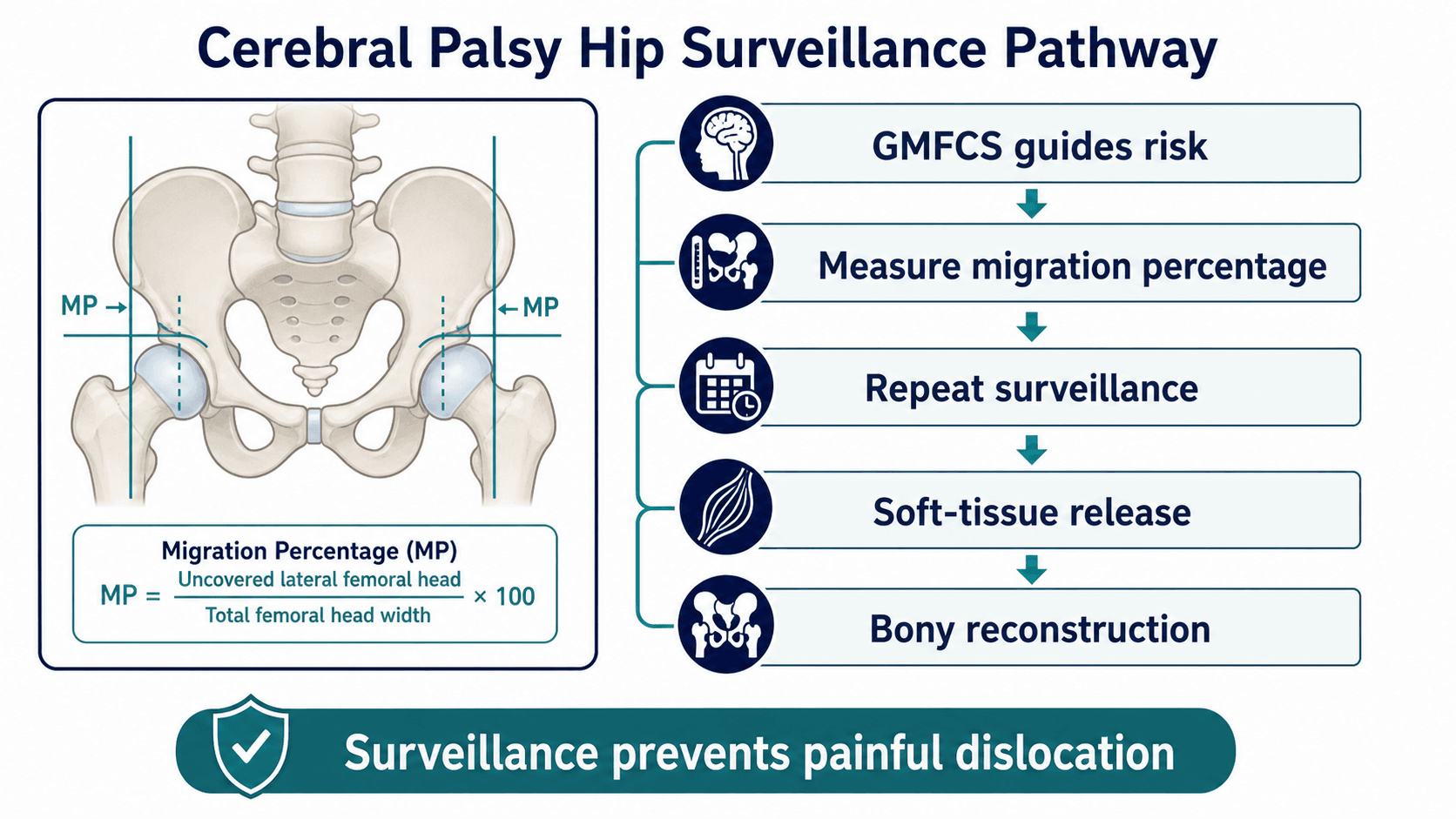
GMFCS risk, migration percentage and prevention of painful dislocation
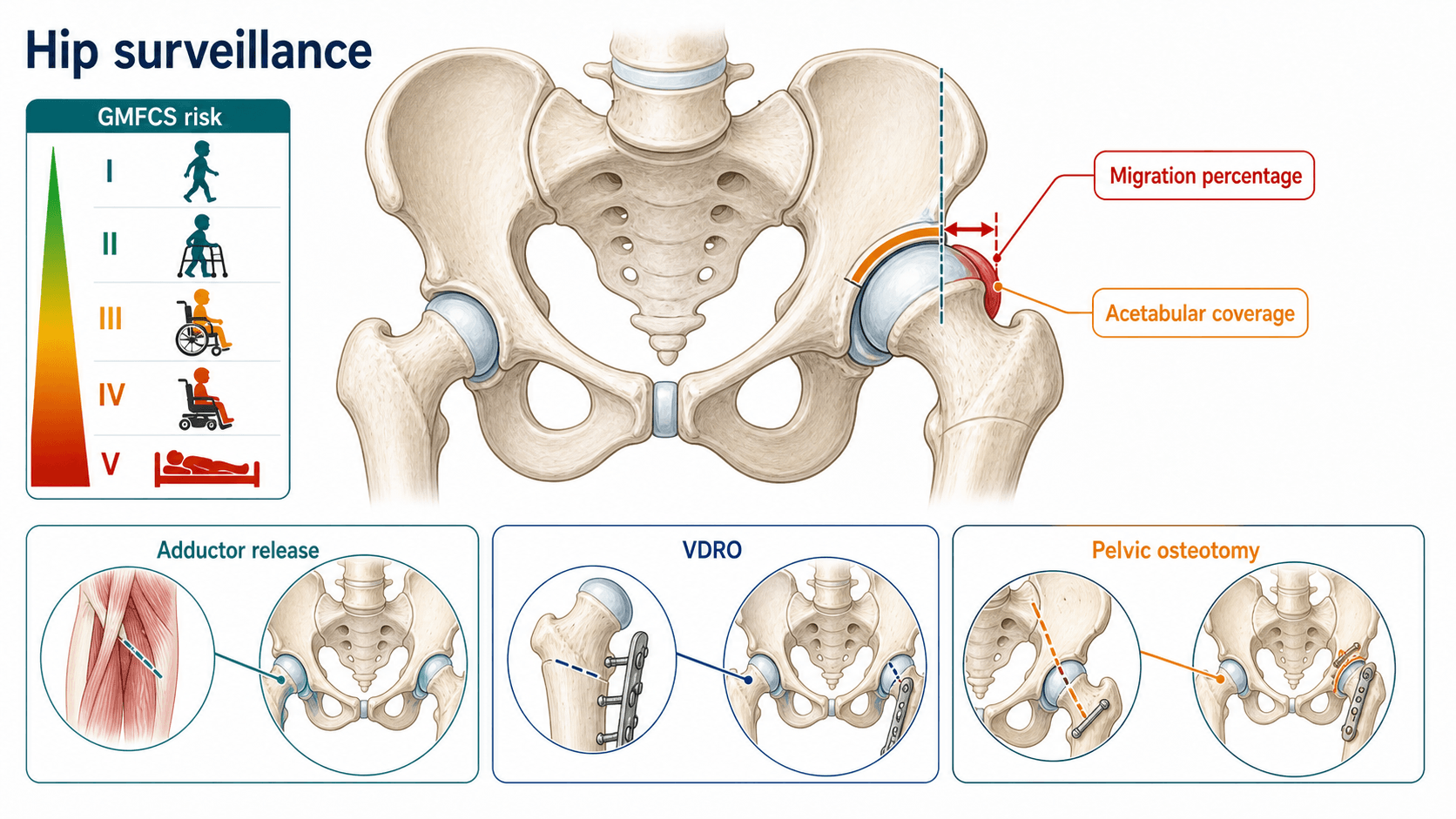
- Hip displacement risk rises with increasing