Flexed-Adducted Thumb from Extensor Deficiency
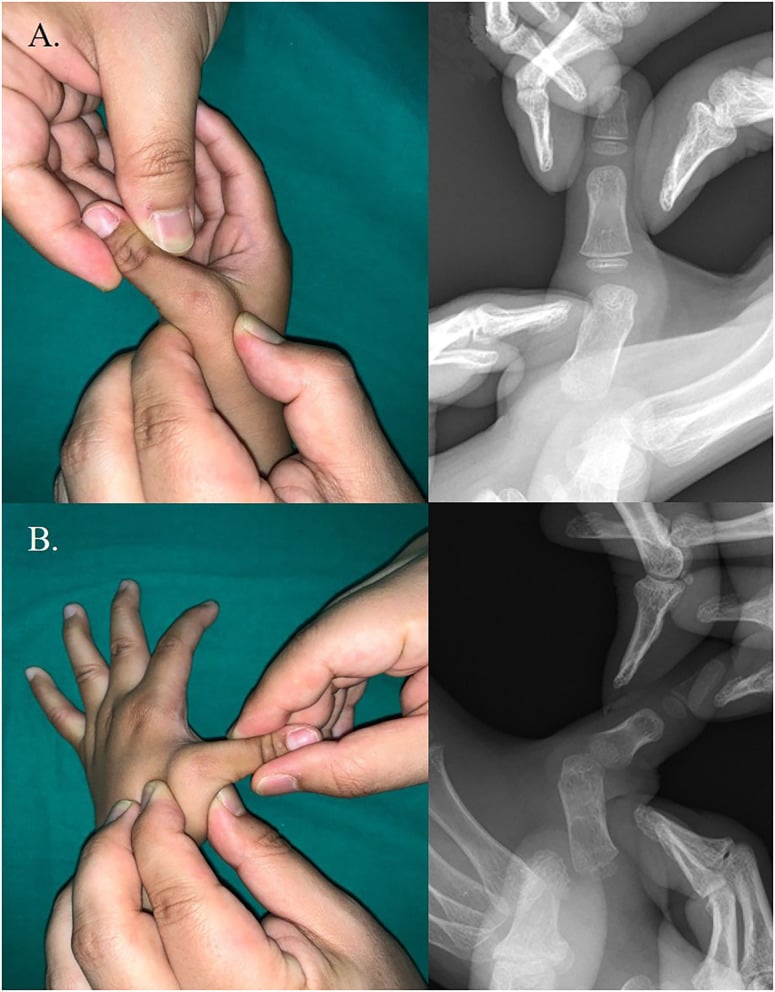
- Congenital clasped thumb is a congenital, often PROGRESSIVE, FLEXION and ADDUCTION deformity in which the thumb is held flexed and adducted into the PALM, caused by a DEFICIENT or ABSENT EXTENSOR mechanism - typically a hypoplastic/absent extensor pollicis brevis, sometimes with extensor pollicis longus involvement - and it is frequently accompanied by FIRST-WEB-SPACE narrowing and metacarpophalangeal-joint LAXITY/instability.
- It must be distinguished from the normal infantile 'cortical thumb' (thumb-in-palm posture in the first few months that resolves) and from a congenital trigger thumb; persistence of the flexed/adducted posture beyond infancy, with an inability to actively extend the thumb, points to a true clasped thumb from extensor deficiency.
- CLASSIFICATION drives management and is fundamentally FLEXIBLE (supple) versus COMPLEX (rigid): the FLEXIBLE type is passively correctable (the thumb can be extended) and responds well to splinting, whereas the COMPLEX type is a fixed deformity, often with collateral/capsular and web contractures, thenar hypoplasia and associated anomalies, and usually requires surgery.
- ASSESSMENT includes a careful examination of active and passive thumb extension, the first web space, MCPJ stability (a STRESS TEST identifies MCPJ instability), thenar muscle development, and a search for associated anomalies and SYNDROMES (e.g. arthrogryposis and others), because the type and any associations change the treatment.
