Extensor Mechanism Disruption | Boutonniere Deformity Risk | Zone III Injury
- Central slip inserts onto middle phalanx base dorsally
- Injury leads to volar migration of lateral bands = boutonniere deformity
- Elson test: PIP extension weakness with DIP floppy = central slip rupture
- Splint PIP in full extension for 6-8 weeks, allow DIP flexion
- Chronic boutonniere may require tendon reconstruction or arthroplasty
- “Boutonniere = PIP flexion + DIP hyperextension
- “Lateral bands migrate volar to PIP axis when central slip fails
- “Elson test is pathognomonic for central slip injury
- “Never delay diagnosis - early splinting prevents deformity
Clinical Imaging
Boutonniere Deformity and Central Slip Injuries

Central slip = middle band of extensor mechanism. Inserts on dorsal base of middle phalanx. Loss of central slip allows lateral bands to migrate volar to PIP axis.
PIP flexion + DIP hyperextension. Results from volar migration of lateral bands when central slip fails. Develops over 3-6 weeks if untreated.
Pathognomonic test for central slip rupture. PIP held at 90° over table edge. Attempted extension: if central slip intact = rigid DIP. If ruptured = floppy DIP + weak PIP extension.
Splint immediately in full PIP extension. Delay beyond 3 weeks risks fixed boutonniere. Splint for 6-8 weeks. Allow DIP flexion to prevent lateral band adhesion.
| Presentation | Diagnosis | Treatment | Key Pearl |
|---|---|---|---|
| Acute closed injury, PIP swelling | Positive Elson test, no wound | PIP extension splint 6-8 weeks | Early diagnosis prevents boutonniere |
| Open laceration over PIP dorsum | Visible central slip disruption | Primary repair + extension splint | Repair within 10-14 days optimal |
| Chronic PIP flexion contracture | Fixed boutonniere deformity | Reconstruction or arthroplasty | Requires lateral band mobilization |
VOLARBoutonniere Deformity Mechanism
Hook:Central slip rupture sends lateral bands VOLAR to create the classic boutonniere!
GRIPElson Test Steps
Hook:GRIP the PIP at 90 degrees and watch the DIP tell you the diagnosis!
PIPEXCentral Slip Injury Treatment
Hook:PIPEX = PIP Extension for central slip injuries!
Overview and Epidemiology
Central slip injuries are frequently missed in the acute setting because initial PIP extension is often preserved via intact lateral bands. The classic boutonniere deformity develops insidiously over 3-6 weeks as the lateral bands gradually migrate volar to the PIP joint axis. Early recognition and splinting prevent this disabling deformity.
- Forced flexion: Ball catching (jammed finger)
- Direct laceration: Dorsal PIP wound
- Crush injury: Industrial accidents
- Volar dislocation PIP: Ruptures central slip on reduction
- Grip weakness: Loss of PIP extension power
- Deformity: Cosmetically and functionally limiting
- Secondary OA: Chronic cases develop PIP arthritis
- Adjacent joints: DIP hyperextension causes pain
Pathophysiology
The extensor mechanism divides into three slips over the proximal phalanx: a central slip (middle band) and two lateral bands. The central slip inserts on the dorsal base of the middle phalanx and is the primary PIP extensor. The lateral bands continue distally to join as the terminal tendon at the DIP. When the central slip ruptures, the lateral bands lose their dorsal restraint and migrate volar to the PIP axis, transforming from PIP extensors into PIP flexors - creating the boutonniere deformity.
| Structure | Insertion | Function | When Injured |
|---|---|---|---|
| Central slip | Dorsal base middle phalanx | Primary PIP extension | Boutonniere deformity develops |
| Lateral bands (2) | Continue to DIP (terminal tendon) | Assist PIP extension, extend DIP | Migrate volar, hyperextend DIP |
| Triangular ligament | Connects lateral bands dorsally | Prevents lateral band separation | Attenuates, allows volar migration |
Normal: Central slip extends PIP, lateral bands held dorsal
After injury: Central slip torn, lateral bands lose dorsal tether
Week 1-2: Lateral bands begin volar migration
Week 3-6: Lateral bands cross volar to PIP axis
Result: Lateral bands now flex PIP and hyperextend DIP
Acute injury: Lateral bands still dorsal to PIP axis
Can extend PIP: Via lateral bands (weak)
Elson test positive: DIP floppy (no central slip tension)
Over weeks: Lateral bands migrate, extension lost
Classification and Types
Classification by Timing
| Stage | Clinical Features | Treatment | Prognosis |
|---|---|---|---|
| Acute (0-3 weeks) | Swelling, weak extension, positive Elson | Extension splinting 6-8 weeks | Excellent with early splinting |
| Subacute (3-12 weeks) | Early boutonniere, mild PIP contracture | Splinting trial, may need serial casting | Good if deformity correctable |
| Chronic (over 12 weeks) | Fixed PIP flexion, DIP hyperextension | Tendon reconstruction or arthroplasty | Variable, depends on PIP stiffness |
Understanding the temporal classification helps predict outcome with conservative treatment.
