Intercalated Segment Concept | SL vs LT Injury | Static vs Dynamic | SLAC Progression
- Intercalated segment = proximal carpal row (no tendon attachments), controlled by ligaments
- DISI = SL tear, lunate follows triquetrum dorsally (extended), SL angle over 70°
- VISI = LT tear, lunate follows scaphoid palmarly (flexed), SL angle under 30°
- Watson scaphoid shift test pathognomonic for SL instability (compare to contralateral)
- Static vs dynamic - static shows on plain films, dynamic needs stress views
- “True lateral X-ray essential - measure SL angle from scaphoid axis to lunate perpendicular
- “SL gap over 3mm on PA = Terry Thomas sign (compare to other side)
- “Capitolunate angle over 15 degrees confirms carpal malalignment
- “DISI progresses to SLAC wrist, VISI to ulnocarpal/midcarpal arthritis
Clinical Imaging
Imaging Atlas



SL ligament injury causes dorsal lunate tilt. SL angle over 70 degrees. Watson scaphoid shift test positive. Leads to SLAC wrist if untreated. 10x more common than VISI.
LT ligament injury causes volar lunate tilt. SL angle under 30 degrees. Reagan's LT ballottement test positive. Leads to ulnocarpal/midcarpal arthritis. Less common.
Dynamic = normal standard X-rays, abnormal stress views (partial tear). Static = abnormal resting X-rays (complete tear). Static has worse prognosis.
Terry Thomas sign = SL gap over 3mm on PA view. Scaphoid ring sign = rotatory subluxation. Gilula's arcs disrupted. Compare to contralateral wrist.
| Feature | DISI | VISI | Normal |
|---|---|---|---|
| SL Angle | Over 70° | Under 30° | 30-60° (avg 47°) |
| Lunate Position | Extended (dorsal tilt) | Flexed (volar tilt) | Neutral |
| Ligament Injured | Scapholunate | Lunotriquetral | Intact |
| Clinical Test | Watson scaphoid shift | Reagan LT ballottement | Negative |
| Arthritis Pattern | SLAC wrist | Ulnocarpal/midcarpal | None |
| Frequency | Common (90%) | Rare (10%) | N/A |
DISIDISI vs VISI Pattern
Hook:D for Dorsal, D for DISI - the lunate tilts Dorsally because SL ligament has strongest Dorsal component
VISIVISI Pattern
Hook:V for Volar, V for VISI - lunate follows scaphoid into Volar (palmar) flexion when LT torn
SCLLMayfield Stages
Hook:SCLL like SKULL - injury progresses around the lunate like drawing a skull, ending with lunate dislocation
DPPSL Ligament Strength
Hook:DPP like Department of Public Prosecutions - Dorsal is the chief prosecutor, hardest to defeat
Overview
Understanding Carpal Instability
Carpal instability represents a spectrum of wrist pathology where normal carpal kinematics are disrupted due to ligamentous injury. The intercalated segment concept is central to understanding DISI and VISI patterns.
The Intercalated Segment Concept
The proximal carpal row (scaphoid, lunate, triquetrum) is termed the "intercalated segment" because it has:
- No direct tendon attachments - movement is passive, controlled by ligaments
- Positioned between the radius and distal carpal row
- Acts as a link transmitting forces across the wrist
The proximal row naturally wants to:
- Flex under axial load (due to scaphoid geometry)
- Extend under compression (due to capitate articulation)
These opposing forces are balanced by the intrinsic intercarpal ligaments (SL and LT).
Why DISI and VISI Occur
DISI (Scapholunate Disruption):
- SL ligament torn leads to scaphoid no longer tethered to lunate
- Scaphoid flexes palmarly under load (natural tendency)
- Lunate, now attached only to triquetrum, extends dorsally
- Result: Lunate tilts dorsally = Dorsal Intercalated Segment Instability
VISI (Lunotriquetral Disruption):
- LT ligament torn leads to triquetrum no longer tethered to lunate
- Lunate loses stabilising effect of helicoid triquetrum
- Lunate follows scaphoid into flexion
- Result: Lunate tilts palmarly = Volar Intercalated Segment Instability
Key Biomechanical Principles:
- Scaphoid naturally flexes; triquetrum naturally extends
- Lunate follows whichever bone it remains attached to
- SL injury leads to lunate following triquetrum into dorsal tilt (DISI)
- LT injury leads to lunate following scaphoid into volar tilt (VISI)
Static vs Dynamic Instability
Dynamic Instability:
- Radiographs appear normal at rest
- Abnormal alignment only with stress views
- Partial ligament injury
- Better prognosis with early treatment
Static Instability:
- Abnormal alignment on standard radiographs
- Complete ligament disruption
- Often requires surgical reconstruction
- Higher risk of secondary arthritis
Pathophysiology and Mechanisms
Functional Anatomy of Carpal Ligaments
Understanding carpal instability requires detailed knowledge of the intrinsic and extrinsic carpal ligaments.
