Angular Deviation in Coronal Plane
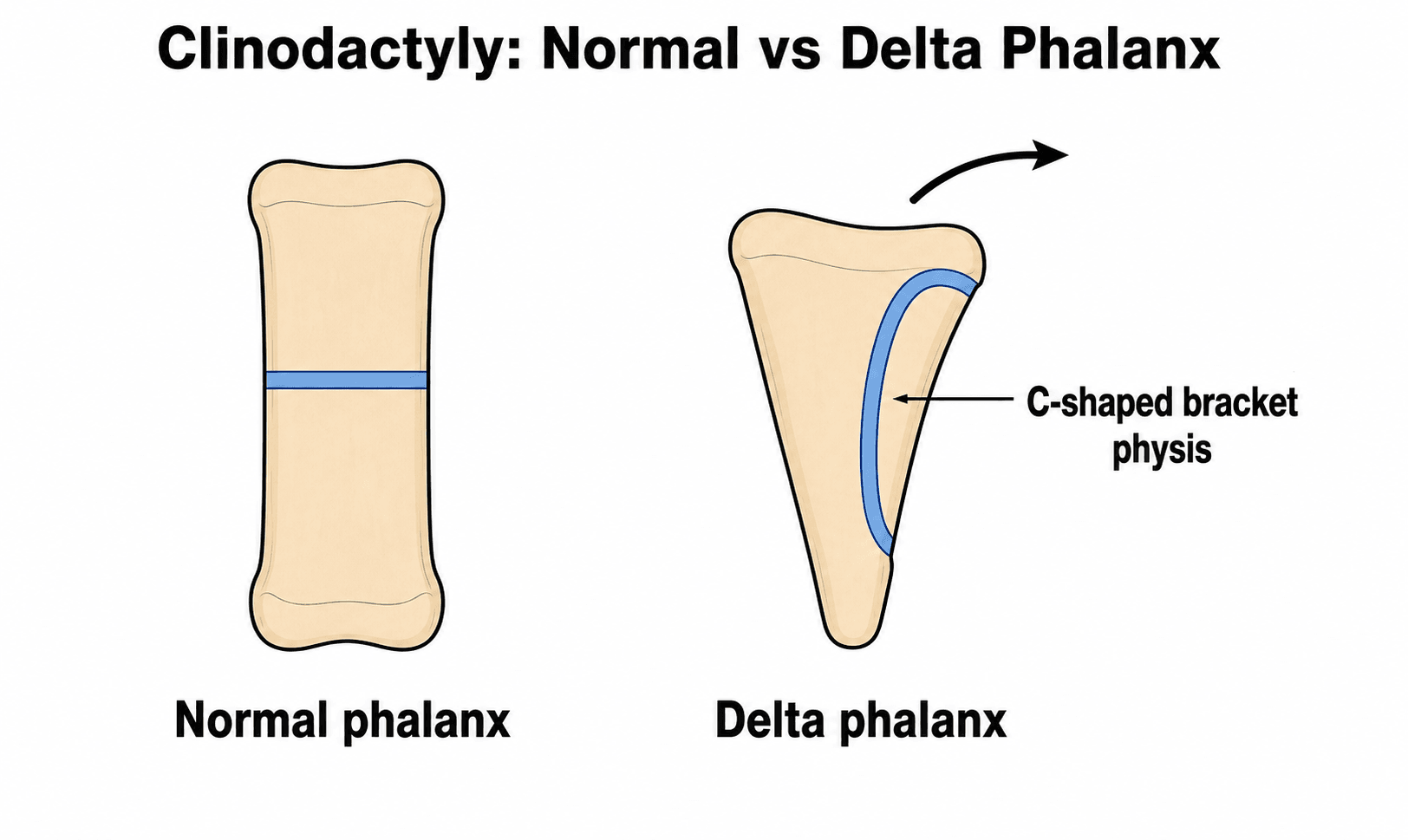
- Delta phalanx: Triangular bone with C-shaped bracket epiphysis that spans two sides causing angular growth.
- Most Common: Small finger (radial deviation) - middle phalanx.
- Down syndrome: Over 50% have clinodactyly.