Clinical Assessment
- Mechanism: Forced flexion vs laceration
- Timing: Acute vs delayed presentation
- Function: Difficulty extending finger, grip weakness
- Pain: Over PIP dorsum, worse with flexion
- Inspect: PIP swelling, open wound, resting posture
- Active extension: Weak or absent at PIP
- Passive extension: Full range (acute) vs contracture (chronic)
- DIP function: Check terminal tendon integrity
Technique: Patient's PIP flexed to 90 degrees over edge of table. Examiner resists attempted PIP extension while palpating DIP.
Intact central slip: Strong PIP extension force, DIP rigid in extension
Ruptured central slip: Weak PIP extension, DIP becomes floppy (extension force transmitted through lateral bands to DIP)
Key point: The floppy DIP is the positive finding - it indicates all extensor force is going through lateral bands to DIP, bypassing the PIP.
| Test | Technique | Positive Finding | Sensitivity |
|---|---|---|---|
| Elson test | PIP at 90°, resist extension, palpate DIP | Weak PIP extension + floppy DIP | Gold standard - highly specific |
| Active PIP extension | Ask patient to extend PIP from flexion | Inability to fully extend (lag) | Can be normal acutely (lateral bands) |
| Boyes test | Passively extend PIP fully, release | PIP drops into flexion immediately | Less specific than Elson |

| Condition | Joint posture | Discriminating finding | Key test / imaging |
|---|---|---|---|
| Central slip injury (boutonniere) | PIP flexion + DIP hyperextension | Weak PIP extension with floppy DIP | Positive Elson test; X-ray for avulsion |
| Mallet finger (terminal tendon) | DIP flexion (drop) + neutral PIP | Loss of active DIP extension, PIP normal | Lateral X-ray for dorsal distal phalanx avulsion |
| Swan neck deformity | PIP hyperextension + DIP flexion (opposite) | Volar plate / FDS laxity, not central slip loss | Bunnell test; assess intrinsic tightness |
| PIP volar plate injury / dorsal dislocation | Painful PIP, possible hyperextension instability | Tenderness volar, stable extensor mechanism | Stress views; Elson test negative |
| Pseudo-boutonniere (volar plate contracture) | Fixed PIP flexion, DIP normal (no hyperextension) | No central slip rupture; flexion contracture from volar scar | Elson test negative; history of hyperextension injury |
| Septic / inflammatory PIP arthritis | Globally swollen, hot, painful PIP | Constitutional signs, no clear extensor deficit | Bloods, joint aspiration if infection suspected |
Pseudo-boutonniere follows a hyperextension injury with volar plate damage: it produces a fixed PIP flexion contracture but a normal DIP (no hyperextension) and a negative Elson test. True boutonniere has DIP hyperextension and a positive Elson test. Mistaking the two leads to inappropriate extension splinting that fails.
Investigations
Imaging Protocol
Views: PA, lateral, oblique of affected finger
Look for: Avulsion fracture of middle phalanx base (dorsal), PIP dislocation, PIP arthritis (chronic cases)
Clinical correlation: Most central slip injuries are purely soft tissue (X-ray normal)
Indication: Assess fracture fragment size and displacement
Threshold: Fragments involving over 25 percent of articular surface may need ORIF
Pre-op planning: Determine fixation strategy (screws vs tension band)
Indication: Chronic boutonniere to assess tendon quality and joint cartilage
Findings: Scarred central slip, volar lateral bands, PIP arthritic changes
Reconstruction planning: Helps decide repair vs reconstruction vs arthroplasty
X-rays are primarily to rule out bony avulsion and assess PIP joint congruity. The diagnosis of central slip injury is clinical (Elson test). Do not wait for MRI to start treatment - if Elson test is positive, splint immediately.