GMFCS level, especially GMFCS IV and V.
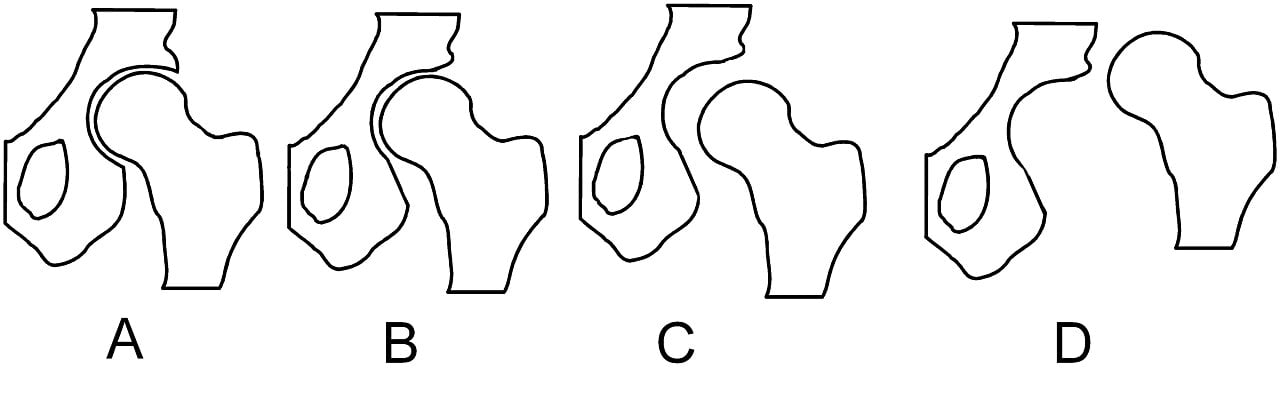
- Reimers migration percentage measures the proportion of femoral head lateral to the acetabular reference line.