Intrinsic Ligaments (Intercarpal)
Scapholunate Ligament (SL):
- Dorsal portion - thickest and strongest (2-3mm)
- Palmar portion - intermediate strength
- Proximal (membranous) portion - weakest, no structural role
- Dorsal SL is the primary restraint to scaphoid flexion/pronation
- Rupture sequence: palmar leads to proximal leads to dorsal
Lunotriquetral Ligament (LT):
- Palmar portion - strongest component
- Dorsal portion - intermediate
- Proximal portion - membranous
- Palmar LT is primary restraint to triquetral extension
- Less commonly injured than SL
Extrinsic Ligaments
Palmar Extrinsic Ligaments (more important):
- Radioscaphocapitate (RSC) - primary palmar stabiliser
- Long radiolunate (LRL) - lunate stabilisation
- Short radiolunate (SRL) - palmar constraint
- Radioscapholunate (RSL) - neurovascular conduit, minimal structural role
Dorsal Extrinsic Ligaments:
- Dorsal radiocarpal (DRC) - dorsal constraint
- Dorsal intercarpal (DIC) - scaphoid-triquetrum link
Carpal Rows and Motion
Proximal Row (Intercalated Segment):
- Scaphoid, lunate, triquetrum
- No direct tendon attachments
- Motion controlled by adjacent bones and ligaments
- Moves as a unit when ligaments intact
Distal Row:
- Trapezium, trapezoid, capitate, hamate
- Rigidly interconnected
- Minimal intercarpal motion
- Fixed relationship with metacarpals
Dart Thrower's Motion:
- Radial deviation + extension to ulnar deviation + flexion
- Predominantly midcarpal motion
- Least stress on intercarpal ligaments
- Explains why this motion is preserved after some injuries
Blood Supply
Scapholunate Ligament:
- Dorsal branch of radial artery
- Anterior interosseous artery
- Limited vascularity in central portion
Lunotriquetral Ligament:
- Ulnar artery branches
- Anterior interosseous artery
- Slightly better vascularity than SL
Neural Innervation
- Posterior interosseous nerve - dorsal ligaments
- Anterior interosseous nerve - palmar ligaments
- Proprioceptive function important for carpal kinematics
- Denervation procedures may address pain but sacrifice proprioception
Classification Systems
Progressive Perilunar Instability
Sequential ligament disruption pattern in hyperextension injuries:
Stage I: Scapholunate ligament rupture resulting in SL dissociation.
Stage II: Plus capitolunate dislocation resulting in perilunate dislocation.
Stage III: Plus lunotriquetral ligament rupture causing LT disruption.
Stage IV: Plus dorsal radiocarpal ligament rupture causing lunate dislocation into carpal tunnel.
Each stage includes all previous stages - Stage IV has complete ligamentous disruption around the lunate.
