Mild Traumatic Brain Injury in Athletes
- Sport-related concussion is a traumatic brain injury induced by BIOMECHANICAL FORCES - a direct blow to the head, face or neck, or a blow elsewhere with force transmitted to the head - that produces TRANSIENT neurological impairment; it is a FUNCTIONAL disturbance rather than a structural injury, so standard CT and MRI are typically NORMAL, and loss of consciousness is NOT required (it occurs in only a minority).
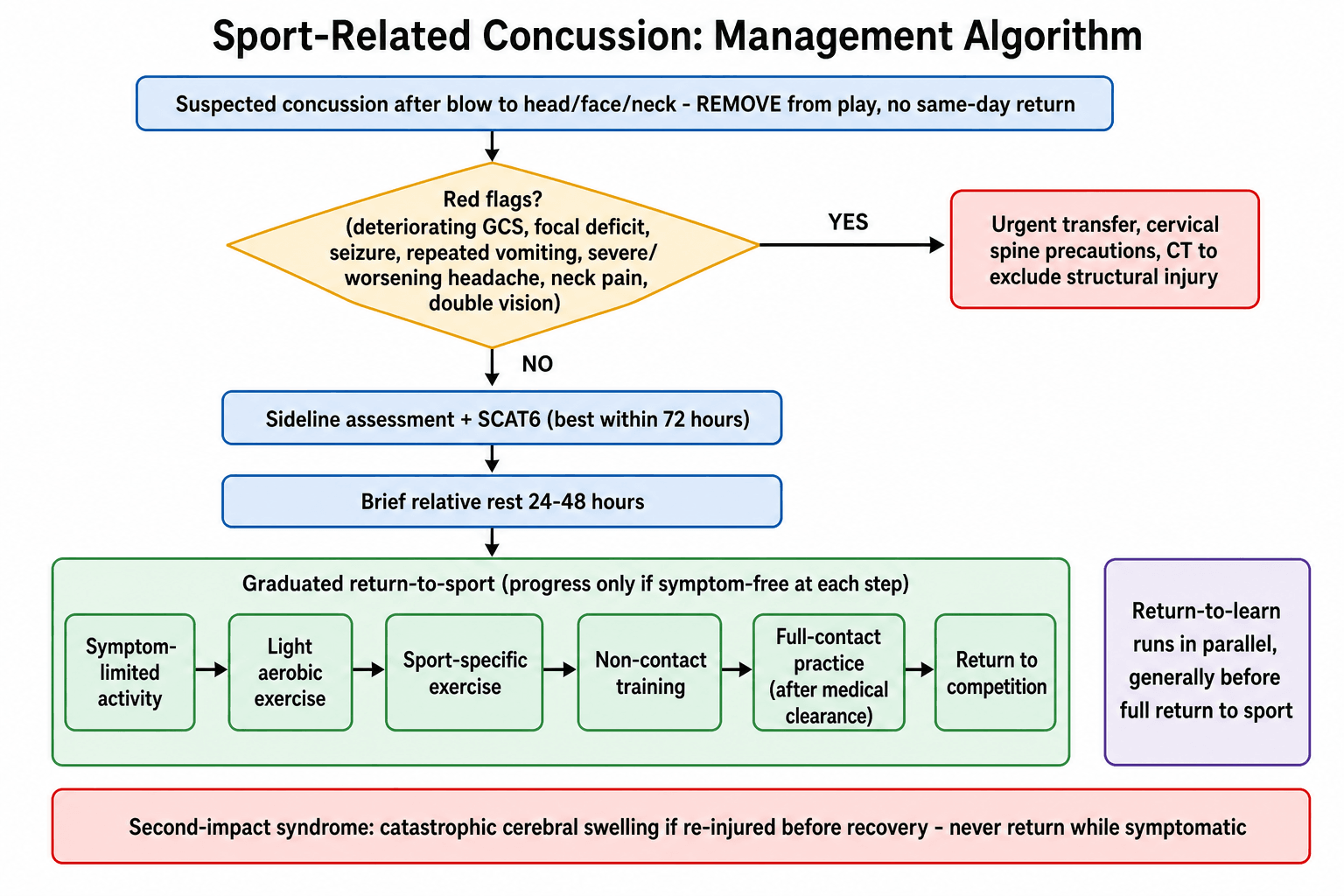
- The IMMEDIATE priority is to REMOVE the athlete from play - the principle is 'if in doubt, sit them out' - with NO SAME-DAY RETURN to play once concussion is suspected, because returning while symptomatic risks worsening injury; a sideline assessment is performed and the athlete monitored, with a brief initial period (about 24-48 hours) of relative physical and cognitive rest before gradually and progressively increasing activity as tolerated.