- Most surveillance pathways recommend referral when migration percentage is over 30 percent or hip abduction is less than 30 degrees.
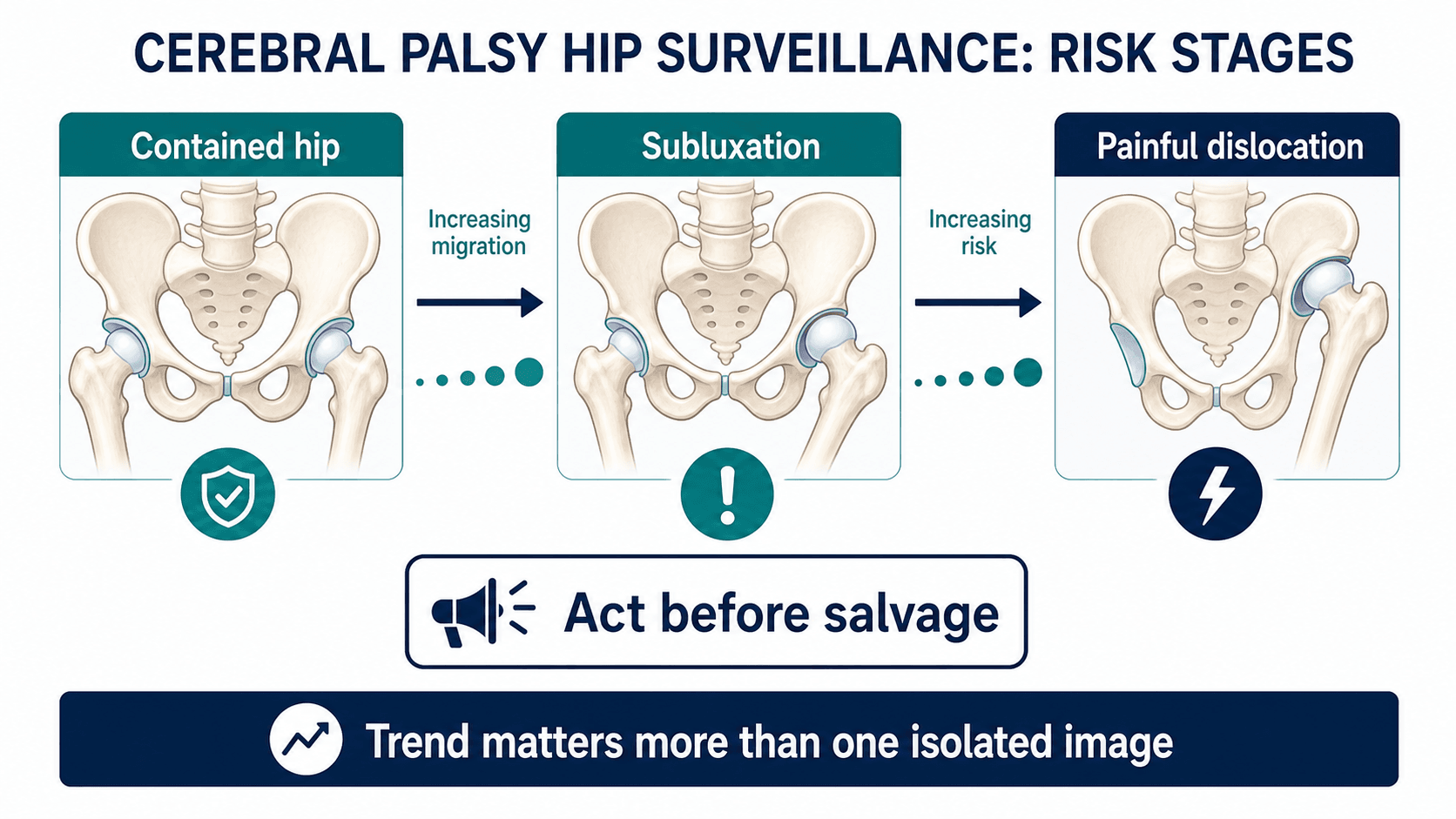
- Early migration may be painless; waiting for pain misses the prevention window.
