Radiculopathy | Dermatomal Patterns | ACDF Indications
- C5-C6 and C6-C7 are most common levels
- MRI is gold standard imaging
- Conservative treatment 90% effective
- ACDF gold standard for surgical cases
- Progressive motor weakness is urgent surgical indication
- “C5 = deltoid and biceps, C6 = biceps reflex, thumb
- “C7 = triceps, middle finger (most common)
- “Spurling sign confirms radicular origin
- “Red flags: myelopathy, progressive deficit
Clinical Imaging
Imaging Atlas

PRIMARY distinction. Radiculopathy = Root (Pain/Weakness). Myelopathy = Cord (Balance/Dexterity/UMN signs). Missed myelopathy fails the station.
Roots exit ABOVE the pedicle. C5/6 Disc → C6 Root. (Contrast with Lumbar where L4/5 Disc → L5 Root).
Must know root levels. C5=deltoid/shoulder. C6=biceps/thumb. C7=triceps/middle finger. C8=hand intrinsics/small finger.
Urgent surgical indication. Gait disturbance, hand clumsiness, hyperreflexia, Babinski positive. Do not delay surgery.
Shoulder Abduction Relief Sign. Pain relief with arm over head = cervical radiculopathy. Key exam finding.
Anterior approach removes disc directly, decompress neural elements, restore height. High fusion rates with cage and plate.
6-12 weeks of conservative treatment for uncomplicated radiculopathy. 90% improve without surgery.
| Presentation | Key Features | Management |
|---|---|---|
| Pure radiculopathy | No myelopathy, no motor deficit | Conservative 6-12 weeks |
| Radiculopathy with motor weakness | Grade 4 power or better | Conservative trial, close follow-up |
| Progressive motor deficit | Worsening weakness | Urgent surgical decompression (ACDF) |
| Myelopathy | Gait, hand function, hyperreflexia | Surgical decompression indicated |
C5-6-7-8Cervical Root Levels
Hook:5-6-7-8, shoulder down to digit eight!
FAILSurgical Indications
Hook:If conservative FAILS, consider surgery!
HARDSACDF Complications
Hook:ACDF can be HARD on the throat and spine long-term!
Overview and Epidemiology
Most cervical radiculopathy improves without surgery. 90% of patients improve with conservative management over 6-12 weeks. Surgery indicated for failed conservative treatment, progressive deficit, or myelopathy.
- Degenerative changes (age)
- Smoking
- Heavy manual labor
- Prior disc disease
- Genetic predisposition
- Disc herniation (soft)
- Osteophyte formation (hard)
- Neuroforaminal narrowing
- Neural compression
- Inflammatory mediators
Pathophysiology and Mechanisms
Cervical Disc Structure
Nucleus pulposus: Central gelatinous material, high water content, provides cushioning.
Annulus fibrosus: Outer fibrous ring, contains nucleus, attaches to vertebrae.
Uncovertebral joints (Luschka): Posterolateral, common site of osteophyte formation.
Posterior longitudinal ligament: Thin in cervical spine, less protection against posterolateral herniation.
Disc degeneration leads to height loss, osteophyte formation, and neural compression.
Cervical roots exit ABOVE their numbered vertebra (C6 root exits C5-C6). This differs from lumbar spine where roots exit BELOW (L5 root exits L5-S1).
Classification Systems
Disc Pathology Classification
| Type | Description | Treatment Implication |
|---|---|---|
| Soft disc | Acute herniation | May resorb, good surgical outcome |
| Hard disc (spondylosis) | Osteophyte, chronic | May require osteophyte removal |
| Combined | Disc plus osteophyte | Common, address both elements |
Soft disc herniations may resolve naturally; hard discs rarely do.
Clinical Assessment
- Pain: Neck, arm (radicular pattern)
- Sensory symptoms: Numbness, tingling
- Motor: Weakness, clumsiness
- Aggravating factors: Extension, rotation
- Red flags: Gait, bladder, bilateral symptoms
- Spurling test: Radicular reproduction
- Motor: Deltoid, biceps, triceps, grip
- Sensory: Dermatomal pattern
- Reflexes: Biceps (C5-C6), triceps (C7)
- Upper motor signs: If myelopathy
| Root | Motor | Reflex | Sensory |
|---|---|---|---|
| C5 | Deltoid, biceps | Biceps | Lateral arm |
| C6 | Biceps, wrist extensors | Brachioradialis | Thumb, lateral forearm |
| C7 | Triceps, wrist flexors | Triceps | Middle finger |
| C8 | Finger flexors, intrinsics | None reliable | Small finger, medial forearm |
Do not miss myelopathy: Gait disturbance, hand clumsiness (buttons), hyperreflexia, Hoffmann sign, upgoing plantars, clonus. Requires urgent referral and imaging.
