Tailbone Injury | Coccydynia
Coccyx Injury Types
Critical Must-Knows
- Mechanism: Direct fall onto buttocks (sitting position). Childbirth. Repetitive trauma.
- Diagnosis: Clinical history and examination. X-ray confirms fracture/dislocation.
- Treatment: Conservative in vast majority. Cushion, NSAIDs, PT.
- Coccydynia: Persistent coccygeal pain. May require injections or, rarely, coccygectomy.
- Prognosis: Most resolve in 4-12 weeks. Small subset develop chronic pain.
Clinical Pearls
- "Most coccyx fractures are managed conservatively.
- "5F: Female, Fat, Forty, Fall, Fracture (risk factors for coccyx injury/coccydynia).
- "Dynamic lateral X-ray (Sitting vs Standing) can assess mobility.
- "Coccygectomy is reserved for refractory coccydynia.
Clinical Imaging
Imaging Gallery



Coccyx Fracture Pitfalls
Missed Other Injuries
Fall Assessment. A fall onto buttocks can also cause sacral fractures, vertebral compression fractures. Complete assessment.
Chronic Pain
Coccydynia. 10-20% develop chronic pain. Warn patients. May need injections or surgery.
Don't Order Routine X-ray
Limited Utility. X-ray often not needed if history is clear. Clinical diagnosis.
Surgery is Rare
Coccygectomy. Reserved for truly refractory cases after 6-12 months of failed conservative treatment.
At a Glance: Coccyx Injury
| Feature | Details |
|---|---|
| Mechanism | Direct fall onto buttocks, Childbirth |
| Pain Location | Tailbone (Sacrococcygeal junction) |
| Diagnosis | Clinical +/- X-ray |
| Treatment | Cushion, NSAIDs, Time |
| Chronic Pain | Coccydynia (10-20%) |
5F5 F's of Coccydynia
| F | Female 5x more common in women |
| F | Fat Obesity is a risk factor |
| F | Forty Peak age 40-50 |
| F | Fall Direct trauma mechanism |
| F | Fracture/Dislocation Injury pattern |
| F | Female 5x more common in women | F | Fall Direct trauma mechanism |
| F | Fat Obesity is a risk factor | F | Fracture/Dislocation Injury pattern |
| F | Forty Peak age 40-50 |
Hook:Risk factors for coccyx problems.
CRANKConservative Treatment
| C | Cushion Donut or wedge cushion for sitting |
| R | Rest Avoid prolonged sitting |
| A | Analgesia NSAIDs, Paracetamol |
| N | No Constipation Stool softeners to reduce straining |
| K | Keep Moving Gentle activity. Avoid bed rest. |
| C | Cushion Donut or wedge cushion for sitting | N | No Constipation Stool softeners to reduce straining |
| R | Rest Avoid prolonged sitting | K | Keep Moving Gentle activity. Avoid bed rest. |
| A | Analgesia NSAIDs, Paracetamol |
Hook:Conservative coccyx care.
Sit vs StandDynamic X-ray
| S | Sitting Lateral X-ray in sitting position |
| V | Versus Compare to... |
| S | Standing Lateral X-ray in standing position |
| S | Sitting Lateral X-ray in sitting position |
| V | Versus Compare to... |
| S | Standing Lateral X-ray in standing position |
Hook:Assess coccygeal mobility.
Overview and Epidemiology
Definition: Coccyx fractures and coccydynia (coccyx pain) result from trauma to the tailbone (coccyx). The coccyx is the terminal segment of the spine, formed by 3-5 fused vertebrae.
Epidemiology:
- Sex: 5x more common in females (shorter, more curved coccyx).
- Age: Peak 40-50 years.
- Risk Factors: Obesity, Female, Direct trauma, Childbirth.
Mechanisms:
- Direct Fall: Sitting position. Most common.
- Childbirth: Traumatic delivery. Coccyx can sublux or fracture.
- Repetitive Trauma: Cycling, Rowing.