- Care symptoms such as difficult hygiene, dressing, sitting and transfers are hip symptoms in severe cerebral palsy.
- Treatment ranges from surveillance and tone management to adductor-psoas release, VDRO, pelvic osteotomy and salvage care.
- “Confirm or assign GMFCS from real-world mobility; do not simply ask a family to provide a classification.
- “Clinical abduction does not replace radiographic migration percentage.
- “The question is not just whether the hip hurts; it is whether sitting, sleep, transfers and hygiene are becoming difficult.
- “The painful chronically dislocated CP hip is much harder than preventable subluxation.
A CP hip can migrate substantially before the child has clear hip pain. Surveillance should be scheduled by risk and migration trend, not triggered only by symptoms.
Images and Diagrams
| Question | Answer | Clinical use |
|---|---|---|
| Who is highest risk? | Children with higher GMFCS levels, especially IV and V. | Set surveillance intensity. |
| What is the key radiographic measure? | Reimers migration percentage. | Quantifies lateral femoral-head displacement and trend. |
| What clinical change matters? | Reduced abduction, difficult hygiene, sitting problems, pain or windswept posture. | Triggers earlier review. |
| What is the goal? | Comfortable located hips that support sitting, hygiene, sleep and care. | Keeps treatment patient-centred. |
HIPSSurveillance Priorities
Hook:HIPS keeps surveillance focused on risk, imaging, migration and function.
CAREClinical History
Hook:CARE reminds the reader that carers often notice function before pain.
VDROReconstruction Logic
Hook:VDRO keeps reconstruction tied to containment and pelvic balance.
Overview/Epidemiology
Hip displacement is a predictable musculoskeletal complication of cerebral palsy, especially in children with limited ambulatory function. The hip may migrate laterally before pain is obvious. Once a hip becomes chronically dislocated, stiff and painful, treatment becomes more complex and often shifts from prevention to salvage.
Hip surveillance exists to prevent that pathway. It identifies children at risk, obtains AP pelvis radiographs at scheduled intervals, measures Reimers migration percentage and escalates care when the hip is migrating or symptoms develop. The program is not simply a radiograph schedule; it is a coordinated assessment of mobility, tone, hip motion, pelvis, spine, seating, hygiene and family goals.
The guiding principles are:
- Higher GMFCS level means higher displacement risk.
- Migration percentage trend is more useful than a single number in isolation.
- Loss of abduction and care difficulty are meaningful clinical changes.
- Hip and spine problems interact through pelvic obliquity and windswept posture.
- Early prevention is preferable to late salvage.
Pathophysiology
Hip displacement in cerebral palsy is driven by muscle imbalance, spasticity, weakness, abnormal posture and growth. Adductors and hip flexors tend to pull the femoral head laterally and superiorly. Coxa valga, excessive femoral anteversion and acetabular dysplasia reduce containment. Non-ambulant children have less protective loading and less active muscle balance around the hip.
As the femoral head migrates, acetabular development worsens. The acetabulum no longer sees a centred femoral head, so dysplasia can progress. Pelvic obliquity, scoliosis and windswept posture can then magnify asymmetry. A hip that began as a painless radiographic migration may become a painful stiff dislocation that affects sleep, sitting, hygiene and transfers.
Migration percentage is not just a radiographic number. It is a marker of loss of containment, worsening acetabular development and increasing risk of future pain.
Classification
- GMFCS I-II: lower risk, but still clinically assessed.
- GMFCS III: intermediate risk; surveillance depends on program and migration trend.
- GMFCS IV-V: highest risk; regular AP pelvis surveillance is essential.
- Growth velocity and age modify progression risk.
Clinical Presentation
History
Do not ask only "does the hip hurt?" A non-verbal or medically complex child may show hip problems through care difficulty, sleep disturbance, irritability or seating intolerance. Confirm or assign GMFCS level from real-world mobility: independent walking, walking with aids, wheelchair use, self-mobility and transfer function.
Ask about:
- Pain during dressing, nappy changes, toileting, transfers or physiotherapy.
- Sitting tolerance, pelvic obliquity, wheelchair fit and equipment problems.
- Sleep disturbance, rest pain or irritability.
- Hygiene difficulty and perineal care.
- Standing frame tolerance and ability to weight bear.
- Previous botulinum toxin, adductor releases, hip surgery or spine surgery.
- Feeding, nutrition, respiratory status, seizures and bone health.
