Non-Progressive UMN Lesion | GMFCS and Hip Surveillance
- Definition: A group of permanent disorders of the development of movement and posture, causing activity limitation, that are attributed to non-progressive disturbances that occurred in the developing fetal or infant brain.
- Hip Surveillance: ALL children with CP need hip surveillance. The frequency is determined by GMFCS level (Level V = Every 6 months).
- GMFCS: The most robust predictor of motor development and hip displacement risk.
- Spasticity vs Contracture: Spasticity is velocity-dependent tone (dynamic). Contracture is fixed shortening (static). Differentiate them using examination (R1/R2) or EUA.
- Lever Arm Dysfunction: Torsional deformities (femoral anteversion, tibial torsion) degrade the power generation of muscles. Must be corrected in SEMLS.
- “GMFCS Level is the single most important prognostic factor.
- “Hip dislocation is silent in CP! Hence surveillance.
- “Never lengthen the Achilles in a crouch gait (makes it worse).
- “Hemiplegic kids nearly always walk (Level I/II).
Pain free? hips can dislocate without pain initially. By the time they hurt, the head is destroyed. Screening is mandatory.
Surgery Risk. Dyskinesia (Dystonia/Chorea) responds POORLY to orthopaedic surgery. Rule out dystonia before cutting tendon/bone.
Single Event. Avoid "Birthday Syndrome" (surgery every year). Aim for Single Event Multi-Level Surgery (SEMLS) at age 8-10.
Do NOT lengthen T-Achilles. In crouch gait, the T-Achilles is often already long (over-lengthened). Lengthening it further causes calcaneal gait (disaster).
| Feature | Spasticity | Dystonia |
|---|---|---|
| Definition | Velocity-dependent resistance | Involuntary muscle contractions/postures |
| Feel | Clasp-knife | Lead-pipe / Fluctuating |
| Sleep | Persists (reduced) | Disappears |
| Surgery | Responds well | Contraindicated / Unpredictable |
Climb, Cane, Crutch, Car, CartGMFCS Levels
Hook:The 5 C's of GMFCS (Simplified).
1234Hemiplegia Patterns (Winters)
Hook:Winters Classification for Hemiplegia.
POSTERRisk Factors
Hook:POSTER child for CP.
Overview and Epidemiology
Definition: Cerebral Palsy (CP) is defined by the Rosenbaum (2005) consensus: "A group of permanent disorders of the development of movement and posture, causing activity limitation, that are attributed to non-progressive disturbances that occurred in the developing fetal or infant brain. The motor disorders are often accompanied by disturbances of sensation, perception, cognition, communication, and behavior, by epilepsy, and by secondary musculoskeletal problems."
Epidemiology:
- Incidence: 2-2.5 per 1000 live births (Stable despite obstetric advances, due to survival of extreme preterms).
- Risk Factors: Prematurity (strongest), Low Birth Weight, Multiple gestation, Infection (Chorioamnionitis).
- Asphyxia: Intrapartum asphyxia accounts for only 10% of cases.
Primary Prevention:
- Magnesium Sulfate: Given to mothers in threatened very preterm labour for fetal neuroprotection. Pooled meta-analysis (Cochrane) shows roughly a one-third relative reduction in CP; individual trials were under-powered for CP alone (see Evidence Base).
- Cooling (Therapeutic Hypothermia): Standard of care for term infants with HIE. Reduces mortality and severe disability.
- Corticosteroids: Antenatal steroids for lung maturity also reduce IVH risk.
Pathophysiology and Mechanisms
Brain Lesions:
- Periventricular Leukomalacia (PVL): Necrosis of white matter near lateral ventricles. Affects medial fibres of the corticospinal tract (legs affected more than arms). Classic cause of Spastic Diplegia in premature infants.
- Intraventricular Hemorrhage (IVH): Common in preterms.
- HIE (Hypoxic Ischemic Encephalopathy): Global injury. Often leads to Quadriplegia or Dyskinetic CP.
- Stroke (MCA Infarct): Cause of Hemiplegia.