- EARLY SPLINTING is the FIRST-LINE treatment for the FLEXIBLE type, and the published results are good: in Lin's series of 11 infants (17 supple thumbs) an abduction-extension splint gave an EXCELLENT result in 15 of 17 thumbs and a good result in the other 2, and in Tsuyuguchi's 43-patient review EVERY patient in the group without contracture responded well to splinting. Both are small, single-centre and uncontrolled, and neither reports how many supple thumbs would have improved without any splint at all.
- A thumb held in the palm in the FIRST THREE MONTHS of life is a NORMAL posture - which is precisely why the diagnosis is usually delayed - so the deformity is judged after that, and bilateral adducted thumbs in a BOY with a large head, developmental delay or leg spasticity should prompt a search for X-linked L1CAM disease (the CRASH/MASA spectrum) rather than an isolated hand diagnosis.
- SURGERY is for the COMPLEX (rigid) type or thumbs that fail splinting, and is TAILORED to the deficient structures: restoring active extension with a TENDON TRANSFER (e.g. to augment/replace the extensors), RELEASING the FIRST-WEB contracture (e.g. Z-plasty/rotation flap), correcting flexor tightness (flexor pollicis longus lengthening where shortened), and STABILISING an unstable/lax MCPJ - the combination depends on the individual deformity.
- “Congenital clasped thumb = flexed + adducted thumb (in the palm) from DEFICIENT/ABSENT EXTENSORS (EPB +/- EPL), often with first-web narrowing + MCPJ laxity.
- “Classify FLEXIBLE (supple, passively correctable -> splinting works) vs COMPLEX (rigid, contractures/anomalies -> surgery). Distinguish from the normal infantile cortical thumb and trigger thumb.
- “Treatment: EARLY SPLINTING first (flexible) - 15 of 17 supple thumbs excellent in Lin's series; surgery for complex/resistant = tendon transfer (restore extension) +/- first-web release +/- FPL lengthening +/- MCPJ stabilisation, tailored to the deficiency.
- “Two syndromic traps: a thumb-in-palm in the first 3 months is NORMAL, and bilateral adducted thumbs in a BOY with hydrocephalus, spastic legs or delay = X-linked L1CAM disease (CRASH: Corpus callosum hypoplasia, Retardation, Adducted thumbs, Spastic paraplegia, Hydrocephalus; MASA is the milder end).
Passively (sometimes actively) correctable thumb. Early splinting (serial extension splints) is first-line and frequently successful.
Fixed deformity with collateral/web contractures, thenar hypoplasia, MCPJ laxity, associated anomalies/syndromes. Usually needs surgery - tendon transfer +/- web release +/- MCPJ stabilisation.
What It Is & How To Assess It
Congenital clasped thumb is a congenital, often progressive flexion and adduction deformity in which the thumb is held into the palm, caused by a deficient or absent extensor mechanism (hypoplastic/absent extensor pollicis brevis, sometimes also extensor pollicis longus), commonly with first-web narrowing and MCPJ laxity. Assess active and passive thumb extension (correctable = flexible; fixed = complex), the first web space, MCPJ stability (a stress test detects instability), thenar development, and look for associated anomalies/syndromes (e.g. arthrogryposis). Distinguish it from the normal infantile cortical thumb (resolves in the first few months) and from congenital trigger thumb.

The Named Classifications: Weckesser and McCarroll
- Weckesser classification (four groups). The original scheme divides congenital clasped thumb by cause and severity: Group I - deficient/absent extensors ONLY (supple, passively correctable - the commonest and most splint-responsive); Group II - extensor deficiency PLUS a fixed flexion contracture (collateral-ligament/volar-plate/skin contracture - not fully correctable); Group III - with thumb/thenar hypoplasia and associated anomalies; Group IV - miscellaneous (e.g. arthrogryposis, windblown hand).