- ASSESSMENT uses structured tools: a sideline screen and the SCAT6 (Sport Concussion Assessment Tool), which discriminates concussed from non-concussed athletes best within 72 hours of injury with diminishing utility up to 7 days, and is NOT a stand-alone return-to-play test; cognition, balance/postural stability and the oculomotor/cervical/vestibular system are assessed, and serial evaluation tracks recovery.
- RED FLAGS that mandate urgent assessment and CONSIDERATION OF CT (to exclude a structural injury such as a haematoma) include a deteriorating conscious level/GCS, focal neurological deficit, seizure, repeated vomiting, severe or worsening headache, increasing confusion or agitation, neck pain/tenderness, or double vision - concussion is a clinical diagnosis once structural injury is excluded.
- Recovery is managed with a stepwise, criteria-based GRADUATED RETURN-TO-SPORT strategy (progressing through stages from symptom-limited activity and light aerobic exercise to sport-specific training, non-contact then full-contact practice, and finally return to competition) and a parallel RETURN-TO-LEARN pathway; progression occurs only if there is no symptom recurrence at each step, and medical clearance is required before full-contact return.
- The serious RISKS that drive cautious management are SECOND-IMPACT SYNDROME (a rare but catastrophic diffuse cerebral swelling after a second head injury sustained before recovery from the first), PERSISTENT post-concussive symptoms, and the long-term concern of repeated head injury (including chronic traumatic encephalopathy); guidelines (the Concussion in Sport Group consensus) provide the framework, and protocols should be sport-specific and kept up to date - particularly in high-incidence collision/combat sports.
- “Sport-related concussion = FUNCTIONAL TBI from biomechanical force; transient impairment; normal CT/MRI; LOC NOT required.
- “REMOVE from play - 'if in doubt, sit them out'; NO same-day return. Assess with SCAT6 (best within 72h; not a stand-alone RTP test). Red flags (deteriorating GCS, focal deficit, seizure, repeated vomiting, neck pain) -> CT.
- “Stepwise GRADUATED return-to-sport + return-to-learn (progress only if symptom-free; medical clearance before full contact). Beware SECOND-IMPACT SYNDROME and repeated injury.
Suspected concussion -> remove from play, no same-day return. Sideline assessment; watch red flags (deteriorating GCS, focal deficit, seizure, repeated vomiting, neck pain) -> CT.
Functional injury (normal CT/MRI). Assess with SCAT6; brief rest then a graduated return-to-sport and return-to-learn - progress only if symptom-free.
Definition, Immediate Management & Assessment
Sport-related concussion is a traumatic brain injury from biomechanical forces (a direct or transmitted blow) causing transient neurological impairment; it is a functional, not structural, injury, so standard CT/MRI are normal and loss of consciousness is not required. The immediate priority is to remove the athlete from play - 'if in doubt, sit them out' - with no same-day return, a sideline assessment, and monitoring, followed by a brief (about 24-48 hour) period of relative physical and cognitive rest then graduated activity. Assessment uses the SCAT6 (best within 72 hours, diminishing to 7 days; not a stand-alone return-to-play test), evaluating cognition, balance and the oculomotor/cervical/vestibular system. Red flags
- deteriorating GCS, focal deficit, seizure, repeated vomiting, severe/worsening headache, neck pain, double vision - mandate urgent assessment and consideration of CT to exclude a structural injury.
The Neurometabolic Cascade: Why a Normal Scan Still Means an Injured Brain
Concussion is a metabolic injury, and the cascade explains almost every clinical rule that follows — why the imaging is normal, why there is a vulnerable window, and why rest is brief rather than absolute.
- Mechanical force stretches axons and depolarises neurons, causing indiscriminate release of excitatory neurotransmitters, principally glutamate. Glutamate acting on NMDA receptors opens channels and produces a massive efflux of potassium and influx of calcium and sodium.