Differential Diagnosis
Arm pain and hand symptoms have many causes outside the cervical disc. The examiner will reward a structured differential that distinguishes neural compression from peripheral entrapment, referred pain and non-musculoskeletal mimics.
| Condition | Distinguishing Features | Confirmatory Test |
|---|---|---|
| Cervical radiculopathy | Dermatomal pain, positive Spurling, relief with Bakody (shoulder abduction) | MRI plus clinical correlation, EMG/NCS |
| Cervical myelopathy | Bilateral/gait symptoms, hand clumsiness, UMN signs (Hoffmann, hyperreflexia) | MRI cord compression plus or minus signal change |
| Carpal tunnel syndrome | Median distribution, nocturnal, Tinel/Phalen positive, no neck pain | Nerve conduction studies |
| Cubital tunnel syndrome | Ulnar distribution (small/ring finger), elbow flexion provokes | NCS across elbow |
| Thoracic outlet syndrome | Positional symptoms, vascular features, lower trunk (C8-T1) pattern | Provocative tests, vascular imaging |
| Brachial neuritis (Parsonage-Turner) | Acute severe shoulder pain then patchy weakness, non-dermatomal | EMG, clinical course |
| Rotator cuff / shoulder pathology | Pain with shoulder movement, no neurology, painful arc | Shoulder exam, ultrasound/MRI |
| Pancoast tumour / apical mass | Lower trunk symptoms, Horner syndrome, weight loss, smoker | Chest imaging, urgent CT |
Always exclude sinister causes of arm/neck symptoms: Pancoast tumour (Horner syndrome, T1 weakness, smoking history), infection/discitis (fever, raised inflammatory markers, immunosuppression) and metastatic disease (night pain, known primary). These change the pathway entirely.
Investigations
MRI - Gold Standard
Indications:
- Suspected radiculopathy or myelopathy
- Failed conservative treatment
- Progressive neurological deficit
- Preoperative planning
What to assess:
- Disc herniation level and side
- Neuroforaminal stenosis
- Cord compression and signal change
- Multi-level disease
T2 signal in cord = myelomalacia, poorer prognosis.
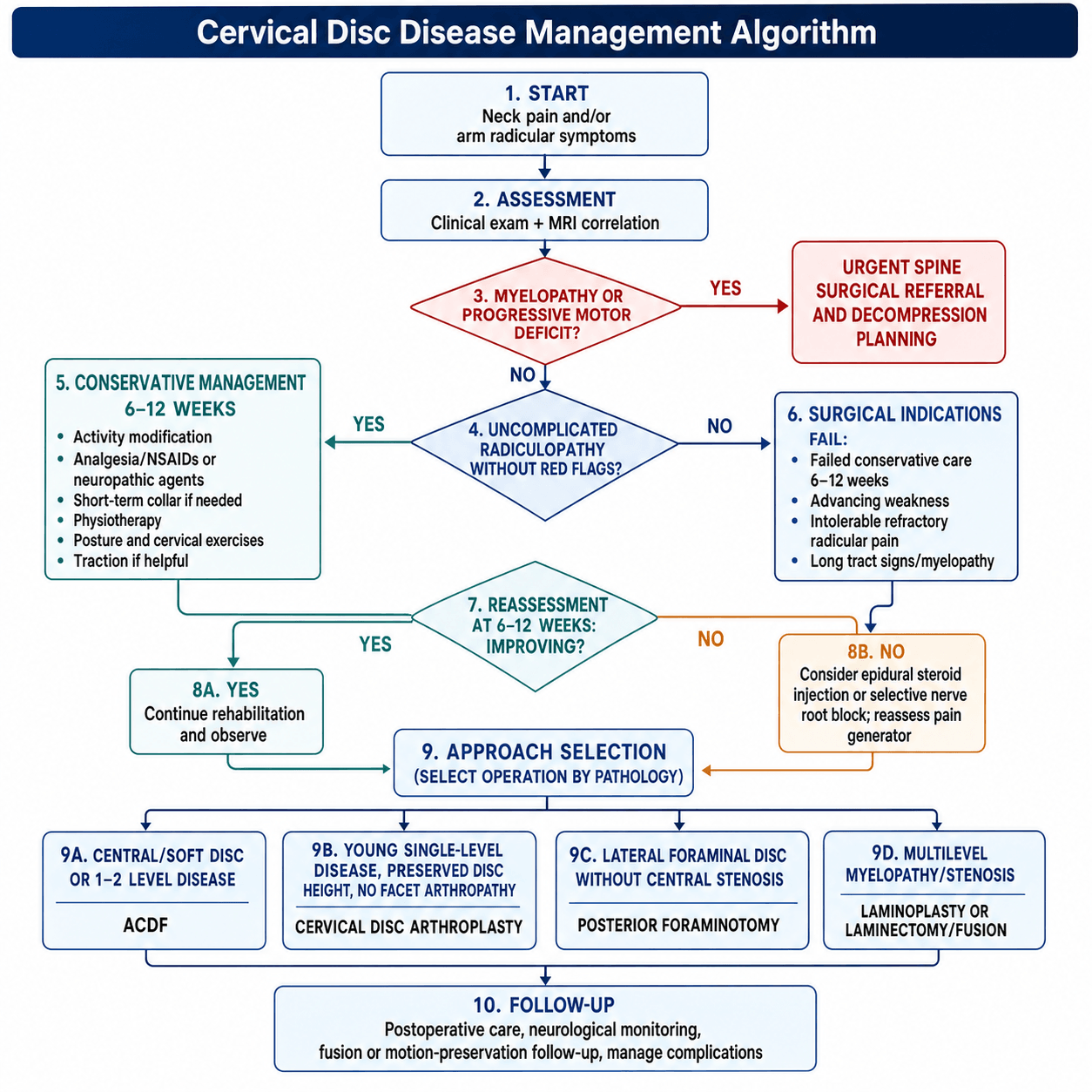
Management Algorithm
Conservative Management
Conservative Protocol
Activity modification. Analgesia (NSAIDs, neuropathic agents). Soft collar short-term if needed.
Physiotherapy. Postural education. Cervical exercises. Traction if helpful.
Reassess symptoms and function. If improving, continue. If not, consider intervention.
90% improve with conservative management. Patience is key.
