Congenital Forefoot Conditions
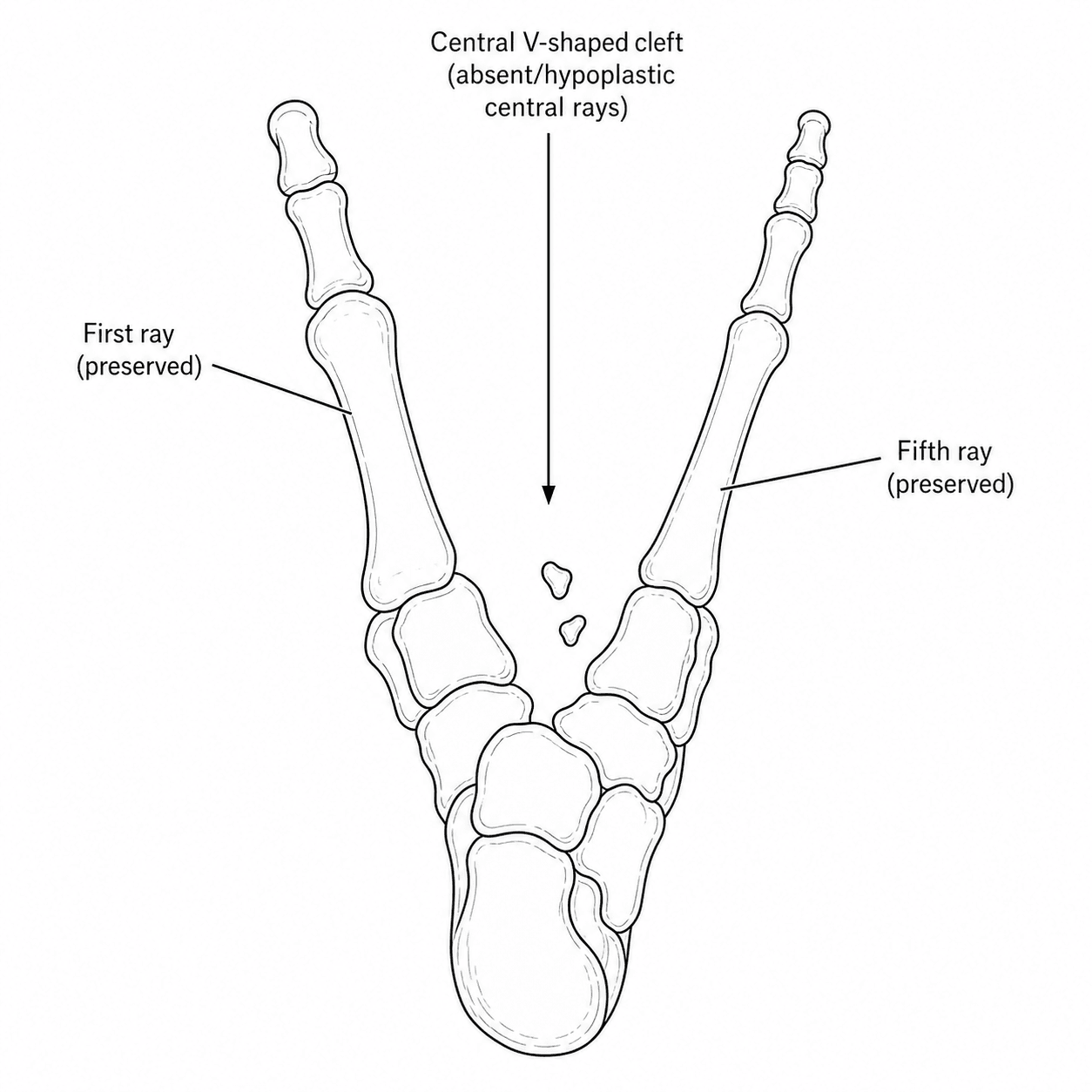
- CLEFT FOOT (split-foot malformation, ectrodactyly, the 'lobster-claw' foot) is a congenital CENTRAL-RAY deficiency: there is absence or hypoplasia of the central metatarsals and phalanges with a median cleft, frequently with syndactyly of the remaining rays, and the spectrum ranges from a mild central cleft to severe loss of multiple rays.