Musculoskeletal Pathology: The brain lesion is static, but the MSK issues are progressive.
- Primary: Loss of selective motor control, spasticity, balance loss.
- Secondary: Muscle contracture (myostatic contracture), lever arm dysfunction (torsion).
- Tertiary: Bony deformity (hip dislocation, scoliosis), joint degeneration.
Lever Arm Dysfunction: Skeletal deformities reduce the efficiency of muscles.
- Femoral Anteversion: Intoeing. Glutes lose abduction power.
- Tibial Torsion: External. Foot pressure axis lateral.
- Pes Valgus: Midfoot break. Gastroc power lost (lever arm shortens).
Classification
Gross Motor Function Classification System (GMFCS)
The gold standard for prognosis and communication. Based on self-initiated movement sitting/walking.
- Level I: Walks without limitations. Runs/Jumps.
- Level II: Walks with limitations (railings, uneven ground). No running.
- Level III: Walks with handheld mobility device (Walker/Crutches). Wheelchair for long distance.
- Level IV: Self-mobility with limitations (Powered chair). Can stand for transfers.
- Level V: Transported in manual wheelchair. Head control issues.
GMFCS is stable over time.
Clinical Assessment
History:
- Birth history (Gestation, ICU stay).
- Milestones (Sit by 2? Walk by ?).
- Communication/Feeding status.
Physical Examination:
- Tone: Modified Ashworth Scale (0-4). Tardieu Scale (R1/R2).
- R1: Angle of first catch (velocity dependent).
- R2: Angle of Max passive range (static length).
- R2-R1: Dynamic component (Spasticity).
- Selective Motor Control (SMC): Ability to isolate joint movement.
- Rotational Profile: Anteversion, Tibial Torsion.
- Spine: Scoliosis check.
- Hips: Abduction range (Risk of dislocation if less than 45).
- Spine: Scoliosis check. Sitting balance. Pelvic obliquity.
Selective Motor Control (SMC): This is the ability to isolate joint movement.
- Test: Ask patient to dorsiflex ankle without flexing hip/knee.
- Significance: Poor SMC predicts poor outcome from tendon transfers. If SMC is absent, transfer will not work "in phase" (but may act as a tenodesis).
Gait Analysis (Observational):
- Sagittal Plane: Look for the "Gait Deviations".
- True Equinus: Hips extended, Knee extended, Ankle plantarflexed.
- Jump Gait: Hip flexed, Knee flexed, Ankle plantarflexed.
- Apparent Equinus: Hip flexed, Knee flexed, Ankle neutral (but looks equinus due to knee flexion).
- Crouch Gait: Hip flexed, Knee flexed (greater than 30 deg), Ankle dorsiflexed (Calcaneus).
- Coronal Plane:
- Scissoring: Adductor spasticity.
- Trendelenburg: Abductor weakness.
- Transverse Plane:
- Intoeing: Femoral anteversion vs Internal Tibial Torsion.
- Outtoeing: External Tibial Torsion (often iatrogenic or compensatory).
Anesthetic Considerations:
- Respiratory: High risk of aspiration (swallow dysfunction) and post-op pneumonia.
- Seizures: Ensure anticonvulsants are continued.
- Latex Allergy: Higher prevalence in CP/Spina Bifida.
- Positioning: Contractures make positioning on the table difficult. Pad purely bony prominences.
- Pain Assessment: FLACC scale for non-verbal children. High risk of under-treatment.
| Feature | Cerebral Palsy | Hereditary Spastic Paraparesis |
|---|---|---|
| Onset | Birth / Infancy (Static) | Childhood / Adult (Progressive) |
| Family History | Rare | Common (Autosomal Dominant) |
| MRI Brain | Abnormal (PVL/IVH) | Normal |
| Progression | Non-progressive (MSK worsens) | Neurology worsens |
Investigations
1. Hip Surveillance (X-rays):
- Why?: To prevent dislocation. Dislocation leads to pain, scoliosis, and hygiene issues in GMFCS V.
