High Arch | Neurological Etiology | Coleman Block Test | Staged Correction
- Coleman block test differentiates flexible vs fixed hindfoot varus - critical for surgical planning
- Neurological workup essential - CMT, spinal dysraphism, tethered cord must be ruled out
- Plantar-flexed 1st ray is the primary driver - forefoot pronates to get heel to ground
- Conservative management first - orthotics, stretching, observation for mild cases
- Staged surgical correction - soft tissue balancing first, then bony correction if needed
- “Viva question: Walk me through the Coleman block test in a child
- “Always examine for neurological causes - CMT, spinal dysraphism, tethered cord
- “Sequential surgery: plantar fascia release → 1st MT osteotomy → calcaneal osteotomy if needed
- “Complications: overcorrection, growth disturbance, recurrence if underlying cause not addressed
Clinical Imaging
Imaging Atlas

Patient stands on 1-inch block under lateral foot (1st and 2nd rays off edge). If hindfoot corrects to neutral or valgus = flexible (driven by forefoot). If hindfoot stays varus = fixed (needs calcaneal osteotomy). This single test dictates your surgical plan in children.
50-60% of pediatric cavus has neurological cause. CMT, spinal dysraphism, tethered cord, cerebral palsy must be ruled out. Always examine for muscle wasting, check family history, consider nerve conduction studies and spinal MRI if indicated.
Tripod effect: Plantar-flexed 1st metatarsal forces forefoot into pronation to get heel to ground. This creates functional hindfoot varus. Correcting the 1st ray often corrects the hindfoot without calcaneal osteotomy if flexible.
Mild cases: Observation, custom orthotics, stretching. Moderate: Serial casting, AFOs. Severe/Progressive: Staged surgical correction. Never rush to surgery - many children improve with growth and conservative management.
| Clinical Scenario | Coleman Block Result | Primary Management | Key Pearl |
|---|---|---|---|
| Mild cavus, asymptomatic, no progression | N/A - observation | Custom orthotics, stretching, observation | Many children never need surgery |
| Moderate cavus, flexible hindfoot varus, progressive | Hindfoot corrects to neutral on block | Plantar fascia release + 1st MT osteotomy | Forefoot-driven deformity - fix the 1st ray |
| Moderate cavus, fixed hindfoot varus | Hindfoot stays varus on block | Add calcaneal lateralizing osteotomy | Fixed deformity needs bone realignment |
| Severe cavus, neurological cause (CMT), weak peroneals | Fixed hindfoot, weak eversion | Staged: soft tissue first, then calcaneal osteotomy + tendon transfers | Address underlying neurological condition |
CAVECavus Foot Deformity Components - CAVE
Hook:CAVE: The child's foot is stuck in a CAVE - deep arch, toes clawed, heel turned in!
LIFTColeman Block Test Interpretation - LIFT
Hook:LIFT the 1st ray off the block - does the hindfoot LIFT out of varus? If yes = flexible!
NEUROPediatric Cavus Etiology - NEURO
Hook:NEURO workup is essential - don't miss the underlying neurological cause!
Overview and Epidemiology
Pediatric cavus foot is a complex three-dimensional deformity characterized by high medial longitudinal arch (cavus), often with hindfoot varus and forefoot adduction. Unlike adult cavovarus which is predominantly CMT-related, pediatric cavus has a broader differential including idiopathic cases, spinal dysraphism, and other neuromuscular conditions.
Epidemiology:
- Less common than flatfoot in children
- Bilateral in 80% of cases (often asymmetric)
- Idiopathic cases may be familial (autosomal dominant pattern in some families)
- Neurological causes more common in pediatric than adult
- Progressive deformity if untreated
Pediatric cavus foot is often the first sign of an underlying neurological condition. Early recognition allows for appropriate workup and treatment of the underlying cause (CMT, spinal dysraphism, tethered cord). The deformity is progressive and leads to lateral ankle instability, peroneal tendinopathy, metatarsalgia, and stress fractures if untreated. Early intervention prevents severe fixed deformity requiring triple arthrodesis.