- It may occur in ISOLATION or as part of a SYNDROME, most notably ectrodactyly-ectodermal dysplasia-clefting (EEC) syndrome, and it is genetically heterogeneous (for example SHFM3 is associated with a 10q24 duplication); because of this, GENETIC COUNSELLING and assessment for associated anomalies (and the hands - split-hand/split-foot malformation) are important.
- MANAGEMENT of cleft foot is individualised and TAILORED to FUNCTION and APPEARANCE: many feet function and shoe reasonably well and need no surgery, while surgical reconstruction (cleft closure, syndactyly release, ray amputation/realignment, removal of ectopic bone, correction of associated deformity) is undertaken for difficulty with weight-bearing/footwear or for cosmesis - early recognition and tailored intervention optimise outcome.
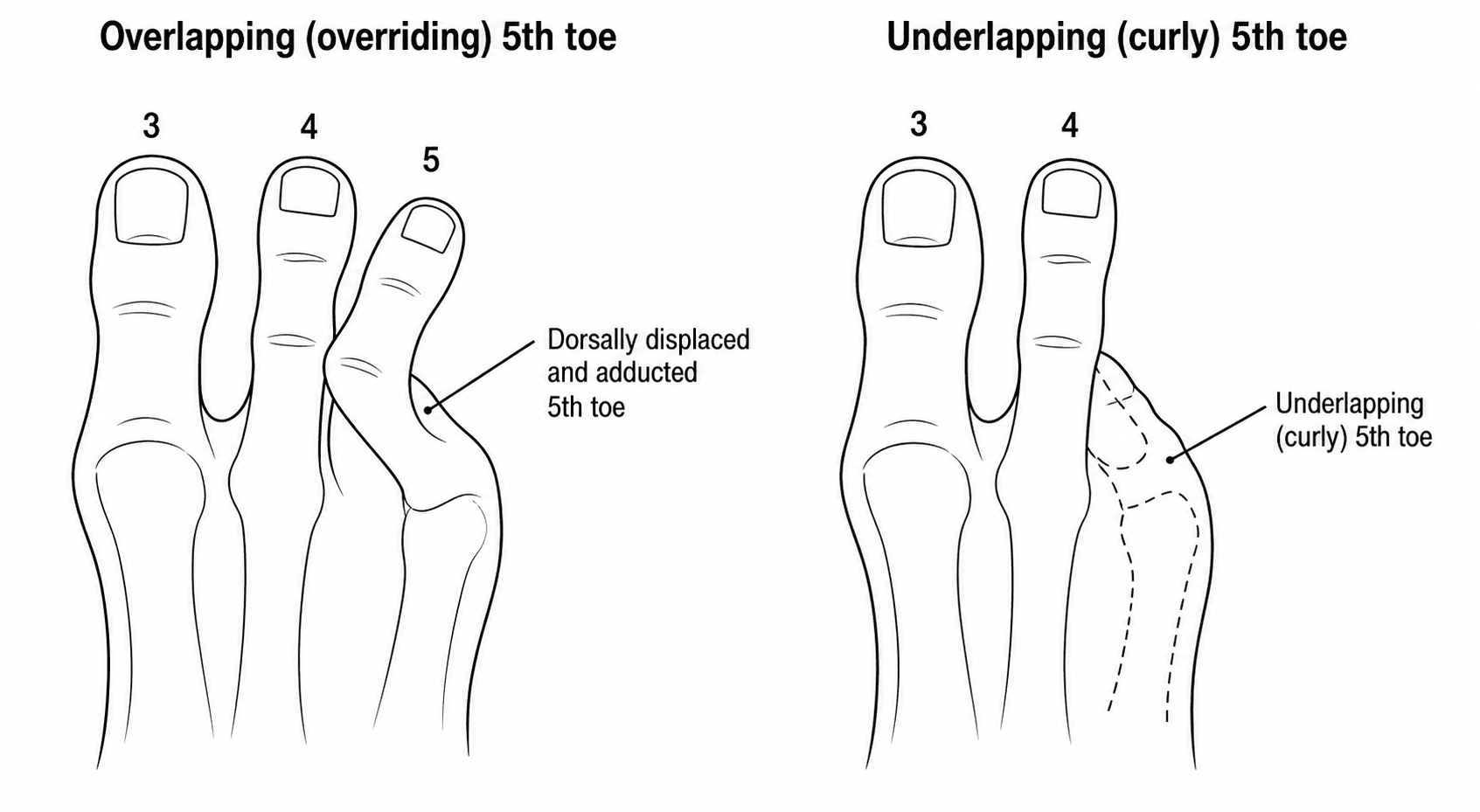
- The OVERLAPPING (congenital overriding) FIFTH TOE is a congenital deformity in which the proximal phalanx is DORSALLY SUBLUXATED and ADDUCTED at the fifth metatarsophalangeal joint, so the fifth toe overrides the fourth; it may be an asymptomatic parental concern or be PAINFUL and disabling with footwear - in children it often corrects with normal ambulation, so intervention is only for persistent symptomatic deformity.
