cast required ankle fusion at 2 years for severe osteoarthritis; all ORIF cases healed with good outcome.
- Proposed an age-related morphology: epiphyseolysis in children, pure dislocation (no fracture) in young adults, and fibular fracture in middle-aged/older adults due to reduced elasticity.
Current Concept Review
- CT with 3D reconstruction should be the diagnostic standard, particularly to define the frequently associated posterior malleolar fragment.
- Repeated closed reduction attempts must be avoided; non-operative treatment almost always fails and early ORIF is standard.
- The injury is disproportionately prone to soft-tissue complications including compartment syndrome; long-term outcomes are mixed with persistent pain, stiffness and degenerative change.
Reliability of Radiographic Signs
- 23 consecutive patients; mean age 44 years; diagnosis confirmed at surgery in 22 and/or on CT in 15.
- Posterior tibiofibular dissociation on the lateral view was the most reliable sign, present in 22 of 23 (96%) and persisting in all cases with unsuccessful closed reduction.
- Posterior talar subluxation (91%) and tibiofibular overlap crossing the joint line on AP (87%) were the other reliable signs and should prompt CT.
Compartment Syndrome Risk
- Case report plus literature review identifying 9 cases of compartment syndrome among 167 reported Bosworth fractures (calculated prevalence 5.4%).
- Risk factors were severe dislocation, repeated closed reduction attempts, and long interval to definitive surgery.
- Delayed diagnosis produced lasting deficits including hallux flexion contracture and lesser-toe clawing.
Successful Closed Reduction (Exception)
- 25-year-old man whose Bosworth fracture-dislocation was reduced closed and treated in a U-shaped plaster splint.
- Full weight-bearing, pain-free, with no ankle or subtalar range-of-motion limitation at 30 months.
- Authors emphasise that successful closed treatment is rare and emergent open surgery remains the recommended default.
Evidence-Based Discussion
Historical context. According to PubMed, David Bosworth's 1947 paper (J Bone Joint Surg Am 29(1):130-5, PMID 20284692) first attributed irreducibility to a bony block — the fibula locked behind the posterior tibial ridge — rather than to soft-tissue interposition. That insight still underpins the modern teaching that traction and rotation alone cannot disengage the fibula.
Diagnostic delay and the radiographs that matter. A recurring theme across the Bartoníček/Rammelt body of work is missed diagnosis. The 2025 radiographic-reliability study (PMID 40691735) showed that posterior tibiofibular dissociation on the lateral view (96%) is the most dependable sign and persists despite attempted closed reduction, followed by posterior talar subluxation (91%) and AP tibiofibular overlap crossing the joint line (87%). Any of these should trigger CT. CT with 3D reconstruction is now the diagnostic standard (2024 EFORT review, PMID 38828971), principally to characterise the associated posterior malleolar fragment.
Controversies and Areas of Uncertainty
Closed vs immediate open reduction
Consensus favours one gentle closed attempt followed by urgent open reduction if it fails. Isolated reports (Ji et al, 2022; Molinari et al, 1990) describe durable success with closed reduction and casting, but repeated attempts demonstrably increase the risk of compartment syndrome and skin necrosis, so persistent manipulation is not justified.
Routine syndesmotic fixation
Because the interosseous membrane and syndesmotic ligaments are extensively disrupted, most authors stabilise the syndesmosis. Whether a screw or a suture-button is superior, and whether every case requires fixation once a Weber B fibula is anatomically plated, remain debated — driven by the wider syndesmosis literature rather than Bosworth-specific trials.
The posterior malleolus
A posterior malleolar fragment is present in roughly 70% of cases and often forms part of the "lock". There is no consensus on a size threshold for fixation specific to Bosworth injuries; decisions follow general posterior-malleolus principles (fragment size, articular involvement, syndesmotic stability), informed by CT.
Evidence quality
The entire literature is Level IV/V — case reports and small series. No randomised or large comparative data exist, so prognosis figures and approach recommendations are based on aggregated case experience and must be presented with appropriate caution.
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Irreducible Ankle Dislocation
"A 25-year-old rugby player presents with a severe ankle deformity after a tackle. The foot is externally rotated 90 degrees. There is a deep skin pucker over the medial malleolus. You attempt reduction in ED but it feels 'blocked'."
Diagnosis: Bosworth Fracture-Dislocation.
Pathology:
- Posterior dislocation of the distal fibula behind the distal tibia.
- The fibula is entrapped by the posterior tubercle of the tibia (incisura fibularis posterior rim).
- The interosseous membrane is torn.
- The "Axilla sign" (medial pucker) is due to severe capsular traction.
Action: Stop closed attempts. Obtain CT or proceed to Urgent Open Reduction.
Intraoperative Reduction Difficulty
"You are in the operating room for a Bosworth fracture. You have performed a lateral approach. You cannot get the fibula back into the notch."
Reduction Maneuvers:
- Bone Hook: Hook the fibula and pull laterally/anteriorly.
- Osteotomy: Rarely, a small osteotomy of the blocking posterior tibial tubercle can be done (if small).
- Soft Tissue Release: Ensure no tendon (peroneals) interposition.
- Patient Position: Ensure muscle relaxation (paralysis).
- Syndesmosis: Once reduced, fix the fibula fracture first, then stabilize syndesmosis.