- Idiopathic Coccydynia: Pain without clear trauma (often postural/degenerative).
Anatomy and Pathophysiology
Anatomy:
- Coccyx: 3-5 fused vertebral segments. Articulates with sacrum at Sacrococcygeal Joint.
- Attachments: Gluteus Maximus, Coccygeus, Levator Ani, Anococcygeal Ligament.
- Mobility: Normally has some flexion/extension at sacrococcygeal joint.
Pathophysiology:
- Acute Injury: Direct impact causes fracture or dislocation of coccyx.
- Inflammation: Local swelling and pain.
- Healing: Most heal with fibrous union over weeks to months.
- Chronic Coccydynia: Persistent pain due to:
- Malunion with abnormal angulation.
- Hypermobility or instability at sacrococcygeal joint.
- Degenerative changes.
- Referred pain (L5/S1, Sacroiliac).
Classification
Injury Types
- Fracture: Break in coccygeal segment.
- Dislocation: Displacement at sacrococcygeal or intercoccygeal joint.
- Fracture-Dislocation: Combined.
Distinction rarely changes management.
Clinical Assessment
History:
- Mechanism: Fall? Childbirth? Gradual onset?
- Pain: Worse with sitting (especially on hard surfaces), Leaning back, Defecation.
- Duration: Acute vs Chronic.
Physical Examination:
- Inspection: Bruising over sacrococcygeal area.
- Palpation: Point tenderness over coccyx (external). Tenderness on bimanual palpation (PR/PV combined with external).
- Coccygeal Mobility: Assess with PR exam. Pain with manipulation?
- Neurological Exam: Usually normal (coccyx does not contain cord).
- Rectal Exam: Exclude rectal pathology.
Differential Diagnosis
Pain localised to the tailbone is not always coccygeal in origin. The most important task is to separate true coccydynia from referred or sinister pathology before committing to long-term coccyx-directed treatment.
Differential Diagnosis of Coccygeal / Tailbone Pain
| Condition | Distinguishing Features | Key Discriminator |
|---|---|---|
| Coccyx fracture / coccydynia | Pain worse sitting and on standing up; point tenderness over coccyx; trauma or childbirth history | Reproduced by direct coccygeal palpation +/- dynamic radiograph lesion |
| Sacral insufficiency / stress fracture | Older osteoporotic patient or athlete; tenderness over sacrum not coccyx | MRI marrow oedema; H-shaped uptake on bone scan (Honda sign) |
| Pilonidal disease | Midline natal-cleft sinus/pits, discharge, abscess; soft-tissue not bony pain | Visible sinus openings and induration in natal cleft |
| Perirectal / anorectal pathology | Abscess, fissure, proctalgia fugax; pain with defecation, anal not coccygeal tenderness | PR exam and anoscopy; no bony coccygeal tenderness |
| Referred lumbosacral pain (L5/S1, SIJ) | Radicular leg symptoms, positive SIJ provocation; coccyx non-tender | Normal coccygeal palpation; positive root/SIJ tests |
| Presacral / sacrococcygeal tumour (chordoma, GCT) | Insidious unrelenting pain, night pain, neurological signs, mass on PR | MRI mass; do not attribute persistent atypical pain to benign coccydynia |
Red Flags - Do Not Miss
Persistent atypical coccygeal pain without clear trauma, night pain, a palpable presacral mass on rectal examination, or neurological signs mandate MRI to exclude chordoma or other sacrococcygeal tumour before labelling pain as benign coccydynia.
Investigations
Imaging (Often Not Needed):
- Clinical Diagnosis: If history is clear (fall, tailbone pain), imaging may not change management.
If Imaging Performed:
- Lateral X-ray (Coccyx): Shows fracture, dislocation, angulation.
- Dynamic Lateral X-rays: Sitting vs Standing. Assess mobility (greater than 25 degrees = Hypermobility).
- MRI: Rarely needed. For persistent pain (exclude tumor, infection).
Rule Out:
- Sacral fracture (if significant trauma).