Etiology:
- CMT (Charcot-Marie-Tooth): Most common inherited neuropathy, presents in childhood/adolescence
- Spinal dysraphism: Spina bifida, tethered cord, diastematomyelia
- Cerebral palsy: Spastic cavus from muscle imbalance
- Polio residual: Less common now but still seen
- Hereditary motor sensory neuropathies: Various types
- Idiopathic (30-40%): No underlying cause, may be familial
- Post-traumatic (5-10%): Compartment syndrome, malunion
- Arthrogryposis: Multiple joint contractures including foot
- Muscular dystrophy: Duchenne, other types
Natural History:
- Progressive deformity: Worsens over years as muscle imbalance continues
- Lateral ankle instability: Recurrent sprains from varus heel strike
- Metatarsalgia: Plantar-flexed 1st ray and claw toes concentrate pressure
- Stress fractures: Lateral column overload, 5th metatarsal common
- Arthritis: Midfoot and ankle joint degeneration by adulthood if untreated
Pathophysiology and Mechanisms
Pathophysiology of Cavus Deformity
The Tripod Effect:
Plantar-flexed 1st metatarsal is the primary driver:
- Weak peroneus longus (in CMT) or intrinsic muscle imbalance
- 1st ray drops plantar, creating high medial arch
- Forefoot must pronate to get heel to ground
- This creates functional hindfoot varus
Compensatory changes:
- Forefoot pronation to accommodate plantar-flexed 1st ray
- Hindfoot varus (functional initially, becomes fixed)
- Claw toes from flexor overpull and intrinsic weakness
- Tight plantar fascia maintains arch elevation
Muscle Imbalance Patterns:
| Muscle Group | Status | Effect | Clinical Finding |
|---|---|---|---|
| Peroneus brevis | Weak | Cannot evert hindfoot | Hindfoot varus, lateral ankle instability |
| Posterior tibialis | Overactive | Inverts hindfoot | Worsens varus, creates adduction |
| Intrinsic muscles | Weak | Cannot stabilize metatarsals | Claw toes, metatarsalgia |
| Tibialis anterior | Weak (CMT) | Cannot dorsiflex | Foot drop, steppage gait |
Pediatric cavus foot is often the presenting sign of an underlying neurological condition. CMT, spinal dysraphism, and tethered cord can all present with cavus foot. Missing the underlying diagnosis delays appropriate treatment and may allow progression to severe fixed deformity. Always perform a thorough neurological examination and consider imaging if indicated.
Classification Systems
Etiological Classification
| Type | Cause | Clinical Features | Management Approach |
|---|---|---|---|
| Neurological | CMT, spinal dysraphism, CP | Progressive, bilateral, muscle wasting | Address underlying condition, staged correction |
| Idiopathic | Unknown, may be familial | Variable progression, may stabilize | Conservative first, surgery if progressive |
| Post-traumatic | Compartment syndrome, malunion | Unilateral, history of trauma | Correct underlying deformity |
Clinical Assessment
History:
- Age of onset: When was high arch first noticed?
- Progression: Is it getting worse?
- Family history: CMT, other neuropathies, similar foot deformity
- Neurological symptoms: Weakness, numbness, balance problems
- Spinal symptoms: Back pain, bladder/bowel issues (tethered cord)
- Functional limitations: Ankle sprains, metatarsalgia, difficulty with shoes
- Bilateral involvement: 80% bilateral, often asymmetric
- Progressive weakness: Suggests neurological cause
- Family history of CMT: Autosomal dominant inheritance
- Spinal symptoms: Back pain, urinary issues suggest dysraphism
- Unilateral with trauma history: Post-traumatic cause
- Rapid progression: May indicate spinal pathology
Physical Examination:
Systematic Examination
- High medial arch: Elevated longitudinal arch, "peek-a-boo heel" sign (see toes from behind medial ankle)
- Hindfoot varus: Heel turned inward, worse on weight-bearing
- Claw toes: Hyperextension MTP, flexion PIP/DIP
- Muscle wasting: Anterior and lateral compartments (stork leg in CMT)
- Calluses: Under 1st metatarsal head, lateral border of foot
- Compare bilateral: 80% bilateral, assess symmetry
- Plantar fascia: Tight, prominent
- 1st metatarsal head: Plantar-flexed, prominent
- Lateral border: Calluses, stress fracture sites
- Peroneal tendons: May be tender, subluxed, or torn
- Ankle ligaments: ATFL/CFL may be lax from recurrent sprains
- Ankle dorsiflexion: May be limited (equinus component)
- Hindfoot inversion/eversion: Assess strength and flexibility
- Forefoot: Plantar-flexed 1st ray, forefoot pronation
- Toes: Clawing, limited extension at MTP joints
- Coleman block test: CRITICAL - determines flexibility
- Muscle strength: Peroneals, tibialis anterior, posterior tibialis
- Neurological exam: Sensation, reflexes, Babinski
- Gait: Varus heel strike, lateral foot contact, steppage if weak TA
- Spine examination: Look for midline defects, hair tufts, dimples
- Reflexes: May be absent in CMT
- Sensation: Stocking distribution loss in neuropathies
- Upper limbs: CMT may affect hands (intrinsic wasting)
- Family examination: Check parents and siblings for subtle signs
Spinal dysraphism and tethered cord commonly present with cavus foot. In ANY child with cavus foot, especially if progressive or associated with neurological symptoms, you MUST examine the spine for midline defects, hair tufts, dimples, or other stigmata. Consider spinal MRI if any suspicion. Missing tethered cord can lead to permanent neurological damage.