Surgical Technique
Anterior Cervical Discectomy and Fusion
Gold standard for single or two-level disease.
Approach:
- Left-sided anterior approach (protects recurrent laryngeal nerve)
- Smith-Robinson between carotid sheath and midline
- Disc excision under microscope/loupe
Key steps:
- Complete discectomy including posterior annulus
- Decompress neuroforamen bilaterally
- Endplate preparation (preserve subchondral bone)
- Cage placement (PEEK or titanium)
- Plate fixation (optional for single level)
Fusion rate greater than 95% with modern techniques.
Left-sided approach preferred for primary ACDF because right recurrent laryngeal nerve has more variable course. Still protect esophagus and avoid excessive retraction.
Complications
| Complication | Incidence | Notes |
|---|---|---|
| Dysphagia | 5-30% early | Usually resolves, retraction-related |
| Hoarseness (RLN) | 1-5% | Usually temporary, protect nerve |
| Pseudarthrosis | 2-5% | May need revision |
| Adjacent segment disease | 2-3% per year | Long-term concern, may need extension |
| Spinal cord injury | Very rare | Devastating, meticulous technique |
ASD is long-term concern after fusion. Rate approximately 2-3% per year requiring surgery. Disc replacement may reduce but not eliminate risk.
Postoperative Care
ACDF Recovery
Monitor swallowing (dysphagia common). Watch for hematoma (airway compromise). Mobilize day 1.
Soft collar optional (surgeon preference). Avoid neck flexion or rotation. Light activity. Swallowing usually improves.
Gentle ROM exercises. Physiotherapy. Driving when comfortable and off narcotics.
Return to most activities. Fusion consolidating. X-ray to confirm fusion.
Dysphagia is common after ACDF (up to 30% early) but usually resolves. Related to esophageal retraction. Persistent dysphagia may indicate hardware prominence or esophageal injury.
Outcomes and Prognosis
Prognostic Factors
Better outcomes:
- Shorter symptom duration
- Single-level disease
- Predominant arm pain (vs neck)
- No myelopathy
Worse outcomes:
- Long-standing symptoms
- Multi-level disease
- Myelopathy with cord signal change
- Workers compensation (psychosocial)
Controversies and Areas of Uncertainty
Arthroplasty reduces reoperation and superior-level degeneration in pooled RCTs, but most trials are industry-sponsored non-inferiority designs. Whether motion preservation truly prevents (rather than delays) adjacent-segment disease over 15-plus years remains unresolved.