- The pumps fight back. The Na⁺/K⁺-ATPase works far above baseline to restore ionic gradients, and that costs ATP. The brain responds with a short burst of hyperglycolysis — glucose hypermetabolism — in the first minutes to hours.
- Supply falls exactly as demand rises. Cerebral blood flow decreases at the same time, so demand and delivery are uncoupled. This mismatch is the energy crisis at the heart of concussion.
- Calcium then poisons the mitochondria. Accumulated intracellular calcium impairs oxidative metabolism, so the early hypermetabolism gives way to a prolonged hypometabolism lasting days to weeks, alongside axonal injury — neurofilament compaction and disrupted axonal transport without frank transection.
- This is the "window of vulnerability". While metabolism is uncoupled the brain tolerates a second insult extremely poorly, which is the physiological basis of second-impact syndrome and the reason a graduated, symptom-guided return exists at all rather than an arbitrary time-based one.
- It also explains the imaging. The abnormality is ionic, metabolic and axonal at a microstructural level, well below the resolution of CT or conventional MRI — so a normal scan is the expected finding, and never evidence against the diagnosis.
- And why early light activity now beats strict rest. Prolonged inactivity worsens deconditioning, mood and symptom focus, whereas sub-symptom-threshold aerobic exercise appears to help restore autonomic and cerebrovascular regulation — the reason guidance moved from "rest until asymptomatic" to a brief 24–48 hours of relative rest followed by graded activity.
Graduated Return & Risks
- Graduated return-to-sport (stepwise): symptom-limited activity -> light aerobic exercise -> sport-specific exercise -> non-contact training drills -> (after medical clearance) full-contact practice -> return to competition. Progress only if there is no symptom recurrence at each step; drop back a stage if symptoms return.
- Return-to-learn in parallel: a stepwise return to school/work/cognitive load, generally before full return to sport.
- Medical clearance is required before full-contact return.
- Beware second-impact syndrome: a rare but catastrophic diffuse cerebral swelling if a second head injury occurs before recovery from the first - the central reason no athlete returns while symptomatic.
- Watch for persistent symptoms (targeted rehabilitation - cervical, vestibular, autonomic) and counsel on the long-term concern of repeated head injury (including chronic traumatic encephalopathy); use sport-specific, up-to-date (Concussion in Sport Group) protocols.
- Name the current statement. The framework in use is the Amsterdam 2023 (6th) International Consensus Statement on Concussion in Sport, which superseded Berlin 2016 and introduced the current tool set — SCAT6 and Child SCAT6 for the acute phase, SCOAT6 for office assessment beyond 72 hours, and the CRT6 for non-clinicians on the sideline. Citing the current statement by name, and knowing that the tools are versioned to it, is a small thing that reads as current practice.
Two principles are non-negotiable in sport-related concussion. First, NO SAME-DAY RETURN to play once concussion is suspected, and progression through the graduated return-to-sport steps only when symptom-free, because returning while symptomatic risks worsening injury and, rarely, the catastrophic second-impact syndrome - 'if in doubt, sit them out'. Second, concussion is a clinical diagnosis of a FUNCTIONAL injury, so before settling on it the clinician must exclude a STRUCTURAL injury: red flags such as a deteriorating conscious level, focal neurological deficit, seizure, repeated vomiting, severe or worsening headache, or neck pain mandate urgent assessment and CT (and cervical-spine evaluation). Manage recovery with the graduated return-to-sport and return-to-learn strategy, require medical clearance before full-contact return, and use up-to-date, sport-specific protocols, especially in high-incidence collision and combat sports.
What Is Actually in the SCAT6 (and the Office Tools)
- The SCAT6 is a multimodal ACUTE tool with an immediate on-field screen - the observable signs, the Maddocks questions (orientation/memory: ground, half, opponent, last score), the Glasgow Coma Scale and a cervical-spine check - and an off-field office portion: a symptom checklist (number and severity of symptoms), a cognitive screen (orientation, immediate memory using a 10-word list to reduce the ceiling effect of the old 5-word list, concentration with digits-backward and months-in-reverse, and delayed recall), a balance/neurological exam (the modified Balance Error Scoring System and tandem gait), and an oculomotor/cervical screen.