- Family priorities: comfort, sitting, sleep, hygiene and ease of care.
Examination
Examine both hips and the whole sitting unit: pelvis, spine, hips, knees and feet. Measure hip abduction with hips flexed and extended. Assess adductor tone, psoas tightness, hamstring tightness, flexion contracture, pelvic obliquity, scoliosis and windswept posture. Look for pain with gentle range of motion and document skin pressure risk.
In severe cerebral palsy, difficult hygiene, seating intolerance and pain during transfers are hip symptoms even when the child cannot localise pain.
Investigations
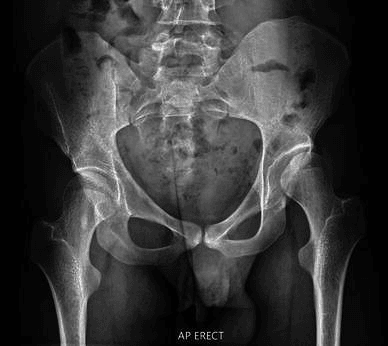
AP pelvis
The core investigation is a standardised AP pelvis radiograph. Positioning should be as consistent as possible, because pelvic rotation and abduction can affect measurement. Measure both hips and record migration percentage. Compare with previous images; trend is central.
Reimers migration percentage
Migration percentage is the proportion of the femoral head lateral to the acetabular reference line. It is calculated as lateral uncovered head width divided by total femoral head width, multiplied by 100. It should be recorded consistently and used with the child's age, GMFCS level, hip abduction and symptoms.
| Step | Measurement action | Practical point |
|---|---|---|
| 1 | Use a standardised supine AP pelvis with femurs neutral. | Adduction can overestimate migration and abduction can underestimate it. |
| 2 | Draw Hilgenreiner line through the triradiate cartilages, or through the teardrops after maturity. | A consistent horizontal reference is needed before Perkin line is drawn. |
| 3 | Draw Perkin line perpendicular to Hilgenreiner line at the lateral acetabular edge. | This defines the lateral acetabular coverage boundary. |
| 4 | Measure the uncovered lateral femoral head and divide by total ossified femoral-head width. | Migration percentage equals uncovered width divided by total width, multiplied by 100. |
| 5 | Compare with the previous radiograph. | Trend and rate of change are more useful than a single number alone. |
Additional imaging
Spine imaging may be needed when scoliosis and pelvic obliquity affect sitting and hip position. CT or additional imaging is selective and usually reserved for complex reconstructive or salvage planning.
| Question | Investigation | Decision it informs |
|---|---|---|
| What is the baseline risk? | GMFCS plus clinical examination | Sets surveillance intensity. |
| Is the hip migrating? | AP pelvis and Reimers migration percentage | Defines displacement and trend. |
| Does clinical function match the X-ray? | Care, sitting, hygiene, sleep and abduction assessment | Guides urgency and goals. |
| Are pelvis and spine influencing the hip? | Spine and pelvis imaging when indicated | Coordinates hip and spine strategy. |
| Is salvage or complex reconstruction being planned? | Selective CT or additional imaging | Clarifies anatomy. |
Differential Diagnosis
Pain or care difficulty in a child with cerebral palsy is not always the hip. The non-verbal child cannot localise the problem, so the clinician must actively exclude common mimics before attributing distress to hip displacement. Migration percentage anchors the assessment, but a high migration percentage does not prove that the hip is the source of a new symptom.
| Cause | Discriminating features | Confirmatory step |
|---|---|---|
| Hip displacement or dislocation | Reduced abduction, pain on hip rotation, rising migration percentage, windswept posture. | AP pelvis with migration percentage and trend. |
| Spastic adductor contracture without subluxation | Tight adductors and reduced abduction but contained hip on radiograph. | Normal migration percentage on standardised AP pelvis. |
| Occult fragility fracture | Sudden pain, swelling or warmth in an osteopenic non-ambulant child, often after minor handling. | Targeted radiograph of the painful segment; consider bone-health review. |
| Septic arthritis or osteomyelitis | Fever, systemic upset, severe rest pain, raised inflammatory markers. | Bloods, ultrasound or aspiration; do not assume mechanical hip. |
| Abdominal or visceral cause | Constipation, reflux, urinary infection, gastrostomy or shunt problems. | Abdominal and systemic examination, urinalysis, relevant imaging. |
| Spine, pelvic obliquity or scoliosis | Trunk or back pain, deteriorating sitting balance, asymmetric pressure. | Spine and pelvis assessment and imaging when indicated. |
| Seating, pressure or equipment problem | Skin breakdown, new wheelchair or orthosis, pain only when seated. | Pressure-area check and seating review with the therapy team. |
| Hardware irritation after prior surgery | Localised tenderness over plate or screws, often late after VDRO. | Radiograph and clinical correlation; consider removal if symptomatic. |
The practical rule: in a distressed non-verbal child, examine the hip, the spine, the abdomen and the skin before concluding the hip is to blame, and confirm the hip hypothesis with a standardised migration percentage rather than examination alone.