Management Algorithm
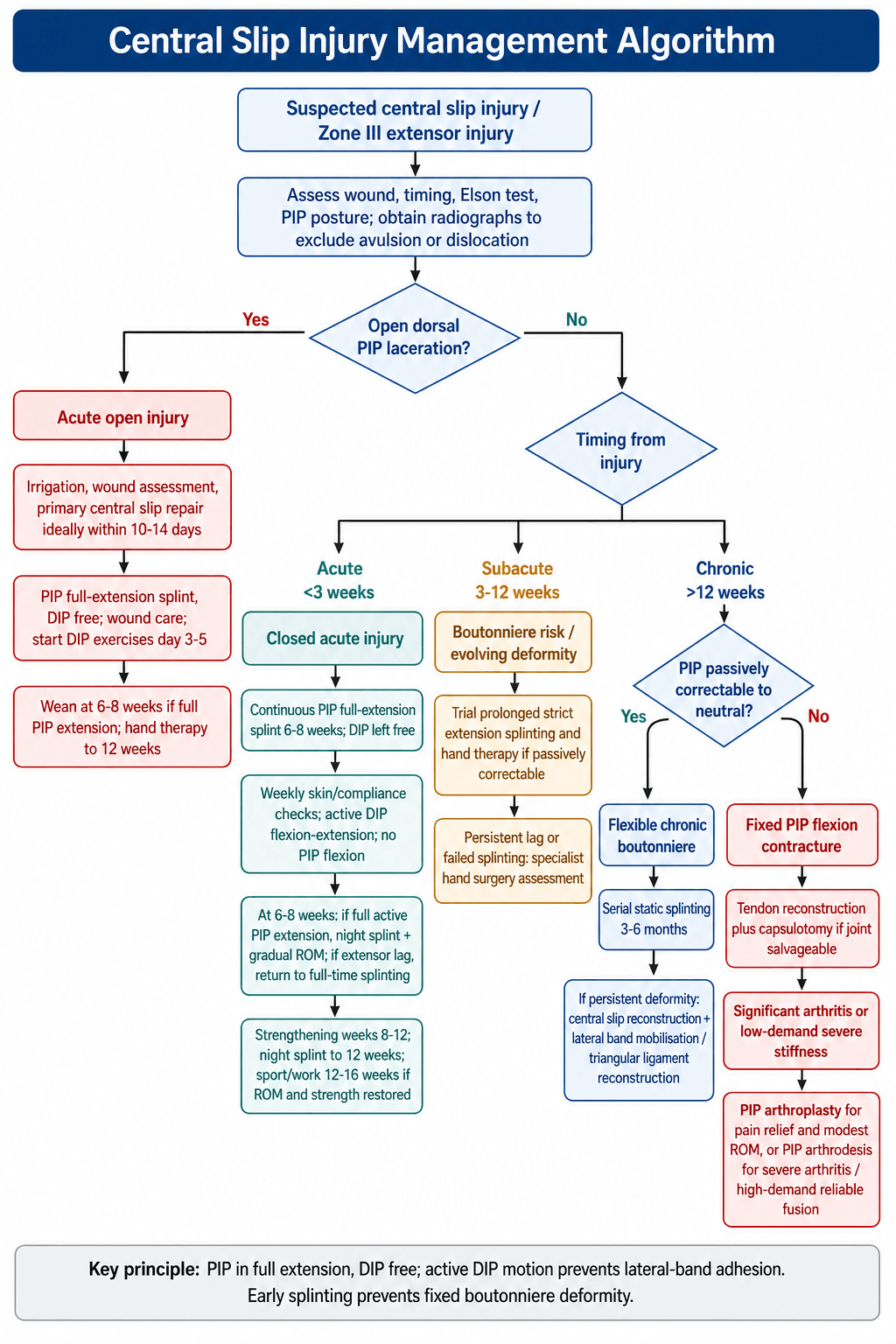
Acute Closed Injury (Under 3 Weeks)
Goal: Prevent boutonniere deformity by maintaining PIP extension while lateral bands remain in anatomic position
Treatment Protocol
Splinting: PIP in full (0 degrees) extension, DIP free
Type: Dorsal aluminum splint, custom thermoplastic, or stack splint
Instructions: Wear continuously, remove only for hygiene under supervision
DIP exercises: Active DIP flexion/extension to prevent lateral band adhesion
Continue: Full-time PIP extension splinting
Check weekly: Skin integrity, compliance, deformity development
DIP ROM: Essential to maintain lateral band excursion
No PIP flexion: Even passive flexion risks lateral band migration
Progressive: Night splinting + gradual PIP ROM exercises
Active extension: Must achieve full PIP extension before weaning
Buddy taping: During daytime activities for protection
Monitor: Any extensor lag = return to full-time splinting
Progressive resistance: Grip strengthening, putty exercises
Night splint: Continue for 12 weeks total
Return to sport: 12-16 weeks if full ROM and strength restored
The key is PIP extension with DIP free. If you immobilize the DIP in extension, the lateral bands will adhere dorsally and lose excursion. Active DIP flexion during PIP extension splinting maintains lateral band mobility and prevents both boutonniere and swan neck deformities.

Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Boutonniere deformity | Near 100 percent if untreated over 6 weeks | Delayed diagnosis, poor compliance | Prevention via early splinting best strategy |
| PIP flexion contracture | 20-30 percent despite treatment | Late presentation, inadequate splinting | Serial splinting or surgical release |
| DIP hyperextension (swan neck) | 10-15 percent in chronic cases | Overcorrection, DIP immobilization during splint | DIP flexion exercises, splint DIP if severe |
| PIP stiffness | Common after surgical repair | Prolonged immobilization, scarring | Early DIP motion, hand therapy at 6 weeks |
| Re-rupture | 5-10 percent after repair | Early return to activity, inadequate splint time | Return to splinting if caught early |
The most important complication to prevent is boutonniere deformity itself. Once established, chronic boutonniere is difficult to correct and often results in permanent functional impairment. The key is high index of suspicion in any PIP injury (perform Elson test) and early splinting (start immediately, continue 6-8 weeks).
Outcomes and Prognosis
| Timing | Treatment | Expected Outcome | Long-term Function |
|---|---|---|---|
| Under 3 weeks (acute) | Extension splinting 6-8 weeks | 90 percent full ROM, rare extensor lag | Excellent return to sport and work |
| 3-12 weeks (subacute) | Prolonged splinting or surgery | 70-80 percent good ROM, mild lag common | Good for daily activities, grip weaker |
| Over 12 weeks (chronic) | Reconstruction or arthroplasty | 50-70 percent useful ROM, variable lag | Functional improvement but rarely normal |
Best prognosis: Acute injury, compliant patient, full-time splinting for 6-8 weeks, early DIP mobilization
Poor prognosis: Delayed diagnosis over 6 weeks, fixed PIP contracture, PIP arthritis on imaging, patient non-compliance
Key threshold: 3 weeks from injury - outcomes decline significantly after this window.
Evidence Base and Key Trials
Rupture of the central slip of the extensor hood: a test for early diagnosis
- Original description of the Elson test for early central slip rupture
- From 90 degrees of PIP flexion over a table edge, the patient extends against resistance
- Absent PIP extension force plus fixed (rigid) DIP extension indicates complete central slip rupture
- Boyes test turns positive only late, once boutonniere deformity is established
Managing swan neck and boutonniere deformities
- Boutonniere arises from loss of coordination between central slip and lateral bands with altered IP joint force balance
- Boutonniere fingers remain functional (PIP flexion and fist preserved); the deformity is largely aesthetic
- Surgical correction must be cautious: gaining PIP extension can impede PIP flexion and worsen function
- Corrective splinting is first line; operative reconstruction is reserved and counselled carefully
Anatomic repair of the central slip with anchor suture augmentation for established boutonniere deformity
- Retrospective series of 13 chronic, supple (Burton stage I) post-traumatic boutonniere deformities
- Direct end-to-end central slip repair augmented with a suture anchor
- Mean PIP extension lag improved from 43.5 degrees by an average of 21.9 degrees
- Excellent or good results in 77 percent (10 of 13); 3 patients had recurrence during ROM exercises
Chronic boutonniere deformity: cross-lateral band technique using palmaris longus autograft
- Seven flexible chronic boutonniere deformities with lateral bands deficient or beyond repair
- Palmaris longus grafts reconstruct both lateral bands, crossing over the middle phalanx
- Mean PIP extension deficit reduced from 54 degrees to 7 degrees
- DIP hyperextension reduced from 9 degrees to 2 degrees with no DIP flexion contracture
Long-term results of extensor tendon repair
- Retrospective review of 101 digits in 62 patients with extensor tendon injury (mostly static splinting)
- Good or excellent results in 64 percent of fingers with no associated injury
- Distal zones (I-IV, including central slip zone III) did significantly worse than proximal zones (V-VIII)
- Loss of flexion was more frequent and greater than loss of extension after repair
Extensor tendon repair (operative technique review)
- Zone III repairs use one to two core sutures plus a running suture; the Elson test should be performed under digital block
- Suture anchors or bone tunnels are used when no distal tendon remains for repair
- Systematic reviews suggest dynamic rehabilitation gives no superior long-term benefit over static splinting
- Running interlocking horizontal mattress repair is stiffer and faster than alternatives
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old basketball player presents 2 days after jamming his left middle finger catching a ball. He has swelling over the PIP joint and difficulty extending the finger. X-rays show no fracture. On examination, he has weak PIP extension and a positive Elson test. What is your diagnosis and management?”