Surgery clearly helps moderate-severe myelopathy. For mild myelopathy (mJOA 15 or above) the choice between early surgery and structured surveillance is debated, though prospective data show benefit even in mild disease.
Anterior plating raises fusion rates and reduces subsidence but increases dysphagia and adjacent-level ossification. Standalone/zero-profile cages reduce dysphagia; the trade-off in multilevel constructs is unsettled.
For multilevel myelopathy with neutral/lordotic alignment, anterior and posterior approaches give comparable neurological recovery. Alignment, number of levels and ossified PLL drive selection more than outcome superiority.
Evidence Base and Key Studies
Persson RCT: Surgery vs Physiotherapy vs Collar
- 81 patients with long-lasting cervical radiculopathy randomised to surgery, physiotherapy or cervical collar
- At 4 months the surgery group had less pain, less sensory loss and greater muscle strength than both conservative groups
- By 16 months there were no differences between groups in pain, sensory loss or paraesthesia
- Slow conservative improvement and recurrent symptoms after surgery made one-year outcomes broadly equal
CASINO: Surgery vs Prolonged Conservative Care
- Multicentre RCT design comparing early surgery (anterior discectomy or posterior foraminotomy) with prolonged conservative care for MRI-proven herniated cervical disc
- Eligible patients had disabling radicular arm pain for at least 2 months
- Primary outcome was arm pain/paraesthesia VAS at one year, with timing of surgery as a key secondary analysis
- Mirrors lumbar sciatica trial design where prolonged conservative care matched early surgery at one year
Fehlings AOSpine North America CSM Study
- Prospective multicentre cohort of 278 patients undergoing surgical decompression for cervical spondylotic myelopathy
- Significant improvement at one year in mJOA, Nurick grade, NDI and most SF-36v2 domains across mild, moderate and severe disease
- Benefit was seen even in mild myelopathy, supporting earlier intervention
- Overall complication rate 18.7%, consistent with prior series
Hilibrand: Adjacent-Segment Disease After Fusion
- 409 anterior cervical arthrodeses followed up to 21 years
- Symptomatic adjacent-segment disease occurred at a relatively constant 2.9% per year
- Kaplan-Meier predicted 25.6% of patients develop new adjacent-level disease within 10 years
- Risk highest at C5-C6 and C6-C7; single-level fusion carried higher risk than multilevel
Meta-analysis: Arthroplasty vs ACDF (mid-to-long term)
- Eight prospective RCTs pooled (1317 arthroplasty vs 1051 ACDF) with at least 48 months follow-up
- Arthroplasty showed higher overall success, NDI success and neurological success
- Lower rate of secondary procedures and superior-level adjacent-segment degeneration with arthroplasty
- Functional scores (NDI, VAS, SF-36 PCS) and satisfaction favoured arthroplasty
Meta-analysis: Single-level Arthroplasty vs ACDF
- Six RCTs, 1745 patients, single-level symptomatic cervical disc disease
- Arthroplasty had higher neurological and overall success at 2 years
- Lower incidence of dysphagia and lower reoperation related to adjacent-segment degeneration
- No significant difference in NDI or neck/arm pain scores between groups
Meta-analysis: ACDF vs Posterior Foraminotomy
- Three RCTs and twelve retrospective studies pooled for single-level unilateral radiculopathy
- No significant difference in NDI, VAS or patient satisfaction between ACDF and posterior foraminotomy
- Posterior foraminotomy had shorter operating time, shorter stay and lower cost
- Reoperation rate was higher after posterior foraminotomy
AAOS / NASS / BOA Guidance on Cervical Radiculopathy
- Initial non-operative management is recommended for uncomplicated radiculopathy without progressive deficit or myelopathy
- MRI is the imaging investigation of choice when surgery is contemplated or red flags are present
- Surgery is advised for persistent disabling symptoms, progressive neurological deficit or myelopathy
- Approach selection (ACDF, arthroplasty, posterior foraminotomy) is guided by pathology level, alignment and number of segments
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old office worker presents with 6 weeks of right arm pain radiating to the middle finger with some weakness in triceps. MRI shows C6-C7 right posterolateral disc herniation. How do you manage?”
“A 62-year-old man presents with 3 months of gait unsteadiness, difficulty with buttons, and bilateral hand numbness. Examination shows hyperreflexia, positive Hoffmann sign, and broad-based gait. MRI shows multi-level stenosis C3-7 with cord signal change at C5-6.”