- Metric: Reimer's Migration Percentage (MP).
- Calculation: Percentage of the femoral head lateral to Perkins' line (Lateral edge of acetabulum).
- Normal: Less than 10% in normal children. Less than 30% acceptable in CP.
- Risk: Greater than 30% ("Hip at Risk"). Often "Silent" (Pain free).
- Dislocated: Greater than 100%. The head is completely lateral to the acetabulum.
2. Gait Analysis (3D Motion Lab):
- Gold Standard for surgical planning in walkers (GMFCS I-III).
- Kinematics: Joint angles.
- Kinetics: Forces/Moments (Joint powers).
- EMG: Muscle firing timing (rectus spasticity in swing?).
- Pedobarography: Foot pressure. 3. Gait Velocity and Oxygen Cost:
- Children with CP use 3-5x more energy to walk than peers.
- Oxygen Cost: measured in mL/kg/m.
- Goal of Surgery: Improve efficiency (Lower Oxygen cost).
4. GDI (Gait Deviation Index):
- A single number representing gait pathology.
- 100: Normal.
- Every 10 points below 100: One standard deviation from normal.
- Typical CP: GDI 60-70.
- Post-SEMLS: Expect increase of 5-10 points (Clinically significant).
5. Functional Assessment Tools:
- GMFM (Gross Motor Function Measure): Even more detailed than GMFCS. Used to track change over time (e.g. pre/post SDR).
- GMFM-88: Validated for CP and Down Syndrome. Includes lying/rolling.
- GMFM-66: Rasch-scaled version. Only for CP.
- FMS (Functional Mobility Scale): Rates mobility at 3 distances (Home, School, Community).
- 5 meters: Home.
- 50 meters: School.
- 500 meters: Community.
- Rating: 1 (Crawler) to 6 (Independent on all surfaces).
- CP-CHILD: Caregiver-reported Quality of Life measure (Comfort, Positioning).
Management Algorithm
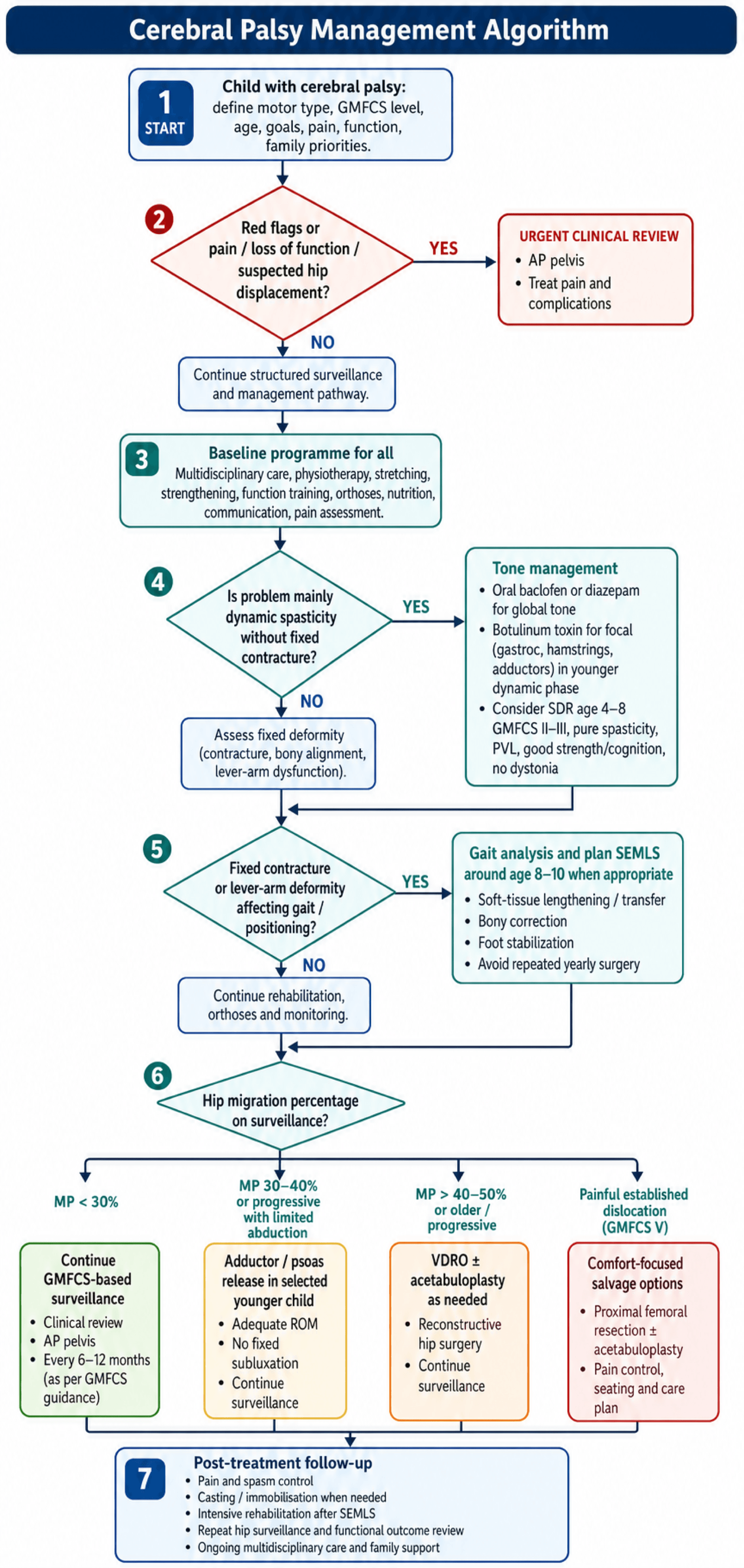
Multidisciplinary Management