Management
| Finding | Usual interpretation | Management direction |
|---|---|---|
| Migration percentage under 30 percent and stable | Contained hip or low current displacement risk. | Continue surveillance according to GMFCS level, age and local pathway. |
| Migration percentage over 30 percent or abduction less than 30 degrees | Hip at risk or clinically tightening hip. | Refer to paediatric orthopaedics and intensify surveillance. |
| Migration percentage around 40 percent or rising quickly | Progressive displacement is likely, especially in GMFCS IV-V. | Assess for soft-tissue release versus reconstructive containment depending age, abduction and acetabular shape. |
| Persistent subluxation with coxa valga, anteversion or acetabular dysplasia | Soft-tissue treatment alone is unlikely to contain the hip. | Plan VDRO, usually with pelvic osteotomy when acetabular deficiency is established. |
| Painful chronic dislocation | Prevention window has passed for that hip. | Prioritise comfort, sitting, hygiene, sleep and salvage options rather than radiographic perfection. |
Surveillance starts by confirming or assigning GMFCS level, measuring hip abduction and obtaining AP pelvis radiographs according to risk. Record migration percentage and trend. Escalate review for migration percentage over 30 percent, rising migration trend, abduction less than 30 degrees, pain, difficult care or pelvic imbalance, using local program thresholds.
Complications
Missed or delayed surveillance
- Silent migration progresses to fixed subluxation or dislocation.
- Acetabular dysplasia becomes harder to reconstruct.
- Pain, sleep disturbance and hygiene difficulty become established.
Surgical and postoperative complications
- Wound problems or infection.
- Respiratory, nutrition or medical complications in medically complex children.
- Cast, brace or positioning difficulty.
- Loss of reduction or recurrent subluxation.
- Avascular necrosis, stiffness or heterotopic ossification.
- Hardware pain or need for removal.
Long-term problems
- Painful chronic dislocation.
- Pelvic obliquity and scoliosis interaction.
- Recurrent displacement.
- Persistent care difficulty despite radiographic improvement.
The best CP hip intervention is often the one timed before the hip becomes painful, stiff and unreconstructable.
Decision-Making in Practice
Hip surveillance in cerebral palsy is a prevention pathway. The aim is to identify progressive migration early enough that soft-tissue balancing, bony containment surgery or salvage decisions can be made before the hip becomes painful, fixed or unreconstructable.
| Decision | How to decide | Management consequence |
|---|---|---|
| Surveillance intensity | GMFCS level, age, migration percentage, rate of change and clinical hip abduction | Higher-risk children need more frequent radiographs and earlier escalation |
| Observe or refer | Stable low migration with good abduction versus rising migration or symptoms | Rising migration should not wait for pain |
| Soft-tissue surgery | Younger child with adductor or psoas tightness and early displacement | May slow progression but requires radiographic follow-up |
| Reconstructive surgery | Established subluxation, acetabular dysplasia, coxa valga, excessive femoral anteversion or progressive migration | Often requires VDRO with or without pelvic osteotomy |
| Salvage pathway | Painful chronic dislocation, severe deformity, poor reconstruction potential or medically fragile child | Goals shift to pain relief, sitting, hygiene and care |
The examination must be linked to the radiograph. Hip abduction, pain with movement, pelvic obliquity, sitting tolerance, hygiene, sleep and transfers matter because the purpose of treatment is not a number on an X-ray; it is a painless, mobile, careable hip. The migration percentage remains the central surveillance measure, but treatment is chosen by combining migration, acetabular development, femoral head shape, femoral anteversion, neck-shaft angle, muscle balance and child-specific goals.
A useful treatment sequence is: identify risk by GMFCS, measure migration reliably, watch the rate of change, preserve abduction, contain the hip before fixed dislocation, and follow long enough to detect recurrence. A child whose migration percentage continues to rise after soft-tissue surgery needs reassessment for bony reconstruction rather than repeated isolated releases.
Guidelines, Registries & Global Practice
Hip surveillance is one of the clearest examples in paediatric orthopaedics where coordinated programmes change outcomes at a population level. The principles are remarkably consistent worldwide: stratify by GMFCS, measure migration percentage on a standardised AP pelvis, and act on trend before pain. The differences lie in thresholds, schedules and access.