Differential Diagnosis of the High-Arched / Cavus Foot in Children
| Condition | Distinguishing Features | Laterality / Onset | Key Discriminator |
|---|---|---|---|
| Charcot-Marie-Tooth (CMT) | Progressive cavovarus, intrinsic and peroneal wasting, hand involvement, family history | Usually bilateral, adolescent onset | Genetic test (PMP22 duplication in CMT1A), nerve conduction studies |
| Tethered cord / spinal dysraphism | Asymmetric deformity, back/midline stigmata, bladder/bowel symptoms, upper motor neuron signs | Often unilateral or asymmetric, may progress rapidly | Whole-spine MRI |
| Cerebral palsy (spastic) | Spasticity, brisk reflexes, equinocavovarus, birth history | Hemiplegic equals unilateral; diplegic equals bilateral | Upper motor neuron signs, developmental history |
| Residual / treated clubfoot | Forefoot adductus, cavus, hindfoot varus, history of clubfoot correction | Bilateral or unilateral, congenital | History of CTEV and prior casting/surgery |
| Idiopathic / subtle cavus | Mild high arch, neutral or mild varus, normal neurology | Bilateral, may be familial | Normal neurological and spinal examination by exclusion |
| Post-traumatic (compartment syndrome) | Unilateral, intrinsic contracture, history of crush/fracture | Unilateral, acquired | Clear antecedent trauma or compartment syndrome |
A truly unilateral or markedly asymmetric paediatric cavus foot is a red flag for a focal spinal cord lesion (tethered cord, diastematomyelia, intraspinal tumour) rather than CMT, which is typically symmetrical and bilateral. This pattern lowers the threshold for whole-spine MRI substantially.
Investigations
Imaging and Diagnostic Protocol
AP foot: Assess forefoot adduction, metatarsal break pattern, degenerative changes Lateral foot: Calcaneal pitch angle (normal 20 degrees, over 30 degrees = cavus), Meary angle (lateral arch), 1st MT plantar-flexion AP ankle: Assess ankle joint arthritis, talar tilt from chronic instability Hindfoot alignment view (Saltzman): Quantifies hindfoot varus (plumb line medial to heel = varus)
Key measurements:
- Calcaneal pitch greater than 30 degrees = cavus
- Meary angle less than 150 degrees = elevated lateral arch
- Talar-1st MT angle (Meary line) apex plantar = cavus
Key measurements include calcaneal pitch angle (greater than 30 degrees indicates cavus), Meary angle, and talar-1st MT angle. These measurements are essential for surgical planning and monitoring progression.
Nerve conduction studies: Reduced motor and sensory conduction velocities in CMT Type 1 (demyelinating) Electromyography: Denervation pattern in affected muscles Genetic testing: PMP22 duplication for CMT1A (70% of CMT cases) MRI spine: If any suspicion of spinal dysraphism or tethered cord - CRITICAL in pediatric
Assess peroneal tendons: Split tears, subluxation common with varus hindfoot Lateral ligament complex: Chronic ATFL/CFL injury from recurrent sprains Articular cartilage: Ankle joint degenerative changes Soft tissue balance: Plantar fascia, posterior tibial tendon quality
Order spinal MRI in pediatric cavus if: (1) Progressive deformity, (2) Neurological symptoms (weakness, numbness, bladder/bowel), (3) Spinal stigmata on exam (midline defects, hair tufts), (4) Family history negative (rules out CMT), (5) Unilateral or asymmetric. Missing tethered cord or spinal dysraphism has serious consequences.