- McCarroll classification (the functional split). The simplified, treatment-oriented scheme used throughout: Type 1 supple/flexible (passively correctable, extensor deficiency - splinting) versus Type 2 complex/rigid (fixed contractures, MCPJ instability, associated anomalies/syndromes - surgery).
- The link. Weckesser Group I maps to the flexible thumb; Groups II-IV map to the complex thumb - so the classification directs whether splinting alone can succeed.
Q: How is congenital clasped thumb classified?
A: The Weckesser scheme has four groups: I = extensor deficiency only (supple, splint-responsive - commonest); II = plus a fixed flexion contracture; III = with thumb/thenar hypoplasia and anomalies; IV = miscellaneous (arthrogryposis, windblown hand). The McCarroll functional split is simpler: Type 1 supple/flexible (passively correctable → splinting) vs Type 2 complex/rigid (contractures/instability/syndromes → surgery). Weckesser I maps to flexible; II-IV to complex.
Splinting Window and the Named Surgical Reconstructions
- The splinting window and protocol. A static/serial extension splint holds the thumb in extension and radial abduction, worn full-time (day and night) for at least a few months. It works best started EARLY - within the first few months of life, before a fixed grasp pattern develops - and the earlier it is begun, the higher the correction rate for a supple thumb; a delayed start or a rigid thumb responds poorly.
- Restoring extension. The classic transfer is the extensor indicis proprius (EIP) to the extensor pollicis longus; alternatives include a flexor digitorum superficialis (FDS) transfer (usually from the ring finger) or brachioradialis/palmaris longus with a graft.
- The other components. First-web release by a four-flap Z-plasty or dorsal rotation flap (with adductor / first-dorsal-interosseous release for a tight web); flexor pollicis longus lengthening for a tight flexor; and MCPJ stabilisation (capsulodesis/chondrodesis or collateral-ligament reconstruction) for an unstable joint.
Q: What are the splinting and surgical specifics for congenital clasped thumb?
A: Splinting = a static/serial extension splint holding the thumb in extension + radial abduction, worn full-time for at least a few months, started early (first months of life, before a fixed grasp pattern) - the earlier, the higher the success for a supple thumb. Surgery restores extension with an EIP-to-EPL transfer (or FDS/brachioradialis), releases the first web (four-flap Z-plasty ± adductor release), lengthens a tight FPL, and stabilises an unstable MCPJ (capsulodesis/chondrodesis).
The Syndrome Behind the Thumb - and What Splinting Actually Achieves
The hand deformity can be the visible end of an X-linked brain disorder. Mutations in L1CAM, the gene for the L1 cell-adhesion molecule, cause a spectrum whose severe end is remembered as CRASH - Corpus callosum hypoplasia, intellectual disability (R), Adducted thumbs, Spastic paraplegia and Hydrocephalus - with MASA (mental retardation, aphasia, shuffling gait, adducted thumbs) the milder end of the same condition. Because the gene sits on the X chromosome the severe phenotype is seen in boys. So in an infant with bilateral adducted thumbs, measure the head circumference and examine the legs and tone before committing to a purely hand diagnosis: hydrocephalus, leg spasticity or developmental delay alongside the thumbs should trigger neurology, imaging and genetic referral, and it changes what a family is told about the child's future far more than the thumb ever will.
A thumb lying in the palm during the first 3 months of life is the normal infantile posture - which is exactly why the diagnosis of a true clasped thumb is usually delayed. Judge the thumb after that window, on active extension, not on a snapshot posture in a newborn.
In Tsuyuguchi's review the supple group's deformity was attributed to predominance of the flexor muscles rather than a demonstrated absent extensor. So "deficient or absent EPB" describes the commonest finding, not a universal one - and it is part of why a supple thumb can be rebalanced by a splint at all.
Q: How well does splinting work, and what do the series not tell you?