- Surgical indications: Over 30 degrees, progressive deformity, functional impairment.
- Procedures: Opening wedge osteotomy (most common) or physiolysis for younger children.
- “Delta phalanx = C-shaped bracket epiphysis
- “Over 30 degrees = surgical threshold
- “Small finger most commonly affected
- “Down syndrome strong association
- “Opening wedge needs bone graft
Delta Phalanx: Triangular/wedge-shaped bone (not rectangular).
C-Shaped Physis: Spans TWO sides of the bone (normal spans one).
Asymmetric Growth: Bracket tethers one side → Progressive angular deformity.
Best View: AP Radiograph. Look for the "C" shape.
Pathognomonic Feature
- Triangular/wedge-shaped bone
- C-shaped bracket epiphysis
- Spans two sides of bone
- Causes progressive deformity
Comparison
- Rectangular phalanx shape
- Straight linear physis
- Spans ONE side only
- Symmetric longitudinal growth
Functional Effects
- Usually cosmetic concern
- Overlapping digits (severe cases)
- Grip interference (rare)
- Keyboard/fine motor (severe)
DELTADELTA Phalanx Features
Hook:DELTA phalanx: triangular bone with C-shaped bracket Epiphysis that spans Longitudinally causing Asymmetric growth and angular Deviation
SMALLSMALL Finger Clinodactyly
Hook:SMALL finger clinodactyly: most common digit (Small), Middle phalanx location, Angular deviation from bracket physis
THIRTYTHIRTY Degrees - Surgery Indication
Hook:THIRTY degrees: Surgery indicated if over 30 degrees, progressive, functionally limiting, or severe cosmetic concern at age 4-6 years
Overview and Epidemiology
Clinodactyly is defined as angular deviation of a digit in the coronal (radioulnar) plane, most commonly affecting the small finger with radial deviation.
Definition and Terminology
- Clinodactyly: From Greek "klinein" (to bend) and "daktylos" (finger)
- Coronal plane deviation: Angular deviation in radioulnar direction
- Distinguish from: Camptodactyly (flexion deformity in sagittal plane)
- Kirner deformity: Specific form affecting small finger distal phalanx with volar-radial curvature
Epidemiology
- General Population: 1-10% incidence (variable based on diagnostic threshold)
- Down Syndrome: Over 50% affected (strongest association)
- Gender: Equal distribution male to female
- Bilaterality: Often bilateral (60-70% of cases)
- Inheritance: Often autosomal dominant with variable penetrance
Associated Conditions
- Incidence
- Over 50%
- Other Hand Features
- Single palmar crease, short 5th finger
- Incidence
- Common
- Other Hand Features
- Complex syndactyly, broad thumb
- Incidence
- Common
- Other Hand Features
- Small hands, asymmetry
- Incidence
- Variable
- Other Hand Features
- Symbrachydactyly, absent pectoralis
- Incidence
- Most common
- Other Hand Features
- No other anomalies
Embryology
- Digital formation occurs at weeks 4-8 of gestation
- Phalangeal development involves chondrification (week 5-6)
- Normal physes form as straight transverse plates
- Delta phalanx results from abnormal chondrification
- Bracket epiphysis develops instead of normal linear physis
Pathoanatomy and Biomechanics
Normal Phalangeal Anatomy
- Rectangular bone: Tubular shape with parallel sides
- Linear physis: Straight transverse growth plate on ONE end
- Symmetric growth: Equal growth on radial and ulnar sides
- Normal alignment: Straight digital cascade in coronal plane
Delta Phalanx Pathoanatomy
Key Features:
- Triangular/wedge shape: Instead of rectangular phalanx
- C-shaped bracket epiphysis: Curves around and spans TWO sides of bone
- Asymmetric growth: Shorter side (usually radial) grows less
- Progressive deformity: Angular deviation increases with skeletal growth
Radiographic Appearance:
- AP view (best): Triangular bone outline, C-shaped physis visible
- Lateral view: May appear relatively normal
- Physeal shape: C or bracket configuration pathognomonic
- Adjacent bones: Usually normal morphology
Biomechanics of Deformity
- Hueter-Volkmann principle: Compression inhibits growth, tension stimulates
- Bracket physis: Tethers one side while allowing growth on other
- Progressive nature: Deformity worsens during growth spurts
- Growth cessation: Deformity stabilizes after skeletal maturity
- Remodeling potential: Limited in coronal plane deformities
Location Distribution
Most Common: Small Finger (5th Digit)
- Middle phalanx involvement (most frequent)
- Radial deviation typical
- Often bilateral
- Associated with Down syndrome
Less Common: Other Digits
- Index finger (2nd most common)
- Thumb (rare, when present often syndromic)
- Multiple digits (syndromic associations)
Most of the common 1-10% population little-finger clinodactyly is physiological: a mild, non-progressive, often familial (autosomal dominant) deviation from a slightly trapezoidal middle phalanx WITHOUT a true longitudinal epiphyseal bracket, needing only observation and reassurance. The minority that is progressive and surgically relevant has a genuine delta phalanx / longitudinal epiphyseal bracket that tethers one side and worsens with growth. The practical message: confirm a true bracket epiphysis on the AP radiograph before labelling a clinodactyly "delta phalanx" or recommending surgery - a mild non-progressive deviation is not a delta phalanx.