Management Algorithm
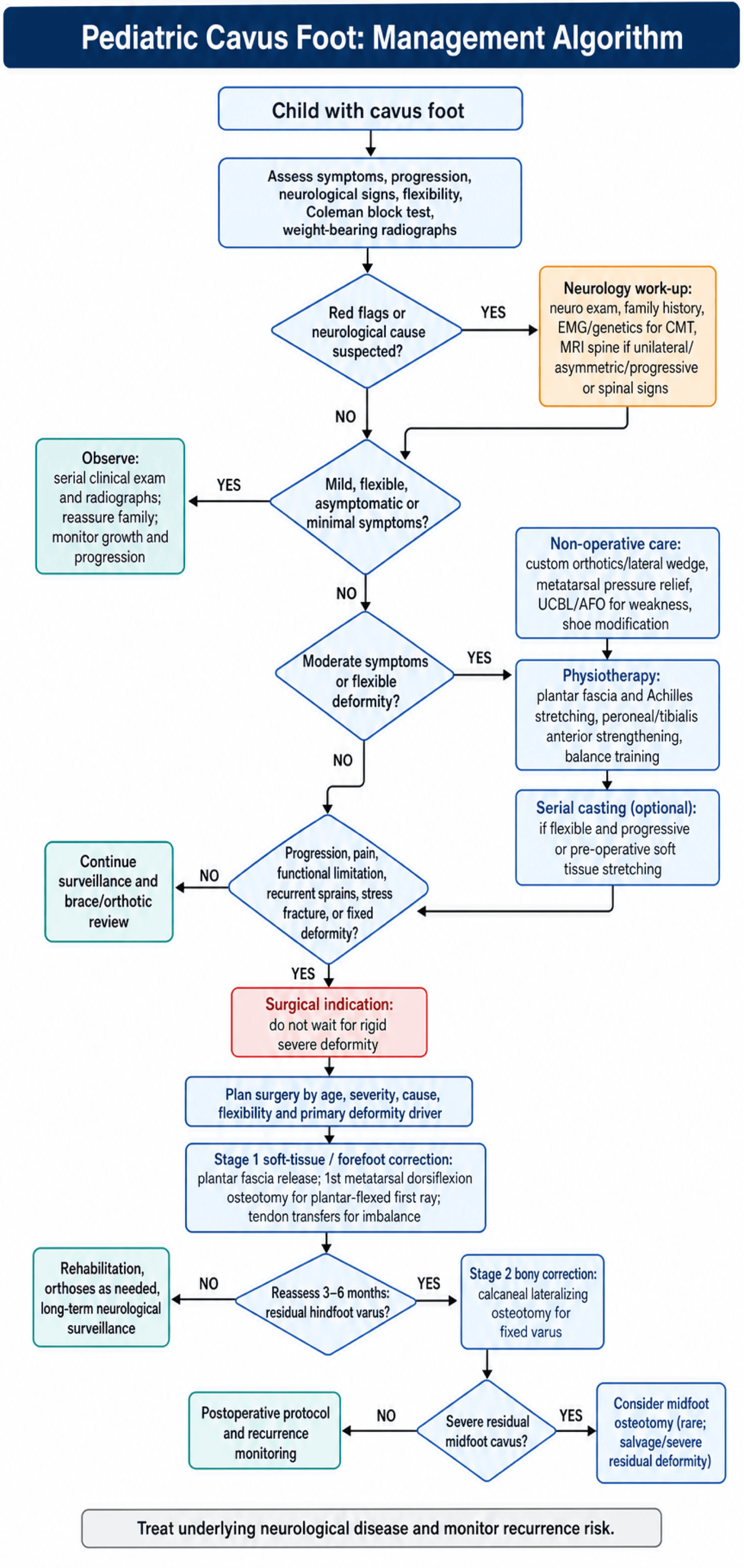
Non-Operative Management (First-Line for Mild Cases)
Many children with mild cavus never need surgery.