- The UNDERLAPPING ('CURLY') FIFTH TOE is also congenital: the proximal phalanx is in VARUS with FLEXION at the metatarsophalangeal joint, frequently with a ROTATIONAL malalignment (supination/pronation judged by the nailbed), and it is usually noticed in infancy and commonly corrects with reassurance and benign neglect up to about age 6, with intervention reserved for persistent pain or footwear difficulty.
- TREATMENT of the fifth-toe deformities is NON-OPERATIVE first - strapping/splinting, accommodative footwear/shoe modification, padding/cushions and functional modification - with SURGERY (e.g. percutaneous flexor tenotomy, capsulotomy, soft-tissue rearrangement/syndactylisation, tendon transfer, osteotomy, phalangectomy or, rarely, amputation) reserved for symptomatic deformity persisting after non-operative measures; no single gold-standard procedure exists, so surgery is tailored to the specific pathology.
- “Cleft foot = central-ray deficiency (ectrodactyly/split-foot, 'lobster-claw'); ISOLATED or SYNDROMIC (EEC; SHFM3/10q24) - genetic counselling + check hands/associations. Surgery tailored to function/cosmesis.
- “Overlapping (overriding) 5th toe = proximal phalanx DORSAL + ADDUCTED at 5th MTP (overrides 4th); underlapping ('curly') 5th toe = proximal phalanx VARUS + FLEXION (rotational).
- “Fifth-toe deformities in children mostly correct/settle with reassurance (up to ~age 6) and non-operative care; surgery (tenotomy, capsulotomy, tendon transfer, osteotomy, phalangectomy) only for persistent symptoms - no gold-standard procedure.
Central-ray deficiency ('lobster-claw'); isolated or syndromic (EEC) - genetic counselling + check the hands/associations. Surgery tailored to function/cosmesis.
Overlapping (dorsal/adducted, overrides 4th) and underlapping/'curly' (varus/flexion). Mostly non-operative in children; surgery only for persistent symptoms.
Cleft Foot (Ectrodactyly / Split-Foot Malformation)
Cleft foot (split-foot malformation, ectrodactyly, the 'lobster-claw' foot) is a congenital central-ray deficiency - absence/hypoplasia of the central metatarsals and phalanges with a median cleft, often with syndactyly of the remaining rays. It may be isolated or part of a syndrome - notably ectrodactyly-ectodermal dysplasia-clefting (EEC) - and is genetically heterogeneous (e.g. SHFM3/10q24 duplication), so genetic counselling and assessment for associated anomalies (including the hands) are important. Management is tailored to function and appearance: many feet shoe and function reasonably and need no surgery, while reconstruction (cleft closure, syndactyly release, ray amputation/realignment, removal of ectopic bone) is for difficulty with weight-bearing/footwear or cosmesis.
Overlapping & Underlapping Fifth Toe
The overlapping (congenital overriding) fifth toe has the proximal phalanx dorsally subluxated and adducted at the 5th MTP joint, so the fifth toe rides over the fourth; it may be asymptomatic or painful with footwear. The underlapping ('curly') fifth toe has the proximal phalanx in varus with flexion, often with a rotational malalignment, and tucks under the adjacent toe. Both are congenital and, in children, commonly correct or settle with normal ambulation and reassurance (up to about age 6). Treatment is non-operative first - strapping/splinting, accommodative footwear, padding - with surgery (percutaneous flexor tenotomy, capsulotomy, soft-tissue rearrangement/syndactylisation, tendon transfer, osteotomy, phalangectomy, rarely amputation) reserved for persistent symptomatic deformity; there is no single gold-standard procedure, so surgery is tailored to the specific deformity.