A delta phalanx in the thumb (often producing a triphalangeal thumb with thumb clinodactyly) is far more likely to be syndromic than little-finger clinodactyly and should trigger a targeted screen. Key associations are Holt-Oram syndrome (cardiac septal defects), Fanconi anaemia, thrombocytopenia-absent-radius (TAR) syndrome, Blackfan-Diamond anaemia and Rubinstein-Taybi syndrome (broad thumbs). The exam point: a thumb (radial-ray) anomaly warrants cardiac and haematological work-up (echocardiography, full blood count/film, and chromosomal-breakage testing where Fanconi is suspected), not just a hand assessment.
Clinical Assessment

History
Key Questions:
- Age when deformity first noticed
- Progressive vs stable deformity
- Family history (autosomal dominant pattern)
- Functional limitations (overlapping, grip problems)
- Syndromic features (developmental delay, cardiac issues)
- Cosmetic concerns (patient/parent perspective)
Physical Examination
Inspection
- Angular deviation measurement (degrees)
- Affected digit(s) and direction of deviation
- Bilaterality
- Associated deformities (syndactyly, polydactyly)
- Radial vs ulnar deviation
- Rotational component
- Nail alignment
- Skin creases
- Down syndrome: Flat facial profile, single palmar crease
- Apert: Craniosynostosis, mitten hand
- Russell-Silver: Growth retardation, asymmetry
A thorough inspection provides the foundation for clinical assessment.
Measurement of Deformity
- Use goniometer with digit in extension
- Measure angle of deviation from longitudinal axis
- Document in degrees
- Compare with contralateral side if bilateral
- More accurate than clinical measurement
- Measure angle between proximal and distal phalanx longitudinal axes
- Use AP radiograph with hand flat
- Document progression over time if serial films
- Mild: Under 10 degrees (observation)
- Moderate: 10-30 degrees (observation vs surgery)
- Severe: Over 30 degrees (surgery usually indicated)
Differential Diagnosis
- Plane of Deformity
- Coronal (radioulnar)
- Key Distinguishing Feature
- Delta phalanx with C-shaped bracket epiphysis; little finger radial deviation
- Plane of Deformity
- Sagittal (flexion)
- Key Distinguishing Feature
- Fixed flexion at PIPJ, usually little finger; no bony wedge phalanx
- Plane of Deformity
- Volar-radial
- Key Distinguishing Feature
- Curvature of the little finger DISTAL phalanx; bilateral, adolescent females
- Plane of Deformity
- Coronal with shortening
- Key Distinguishing Feature
- GDF5-related shortening of index/middle phalanges with clinodactyly component
- Plane of Deformity
- No angulation (stiffness)
- Key Distinguishing Feature
- Congenital interphalangeal joint fusion; absent skin creases, no motion
- Plane of Deformity
- Coronal or sagittal
- Key Distinguishing Feature
- History of injury; normal physeal morphology, no bracket epiphysis
The threshold of 30 degrees is widely accepted as the point where surgical correction should be considered. Below 30 degrees, most clinodactyly is cosmetic with minimal functional impact and observation is appropriate. Over 30 degrees, there is increased risk of progressive deformity, overlapping digits, and functional impairment warranting surgical intervention.