Global epidemiology
- Cerebral palsy affects roughly 2 per 1000 live births and is the commonest cause of childhood physical disability worldwide.
- Hip displacement is the second most common musculoskeletal deformity in cerebral palsy after equinus.
- Displacement risk tracks GMFCS almost linearly: close to 0 percent at GMFCS I rising to around 60 to 90 percent at GMFCS V across population cohorts.
- CP subtype matters: near 0 percent risk in pure ataxia versus up to about 79 percent in spastic tetraplegia.
- Without surveillance, late painful dislocation historically affected a meaningful minority of non-ambulant children; structured programmes reduce dislocation to around or below 0.5 percent.
Side-by-side guidance
| Source | Core trigger to refer or act | Emphasis |
|---|---|---|
| AACPDM care pathway (international) | Migration percentage over 30 percent or hip abduction under 30 degrees. | Evidence-graded pathway tying schedule to GMFCS, age and migration percentage. |
| Australian Standards of Care (Wynter et al.) | GMFCS-stratified radiograph schedule with defined start, frequency and discharge. | Consensus template widely adopted for programme design. |
| CPUP / CPIP registry models (Sweden, UK, others) | Risk scoring combining age, GMFCS, head-shaft angle and migration percentage. | Registry-driven, predictive and auditable. |
| BOA / paediatric society guidance (UK) | Programmatic referral on rising migration percentage in non-ambulant children. | Embedding surveillance into routine CP care pathways. |
| AO and reconstructive principles | Bony reconstruction when soft-tissue surgery cannot contain the hip. | Operative containment: VDRO with pelvic osteotomy when acetabular deficiency is established. |
Registries and programmatic data
- CPUP (Sweden) and CPIP (United Kingdom, Scotland and others) are the model national registries, providing the strongest population evidence that surveillance prevents dislocation.
- Registry data underpin risk tools such as the CPUP Hip Score and allow external validation across countries.
- Common themes: standardised migration percentage measurement, GMFCS-linked schedules and prospective audit of dislocation rates.
High- versus limited-resource practice
- High-resource settings: universal registries, scheduled radiographs from age 1 to 2 years, multidisciplinary clinics and timely preventive surgery.
- Limited-resource settings: surveillance may be opportunistic, presentation is often late with established painful dislocation, and salvage rather than prevention may dominate.
- A pragmatic minimum anywhere is to identify GMFCS IV and V children, obtain a baseline AP pelvis, and arrange repeat imaging on any rising migration percentage even when a formal registry is unavailable.
Whatever the country, the examinable principle is identical: GMFCS-based risk, standardised migration percentage and action on trend before pain. Programme details vary; the surveillance logic does not.
Controversies and Areas of Uncertainty
Hip surveillance is well established, but several practical questions remain genuinely contested and are good viva discriminators.
- Exact referral threshold. Migration percentage of 30 percent (AACPDM) versus 33 percent versus 40 percent (several registry definitions of displacement) are all in use. The trend and rate of change often matter more than crossing a single number.
- Best frequency and stopping point of radiographs. Schedules differ by GMFCS level and country, and the optimal point to discharge an ambulant child or a skeletally mature non-ambulant child is debated.
- Role of soft-tissue release alone. Adductor and psoas surgery can slow migration in younger children, but many hips progress and need later bony reconstruction. Selecting which early hips benefit remains imperfect.
- Timing of bony reconstruction. Whether to operate at a defined migration percentage or to wait for clear progression, and how to balance one-stage bilateral correction against staged surgery, varies between centres.
- Salvage choice. For a painful, unreconstructable dislocated hip there is no single best salvage; proximal femoral resection, valgus osteotomy, interposition and arthrodesis all have advocates, and the evidence is largely low level.
- Value of head-shaft angle and additional measures. Newer predictors (head-shaft angle, acetabular index) improve risk scores, but how much they should change individual decisions over migration percentage alone is still being defined.
- Surveillance after intervention. How long and how often to image after preventive or reconstructive surgery to detect recurrence lacks strong consensus.
In a viva, present thresholds as programme-dependent guides, not universal cut-offs, and emphasise trend, the whole clinical picture and family goals.
Evidence Signals
Population-based surveillance prevents dislocation (landmark)
- In the southern Sweden CPUP programme, hip dislocation fell from 8 percent in a historical control cohort to 0.5 percent in the first surveillance cohort and 0 percent in the second.
- Across 689 surveilled children, 91 (13 percent) underwent preventive surgery and none in the second cohort dislocated.