“You performed a single-level ACDF at C5-6 yesterday. The patient calls the ward complaining of difficulty breathing and voice change. What is your management?”
MCQ Practice Points
Q: Which root is affected by a C5-C6 disc herniation? A: C6 root. In the cervical spine, the root exits ABOVE the disc (C6 root exits at C5-C6).
Q: What dermatomal pattern characterizes C7 radiculopathy? A: Middle finger sensory changes, triceps weakness, triceps reflex diminished. C7 is most common radiculopathy.
Q: What is the most important surgical indication in cervical disc disease? A: Myelopathy. Long tract signs indicate cord compression and require urgent surgical decompression.
Q: Why is left-sided approach preferred for ACDF? A: Recurrent laryngeal nerve protection. Right RLN has more variable course around subclavian artery.
Q: How long should conservative treatment continue before considering surgery? A: 6-12 weeks for uncomplicated radiculopathy. 90% improve without surgery.
Guidelines, Registries & Global Practice
Global Epidemiology
- Cervical radiculopathy has a reported annual incidence of approximately 80 per 100,000 population, peaking in the fifth and sixth decades.
- C7 (from C6-C7 disc) is the most commonly affected root, followed by C6 (from C5-C6).
- Cervical spondylotic myelopathy is the leading cause of acquired spinal cord dysfunction in adults worldwide and rises sharply with age.
- A minority of acute radiculopathy is true soft-disc herniation; most chronic presentations reflect spondylotic (hard-disc/osteophyte) compression.
Side-by-side Guideline Comparison
| Body | Initial Management | Surgical Trigger / Approach Emphasis |
|---|---|---|
| NASS / AAOS (US) | Conservative first for uncomplicated radiculopathy; MRI when surgery considered | Persistent disabling symptoms, progressive deficit, myelopathy; approach per pathology |
| BOA / British practice (UK) | Primary care led conservative care, physiotherapy, analgesia | Red flags or failed conservative care prompt spinal referral and MRI |
| AO Spine | Risk-stratified pathway; structured myelopathy assessment (mJOA) | Decompression for moderate-severe myelopathy; consider surgery in mild progressive disease |
| EFORT / European consensus | Evidence-based conservative trial before intervention | Approach matched to alignment, levels and ossified PLL |
- Dedicated cervical-disc registries are less mature than hip/knee arthroplasty registries, but national spine registries (e.g. Swedish Swespine, UK British Spine Registry) capture ACDF and arthroplasty outcomes.
- Pooled RCT and registry data report fusion rates over 95% with modern cage-plate ACDF.
- Arthroplasty registries show low but real revision for heterotopic ossification and device migration.
- High-resource: ready MRI access, microscope/loupe ACDF, arthroplasty and navigation available; earlier myelopathy detection.
- Limited-resource: reliance on radiographs and CT myelography, longer conservative trials, autograft over costly implants, later myelopathy presentation with worse baseline mJOA.
- Core principles (conservative-first radiculopathy, timely myelopathy decompression) are universal.
Across all major societies the message is consistent: conservative management first for uncomplicated radiculopathy, MRI when surgery is contemplated, and timely surgical decompression for myelopathy or progressive deficit. Approach selection is driven by pathology, alignment and number of levels, not geography.
Root Levels
- C5: Deltoid, shoulder abduction, lateral arm
- C6: Biceps, wrist extension, thumb
- C7: Triceps, wrist flexion, middle finger
- C8: Intrinsics, finger flexion, small finger
Conservative Trial
- 6-12 weeks for uncomplicated
- 90% success rate
- NSAIDs, neuropathic agents, PT
- Red flags require urgent surgery
Surgical Indications (FAIL)
- Failed conservative (6-12 weeks)
- Advancing weakness (progressive)
- Intolerable pain (refractory)
- Long tract signs (myelopathy - urgent)
ACDF Pearls
- Left-sided approach (protect RLN)
- Complete discectomy and decompression
- Cage plus or minus plate
- Greater 95% fusion rate
Complications (HARDS)
- Hoarseness (RLN injury)
- Adjacent segment disease
- Recurrent symptoms (pseudarthrosis)
- Dysphagia (common, resolves)
- Spinal cord injury (rare)
Myelopathy Signs
- Gait disturbance
- Hand clumsiness (buttons)
- Hyperreflexia, Hoffmann, Babinski
- Do not delay surgery