Investigations
Radiographic Imaging
- AP hand: Essential - shows angular deformity and delta phalanx
- Lateral hand: Supplementary - may miss deformity in coronal plane
- Oblique: Sometimes helpful for bracket epiphysis visualization
-
Delta phalanx identification
- Triangular or wedge-shaped bone
- C-shaped or bracket epiphysis
- Best seen on AP view
-
Angular measurement
- Measure angle between adjacent phalanges
- Document severity
- Serial films to assess progression
-
Growth plate assessment
- Open vs closing physis (affects surgical options)
- Bracket configuration
- Physeal asymmetry
-
Adjacent structures
- Joint congruity
- Collateral ligament stress
- Rotation component
Additional Imaging
- Advanced imaging rarely needed: Plain radiographs sufficient in most cases
- CT scan: Reserved for complex deformities or preoperative planning
- MRI: Not routinely indicated
Other Investigations
- Genetic testing: Karyotype for Down syndrome
- Cardiac echo: Congenital heart disease in syndromes
- Developmental assessment: Global development evaluation
- Genetic counseling: Familial cases
- No additional testing required
- X-rays confirm diagnosis
- Monitor for progression
Management Algorithm
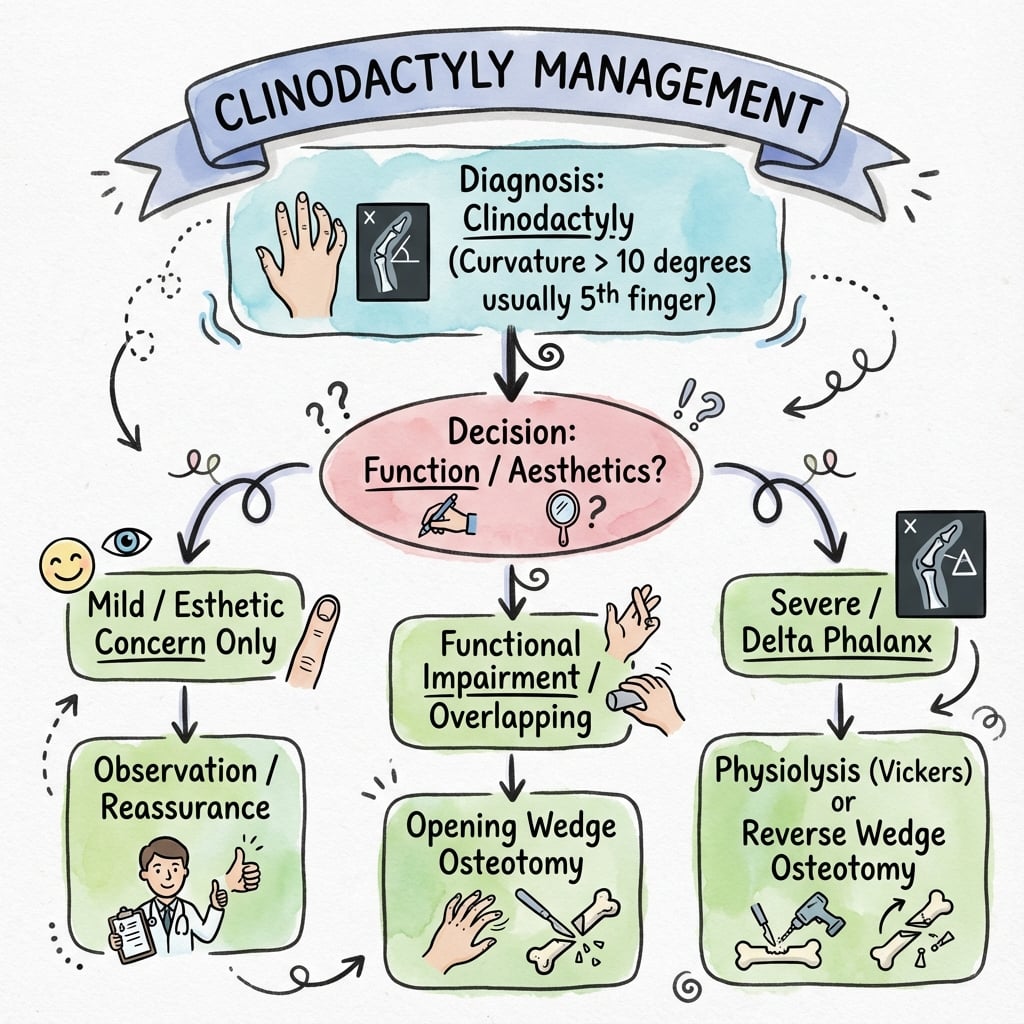
Treatment Decision Algorithm
Step 1: Measure Deformity
- Clinical and radiographic measurement
- Document degrees of angulation
- Assess functional impact
Step 2: Classify Severity
- Mild (under 10 degrees): Observation
- Moderate (10-30 degrees): Observation unless progressive or functional issues
- Severe (over 30 degrees): Consider surgery
Step 3: Assess Progression
- Compare serial radiographs if available
- If progressive (increasing deformity), lower threshold for surgery
- Stable deformity can be observed
Step 4: Evaluate Functional Impact
- Overlapping digits
- Grip interference
- Fine motor limitations
- Patient/parent cosmetic concerns
Step 5: Consider Age and Growth
- Under 4 years: Usually observe unless severe
- 4-6 years: Optimal surgical age if indicated
- Over 10 years: Still can operate, less remodeling potential
- Skeletal maturity: Closing wedge osteotomy preferred
Step 6: Surgical Decision
- Indications: Over 30 degrees OR progressive OR functional impairment
- Procedure: Opening wedge (young with open physis) vs physiolysis (very young)
- Timing: Age 4-6 years optimal