- Physiotherapy: Stretch, Strengthen, Functional training.
- Orthotics:
- AFO (Ankle Foot Orthosis): Solid (for crouch/equinus) or Hinged (for simple drop foot).
- GRAFO: Ground Reaction AFO (Pre-tibial shell) for CROUCH gait (prevents tibial advancement).
- Tone Management:
- Oral: Baclofen, Diazepam (global effect).
- Botox: Focal spasticity. Good for young kids (dynamic phase). Target: Gastroc, Hamstrings, Adductors.
- Intrathecal Baclofen (ITB): For severe severe quadriplegia (GMFCS IV/V) with dystonia.
Botox is most effective in the "Dynamic Phase" (Age 2-6).
Surgical Technique
Hip Reconstruction
Hip Surveillance Surgery
For Migration greater than 30-40% or progressive subluxation.
- Soft Tissue (Preventive): Adductor/Psoas Release.
- Indication: MP greater than 30% in young child (less than 4) with abduction less than 30 deg.
- Bony Reconstruction: VDRO + Acetabuloplasty (Dega/San Diego).
- Indication: MP greater than 40-50% in older child (greater than 4).
- VDRO: Shorten (release tension), Varus (better cover), Derotate (fix anteversion).
- Pelvis: Hinge osteotomy to cover anterior/lateral head.
- Dega Technique: Curvilinear cut above acetabulum (leaving posterior cortex intact). Lever down the roof. Bone graft wedge. Ideal for deficient anterior/lateral coverage.
- San Diego: Similar to Dega but extends to sciatic notch (more coverage).
- Salter: Less common in CP (re-directs whole acetabulum, but creates retroversion which is bad in CP).
- Salvage: Castle Procedure (Resection Interposition) or Proximal Femoral Replacement.
- Indication: Painful GMFCS V dislocated hip with destroyed head.
Total Hip Arthroplasty is generally contraindicated in GMFCS V due to high dislocation risk.