Conservative Treatment Protocol
- Asymptomatic mild cavus: Observation only
- Monitor progression: Serial clinical exams and radiographs
- Reassure family: Many cases stabilize or improve with growth
- No intervention needed if no functional limitations
- Custom orthotics: Lateral wedge to accommodate varus, metatarsal pad for pressure relief
- AFOs (ankle-foot orthoses): For weak dorsiflexors, prevent foot drop
- UCBL (University of California Biomechanics Laboratory) inserts: Control hindfoot varus
- Shoe modifications: Lateral heel wedge, rocker bottom
- Plantar fascia stretching: May help mild cases
- Achilles stretching: If equinus component present
- Strengthening: Peroneals, tibialis anterior if weak
- Balance training: Important for neurological causes
- For flexible deformities: May help correct mild cavus
- Not as effective as in clubfoot: Cavus is more rigid
- May be used pre-operatively: To stretch soft tissues
Indications for surgery: (1) Progressive deformity despite conservative management, (2) Pain or functional limitations, (3) Recurrent ankle sprains, (4) Stress fractures, (5) Fixed deformity. Do not delay surgery unnecessarily - fixed deformities are harder to correct.
Surgical Technique
Staged Surgical Correction
Never correct everything at once - staged approach reduces complications.
Stage 1: Soft Tissue Balancing
Technique: Open or endoscopic release of plantar fascia Goal: Drop the arch, reduce cavus Approach: Medial or plantar incision, release central and medial bands Post-op: Weight-bearing in cast for 2-3 weeks
Technique: Dorsal closing wedge osteotomy of 1st metatarsal Goal: Correct plantar-flexed 1st ray (primary deformity driver) Approach: Dorsal approach, preserve growth plate if open Fixation: K-wires or screws depending on age Post-op: Non-weight-bearing 4-6 weeks
Peroneus longus to brevis: If peroneus brevis weak (CMT pattern) Posterior tibial transfer: For severe imbalance (transfer to dorsum) EHL/FHL transfers: For claw toes if severe Timing: May be done with Stage 1 or Stage 2
Stage 2: Bony Correction (If Needed)
Re-evaluate: Clinical exam, radiographs, Coleman block test If hindfoot still varus: Proceed to Stage 2 If corrected: May not need Stage 2
Technique: Lateral closing wedge or lateralizing slide osteotomy Goal: Correct fixed hindfoot varus Approach: Lateral approach, preserve peroneal tendons Fixation: Screws, avoid growth plate if open Post-op: Non-weight-bearing 6-8 weeks
Technique: Cole midfoot dorsal closing wedge osteotomy Goal: Correct severe residual midfoot cavus Indication: Only if significant cavus remains after Stage 1 and 2 Rarely needed: Most cases corrected with Stages 1 and 2
Staged correction allows assessment after each stage. Many patients are corrected with Stage 1 alone (plantar fascia release + 1st MT osteotomy). Only proceed to Stage 2 (calcaneal osteotomy) if hindfoot varus persists. This approach reduces the risk of overcorrection and complications compared to correcting everything at once.
Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Overcorrection to valgus | 5-10% | Aggressive calcaneal osteotomy | Reverse calcaneal osteotomy if severe |
| Recurrence | 10-20% | Underlying cause not addressed, growth | Re-operation, address underlying condition |
| Nonunion | 5-10% | Calcaneal osteotomy, poor fixation | Revision with bone graft |
| Growth disturbance | Rare | Osteotomy through growth plate | Monitor growth, may need epiphysiodesis |
| Peroneal nerve injury | Rare | Lateral approach to calcaneus | Usually resolves, may need exploration |
| Stiffness | 10-15% | Multiple procedures, severe deformity | Aggressive rehabilitation |
Recurrence is common if the underlying neurological cause is not addressed. CMT, spinal dysraphism, and other conditions will continue to cause muscle imbalance. Surgery corrects the deformity but does not treat the underlying condition. Ongoing management of the neurological condition is essential to prevent recurrence.