Clinical Assessment
History and Examination
History
Mechanism of Injury:
- Fall on outstretched hand (FOOSH) - most common
- Hyperextension with ulnar deviation leads to SL injury
- Extension with radial deviation leads to LT injury
- High-energy trauma: perilunate dislocations
Symptoms:
- Wrist pain (dorsal for SL, ulnar for LT)
- Weakness of grip
- "Clunking" or "clicking" with movement
- Pain with weight-bearing activities
- Swelling (often minimal in chronic cases)
Red Flags:
- Acute severe deformity leads to perilunate dislocation
- Median nerve symptoms leads to acute carpal tunnel from dislocation
- Associated fractures (scaphoid, radial styloid)
Physical Examination
Inspection:
- Swelling (dorsal = SL, ulnar = LT)
- Prominence of ulnar head (LT injury)
- Carpal height loss (chronic instability)
Palpation:
- SL interval tenderness (1cm distal to Lister's tubercle)
- LT interval tenderness (ulnar to lunate)
- Scaphoid tubercle tenderness (SL injury)
Special Tests for Scapholunate Instability
Watson Scaphoid Shift Test:
- Patient's forearm in neutral rotation
- Examiner's thumb on scaphoid tubercle, fingers dorsally
- Apply pressure while moving wrist from ulnar to radial deviation
- Positive: Painful clunk as scaphoid subluxes dorsally
- Compare to contralateral side - may be positive bilaterally in lax individuals
Scaphoid Compression Test:
- Axial load to thumb metacarpal
- Positive: Pain at SL interval
- Tests SL ligament integrity under compression
Finger Extension Test:
- Resist active finger extension
- Positive: Increased dorsal wrist pain
- Indicates SL pathology
Special Tests for Lunotriquetral Instability
LT Ballottement Test (Reagan's Test):
- Stabilise lunate with one hand
- Translate triquetrum dorsally and palmarly
- Positive: Pain, crepitus, or increased motion
- Compare to contralateral side
LT Compression Test:
- Ulnar deviation of wrist
- Apply axial load through ring/small finger metacarpals
- Positive: Pain at LT interval
Shuck Test:
- Pisiform used as lever to load LT joint
- Positive: Pain, clicking
Carpal Instability Patterns
Carpal Instability Dissociative (CID):
- Disruption within a carpal row
- SL dissociation leads to DISI
- LT dissociation leads to VISI
- Most common pattern
Carpal Instability Non-Dissociative (CIND):
- Disruption between carpal rows
- Radiocarpal or midcarpal instability
- Often involves extrinsic ligament injury
- Catch-up clunk with ulnar to radial deviation
Carpal Instability Combined (CIC):
- Both dissociative and non-dissociative
- Perilunate injuries
- Severe trauma
Carpal Instability Adaptive (CIA):
- Secondary to malunited distal radius fracture
- Dorsal malunion leads to compensatory VISI
- Palmar malunion leads to compensatory DISI
- Treat the radius, not the carpal malalignment
Differential Diagnosis
| Condition | Key distinguishing features | Discriminating test / investigation |
|---|---|---|
| Scapholunate dissociation (DISI) | Dorsoradial pain, weak grip, painful clunk on radial deviation | SL angle greater than 70 degrees on lateral; Terry Thomas sign; positive Watson shift |
| Lunotriquetral dissociation (VISI) | Ulnar-sided pain, clicking on ulnar deviation | SL angle less than 30 degrees; positive Reagan ballottement; MR arthrogram |
| Midcarpal instability (CIND) | Painless or painful catch-up clunk with ulnar deviation, ligamentous laxity | Normal SL/LT intervals; dynamic fluoroscopy shows sudden midcarpal shift |
| TFCC tear / DRUJ instability | Ulnar pain, painful forearm rotation, click on pronosupination | Positive fovea sign and TFCC stress test; MR arthrogram; DRUJ ballottement |
| Occult scaphoid fracture | Acute radial pain, anatomical snuffbox tenderness after FOOSH | Repeat radiographs/CT/MRI; intact SL interval distinguishes from SL injury |
| Kienbock disease (lunate AVN) | Insidious central dorsal wrist pain, stiffness, no clear trauma | Lunate sclerosis/collapse on radiograph; MRI marrow change; normal SL angle early |
Investigations
Imaging Studies
Plain Radiographs
Standard Views:
- PA view - carpal spacing, arcs of Gilula
- True lateral - carpal angles (most important for DISI/VISI)
- Scaphoid view - scaphoid pathology
- Contralateral comparison - essential for borderline cases
Key Measurements on Lateral View:
Scapholunate Angle:
- Line along long axis of scaphoid
- Line perpendicular to lunate distal articular surface
- Normal: 30-60 degrees (average 47 degrees)
- DISI: greater than 70 degrees
- VISI: less than 30 degrees
Capitolunate Angle:
- Line along long axis of capitate
- Line perpendicular to lunate
- Normal: less than 15 degrees
- Greater than 15 degrees = instability
Radiolunate Angle:
- Long axis of radius to lunate
- Normal: neutral (0 degrees ± 10)
- Abnormal in DISI/VISI patterns
PA View Findings:
SL Gap (Terry Thomas Sign):
- Normal SL interval: less than 3mm
- Greater than 3mm suggests SL injury
- Greater than 5mm = complete SL tear
- Compare to contralateral side
Gilula's Arcs:
- Arc I: Proximal carpal row proximal surfaces
- Arc II: Proximal carpal row distal surfaces
- Arc III: Capitate-hamate proximal surfaces
- Disruption indicates intercarpal pathology
Scaphoid Ring Sign:
- Cortical ring appearance of scaphoid
- Indicates scaphoid flexion (rotatory subluxation)
- Seen in SL dissociation/DISI
Stress Radiographs
Clenched Fist View:
- AP view with tight fist
- Loads scapholunate interval
- May reveal dynamic widening
Radial/Ulnar Deviation Views:
- Maximum radial and ulnar deviation
- Assess scaphoid motion
- Dynamic DISI may only appear in radial deviation
Fluoroscopy:
- Real-time assessment of carpal motion
- Dart thrower's arc evaluation
- Provocative manoeuvres under imaging
Advanced Imaging
MRI:
- Soft tissue ligament visualisation
- SL and LT ligament integrity
- Associated TFCC pathology
- Bone marrow oedema pattern
MR Arthrography:
- Gold standard for ligament tears
- 90% sensitivity/specificity for SL tears
- Contrast leak patterns:
- Radiocarpal space leads to midcarpal = SL tear
- Midcarpal leads to radiocarpal = LT tear
CT:
- Bone detail
- Fracture identification
- 3D reconstructions for surgical planning
Arthroscopy:
- Definitive diagnostic tool
- Allows dynamic assessment
- Grading of ligament tears (Geissler classification)
- Therapeutic intervention possible
Geissler Arthroscopic Classification
Grade I:
- Attenuation/haemorrhage of interosseous ligament
- No instability with probing
Grade II:
- Ligament attenuation with incongruity
- Step-off visible between carpal bones
- Probe cannot be passed between bones
Grade III:
- Incongruity and step-off
- Probe can pass between bones (from midcarpal side)
- Volar ligament intact
Grade IV:
- Complete ligament disruption
- 2.7mm arthroscope passes through gap
- Gross instability
Management
Indications:
Pre-dynamic instability with partial ligament tears and no instability on examination. Patient factors precluding surgery. Temporary stabilisation before definitive surgery.
Treatment Protocol:
Immobilisation in slight flexion and ulnar deviation for 4-6 weeks with cast or splint. Physiotherapy for proprioception and grip strengthening. Activity modification to avoid provocative movements. Serial examinations to monitor for progression.
Surgical Technique
Setup and Approach:
Supine position with arm table, tourniquet applied to upper arm. Dorsal longitudinal incision centred over Lister's tubercle extending 4-5cm. Develop interval between 3rd and 4th extensor compartments. Protect extensor tendons and create dorsal capsulotomy (ligament-sparing or traditional).
Direct Repair Technique:
Identify torn SL ligament remnants. Debride non-viable tissue. Place suture anchors in scaphoid and lunate. Repair dorsal SL ligament with non-absorbable sutures. May augment with dorsal capsulodesis.
Reconstruction (Modified Brunelli):
Harvest FCR tendon strip (10cm length, 1/2 width). Drill 3.2mm tunnel through scaphoid from distal pole to SL interval. Pass tendon graft through scaphoid tunnel. Anchor to lunate with suture anchor or bone tunnel. Tensioned with wrist in neutral or slight extension.
K-wire Fixation:
Place 1.1-1.4mm K-wires across SL joint (2 wires) and scaphocapitate joint (1-2 wires). Check reduction fluoroscopically. Wires remain 8-10 weeks.
Complications
Complications of Carpal Instability
Natural History (Untreated)
DISI/Scapholunate Dissociation:
- Progressive radioscaphoid arthritis
- SLAC wrist pattern (Stages I to II to III)
- Similar to SNAC wrist progression
- 30-50% develop arthritis within 10 years
VISI/Lunotriquetral Dissociation:
- Less predictable progression
- Ulnocarpal impaction may develop
- Midcarpal arthritis possible
- Generally slower progression than DISI
Complications of Surgery
Early Complications:
Infection:
- Superficial: 2-5%
- Deep: less than 1%
- Treatment: antibiotics, debridement if needed
Nerve Injury:
- Superficial radial nerve (dorsal approach)
- DBRCU (dorsal approach)
- Posterior interosseous nerve
- Usually neuropraxia, resolves
Hardware Problems:
- K-wire migration/breakage
- Screw prominence
- Removal often required
Late Complications:
Persistent Instability:
- Incomplete ligament healing
- Stretched repair
- May require revision or salvage
Stiffness:
- Common after prolonged immobilisation
- Intensive physiotherapy required
- May require tenolysis/capsular release
Recurrent DISI/VISI:
- Progressive stretching of reconstruction
- Revision surgery options limited
- May progress to salvage
Secondary Arthritis:
- Altered joint loading
- Progressive cartilage degeneration
- Ultimate outcome similar to untreated instability
- Salvage fusion may be required
Procedure-Specific Complications:
Limited Fusions (STT, SC):
- Non-union: 5-15%
- Hardware prominence
- Adjacent joint arthritis
- Residual instability
Proximal Row Carpectomy:
- Radiocapitate arthritis
- Progressive pain
- May require total wrist fusion
Total Wrist Fusion:
- Loss of all wrist motion
- Hardware failure
- Non-union: less than 5%
- Adjacent joint stress
Managing Failed Surgery
Workup:
- Detailed history: what was done, when, outcomes
- Physical examination
- CT for fusion assessment
- MRI for soft tissue evaluation
- Diagnostic arthroscopy if needed
Revision Options:
- Re-repair/reconstruction (early failure)
- Conversion to limited fusion
- Salvage procedures
Patient Counselling:
- Progressive procedures available
- Each surgery reduces options
- Ultimate salvage is wrist fusion
- Realistic expectations essential
Postoperative Care
Immobilisation:
Long-arm cast or splint for first 2-4 weeks to control forearm rotation. Transition to short-arm cast/splint for remaining 4-6 weeks. Wrist positioned in slight extension and ulnar deviation.