- Pilonidal disease.
- Rectal pathology.
Management Algorithm
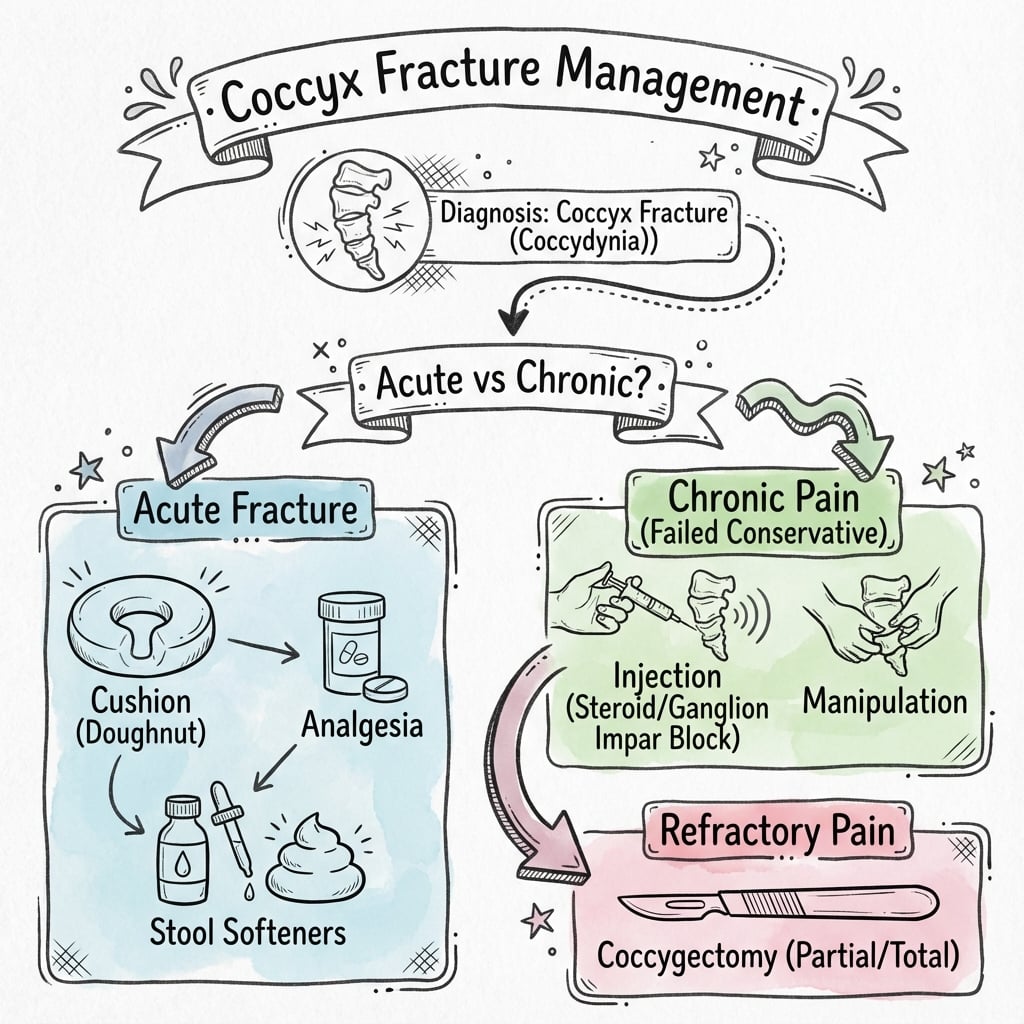
Conservative (Standard)
- Cushion: Donut or wedge cushion. Reduces pressure on coccyx when sitting.
- Analgesia: NSAIDs (first line). Paracetamol. Opioids rarely needed.
- Stool Softeners: Reduce straining during bowel movements.
- Activity Modification: Avoid prolonged sitting on hard surfaces.
- Physiotherapy: Pelvic floor exercises. Manual therapy.
- Time: Most resolve in 4-12 weeks.