Complications
| Complication | Risk Factor | Management |
|---|---|---|
| Over-lengthening | TAL (Tendo-Achilles) | Calcaneal gait (Crouch). Hard to fix. |
| Recurrence | Young age (less than 6) at time of surgery | Repeat surgery |
| Hip Re-dislocation | GMFCS V / Scoliosis | Salvage surgery |
| Pathologic Fracture | Osteopenia / Cast immobilization | Gentle handling / Bisphosphonates |
| Baclofen Pump Risk | Catheter kink / Infection / Overdose | Emergency pump interrogation |
Baclofen Pump Failure:
- Overdose: Coma, Respiratory depression, Hypotension. Support airway. Physostigmine (controversial).
- Withdrawal: Itchy, Agitated, Rigid, Seizures, Hyperthermia. Life threatening. Restore Baclofen (oral/intrathecal) immediately.
Postoperative Care
Pain management is critical, especially in Spastic CP where pain triggers spasm, which triggers more pain.
- Spasm Protocols: Benzodiazepines (Diazepam) + Gabapentin.
- Immobilization: Petrie Casts (Broomstick) or Spica for hips.
- Rehab: Intensive inpatient rehab for 6-12 weeks post-SEMLS.
Outcomes
- Walking: GMFCS I/II walk well. III walk with aids. IV/V do not walk.
- Employment: Competitive employment rates are low (GMFCS dependent).
- Pain: Over 50% of adults with CP report chronic musculoskeletal pain.
- Life Expectancy: Reduced in GMFCS V (respiratory issues). Near normal in I-III.
Hamstring Surgery Outcomes


Evidence Base
GMFCS — The Classification Paper
- Delphi consensus among 48 experts produced the 5-level GMFCS.
- Interrater reliability (kappa) 0.75 for children aged 2-12 years; lower (0.55) under 2 years.
- Designed as a staging system analogous to medical grading scales.
Hip Surveillance Prevents Dislocation (CPUP)
- 20-year results of the Swedish CPUP surveillance programme.
- Hip dislocation fell from 8% in the historical control group to effectively 0% in surveilled cohorts (p less than 0.001).
- The only 2 study-group children who dislocated were too unwell for preventive surgery.
- Of 689 surveilled children, 13% required preventive surgery.
Primary Surgery for Hip Displacement
- Compared adductor-iliopsoas tenotomy (APT) vs femoral osteotomy (FO) as primary preventive surgery.
- At minimum 5 years, reoperation was 43% after APT and 39% after FO.
- Residual migration percentage over 50% in 2% (APT) vs 9% (FO).
- After soft-tissue release, higher preoperative migration percentage predicted failure.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Discuss your management approach.”
Controversies & Areas of Uncertainty
- SDR vs intrathecal baclofen vs SEMLS: For ambulant spastic diplegia there is no high-quality head-to-head RCT. Long-term cohorts (Tedroff) show SDR durably reduces tone but does not prevent later orthopaedic surgery or contracture — challenging the idea that early tone reduction alone changes natural history.
- Does SEMLS truly change long-term function? Gait-lab kinematics (GDI) improve, but functional/participation gains and durability are debated, and the evidence base lacks RCTs (McGinley).
- Optimal hip surveillance threshold for intervention: Migration percentage thresholds (30% vs 40% vs trend/velocity) and whether soft-tissue release alone suffices vary between programmes; reoperation rates remain high (Kiapekos).
- Magnesium sulfate magnitude of effect: Individual trials (including ACTOMgSO4/Crowther) were under-powered for CP as a sole endpoint; the neuroprotective recommendation rests on pooled meta-analysis, and optimal dosing/timing still varies.
- Single-event vs staged surgery: "Birthday syndrome" is condemned, yet very large single events carry higher perioperative and rehabilitation burden — the ideal bundling remains individualised.
- Botulinum toxin and muscle morphology: Concern that repeated BTX-A injections may cause long-term muscle atrophy/fibrosis in the developing muscle, tempering enthusiasm for high-frequency dosing.
MCQ Practice Points
Q: What is the most common physiologic type of CP? A: Spastic (Pyramidal) - approx 80%. Dyskinetic is 10-15%. Ataxic less than 5%.