“A 45-year-old presents with chronic PIP flexion deformity of the ring finger following an untreated injury 6 months ago. He has fixed 40-degree PIP flexion contracture and 20-degree DIP hyperextension. PIP can be passively extended to 20 degrees flexion but not neutral. X-rays show early PIP joint space narrowing. How would you manage this?”
“A 35-year-old sustains a 2cm laceration over the dorsum of the PIP joint of his index finger from a kitchen knife. In the emergency department, you can see the central slip is completely divided. The wound is clean and occurred 6 hours ago. How would you manage this?”
MCQ Practice Points
Q: What is the insertion of the central slip of the extensor mechanism? A: Dorsal base of the middle phalanx. The extensor mechanism divides into three slips at the proximal phalanx level: the central slip (middle band) inserts on the middle phalanx base, while the two lateral bands continue distally to form the terminal tendon inserting on the distal phalanx.
Q: What is the Elson test and what does a positive test indicate? A: Elson test diagnoses central slip rupture. The patient's PIP is flexed to 90 degrees over the table edge. The examiner resists attempted PIP extension while palpating the DIP. A positive test shows weak PIP extension force and a floppy DIP (not rigid). This indicates central slip rupture - all extensor force is transmitted through lateral bands to the DIP, bypassing the PIP.
Q: What is a boutonniere deformity and how does it develop? A: Boutonniere deformity is PIP flexion with DIP hyperextension. It develops when the central slip ruptures and the lateral bands gradually migrate volar to the PIP joint axis over 3-6 weeks. Once volar, the lateral bands act as PIP flexors (instead of extensors) and DIP hyperextensors, creating the classic deformity pattern.
Q: What is the splinting protocol for acute central slip injury? A: PIP in full (0 degrees) extension for 6-8 weeks continuously, with DIP free. The key is maintaining PIP extension to prevent lateral band volar migration while allowing DIP flexion exercises to maintain lateral band excursion and prevent adhesion. Splinting both PIP and DIP risks swan neck deformity.
Q: What is the critical time window for preventing boutonniere deformity? A: Within 3 weeks of injury. If extension splinting is started within 3 weeks, 90 percent of patients avoid boutonniere deformity. After 3-6 weeks, the lateral bands have migrated volar and conservative treatment success drops significantly, often requiring surgical reconstruction.
Q: When is surgical reconstruction indicated for boutonniere deformity? A: Chronic fixed deformity over 12 weeks that does not passively correct to neutral. Acute injuries (under 3 weeks) are treated with splinting. Subacute (3-12 weeks) can trial prolonged splinting. Surgery is needed when the PIP has a fixed flexion contracture, requiring capsular release, lateral band relocation, and central slip reconstruction or arthroplasty.