This algorithm guides individualized treatment decisions.
Physiolysis is reserved for YOUNG children (under 6 years) with substantial remaining growth. It works by excising the bracket epiphysis and allowing normal symmetric physeal growth to gradually correct the deformity. Opening wedge osteotomy is the most common procedure for ages 4-6 years, providing immediate predictable correction with bone grafting.
Surgical Technique
Opening Wedge Osteotomy Technique
- Age 4-6 years (most common)
- Angular deformity over 30 degrees
- Open growth plates with limited remaining growth
- Desire for immediate correction
- AP radiograph to measure deformity
- Calculate wedge angle needed
- Template correction
- Plan bone graft harvest site (iliac crest or olecranon)
-
Exposure
- Dorsal longitudinal incision over affected phalanx
- Identify and protect digital nerves (radial and ulnar)
- Incise periosteum longitudinally
- Elevate periosteum from bone
-
Osteotomy
- Create osteotomy at apex of deformity (usually mid-shaft)
- Use small sagittal saw or osteotome
- Create transverse cut perpendicular to long axis
- Incomplete osteotomy - leave hinge on concave (shorter) side
-
Opening Wedge
- Gently open osteotomy on long (convex) side
- Use small lamina spreader or osteotomes
- Open to templated angle
- Check alignment clinically and with fluoroscopy
-
Bone Grafting
- Harvest autograft (iliac crest or olecranon) OR use allograft
- Insert graft into wedge defect
- Ensure stable graft position
- Goal: Maintain correction and achieve union
-
Fixation
- Insert smooth K-wires (usually 2)
- Cross configuration for rotational stability
- Wires across osteotomy site
- Leave wires out through skin for later removal
- Alternative: Absorbable pins in young children
-
Closure
- Close periosteum over bone and graft
- Subcutaneous and skin closure
- Apply dorsal splint
- Maintain hinge on concave side for stability
- Avoid neurovascular injury - stay dorsal
- Adequate bone graft to fill defect
- Crossed K-wires prevent rotation
- Slight overcorrection acceptable (5-10 degrees)
Opening wedge provides immediate, predictable correction.
When performing opening wedge osteotomy, create an INCOMPLETE cut leaving a hinge on the concave (shorter) side. This provides stability and prevents overcorrection while allowing controlled opening of the wedge on the convex side.