90% resolve with conservative care.
Surgical Technique
Coccygectomy Technique
- Position: Prone (jack-knife or flat).
- Prophylaxis: Antibiotics. Bowel prep not usually needed.
- Incision: Midline longitudinal over coccyx.
- Dissection: Incise periosteum. Dissect subperiosteally. Identify sacrococcygeal joint.
- Excision: Divide at sacrococcygeal joint (or leave most proximal segment). Remove coccyx.
- Closure: Close periosteum if possible. Layered closure. Avoid dead space.
- Post-op: Wound care. Avoid sitting directly on wound.
Standard midline approach with careful subperiosteal dissection.
Complications
Complications
| Complication | Risk Factor | Management |
|---|---|---|
| Chronic Coccydynia | Severe injury / Malunion | Injections / Coccygectomy |
| Wound Infection (Post-op) | Proximity to anus | Antibiotics / Washout |
| Rectal Injury (Surgery) | Dissection error | Primary repair |
| Hematoma/Seroma | Inadequate hemostasis | Drainage |
| Persistent Pain (Post-op) | Nerve irritation | Reassurance / Injections |
Postoperative Care
After Coccygectomy:
- Wound care (close to anus - risk of infection).
- Avoid direct sitting on wound for 2-4 weeks (cushion).
- Antibiotics if infection concern.
- Stool softeners.
- Return to normal activity: 4-6 weeks.
Outcomes
- Conservative: 90% resolve in weeks to months.
- Coccygectomy: 70-90% significant improvement in refractory cases.
- Chronic Coccydynia: Minority have persistent issues.
Evidence Base
Dynamic Radiographs Define Coccydynia Lesions
- 208 consecutive coccydynia patients imaged standing then in the painful sitting position.
- Two culprit lesions on dynamic films: posterior luxation and hypermobility; BMI determined lesion type (posterior luxation 51% in obese vs 3.7% in thin patients).
- Recent trauma (under 1 month) raised the instability rate from 55.6% to 77.1%; protocol identified the culprit lesion in 69.2% of cases.
Treatment Manipulation Outcomes by Coccyx Mobility
- Randomised pilot of three manual treatments (levator ani massage, joint mobilisation, levator stretch) in coccydynia.
- Overall satisfactory results in only 25.7% at 6 months and 24.3% at 2 years.
- Patients with a normally mobile coccyx fared best; an immobile coccyx had the poorest results.
Coccydynia: Aetiology and Conservative Treatment
- Five-year prospective trial of 120 patients; cause is a localised musculoskeletal abnormality, not lumbosacral disc prolapse.
- Physiotherapy of little help; local corticosteroid plus anaesthetic injection helped 60%.
- Injection combined with manipulation cured about 85%; coccygectomy needed in almost 20% with over 90% success.
Viva Scenarios
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
The Fall on Ice
"What is your diagnosis and management?"
MCQ Practice Points
Mechanism
Q: What is the most common mechanism for coccyx fractures? A: Direct fall onto buttocks (sitting position).
Treatment
Q: What is the first-line treatment for acute coccyx fractures? A: Conservative - Cushion (donut or wedge), NSAIDs, Activity modification, Stool softeners.
Chronic Pain
Q: What percentage of coccyx injuries develop chronic coccydynia? A: 10-20%.
Dynamic X-ray
Q: What does dynamic lateral X-ray assess? A: Coccygeal mobility. Greater than 25 degrees movement between sitting and standing indicates hypermobility.
Surgery
Q: What is the surgical treatment for refractory coccydynia? A: Coccygectomy - Excision of the coccyx. Reserved for failures of 6-12 months of conservative treatment and injections.
Controversies & Areas of Uncertainty
Coccydynia is a low-evidence field: most data are retrospective, outcome measures are inconsistent, and no high-quality RCT compares the modern treatment ladder head-to-head.
Value of Routine Imaging
Whether plain films change acute management is debated. In a clear traumatic history with isolated coccygeal tenderness, radiographs rarely alter conservative care; imaging is most useful for chronic or atypical pain to classify the lesion or exclude tumour.