- Overlapping (overriding)
- Dorsally subluxated + adducted at 5th MTP
- Underlapping ('curly')
- Varus + flexion at MTP (often rotational)
- Overlapping (overriding)
- Rides OVER the 4th toe
- Underlapping ('curly')
- Tucks UNDER the adjacent toe
- Overlapping (overriding)
- Often corrects with ambulation; treat if symptomatic
- Underlapping ('curly')
- Often corrects with reassurance up to ~age 6
- Overlapping (overriding)
- Strapping/splinting, shoe modification
- Underlapping ('curly')
- Accommodative shoes, cushions, functional modification
- Overlapping (overriding)
- Osteoclysis, tenotomy, capsulotomy, syndactylisation, tendon transfer, phalangectomy, amputation
- Underlapping ('curly')
- Flexor tenotomy, capsulotomy, tissue rearrangement, osteotomy, spur removal
Management Principles
- Cleft foot: assess for syndromic features (EEC) and associated anomalies including the hands; arrange GENETIC COUNSELLING; manage by tailoring to function and cosmesis - many need no surgery, others need reconstruction (cleft closure, syndactyly release, ray realignment/amputation).
- Fifth-toe deformities (children): reassure - most correct/settle with normal ambulation up to about age 6; non-operative measures (strapping/splinting, accommodative footwear, padding) first.
- Surgery for persistent symptomatic fifth-toe deformity: tailored to the pathology (flexor tenotomy, capsulotomy, soft-tissue rearrangement/syndactylisation, tendon transfer, osteotomy, phalangectomy, rarely amputation) - no single gold-standard procedure.
- Decide on symptoms/function, not appearance alone - intervene for pain and footwear difficulty (and significant cosmetic/functional concern), not for the radiograph or look in isolation.
Two judgements matter in these congenital forefoot conditions. For CLEFT FOOT, the foot is not the whole story: it may be part of a syndrome such as EEC and is often associated with split-HAND malformation and other anomalies, so the child needs assessment of the hands and associated systems and genetic counselling, and surgery should be tailored to function and appearance rather than performed reflexively (many cleft feet shoe and function well). For the FIFTH-TOE deformities, the key is patience: most overlapping and underlapping fifth toes in children correct or settle with normal ambulation and reassurance up to about age 6, so the default is non-operative management, and surgery is reserved for deformity that remains painful or causes footwear difficulty after non-operative measures - with the procedure tailored to the specific pathology, since no single operation is the gold standard.
Classifying Cleft Foot: Typical vs Atypical
Across the spectrum from a mild central cleft to severe loss of multiple rays, the classification that matters is the typical vs atypical distinction, which carries the inheritance and counselling implications:
- Typical cleft foot (true central-ray deficiency / SHFM). A central, V-shaped cleft from deficiency of the central ray(s), frequently bilateral, often with split-HAND involvement, and commonly familial (autosomal dominant with variable expressivity and incomplete penetrance - so a mildly affected parent may have a severely affected child). This is the form linked to the SHFM loci (e.g. SHFM3/10q24) and to EEC syndrome - the form for which genetic counselling is most relevant.
- Atypical cleft foot (now usually termed symbrachydactyly). A wider, U-shaped defect with more rays absent (sometimes a near-monodactylous foot), typically unilateral and sporadic (not inherited and not part of the SHFM genetic spectrum) - so the recurrence risk and counselling differ. Modern usage prefers "symbrachydactyly" over "atypical cleft."
- Grading severity. Foot-specific schemes grade by the number of remaining rays/metatarsals and the presence of transverse bones, which guides whether reconstruction (cleft closure, syndactyly release, ray realignment) or simply accommodative footwear is appropriate.
So the first classifying question - typical (central, often bilateral/familial, hand-associated) versus atypical/ symbrachydactyly (U-shaped, unilateral, sporadic) - directly shapes the genetic counselling. (The split-HAND counterpart and its Manske classification are covered in our Cleft Hand topic.)