Complications
Intraoperative Complications
- Neurovascular injury: Digital nerves at risk - stay dorsal, identify and protect
- Complete osteotomy: Loss of hinge - leads to instability
- Inadequate correction: Undercorrection - may need revision
- Overcorrection: Usually minor, can remodel
- Bone graft dislodgment: Ensure stable graft position
Early Postoperative Complications (under 6 weeks)
Infection/Dehiscence
- Wound infection: 1-2% incidence
- Dehiscence over K-wires
- Pin site infection
- Treatment: Local wound care, antibiotics
Loss of Fixation
- K-wire migration or breakage
- Loss of correction
- Rare with proper technique
- May require revision fixation
Rare but Serious
- Digital artery injury
- Compromise of digit perfusion
- Immediate recognition critical
- Urgent exploration if suspected
Late Complications (over 6 weeks)
- Incidence: 10-20% after physiolysis (higher than osteotomy)
- Causes: Incomplete physeal excision, growth recurrence
- Management: Observation vs revision osteotomy
- Rare: under 5% with adequate bone graft
- Risk factors: Inadequate graft, excessive motion
- Management: Revision grafting if symptomatic
- Undercorrection: Most common issue (10-15%)
- Overcorrection: Less common, usually minor
- Management: Revision osteotomy if severe, observe if mild
- PIPJ stiffness: 10-20% have some stiffness
- Usually mild: 10-20 degree loss
- Prevention: Early ROM after K-wire removal
- Management: Hand therapy, rare need for manipulation
- Physeal damage: Rare with careful technique
- Shortening: Expected with closing wedge (2-3mm)
- Angular deformity: From asymmetric growth arrest
Postoperative Care and Rehabilitation
Immediate Postoperative (0-4 weeks)
- Dorsal blocking splint
- Include MCPJ, PIPJ, and DIPJ of affected digit
- Buddy tape to adjacent digit for stability
- Elevate hand for first 48-72 hours
- K-wires left protruding through skin
- Pin site care: Clean with saline daily
- Monitor for infection signs
- Keep splint clean and dry
- Usually minimal pain after first 2-3 days
- Paracetamol or ibuprofen sufficient
- Ice therapy for swelling
Intermediate Phase (4-6 weeks)
- X-ray at 4 weeks to assess healing
- Check alignment maintenance
- Assess bone graft incorporation
- Usually 4-6 weeks postoperatively
- Once radiographic union evident
- Can remove in clinic (no anesthesia usually needed in cooperative child)
- Continue splinting part-time after removal
Late Phase (6 weeks to 3 months)
- Gradual weaning after K-wire removal
- Night splinting for additional 2-4 weeks
- Progressive return to activities
- Begin gentle active ROM after K-wire removal
- Focus on PIPJ and DIPJ motion
- Buddy tape during activities
- Hand therapy if significant stiffness
- Progressive strengthening at 8-10 weeks
- Age-appropriate activities
- Return to unrestricted activity at 12 weeks
Long-term Follow-up
- 3 months: Clinical and radiographic assessment
- 6 months: Assess final alignment and function
- Annual: Monitor through skeletal maturity for recurrence
- Skeletal maturity: Final assessment, discharge if stable
Outcomes and Prognosis
Expected Outcomes
- Correction: Excellent angular correction in over 90%
- Recurrence: Low (under 5%) with adequate technique
- Function: Minimal impact, good ROM
- Satisfaction: High patient/parent satisfaction
- Correction: Variable, 60-80% achieve satisfactory correction
- Recurrence: Higher (10-20%) than osteotomy
- Gradual: Correction occurs over 2-3 years
- May need secondary procedure: 15-20% require later osteotomy
- Mild deformity (under 30 degrees): Usually stable, good function
- Progression: 10-20% progress during growth spurts
- Functional impact: Minimal in most cases
- Satisfaction: Good for mild deformities
Prognostic Factors
- Good Outcome
- Moderate deformity (30-45 degrees)
- Poorer Outcome
- Severe deformity (over 60 degrees)
- Good Outcome
- 4-6 years
- Poorer Outcome
- Very young (under 3) or late (over 10)
- Good Outcome
- Opening wedge osteotomy
- Poorer Outcome
- Physiolysis (unpredictable)
- Good Outcome
- Autograft iliac crest
- Poorer Outcome
- No graft or inadequate graft
- Good Outcome