A: Lin (1999) splinted 17 supple thumbs in 11 infants with a short opponens-type splint holding abduction and extension without blocking the wrist: 15 of 17 excellent, the remaining 2 good on the Weckesser grading. Tsuyuguchi (1985) reviewed 43 patients (75 hands) over 10 years - 42 hands splinted, 16 operated, and 17 simply observed - and all of the group without contracture responded to splinting, while 12 of 16 operated hands (severe or splint-resistant) achieved a satisfactory result. The caveat that matters: these are small, uncontrolled, single-centre series, 17 hands in Tsuyuguchi's cohort were followed with neither splint nor surgery, and no study compares splinting against simple observation - so the correct claim is that a supple thumb splinted early does very well, not that the splint is proven to be what corrected it.
Management Algorithm
- Flexible (supple)
- Correctable (thumb can be extended)
- Complex (rigid)
- Fixed - not passively correctable
- Flexible (supple)
- Mainly extensor deficiency
- Complex (rigid)
- Collateral/web contracture, thenar hypoplasia, MCPJ laxity, anomalies
- Flexible (supple)
- Early splinting (serial extension)
- Complex (rigid)
- Surgery (after assessment)
- Flexible (supple)
- Only if splinting fails
- Complex (rigid)
- Tendon transfer +/- first-web release +/- FPL lengthening +/- MCPJ stabilisation
- Flexible (supple)
- Less likely
- Complex (rigid)
- More likely (e.g. arthrogryposis)
- Early splinting (first-line, flexible type): serial/static extension splinting started in infancy and worn for a prolonged period can correct a supple clasped thumb and is frequently successful.
- Surgery (complex/rigid or splint-resistant), tailored to the deficiency:
- Tendon transfer to restore active extension (augment/replace deficient extensors).
- First-web release (Z-plasty/rotation flap) for web contracture.
- Flexor pollicis longus lengthening if the flexor is tight.
- MCPJ stabilisation for an unstable/lax joint.
- Assess for syndromes/anomalies before planning - they alter prognosis and technique.
The associations run in two directions. A rigid clasped thumb with contractures at other joints belongs to the arthrogryposis spectrum, which made up a third of the largest published cohort. A thumb that is small as well as clasped, with a deficient thenar mass and an unstable MCPJ, may be thumb hypoplasia rather than a clasped thumb, and that distinction changes the operation entirely. A fixed flexed interphalangeal joint with a palpable nodule is a trigger thumb, not this diagnosis. The wider framework for congenital differences of the hand sits in the congenital hand overview.
Two judgements matter in congenital clasped thumb. First, classify the thumb as flexible or complex, because a flexible (supple) clasped thumb often corrects with early extension splinting and should be given that chance before surgery - splinting started in infancy and continued for a prolonged period is frequently successful, whereas a delayed or rigid thumb is harder to correct. Second, do not treat the thumb in isolation: a complex, rigid clasped thumb is more likely to have associated contractures, MCPJ instability, thenar hypoplasia, and an underlying syndrome such as arthrogryposis, so a careful examination (including an MCPJ stress test) and a search for associated anomalies are essential, and the surgical plan must be tailored to exactly which structures are deficient rather than applying a single operation to every thumb.
Mnemonics & Memory Aids
CLASP
Hook:CLASP: Classify, Lacking extensors, Adducted/flexed thumb, Splint early, Procedures for the complex thumb.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“An infant holds the thumb flexed into the palm and cannot actively extend it. How do you assess and manage this?”