The Misdiagnosed Bosworth
"A 44-year-old is referred from a peripheral hospital 5 days after an 'ankle sprain' that was splinted as a Weber B fracture. They have ongoing severe pain, cannot weight-bear, and the foot looks externally rotated. The original AP radiograph shows tibiofibular overlap crossing the joint line."
Why missed: On the AP view a Bosworth lesion mimics a 'badly reduced' Weber B fracture. The lateral view was not scrutinised for the posterior fibula.
Confirm:
- Repeat dedicated AP and lateral radiographs. Look for posterior tibiofibular dissociation on the lateral view (the most reliable sign) and posterior talar subluxation.
- Obtain CT with 3D reconstruction to define the entrapment and the posterior malleolar fragment.
Manage:
- Assess skin and neurovascular status urgently; a delayed/neglected Bosworth is at high risk of soft-tissue compromise and compartment syndrome.
- Proceed to open reduction (posterolateral approach), fibular and posterior malleolar fixation, and syndesmotic stabilisation. Avoid further forceful closed attempts.
- Counsel about a guarded prognosis given the delay.
MCQ Practice Points
MCQ Focus: Anatomy
Q: What structure acts as the fulcrum trapping the fibula in a Bosworth injury? A: The Posterior Tubercle of the distal tibia (posterior aspect of the incisura fibularis).
MCQ Focus: Imaging
Q: Which X-ray view is diagnostic for Bosworth fracture-dislocation? A: The Lateral Ankle view, showing the fibula posterior to the tibia (overlap is normally present; clear space implies dislocation).
MCQ Focus: Treatment
Q: Primary management for a confirmed Bosworth injury? A: Open Reduction. Closed reduction typically fails and risks fracture.
MCQ Focus: Associated Injury
Q: Bosworth fracture-dislocations are almost universally associated with injury to which ligamentous complex? A: The Syndesmosis (AITFL, PITFL, IOM).
MCQ Focus: Complication
Q: The 'Axilla Sign' in ankle trauma suggests risk of which complication? A: Skin necrosis (medial side) and Bosworth injury.
Guidelines, Registries & Global Practice
Global epidemiology:
- A rare injury worldwide (under 2% of ankle fractures), with roughly 175 cases in the world literature; concentrated in major trauma centres because of referral patterns.
- Mechanism is consistent across regions: severe external rotation of the planted, supinated foot — classically a planted-foot tackle in contact sport (rugby, soccer, gridiron, Australian football) or a high-energy fall/motor-vehicle crash.
- Age-dependent morphology (Bartoníček, 2007): physeal separation in children/adolescents, pure dislocation in young adults, fibular fracture in middle-aged/older adults.
Guideline and consensus positions (side by side):
| Body / source | Position relevant to Bosworth |
|---|---|
| AO Foundation | Treat as an unstable ankle fracture-dislocation: urgent reduction of the dislocation, anatomical fibular length/rotation, and syndesmotic stabilisation. |
| EFORT (current concept review, 2024) | CT with 3D reconstruction as diagnostic standard; avoid repeated closed attempts; early ORIF is standard; postoperative CT to confirm reduction. |
| BOA / BOAST (Open Fractures & Ankle principles, UK) | Emphasis on early reduction of a deformed/dislocated ankle to protect skin, senior-led decision-making, and timely transfer if soft tissues are at risk. |
| AAOS (general ankle-fracture guidance, US) | No Bosworth-specific guideline; managed under unstable ankle-fracture and syndesmosis principles. |
Note: there is no Bosworth-specific guideline from any society — the literature is Level IV/V — so recommendations are extrapolated from ankle fracture-dislocation and syndesmosis principles.
Registry context:
- No arthroplasty/implant registry captures Bosworth injuries specifically. National ankle-fracture and syndesmosis data (e.g. from large trauma registries) inform syndesmotic fixation practice generally — the screw-versus-suture-button debate is driven by that wider evidence, not Bosworth-specific data.
High- vs limited-resource practice variation:
- Well-resourced settings: Early CT, posterolateral ORIF, intra-operative and postoperative CT to confirm syndesmotic and posterior-malleolar reduction, suture-button or screw fixation, and functional rehabilitation in a removable boot.
- Limited-resource settings: Diagnosis rests on careful scrutiny of plain radiographs (the lateral view for posterior fibular dissociation) where CT is unavailable; reduction must not be repeatedly attempted; early transfer to a unit able to perform open reduction is the priority, since delay drives skin necrosis and compartment syndrome.
Bosworth Fracture-Dislocation
Clinical summary
Key Features
- •Fibula dislocated POSTERIOR to tibia
- •Trapped by posterior tibial tubercle
- •Irreducible by closed means
- •Axilla sign (medial skin pucker)
- •Lateral X-ray is diagnostic
Management
- •Urgent Open Reduction (ORIF)
- •Posterolateral approach often best
- •Fix fibula fracture
- •Stabilize syndesmosis (100% injured)
- •Watch for compartment syndrome
Common Pitfalls
- •Mistaking for simple ankle fracture on AP view
- •Continuing forceful closed reduction (causes fracture)
- •Delaying surgery (skin necrosis risk)
- •Missing proximal fibula fracture (Maisonneuve)
Prognosis
- •Stiffness is common
- •Post-traumatic arthritis risk
- •Good outcome if reduced within 24 hours
- •Poor outcome if missed/delayed