- Isolated clinodactyly
- Poorer Outcome
- Syndromic (may have other issues)
Functional Outcomes
- Range of Motion: Usually normal or near-normal (within 10 degrees of contralateral)
- Grip Strength: Not affected by surgery
- Fine Motor: Returns to baseline
- Cosmesis: Significant improvement, scar usually inconspicuous
- Patient Satisfaction: High (over 85% satisfied or very satisfied)
Long-term Prognosis
- Excellent prognosis for isolated clinodactyly with surgery
- Low risk of recurrence with opening wedge technique
- Normal hand function expected
- No increased risk of arthritis from surgery
- Psychosocial impact: Improved confidence with correction
Guidelines, Registries & Global Practice
Global Epidemiology
Clinodactyly is one of the most common congenital digital differences worldwide, though reported figures vary widely with diagnostic threshold (most series quote a 1-10% population frequency for mild deviation). Population-based registry data place congenital upper limb anomalies as individually rare but collectively a meaningful paediatric workload: in the Stockholm County cohort, 562 affected children were identified among 261,914 live births, with "deformations" (the Oberg-Manske-Tonkin subgroup that contains clinodactyly) accounting for 124 of 577 anomalies (Ekblom et al, J Hand Surg Am 2014).
- Reported value
- 1-10% (threshold-dependent)
- Source
- Clinical series consensus
- Reported value
- Majority of children affected
- Source
- Trisomy 21 phenotype literature
- Reported value
- Little (5th) finger, radial deviation, middle phalanx
- Source
- Operative series (Piper 2015; Ali 2009)
- Reported value
- 562 children / 261,914 births (Stockholm)
- Source
- Ekblom 2014 (PMID 24480684)
Classification & Guidance Framework
There is no single high-level society guideline (e.g. AAOS clinical practice guideline) dedicated to clinodactyly; management rests on classification frameworks and Level III-IV operative evidence. The table summarises the principal frameworks referenced internationally.
- Region
- International (IFSSH-endorsed)
- Role in clinodactyly
- Places clinodactyly within the malformation/deformation axis; current standard for congenital hand differences
- Evidence basis
- Registry-validated (Ekblom 2014, Level III)
- Region
- International
- Role in clinodactyly
- Earlier descriptive classification, now largely superseded by OMT
- Evidence basis
- Descriptive consensus
- Region
- UK
- Role in clinodactyly
- Paediatric congenital hand pathways; refer functionally/cosmetically significant cases to specialist congenital hand units
- Evidence basis
- Expert/pathway guidance
- Region
- USA
- Role in clinodactyly
- Surgeon education and operative principles for delta phalanx correction
- Evidence basis
- Expert/Level IV
- Region
- Europe
- Role in clinodactyly
- Continuing-education curricula and consensus on paediatric hand reconstruction
- Evidence basis
- Expert/consensus
Registry & Practice Variation
Dedicated arthroplasty-style registries do not exist for clinodactyly; the relevant evidence is from national congenital-anomaly and hand-surgery registries (e.g. Swedish registry data above) plus single-centre operative cohorts. Practice variation centres on procedure choice rather than indication threshold:
- Procedure selection varies by age and growth remaining: Vickers physiolysis (epiphyseal bracket resection with fat-graft interposition) is favoured in skeletally immature children, while opening or closing wedge osteotomy predominates nearer skeletal maturity. A comparative cohort found physiolysis achieved similar correction to osteotomy with fewer reoperations for deformity under 55 degrees (Gillis et al, Hand 2019).
- Surgical threshold is broadly consistent internationally: observation for mild/stable deformity, intervention for deformity greater than ~30 degrees, documented progression, or functional impairment (digital overlap, grip interference).
- Multidisciplinary syndromic screening is standard worldwide where clinodactyly is associated with Down syndrome or other syndromes, with genetic and developmental follow-up integrated into care.