Postoperative Care and Rehabilitation
Postoperative Protocol
- Cast immobilization: Non-weight-bearing
- Elevation: Reduce swelling
- Pain management: Adequate analgesia
- Wound care: Monitor for infection
- Continue non-weight-bearing: Until radiographic healing
- Gentle ROM: Ankle, subtalar, midfoot (if not fused)
- Wound healing: Monitor incisions
- Radiographs: Check healing at 6 weeks
- Gradual weight-bearing: As tolerated, progress to full
- Physical therapy: Strengthening, stretching, gait training
- Orthotics: May need custom orthotics post-operatively
- Activity modification: Avoid high-impact initially
- Full weight-bearing: Normal gait pattern
- Sport-specific training: If applicable
- Monitor for recurrence: Clinical and radiographic follow-up
- Address underlying condition: Ongoing neurological management
Long-term Follow-up:
- Annual clinical and radiographic assessment
- Monitor for recurrence (especially if underlying cause not addressed)
- Address progression of underlying neurological condition
- May need additional procedures if recurrence occurs
Outcomes
Long-Term Outcomes:
- Good to excellent results in 80-90% with staged correction
- Recurrence more common if underlying neurological cause not addressed
- Staged approach has better outcomes than single-stage correction
- Most children return to normal activities
- May need additional procedures if recurrence occurs
Predictors of Poor Outcome:
- Underlying neurological cause not addressed
- Fixed deformity at presentation
- Overcorrection to valgus
- Nonunion after calcaneal osteotomy
- Growth disturbance
Recurrence occurs in 10-20% of cases, especially if the underlying neurological cause is not managed. CMT and other progressive conditions will continue to cause muscle imbalance. Surgery corrects the deformity but does not treat the underlying condition. Ongoing neurological management and monitoring are essential.
Evidence Base
A Simple Test for Hindfoot Flexibility in the Cavovarus Foot (Coleman Block Test)
- Original description of the lateral-block (Coleman) test for the cavovarus foot
- Placing the heel and lateral border on a block while the first ray hangs free unloads the plantar-flexed first ray
- Hindfoot correction on the block indicates a forefoot-driven, flexible varus
- Persistent hindfoot varus on the block indicates a fixed (structural) hindfoot deformity
Cavus Foot Deformity in Children
- Authoritative AAOS review of paediatric cavus foot evaluation and treatment
- Cavovarus is the commonest pattern; CMT is the most frequent progressive cause, with cerebral palsy and poliomyelitis among non-progressive causes
- Deformity begins flexible and becomes a fixed bony deformity if untreated
- Triple arthrodesis has poor long-term results in progressive deformity with sensory impairment
Is a Plantarflexed First Ray the Primary Deformity in Children with CMT Cavovarus Feet? A Pedobarographic Analysis
- 118 feet from 60 children with CMT analysed with dynamic pedobarography
- First-ray contact preceded fifth-ray contact in only 39.7% of varus feet versus 34.0% of non-varus feet (P=0.526)
- About 60% of varus feet landed in varus before first-ray contact, suggesting the foot is pre-positioned in varus
- Challenges the assumption that a plantar-flexed first ray is the sole primary driver in all CMT feet
Is Non-operative Management of Childhood Neurologic Cavovarus Foot Effective?
- 23 children (35 feet) with neurologic cavovarus treated with an untwisting nocturnal splint, with an untwisting walking cast in some
- Good or very good clinical results in 23 of 35 feet (65%) at mean 4.5-year follow-up
- Of feet followed to skeletal maturity, about half (10 of 21) achieved good or very good results without surgery; no triple arthrodeses were required
- Young age at initiation and poor splint compliance predicted worse outcomes
Talocalcaneonavicular Realignment for Severe Resistant Neurologic Cavovarus and Equinocavovarus in Children
- Prospective cohort of 26 patients (36 feet); 54% cerebral palsy, 23% CMT; median age 12.1 years
- Significant improvement in talocalcaneal, talus-first metatarsal and talonavicular coverage angles and in functional scores (P<0.01)
- Median follow-up 32.9 months with only 3 minor complications (hypersensitivity, partial recurrence, undercorrection)
- Subtalar (talocalcaneonavicular) realignment is the foundational step in comprehensive multi-segmental reconstruction
Treatment of the Cavus Foot in the Paediatric Patient with Charcot-Marie-Tooth
- Over half of patients with CMT develop foot and ankle problems, of which cavovarus is by far the commonest
- Deformity arises from imbalance between peroneus longus and tibialis anterior, and between tibialis posterior and peroneus brevis
- Early soft-tissue procedures and osteotomies in the flexible foot can restore posture and delay bony salvage
- Triple arthrodesis is a salvage option for severely rigid feet, and deformity may progress despite surgery
Malalignment and Lateral Ankle Instability in the Cavovarus Foot
- Hindfoot and tibial varus malalignment is an underestimated cause of chronic lateral ankle instability and later ankle arthritis
- A high index of suspicion for varus malalignment is required when assessing recurrent ankle instability
- Management should include a generous indication for accurate hindfoot realignment
- In young, active patients realignment should be combined with formal lateral ligament repair
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 10-year-old boy presents with bilateral high arches. His parents noticed the arches getting higher over the past year. He has had several ankle sprains.”