Monitoring:
Wound check at 10-14 days. Suture/staple removal at 2 weeks. Monitor for infection, neurovascular compromise. X-rays at 2 and 6 weeks to assess hardware and reduction.
Early Exercises:
Active finger ROM from day one to prevent stiffness. Shoulder and elbow ROM exercises. Oedema control with elevation and compression.
Outcomes and Prognosis
Long-Term Outcomes
SL Instability Treatment Outcomes:
Direct repair (acute): 80-90% good/excellent results when performed within 3 weeks of injury. Results deteriorate significantly after 6 weeks.
Capsulodesis: 70% satisfaction at 5 years, but 30% recurrent DISI. Better for dynamic instability as bridge procedure.
Tendon reconstruction (modified Brunelli): 78% good/excellent at 3 years declining to 56% at 10 years. Progressive stretching of reconstruction is a concern.
Limited fusions (STT, scaphocapitate): 75-85% pain relief. Approximately 50% motion preservation. 5-15% non-union rate.
LT Instability Treatment Outcomes:
Direct repair (acute): Better outcomes than chronic repair. 80% good results when performed acutely.
LT arthrodesis: 90% union rate. Minimal motion loss. Most predictable outcome for chronic LT instability.
Salvage Procedure Outcomes:
PRC: 80% good/excellent at 5-10 years. Preserves functional ROM. May deteriorate over time with radiocapitate arthritis.
Four-corner fusion: Similar outcomes to PRC. May be preferred for heavy manual labourers.
Total wrist fusion: Reliable pain relief. Complete loss of wrist motion. Last resort option.
Prognostic Factors:
Favourable: Acute injury (under 6 weeks), dynamic instability, young age, no arthritis, good compliance.
Unfavourable: Chronic injury, static instability, arthritis present, heavy manual occupation, bilateral disease.
Evidence Base
Current Evidence
Mayfield Classification - Progressive Perilunar Instability
- Cadaveric loading of 32 wrists to failure (mechanism: extension, ulnar deviation, intercarpal supination) produced 13 perilunate and 2 lunate dislocations in a sequential, predictable fashion. Defined the four-stage perilunar instability (PLI) scale: Stage I (scapholunate diastasis, least instability) through Stage IV (lunate dislocation, greatest instability). Reduction was achieved by reversing the injury mechanism.
Geissler Arthroscopic Classification (Original Description)
- Arthroscopy of 60 displaced intra-articular distal radius fractures found intracarpal soft-tissue injury in 41 patients (68%): TFCC tears (26), scapholunate interosseous tears (19) and lunotriquetral tears (9). This is the source describing the arthroscopic grading of interosseous ligament injury (probing from the midcarpal joint) now known as the Geissler classification.
Dorsal Capsulodesis - Intermediate Outcomes
- 31 patients with chronic SL dissociation (18 dynamic, 13 static) treated by dorsal capsulodesis (Blatt or Mayo technique), mean follow-up 54 months. Wrist motion fell ~20% and grip strength did not improve. Pain improved but only 2 patients were pain-free. Radiographically the SL gap increased (2.7 to 3.9 mm) and the SL angle increased (56 to 62 degrees) - capsulodesis did not maintain carpal alignment.
Dorsal Intercarpal Ligament Capsulodesis - Long-Term
- 59 patients followed a mean of 8.25 years after capsulodesis for static SL instability. Mean DASH 28 and Mayo wrist score 61. After early improvement, mean SL and radiolunate angles deteriorated back toward pre-operative values and carpal height index fell; 78% had radiographic degenerative arthritis. Capsulodesis did not maintain carpal reduction over time, although most patients retained acceptable function.