Q: How often should a GMFCS Level V child have a hip X-ray? A: Every 6 months. (High risk of rapid displacement). Level I usually discharged at 5 years.
Q: What determines the difference between GMFCS II and III? A: Handheld Mobility Device. Level II walks without aids (may use rail). Level III needs crutches/walker.
Q: What determines the difference between GMFCS IV and V? A: Self-Mobility. Level IV can drive a powered chair or mobilize short distances. Level V has no means of independent mobility (must be pushed).
Q: What is the likelihood of a child with Hemiplegic CP walking? A: Nearly 100% (Usually GMFCS I or II). If a hemiplegic child is not walking, reconsider diagnosis.
Q: Periventricular Leukomalacia (PVL) is most strongly associated with which CP pattern? A: Spastic Diplegia. The medial fibers (legs) of the corticospinal tract are affected.
Guidelines, Registries & Global Practice
Global Epidemiology:
- Prevalence: ~2.0-2.5 per 1000 live births in high-income settings; higher in low- and middle-income countries (LMICs) where prevalence may exceed 3 per 1000, with a higher proportion of severe, GMFCS IV-V and post-neonatally acquired CP (infection, kernicterus, birth asphyxia).
- Trend: Prevalence has plateaued or fallen modestly in high-income countries despite improved survival of extreme preterms, attributed to antenatal magnesium sulfate, antenatal steroids, and therapeutic hypothermia.
- Distribution: Spastic subtype ~80%; spastic diplegia/hemiplegia predominate; bilateral GMFCS IV-V drive the orthopaedic burden (hip, spine).
| Body / Region | Hip Surveillance | Tone & Surgery Emphasis |
|---|---|---|
| AusACPDM (Australasia) | GMFCS-stratified schedule; 6-monthly films for GMFCS IV-V | Early preventive soft-tissue release; SEMLS for ambulant CP |
| AACPDM (North America) | Care pathways endorse GMFCS-based screening | Multidisciplinary tone clinics; SDR in selected GMFCS II-III |
| BSCOS / UK (BOAST-aligned) | National CP Integrated Pathway (e.g. CPIPS) — GMFCS-based films | Surveillance-led prevention; NICE NG62 supports MDT spasticity care |
| CPUP (Sweden/Scandinavia) | Founding surveillance registry; near-zero dislocation | Registry-driven prevention; benchmark for outcomes |
Registries & Surveillance Networks:
- CPUP (Sweden/Norway/Denmark/Scotland): The reference hip and spine surveillance registry; demonstrated near-elimination of hip dislocation.
- SCPE (Surveillance of Cerebral Palsy in Europe): Harmonised CP definitions and population prevalence data across European centres.
- CPIPS / UK national CP integrated pathway and Australian CP Register: National-scale GMFCS-based surveillance and outcome tracking.
High- vs Limited-Resource Practice Variation:
- High-resource: Routine GMFCS-based radiographic hip surveillance, 3D gait labs for SEMLS planning, intrathecal baclofen, SDR programmes, neonatal neuroprotection bundles.
- Limited-resource: Later presentation with established dislocation/contracture; emphasis on physiotherapy, low-cost orthoses, and salvage rather than preventive surgery; gait labs and SDR rarely available. Prevention of kernicterus and birth-asphyxia CP is a major public-health priority.
GMFCS Levels
- I: Walks / Runs
- II: Walks / Railing / Uneven issues
- III: Handheld Device (Walker)
- IV: Powered Mobility
- V: Pushed (Head control issues)
Hip Surveillance
- Gold Standard: Reimer's MP
- Normal: less than 10%
- Risk: greater than 30%
- Freq: GMFCS V = 6 monthly
Management
- Botox: Focal Dynamic Spasticity
- Baclofen: Global Spasticity
- SEMLS: Age 8-10, Bony + Soft Tissue
- SDR: Pure Spasticity, GMFCS II/III
Key Concepts
- Non-progressive brain lesion
- Progressive MSK deformity
- Lever Arm Dysfunction
- Avoid Birthday Syndrome