“A 14-year-old girl with CMT has progressive bilateral cavovarus feet. The Coleman block test shows the hindfoot corrects to neutral on the right but stays varus on the left.”
“A 12-year-old boy had a calcaneal lateralizing osteotomy for cavovarus foot 6 months ago. He now presents with a valgus hindfoot and lateral ankle pain.”
MCQ Practice Points
Q: What does the Coleman block test determine in cavus foot? A: The Coleman block test determines if hindfoot varus is flexible (forefoot-driven) or fixed. Patient stands on 1-inch block under lateral foot with 1st and 2nd rays off. If hindfoot corrects to neutral = flexible, 1st MT osteotomy may suffice. If stays varus = fixed, needs calcaneal osteotomy.
Q: What is the most common neurological cause of pediatric cavus foot? A: Charcot-Marie-Tooth (CMT) disease is the most common neurological cause. CMT is an inherited motor and sensory neuropathy that causes progressive muscle weakness and imbalance, leading to cavovarus foot deformity. Always consider CMT in pediatric cavus, especially if bilateral and progressive.
Q: What is the recommended surgical approach for pediatric cavus foot? A: Staged correction is preferred. Stage 1: Plantar fascia release + 1st metatarsal dorsiflexion osteotomy. Reassess after 3-6 months. Stage 2: Calcaneal lateralizing osteotomy only if hindfoot varus persists. Staged approach has better outcomes and lower complication rates than single-stage correction.
Q: What is the primary driver of cavus foot deformity? A: Plantar-flexed 1st metatarsal is the primary driver. The tripod effect: plantar-flexed 1st ray forces forefoot to pronate to get heel to ground, creating functional hindfoot varus. Correcting the 1st ray often corrects the hindfoot without calcaneal osteotomy if flexible.
Q: When should you order spinal MRI in pediatric cavus foot? A: Order spinal MRI if: progressive deformity, neurological symptoms (weakness, numbness, bladder/bowel), spinal stigmata on exam (midline defects, hair tufts), negative family history (rules out CMT), or unilateral/asymmetric presentation. Missing tethered cord or spinal dysraphism has serious consequences.
Q: What is the recurrence rate after cavus foot correction? A: 10-20% recurrence rate, especially if underlying neurological cause is not addressed. CMT and other progressive conditions continue to cause muscle imbalance. Surgery corrects the deformity but does not treat the underlying condition. Ongoing neurological management is essential.
Guidelines, Registries & Global Practice
Global epidemiology. Charcot-Marie-Tooth disease is the most common inherited peripheral neuropathy, with population prevalence generally cited around 1 in 2,500, and CMT1A (PMP22 duplication) accounting for the majority of demyelinating cases. Because over half of children with CMT develop foot and ankle problems, of which cavovarus is by far the commonest pattern, cavovarus foot is a near-universal management consideration in paediatric neuromuscular clinics worldwide (Olney, Foot Ankle Clin 2000, PMID 11232232; Schwend & Drennan, J Am Acad Orthop Surg 2003, PMID 12828450). In a paediatric population, neurological causes (CMT, spinal dysraphism, cerebral palsy, residual polio in low-income settings) predominate over the idiopathic cavus that is relatively more common in adults.