Long-term follow-up through skeletal maturity to detect recurrence is standard practice across health systems, and telehealth has broadened access for serial radiographic and clinical monitoring of geographically remote families.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 5-year-old child with Down syndrome presents with bilateral small finger radial deviation. Radiographs show delta phalanx of middle phalanx with 35 degrees angulation. Parents are concerned about appearance. What is your management?”
“A 3-year-old child presents with small finger clinodactyly. Current deformity is 20 degrees on radiograph, but parent brings old X-ray from age 1 showing only 10 degrees. The deformity is clearly progressive. What is your recommendation?”
“You are performing opening wedge osteotomy for 40 degrees clinodactyly in a 5-year-old. After making the osteotomy, you open the wedge but the correction seems unstable. What are the potential issues and how do you manage?”
DEFINITION & PATHOANATOMY
- Angular deviation in CORONAL plane
- Delta phalanx = triangular bone
- C-shaped BRACKET epiphysis (2 sides)
- Normal physis = straight (1 side only)
- Asymmetric growth = progressive deformity
EPIDEMIOLOGY
- Incidence: 1-10% general population
- Down syndrome: Over 50%
- Small finger most common (radial deviation)
- Middle phalanx typical location
- Often bilateral (60-70%)
SURGICAL INDICATIONS
- Over 30 degrees angulation
- Progressive deformity (documented on X-rays)
- Functional impairment (overlap, grip)
- Significant cosmetic concern
- Age 4-6 years optimal for surgery
SURGICAL OPTIONS
- Opening wedge: Age 4-6, needs bone graft
- Physiolysis: Age under 6, unpredictable
- Closing wedge: Older child, no graft
- Bone graft: Iliac crest or olecranon
- Fixation: Crossed K-wires x 4-6 weeks
OPENING WEDGE TECHNIQUE
- Osteotomy at apex of deformity
- INCOMPLETE cut - hinge on concave side
- Open wedge on convex (long) side
- Bone graft to fill defect
- Crossed K-wires for stability
COMPLICATIONS
- Recurrence: 10-20% (physiolysis higher)
- Undercorrection: Most common issue
- Stiffness: 10-20% (usually mild)
- Nonunion: Under 5% with graft
- Neurovascular injury: Rare with technique
Evidence Base
- 13 digits in 9 children, all with more than 20 degrees pre-operative clinical angulation (mean 36 degrees)
- Significant improvement in clinical and radiographic angle (mean correction 32 degrees), maintained in 12 of 13 digits
- Pre-operative pain in 6 patients resolved in all post-operatively
- Three digits developed distal interphalangeal joint stiffness; one recurrence
- Comparative cohort of 30 digits (Vickers physiolysis) versus 11 digits (osteotomy)
- Physiolysis corrected angulation 43.0 to 23.9 degrees (46.2%); osteotomy 39.2 to 22.4 degrees (55.3%)
- More reoperations occurred in the osteotomy group; physiolysis had minimal complications
- Vickers physiolysis most effective for deformity of less than 55 degrees and isolated (non-syndactyly) clinodactyly
- 27 fingers in 22 patients treated by central epiphyseal (bracket) resection with fat-graft interposition, minimum 6-year follow-up
- Mean angle corrected from 38 degrees pre-operatively to 8 degrees at final follow-up (mean correction 79%)
- Residual deformity of less than 10 degrees - effectively full correction - in 15 of 27 fingers
- No patient required a later closing wedge osteotomy for insufficient correction
- 25 fingers in 17 patients, all with more than 25 degrees of angulation, treated by closing wedge osteotomy and K-wire fixation
- Clinical deformity corrected from a mean of 33 degrees to 9 degrees; radiographic from 29 degrees to 5 degrees
- Distal interphalangeal joint arc of motion essentially preserved (84 to 81 degrees)
- High parental satisfaction; recommended for moderate (15 to 30 degrees) and severe (over 30 degrees) deformity
- Population-based cohort of 562 children with congenital upper limb anomalies among 261,914 live births in Stockholm County (1997-2007)
- All anomalies could be organised within the Oberg, Manske and Tonkin (OMT) classification, now the international standard
- Deformations (which include clinodactyly) comprised 124 of 577 anomalies
- Registry data confirm congenital hand differences are individually rare but collectively a meaningful paediatric workload