Guidelines, Registries & Global Practice
- Zone III extensor injuries are among the more common extensor tendon injuries seen in hand units worldwide
- Closed central slip rupture typically follows ball-sport jamming, falls, or forced PIP flexion across all regions
- Open lacerations dominate in occupational and assault settings (knife, glass, machinery)
- Volar PIP dislocation is an underrecognised cause and a frequent source of missed diagnosis
- High-resource: certified hand therapists fabricate custom thermoplastic or relative-motion splints with weekly review
- Limited-resource: low-cost aluminium/foam splints and buddy strapping are effective if applied early
- Universal principle: outcome depends far more on prompt diagnosis (Elson test) and splint compliance than on splint cost
- Surgery: chronic reconstruction is concentrated in specialist hand centres globally
| Source | Diagnosis emphasis | Acute treatment | Surgery / reconstruction |
|---|---|---|---|
| ASSH / IFSSH (hand surgery societies) | Elson test, ideally under digital block, on every PIP dorsal injury | Continuous PIP extension splint 6 weeks, DIP free for active flexion | Anatomic repair (suture anchor) for established supple deformity |
| BSSH / BOA (UK) | Clinical diagnosis; X-ray to exclude avulsion, not to confirm | Orthosis-led conservative care via hand therapy; relative-motion splints increasingly used | Reserved for failed conservative care or open injury |
| AAOS / US hand units | High index of suspicion; tenodesis and Elson testing | Static extension splinting; dynamic regimens optional (no proven superiority) | Repair, lateral band relocation, or tendon graft by deformity type |
| AO Foundation | Assess for bony central slip avulsion at middle phalanx base | Splint if soft tissue; ORIF if displaced avulsion involving the joint | Fragment fixation principles for bony avulsions |
There is no dedicated arthroplasty/implant registry for central slip injuries, as most are soft-tissue and treated non-operatively. The evidence base is dominated by small case series and operative-technique reviews rather than randomised trials, so guidance is principle-based: diagnose early, splint the PIP in extension with the DIP free, and reserve surgery for established or open injuries.
Record in every acute PIP injury:
- Elson test performed and its result (positive / negative)
- Splinting instructions given (PIP extension, DIP free, duration 6-8 weeks)
- Patient counselled on boutonniere risk if non-compliant
- Follow-up arranged within one week to assess compliance
A missed central slip diagnosis leading to a fixed boutonniere is a recurring source of complaints and claims worldwide. Always perform and document the Elson test on any PIP dorsal injury, even when the initial X-ray is normal.
Controversies & Areas of Uncertainty
Relative-motion extension orthoses allow early controlled motion and may reduce stiffness, but systematic-review evidence shows no clear long-term superiority over static extension splinting for zone III injuries. Choice is often pragmatic and therapist-led.
Six to eight weeks is conventional, but the precise minimum is not defined by high-quality trials. Most guidance favours at least six weeks of continuous PIP extension, balancing deformity prevention against stiffness from over-immobilisation.
A functional but cosmetically displeasing boutonniere may be best left alone: surgery to gain PIP extension can cost PIP flexion. Reconstruction is offered cautiously, mainly for supple, passively correctable deformities or significant functional limitation.
Anatomic anchor-augmented repair, lateral band relocation, and crossed palmaris longus grafting all report fair-to-good results in small series, with no head-to-head trials. Technique is dictated by tissue quality and surgeon experience rather than firm evidence.
Key Anatomy
- Central slip = middle band of extensor mechanism, inserts dorsal base middle phalanx
- Lateral bands = continue to DIP as terminal tendon
- Central slip rupture allows lateral bands to migrate volar to PIP axis
- Volar lateral bands become PIP flexors and DIP hyperextensors = boutonniere
Diagnosis
- Elson test = pathognomonic (PIP at 90°, weak extension + floppy DIP)
- Acute injury may have near-normal PIP extension (via lateral bands)
- X-ray: check for avulsion fracture middle phalanx base
- High index of suspicion on any PIP dorsal injury or forced flexion mechanism
Treatment Algorithm
- Acute (under 3 weeks) = PIP extension splint 6-8 weeks, DIP free
- Acute open = primary repair + splinting (same duration)
- Subacute (3-12 weeks) = trial prolonged splinting vs surgery
- Chronic fixed (over 12 weeks) = reconstruction or arthroplasty
Splinting Pearls
- PIP in full (0 degrees) extension continuously 6-8 weeks
- DIP must be free - active DIP flexion prevents lateral band adhesion
- Never splint PIP and DIP together (risks swan neck)
- Wean at 6-8 weeks: night splint + gradual ROM, monitor for lag
Complications
- Boutonniere deformity = near 100 percent if untreated over 6 weeks
- PIP flexion contracture = 20-30 percent even with treatment
- Re-rupture = 5-10 percent if return to activity too early
- Stiffness = common after surgery or prolonged immobilization