Lunotriquetral Arthrodesis - Technique and Union
- 22 patients undergoing LT arthrodesis. Herbert screw supplemented with a K-wire, combined with immobilisation longer than 6 weeks, achieved union in all patients - including revision of prior failed arthrodesis. Pain improved in all and all previously-working patients returned to work. Routine PA/lateral films frequently failed to profile the fusion; fluoroscopy or tomography is recommended to confirm union.
LT Arthrodesis - High Failure Rate Caution
- 29 patients with chronic LT ligament tears treated by LT arthrodesis. Fusion was achieved in only 16 cases with non-union persisting in 13; 17 wrists remained painful and 19 patients required on average two additional procedures, three progressing to total wrist arthrodesis. The authors questioned the procedure relative to ligamentoplasty and extended (four-corner) arthrodesis.
Garcia-Elias Three-Ligament Tenodesis (Reference Reconstruction)
- Describes a prognostic six-stage treatment algorithm for SL instability and the three-ligament tenodesis (3LT) for non-repairable complete SL rupture causing reducible carpal malalignment without secondary osteoarthritis. Reports promising early results for restoring carpal alignment, combining features of three earlier techniques.
SLAC Wrist - Natural History of Untreated SL Dissociation
- Review of 4000 wrist radiographs identified 210 cases of degenerative arthritis. The commonest pattern (57%) was radioscaphoid-to-scaphocapitate degeneration (SLAC), 27% was scapho-trapezio-trapezoid, and 15% combined. The radiolunate joint is characteristically spared, defining the predictable SLAC progression.
Capsulodesis vs Reconstruction - Pooled Evidence
- Systematic review of 308 patients across 11 studies (chronic SL tears, mean 11 months to surgery). No significant difference between capsulodesis and ligament reconstruction in wrist flexion or extension. Pooled post-operative SL angle/gap were 60.3 degrees / 3.44 mm after capsulodesis and 56.5 degrees / 2.72 mm after reconstruction. Studies were heterogeneous, precluding a definitive recommendation.
Viva Scenarios
Examination Practice
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old man presents 3 months after a fall on his outstretched hand. He has persistent dorsal wrist pain and weakness. X-rays show widened SL interval and increased SL angle. How would you assess and manage this patient?”
“You are shown a lateral wrist X-ray with SL angle of 25 degrees and capitolunate angle of 20 degrees. What is the diagnosis and how does this differ from DISI?”
“Describe the Mayfield classification of perilunate instability and explain the anatomical basis for this progression.”
MCQ Practice Points
Q: What SL angle confirms DISI pattern on lateral wrist radiograph?
A: Greater than 70 degrees confirms DISI pattern. Normal SL angle is 30-60 degrees (average 47 degrees). VISI pattern shows SL angle less than 30 degrees.
Q: A patient with perilunate dislocation has disruption of SL and LT ligaments with the lunate still in the lunate fossa. What Mayfield stage is this?
A: Stage III - includes SL disruption (Stage I), capitolunate disruption (Stage II), and LT disruption (Stage III). Stage IV would show lunate dislocation into carpal tunnel.
Q: Which clinical test is most specific for scapholunate ligament injury?
A: Watson scaphoid shift test - pressure on scaphoid tubercle while moving wrist from ulnar to radial deviation produces painful dorsal subluxation clunk. Must compare to contralateral side as may be positive bilaterally in lax individuals.
Q: What is the preferred treatment for chronic LT instability with static VISI deformity?
A: LT arthrodesis - provides 90% union rate with minimal motion loss since LT joint contributes little to overall wrist motion. More predictable than ligament reconstruction.
Q: What is the natural history of untreated chronic SL dissociation?
A: SLAC wrist (scapholunate advanced collapse) - predictable arthritis pattern progressing from radial styloid to scaphoid fossa to capitolunate joint. Radiolunate joint typically spared. 30-50% develop arthritis within 10 years.
Guidelines, Registries & Global Practice
Global Epidemiology
Scapholunate (SL) interosseous ligament injury is the commonest form of carpal instability and is frequently occult at first presentation. According to PubMed, arthroscopic studies of displaced intra-articular distal radius fractures found intracarpal soft-tissue injury in 68% of wrists, with SL tears in around one-third (Geissler 1996, PMID 8613442). High-energy AO type B (shearing) distal radius fractures carry an especially high SL injury burden - 14 of 15 wrists in one series (Yoshida 2015, PMID 26388007). DISI substantially outnumbers VISI in clinical practice, and the untreated SL-dissociation natural history is a predictable SLAC arthritis pattern present in roughly 57% of degenerative wrists reviewed radiographically (Watson & Ballet 1984, PMID 6725894).