- It is not a diagnosis or a clearance test: it supplements clinical judgement, is ideally compared with a baseline, and has maximal utility within 72 hours (diminishing to 7 days).
- Continuing/office assessment: beyond the acute window use the SCOAT6 (Sport Concussion Office Assessment Tool) for sub-acute follow-up, and the Child SCAT6 / Child SCOAT6 for younger children (around ages 8 to 12); data remain limited in young children, women and diverse populations.
The SCAT6 = on-field screen (Maddocks questions, GCS, cervical spine) + office portion (symptom checklist, cognition with a 10-word list/digits-backward/delayed recall, mBESS + tandem gait, oculomotor/cervical). It supplements judgement (not a stand-alone diagnosis/clearance), is best within 72 hours, and is followed sub-acutely by the SCOAT6 (and Child versions).
Who Recovers Slowly: Modifiers, Persistent Symptoms and Active Rehab
- The expected course and the definition: most concussions resolve within about 2 weeks in adults and about 4 weeks in children/adolescents; symptoms persisting beyond that window are persisting post-concussion symptoms.
- Modifiers that predict prolonged recovery: a high initial symptom burden, previous concussions, a personal/family history of migraine or headache, pre-existing anxiety/depression or other mental-health problems, learning disability/ADHD, female sex, younger (adolescent) age, and prominent acute dizziness/vestibular or neck symptoms.
- The management shift - active rehab, not prolonged rest: strict/prolonged "cocoon" rest can worsen recovery, so after only a brief initial relative rest, begin early sub-symptom-threshold aerobic exercise and targeted, active rehabilitation - cervical physiotherapy, vestibulo-ocular rehab, and treatment of headache, mood and sleep - within a multidisciplinary approach, rather than waiting passively.
Most concussions settle by ~2 weeks (adults) / ~4 weeks (children); beyond that is persisting post-concussion symptoms. Predictors: high symptom load, prior concussions, migraine, mental-health history, ADHD/learning disability, female sex, younger age, early vestibular/neck symptoms. Treat with early sub-threshold aerobic exercise + targeted cervical/vestibular rehab - prolonged strict rest harms.
Mnemonics & Memory Aids
HEADS
Hook:HEADS: Hold them out, Exclude structural injury, Assess with SCAT6, Don't rush (graduated return), Second-impact syndrome.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A player takes a blow to the head and seems dazed. How do you manage the suspected concussion on the sideline?”
“Describe the return-to-sport process after concussion and the main risks.”
Evidence & Key Studies
Acute evaluation of sport-related concussion and the SCAT6 (systematic review)
- The Sport Concussion Assessment Tool (SCAT) discriminates concussed from non-concussed athletes, with maximal utility within the first 72 hours of injury and diminishing utility up to 7 days.
- The SCAT has limited utility as a return-to-play tool beyond 7 days, supporting its use in the acute phase as part of (not a substitute for) clinical assessment; more challenging cognitive tests (e.g. 10-word list) were recommended for the SCAT6.
- Acute assessment spans cognition, balance/postural stability and oculomotor/cervical/vestibular function; data are limited in young children, women and diverse populations.
Return-to-play protocols after sport-related concussion across international sporting organisations
- The Concussion in Sport Group (CISG) consensus provides the scientific basis for managing sport-related concussion, including a graduated return-to-play protocol.
- Across organisations, return-to-play protocols have a similar number of steps and each requires at least one medical examination before clearing an athlete, but vary in the initial rest period and time to complete the protocol.
- Sport-specific guidelines aligned with the latest consensus, updated regularly, are recommended - especially in combat sports with a high incidence of head injury.
The role and time-window of the SCAT/SCAT6 (best within 72 hours, diminishing to 7 days, not a stand-alone return-to-play test) and the assessment domains come from the cited Echemendia systematic review; the graduated return-to-play framework, the requirement for medical examination before clearance, the variation across organisations, and the recommendation for up-to-date sport-specific protocols (especially in high-incidence combat sports) from the cited Prock study. The definition (a functional injury with normal structural imaging, LOC not required), the 'if in doubt, sit them out' / no-same-day-return rule, the red flags for CT, the return-to-learn pathway, and second-impact syndrome are standard, well-established teaching (aligned with the Concussion in Sport Group consensus). (See also our Cervical Spine Injury and Burners and Stingers topics.)