- Every child who did dislocate reported severe pain at least periodically, and four needed salvage surgery.
Displacement risk rises steeply with GMFCS level and subtype
- Risk of displacement with migration percentage over 40 percent rose from 0 percent in GMFCS I to 64 percent in GMFCS V across 212 children.
- Risk by subtype ranged from 0 percent in pure ataxia to 79 percent in spastic tetraplegia.
- Passive hip range of motion did not differ between displaced and non-displaced hips, so abduction alone is a poor screening test.
Natural history: migration progresses with decreasing function
- Among 335 Norwegian children, displacement (migration percentage over 33 percent) occurred in 26 percent overall and 63 percent of those in GMFCS IV or V.
- Mean progression in migration percentage rose from 0.2 percent per year at GMFCS I to 9.5 percent per year at GMFCS V.
- Dislocation occurred at a mean age of about 4.5 years, supporting early surveillance from age 1 to 2 years.
CPUP Hip Score predicts displacement risk
- A risk score combining age, GMFCS level, head-shaft angle and initial migration percentage predicted displacement (migration percentage over 40 percent) within five years.
- All four variables independently affected risk in 145 GMFCS III to V children.
- Discriminatory accuracy was high, with an area under the curve of 0.87.
CPUP Hip Score externally validated in a new population
- In 367 Scottish children in GMFCS III to V, the CPUP Hip Score discriminated risk well, with an area under the curve of 0.78, rising to 0.85 with re-estimated weights.
- Calibration was insufficient and absolute risks were overestimated, so the score ranked risk better than it predicted exact probabilities.
- Discrimination held across a different national pathway, supporting the underlying risk variables.
Reimers migration percentage and adductor surgery
- Reimers tracked hip migration before and after adductor transfer versus adductor tenotomy in spastic cerebral palsy.
- Both procedures slowed migration with no significant difference (about 4 and 7 percent per year respectively).
- Adductor transfer was more burdensome with no proven advantage, so simple tenotomy was favoured.
Clinical Reasoning Notes
Structured clinical approach
Use this sequence:
- Confirm or assign GMFCS from real-world mobility.
- Ask about care, sitting, hygiene, sleep, transfers and pain.
- Examine abduction, tone, contracture, pelvis and spine.
- Obtain AP pelvis and measure migration percentage.
- Decide surveillance interval, referral or treatment based on GMFCS, migration percentage, trend, abduction and symptoms.
- State the goal: comfortable located hips that support sitting, hygiene and care.
Common pitfalls
- Waiting for pain before imaging.
- Asking the family for a GMFCS label rather than assigning it from function.
- Treating adductor tightness without measuring migration percentage.
- Measuring only one hip.
- Forgetting pelvic obliquity and scoliosis.
- Offering reconstruction without discussing seating, hygiene and family goals.
- Thinking salvage care is only about the X-ray rather than comfort.
Evidence Base
AACPDM hip surveillance care pathway
- Hip surveillance is based on GMFCS level, age and migration percentage.
- Referral is recommended when migration percentage is over 30 percent or hip abduction is less than 30 degrees.
- Surveillance aims to detect displacement before pain and dislocation.
Consensus standards: timing and frequency of surveillance
- A multidisciplinary consensus defined when to start, how often to repeat and when to discharge from hip surveillance by GMFCS level.
- Radiograph frequency is tied to GMFCS level and migration-percentage trajectory rather than symptoms.
- The statement became a widely adopted template for national surveillance pathways.
Surveillance as a risk-management system
- Hip displacement is silent but progressive and is driven by flexor-adductor spasticity, abductor weakness and delayed weight-bearing.
- Migration percentage and GMFCS underpin surveillance models worldwide.
- More than 25 years of evidence supports universal surveillance, yet awareness and access remain uneven globally.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A non-ambulant child with cerebral palsy attends for routine review. How do you assess hip risk?”
“A child with severe cerebral palsy has a painful chronically dislocated hip. What are the goals of treatment?”
“A 5-year-old with GMFCS IV spastic quadriplegia had a migration percentage of 25 percent last year. The new AP pelvis shows 42 percent on the left with reduced abduction. The hip is not yet obviously painful. What do you do?”
Risk
- GMFCS IV-V
- Reduced abduction
- Rising MP
- Pelvic obliquity
- Windswept posture
Measure
- AP pelvis
- Migration percentage
- Both hips
- Trend
- Hip abduction
Treat
- Surveillance
- Tone and seating
- Adductor-psoas release
- VDRO
- Pelvic osteotomy
- Salvage selected
Goals
- Comfort
- Sitting
- Hygiene
- Sleep
- Ease of care