Guideline & Society Positions (Side-by-Side)
There is no single high-level clinical practice guideline dedicated to DISI/VISI; recommendations are derived from hand-surgery society consensus and systematic reviews. Evidence underpinning operative choices is uniformly low (Level III-IV).
| Body / Source | Position | Evidence level |
|---|---|---|
| AAOS / ASSH (USA) | Hand-surgeon-led care; arthroscopy is the diagnostic reference standard; early repair for acute reparable SL tears | Consensus / Level IV |
| BSSH / BOA (UK) | Staged management by Garcia-Elias algorithm; reconstruction for reducible static DISI without arthritis | Consensus / Level IV |
| FESSH / EFORT (Europe) | Acute repair preferred where feasible; 3-ligament tenodesis as reference reconstruction | Consensus / Level IV |
| Cochrane / systematic reviews | No technique proven superior for chronic SL instability; prospective trials needed | Level III (heterogeneous) |
Registry Evidence
No national joint registry (AOANJRR, NJR, AJRR) collects carpal-ligament reconstruction as a discrete, tracked procedure, so registry-grade survivorship data do not exist for DISI/VISI surgery. The best available pooled evidence comes from systematic reviews rather than registries.
- Chronic non-arthritic SL dissociation: pain fell from 6.0 to 2.8 at 2 years with capsulodesis and tenodesis performing similarly; complication rate 20%, CRPS 3.8% (Naqui 2017, PMID 29022774).
- Capsulodesis versus reconstruction: no significant difference in motion or radiographic correction across 308 patients (Wang 2016, PMID 28690470).
- Acute perilunate injuries: pooled complications include arthritis 30%, carpal instability 15%, lunate avascular necrosis 12% (Lee 2023, PMID 36708152).
Practice Variation
- Diagnosis. Wrist arthroscopy is the diagnostic reference standard internationally, but access varies; MRI and MR arthrography (around 90% sensitivity/specificity for SL tears) are first-line where arthroscopy is rationed.
- Timing. Universal agreement that acute reparable SL tears (within ~6 weeks) do best with early repair; the threshold for reconstruction versus salvage in chronic disease varies by surgeon and resource setting.
- Reconstruction choice. Three-ligament tenodesis (Garcia-Elias) predominates in Europe/UK; RASL, internal-brace augmentation and capsulodesis remain in use across North America, reflecting absence of comparative superiority data.
- Rehabilitation. Specialist hand therapy and custom thermoplastic splinting are standard of care in high-income systems (e.g. AHTA-accredited therapists in Australia; BAHT in the UK; ASHT/CHT in North America) but are less consistently available in lower-resourced settings.
Local Access Notes (Australia)
Most carpal ligament injuries are first managed in emergency departments or primary care, with early referral to fellowship-trained hand surgeons for positive clinical tests or radiographic abnormality. MRI/MR arthrography is widely available in metropolitan areas though public wait times (commonly several weeks) can delay diagnosis of acute injuries, so expedited imaging is advised when acute repair is contemplated. Reconstruction, arthrodesis and wrist arthroscopy are funded within the public hospital system. Standard analgesics (paracetamol, NSAIDs, opioids) are available on the PBS; there are no device-specific PBS listings for these procedures.