What it is
- Progressive thumb flexion + adduction (held in the palm)
- Deficient/absent extensor mechanism (EPB +/- EPL)
- Often first-web narrowing + MCPJ laxity
Assess / classify
- Flexible (passively correctable) vs complex (rigid)
- Examine web, thenar, MCPJ stability (stress test)
- Thumb in the palm before 3 months is NORMAL - judge after that, on active extension
- Distinguish from trigger thumb; check for syndromes (arthrogryposis - a third of the largest cohort)
- Bilateral adducted thumbs in a boy: head circumference, tone, delay - X-linked L1CAM (CRASH/MASA)
Management
- Flexible: early extension splinting (15 of 17 supple thumbs excellent, Lin; all group I responded, Tsuyuguchi)
- Complex/resistant: surgery tailored to the deficiency
- Tendon transfer (restore extension) +/- first-web release +/- FPL lengthening +/- MCPJ stabilisation
Evidence & Key Studies
Characteristics of congenital clasped thumb: a case report and literature review
- Congenital clasped thumb is a progressive flexion and adduction deformity, usually accompanied by first-web-space narrowing and metacarpophalangeal-joint laxity, presenting with heterogeneous abnormalities and syndromes.
- Treatment varies with the classification: a flexible type can be treated with splinting (which showed promising results), whereas a complex type is treated surgically.
- Accurate diagnosis through history, physical examination and a stress test for MCPJ instability, with appropriate classification, is essential for treatment.
Congenital clasped thumb: a review of forty-three cases
- 43 patients (75 hands) over 10 years in a single institution, mean follow-up 32 months, divided into group I without contracture (14 patients, 24 hands), group II with palmar-side contractures (14 patients, 21 hands) and group III with arthrogryposis multiplex congenita (15 patients, 30 hands) - so a third of this cohort was arthrogrypotic.
- 42 hands were splinted, 16 were operated and 17 were followed conservatively with neither splint nor surgery; all group I patients responded well to splinting, and the deformity in that group was attributed to predominance of the flexor muscles rather than a demonstrated absent extensor.
- Of the 16 hands operated for severe deformity or splint failure - palmar soft-tissue release, skin graft and extensor reconstruction - a satisfactory result was obtained in 12.
A simple splinting method for correction of supple congenital clasped thumbs in infants
- 11 infants with 17 supple-type congenital clasped thumbs treated with a short opponens-type splint holding the thumb in abduction and extension while deliberately leaving wrist movement free.
- Functional results were excellent in 15 of 17 thumbs and good in the remaining 2 on the Weckesser grading - the clearest denominator available for the claim that splinting a supple thumb works.
- The splint was easy to apply and could be refitted at each visit; the series is small, uncontrolled and has no observation-only comparison group.
CRASH syndrome: does it teach us about neurotrophic functions of cell adhesion molecules?
- Mutations in the L1 cell-adhesion molecule gene cause CRASH syndrome: corpus callosum hypoplasia, intellectual disability, adducted thumbs, spastic paraplegia and hydrocephalus.
- The condition is inherited and X-linked, so the adducted thumbs are a visible marker of a central nervous system disorder rather than an isolated hand anomaly.
- A later mouse model of L1 syndrome reproduces the same phenotype - hydrocephalus of varying severity, intellectual deficit, spasticity of the legs and adducted thumbs - confirming the thumb sits within that constellation (Loers 2021, PMID 33484186).
The description of congenital clasped thumb (a progressive flexion-adduction deformity with first-web narrowing and MCPJ laxity), the flexible-versus-complex classification driving treatment (splinting for the flexible type, surgery for the complex type), and the value of a stress test for MCPJ instability come from the cited Kim report. The splinting results (15 of 17 supple thumbs excellent) come from Lin; the cohort structure, the one-third proportion with arthrogryposis, the flexor-predominance mechanism in the supple group and the 12-of-16 surgical result come from Tsuyuguchi; the CRASH/MASA constellation and its X-linked L1CAM basis come from Zhang, with the phenotype confirmed in the Loers model. The underlying extensor (EPB/EPL) deficiency, the differential with the normal infantile cortical thumb and trigger thumb, and the tailored surgical options (tendon transfer, first-web release, FPL lengthening, MCPJ stabilisation) are standard, well-established teaching. No trial compares splinting with observation alone, and no series reports what proportion of supple clasped thumbs correct without any treatment, so neither figure is given here.