Side-by-side guidance and consensus across regions. There is no single high-level (RCT-based) international guideline that dictates operative thresholds for paediatric cavovarus; practice is built on instructional reviews, expert consensus and observational cohorts. The convergent principles below are drawn from the verified evidence base.
| Body / Source | Region | Position | Evidence Level |
|---|---|---|---|
| AAOS instructional review (Schwend & Drennan) | North America | Neurological assessment directs treatment; preserve a plantigrade mobile motor-balanced foot; favour soft-tissue release and osteotomy over arthrodesis; reserve triple arthrodesis as salvage | Level 5 (expert review) |
| Coleman & Chesnut block-test principle | International (foundational) | Flexible hindfoot varus = forefoot/soft-tissue surgery; fixed varus = calcaneal osteotomy | Level 5 (foundational technique) |
| European paediatric foot units (e.g. French untwisting-brace protocol) | Europe | Early bracing once progression detected can avoid or delay surgery to a single procedure near maturity | Level 4 (cohort) |
| BOA / BSCOS practice (UK) | UK | Multidisciplinary paediatric orthopaedic and neurology pathway; whole-spine MRI for asymmetric or atypical cavus; staged joint-preserving correction | Consensus / pathway |
| EFORT / European paediatric orthopaedic consensus | Europe | Joint-preserving, deformity-specific reconstruction preferred over early arthrodesis in the growing foot | Consensus / review |
- No dedicated international paediatric cavovarus registry exists; evidence is from single-centre prospective and retrospective cohorts
- Prospective cohort data support joint-preserving subtalar (talocalcaneonavicular) realignment for severe resistant deformity with low complication rates (PMID 39382214)
- Dynamic pedobarography cohorts question the universal "forefoot-driven" model, favouring force-rebalancing strategies (PMID 39132914)
- National CMT patient registries (e.g. INC/RDCRN, European CMT networks) capture natural history but not foot-surgery outcomes specifically
- Bracing-first vs early-surgery thresholds vary markedly between European and North American centres
- Use of single-stage vs staged reconstruction varies with surgeon preference and deformity rigidity
- In low-resource settings residual poliomyelitis remains a relevant cause; access to genetic testing and MRI is uneven globally
- Universal agreement on two points: exclude a neurological cause, and use the Coleman block test to guide hindfoot surgery
Key documentation points:
- Thorough neurological examination performed (including upper limbs and reflexes)
- Coleman block test result documented (flexible vs fixed)
- Discussion of underlying causes (CMT, spinal pathology, cerebral palsy)
- Spinal examination findings (midline defects, hair tufts, dimples)
- Indication for and result of whole-spine MRI if ordered
- Discussion of recurrence risk if the underlying cause is not addressed
Don't Miss Spinal Pathology: Missing tethered cord or spinal dysraphism in a child with cavus foot is a serious clinical error. Always document the spinal examination and the reasoning for or against whole-spine MRI, particularly for any unilateral or asymmetric deformity.
Key Pathophysiology
- 50-60% neurological cause - CMT most common
- Plantar-flexed 1st ray = primary deformity driver
- Tripod effect: 1st MT too low → forefoot pronates → hindfoot varus
- Coleman block test = gold standard for flexibility
Clinical Assessment
- Coleman block test: Stand on 1-inch block under lateral foot - does hindfoot correct?
- Neurological exam: Muscle strength, reflexes, sensation, spine examination
- Muscle wasting: Anterior/lateral compartments (stork leg in CMT)
- Calcaneal pitch angle: greater than 30 degrees = cavus (normal 20 degrees)
Etiology Workup
- CMT: Family history, nerve conduction studies, genetic testing
- Spinal dysraphism: Spine exam, spinal MRI if any suspicion
- Tethered cord: Progressive deformity, bladder/bowel symptoms, spinal MRI
- Idiopathic: No underlying cause, may be familial
Surgical Algorithm
- Flexible hindfoot (Coleman negative): Plantar fascia release + 1st MT osteotomy
- Fixed hindfoot (Coleman positive): Add calcaneal lateralizing osteotomy
- Staged approach: Stage 1 first, reassess, Stage 2 if needed
- Never do everything at once - high complication rate
Complications
- Overcorrection to valgus: 5-10% incidence
- Recurrence: 10-20% if underlying cause not addressed
- Nonunion: 5-10% after calcaneal osteotomy
- Growth disturbance: Rare, avoid osteotomy through growth plate