Radiographic Criteria
- Normal SL angle: 30-60° (average 47°)
- DISI: SL angle over 70°, lunate extended dorsally
- VISI: SL angle under 30°, lunate flexed palmarly
- Normal CL angle: under 15°
- SL gap over 3mm = Terry Thomas sign
- Scaphoid ring sign = rotatory subluxation
Clinical Tests
- Watson scaphoid shift: SL instability (DISI)
- LT ballottement (Reagan's): LT instability (VISI)
- Compare all tests to contralateral side
- Dynamic instability = positive stress tests only
- Static instability = abnormal standard X-rays
Mayfield Stages
- Stage I: SL ligament
- Stage II: + Capitolunate (perilunate dislocation)
- Stage III: + LT ligament
- Stage IV: + Dorsal radiocarpal (lunate dislocation)
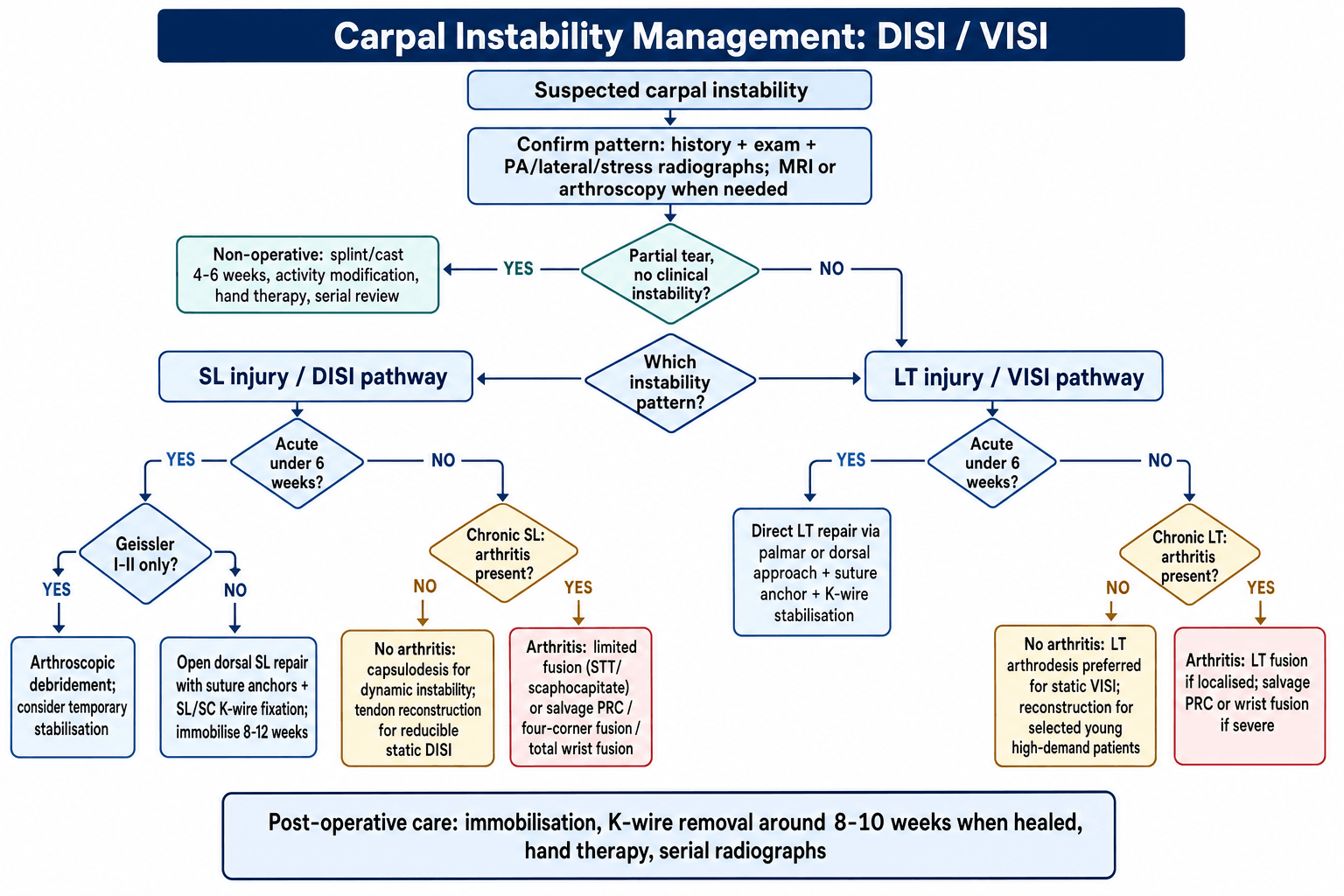
Treatment Algorithm
- Acute SL (under 6 weeks): Direct repair + K-wires
- Chronic SL (no arthritis): Tendon reconstruction
- SL + arthritis: Limited fusion or salvage
- LT instability: Arthrodesis preferred (90% union)
- Salvage: PRC, 4-corner fusion, wrist fusion
Key Biomechanics
- Scaphoid flexes; triquetrum extends
- Lunate follows attached bone
- SL tear leads to lunate follows triquetrum leads to DISI
- LT tear leads to lunate follows scaphoid leads to VISI
- DISI 10× more common than VISI
Exam Tips
- Always compare to contralateral wrist
- Explain intercalated segment concept
- Know Mayfield stages for viva
- Understand why reconstructions fail over time
- Be able to interpret lateral wrist X-rays