Dynamic Radiograph Threshold
The "greater than 25 degrees" cut-off for hypermobility (and posterior subluxation) derives from a small number of cohorts; normal mobility varies widely and the threshold is not universally validated. Use as a guide, not an absolute rule.
Injection vs Surgery Sequencing
Ganglion impar block and corticosteroid injection have only very-low-certainty evidence, yet are routinely used before coccygectomy. Whether interventions meaningfully delay or prevent surgery, versus simply postponing definitive treatment, is unresolved.
Partial vs Total Coccygectomy
Whether to excise the whole coccyx or leave the proximal segment, and the role of newer non-destructive techniques (radiofrequency, shockwave), lacks comparative trial data; practice is surgeon-dependent.
Guidelines, Registries & Global Practice
Global epidemiology
- Coccydynia accounts for under 1% of all back-pain presentations; true incidence is unknown because most cases never reach secondary care.
- Female predominance roughly 5:1, attributed to a shorter, more posteriorly angled coccyx and obstetric trauma; peak age 40-50 years (per Maigne and Wray cohorts).
- Obesity and very low BMI are both risk factors via altered sitting mechanics (Maigne 2000).
Guideline & society positions (side-by-side)
How Major Bodies Frame Coccyx Injury / Coccydynia
| Body / Source | Imaging Stance | Treatment Emphasis |
|---|---|---|
| General trauma teaching (AO / fracture principles) | Isolated coccyx fracture is a clinical diagnosis; image to exclude sacral or pelvic-ring injury if mechanism warrants | Non-operative; coccyx fractures essentially never need acute fixation |
| UK practice (BOA/NICE low-back-pain framing) | Avoid routine radiographs for non-specific tailbone pain; reserve imaging/MRI for red flags | Conservative stepwise care; refer refractory pain to spine/pain services |
| Spine/pain literature (Global Spine J SR 2021) | Dynamic sit-stand radiographs to classify chronic cases | Stepwise ladder: conservative then injection/RFT/ESWT then coccygectomy |
| Interventional pain (RA&PM meta-analysis 2026) | Fluoroscopy/US-guided block of the ganglion impar | Non-neurodestructive ganglion impar block before surgery (very-low-certainty evidence) |
Registry note
- There is no dedicated coccyx implant/arthroplasty registry (no implant involved). The largest pooled outcome dataset comes from spine registries and systematic reviews (e.g. DaneSpine data within the Global Spine J review) rather than a single national registry.
High- vs limited-resource practice variation
- Well-resourced settings: ready access to MRI for red-flag exclusion, fluoroscopy/ultrasound-guided ganglion impar blocks, radiofrequency and shockwave therapy, and specialist coccygectomy in selected centres.
- Limited-resource settings: diagnosis is clinical; treatment centres on cushioning, NSAIDs, stool softeners, activity modification and physiotherapy. Injections and surgery are reserved for the rare refractory case referred to a regional centre. The good prognosis of conservative care makes this entirely appropriate for most patients worldwide.
Clinical summary
5 F's
- •Female (5x more common)
- •Fat (obesity is risk factor)
- •Forty (peak age 40-50)
- •Fall (direct trauma mechanism)
- •Fracture/Dislocation pattern
Treatment
- •Cushion (Donut/Wedge) for sitting
- •NSAIDs for pain control
- •Stool Softeners to reduce straining
- •Activity modification (avoid hard chairs)
- •Time heals most (4-12 weeks)
Chronic Coccydynia
- •Dynamic X-ray (sitting vs standing)
- •Hypermobility: greater than 25° movement
- •Ganglion Impar block first-line
- •Coccygectomy for failures after 6-12 months
- •70-90% success with coccygectomy
Key Numbers
- •90% conservative success rate
- •70-90% surgery success rate
- •10-20% develop chronic coccydynia
- •10-15% wound infection post-op
- •4-12 weeks typical recovery