Grading the foot itself. The named scheme is the Blauth and Borisch classification, which grades cleft foot by the number and morphology of the metatarsals remaining (from a foot with all five metatarsals present and only a soft-tissue cleft, through progressive central metatarsal absence, to a severely monodactylous foot). It is useful because the count, rather than the appearance of the cleft, is what predicts whether the foot needs nothing more than accommodative footwear or a genuine reconstruction.
Naming what you are looking for in EEC. "Assess for syndromic features" is only useful if you can say what they are. EEC is Ectrodactyly, Ectodermal dysplasia and Clefting, most often from a TP63 mutation:
- Ectodermal dysplasia - sparse fine hair, abnormal or absent teeth, dystrophic nails, dry skin and reduced sweating.
- Clefting - cleft lip and/or palate.
- Lacrimal duct obstruction - a characteristic and easily missed feature causing chronic tearing and recurrent eye infection; ask about it specifically.
- Genitourinary and renal anomalies - warranting a renal ultrasound.
- Conductive or sensorineural hearing loss - so arrange a hearing assessment.
Examine the hands in every cleft foot, and refer to clinical genetics: the inheritance is autosomal dominant with variable expressivity, so a parent with a trivially abnormal hand may not know they carry it.
Classify cleft foot as typical (central V-shaped cleft, often bilateral, familial AD with variable penetrance, hand-associated, linked to SHFM3/10q24 and EEC → genetic counselling) versus atypical / symbrachydactyly (U-shaped, more rays missing, unilateral and sporadic → different recurrence risk). The typical/atypical split is what drives the inheritance counselling.
The Named Operations for the Fifth-Toe Deformities
- The Butler procedure is the classic operation for the congenital overriding (overlapping) fifth toe: a double racquet-shaped (dorsal and plantar) incision around the base of the toe lets the extensor tendon and the dorsal MTP capsule be released so the toe is repositioned plantarward and into the corrected alignment, with the skin closure holding the new position. It corrects the deformity while preserving the toe (in contrast to amputation).
- Percutaneous flexor tenotomy is the simple, effective procedure for the flexible underlapping ('curly') toe - dividing the tight flexor digitorum longus (and brevis) through a tiny stab releases the flexion/ curl; it works well in children and avoids open surgery.
- Syndactylisation (suturing the fifth toe to the fourth, a Kelikian-type "buddy" procedure) is an option for a recurrent or unstable toe.
- Bone procedures - phalangectomy (removing the proximal phalanx) or a corrective osteotomy - and, rarely, amputation of the fifth toe are reserved for severe, recalcitrant or salvage situations.
- Choosing. Match the procedure to the pathology: a fixed dorsal-adduction overriding toe needs the soft-tissue release/repositioning of a Butler, whereas a flexible curly toe needs only a flexor tenotomy - consistent with there being no single gold-standard operation. (General lesser-toe and curly-toe surgery is covered in our Lesser Toe Deformities and Curly Toes topics.)
Name the operations: the Butler procedure (double racquet incision, extensor/capsular release and repositioning) for the overriding fifth toe; a percutaneous flexor tenotomy for the flexible curly/underlapping toe; syndactylisation for recurrence; phalangectomy/osteotomy or rarely amputation for salvage. Match the operation to the pathology - there is no gold-standard procedure.
Mnemonics & Memory Aids
CLEFT
Hook:CLEFT: Central-ray deficiency, Look for syndrome/split-hand, EEC/genetic counselling, Function/cosmesis-tailored surgery, Toe (5th) deformities mostly non-operative.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child has a 'lobster-claw' foot. What is it, and what is your approach?”
“How do you manage an overlapping and an underlapping fifth toe in a child?”
Cleft foot
- Central-ray deficiency (split-foot malformation / ectrodactyly, 'lobster-claw')
- Isolated or syndromic (EEC); genetically heterogeneous (SHFM3/10q24)
- Check the hands (split-hand) and associated anomalies; genetic counselling
Cleft foot management
- Tailored to function and appearance
- Many shoe/function well -> no surgery
- Reconstruction (cleft closure, syndactyly release, ray realignment/amputation) for footwear/weight-bearing/cosmesis
Fifth-toe deformities
- Overlapping (overriding): proximal phalanx dorsal + adducted at 5th MTP (over the 4th)
- Underlapping ('curly'): proximal phalanx varus + flexion (often rotational)
- Children: mostly correct/settle with ambulation + reassurance (up to ~age 6)
Fifth-toe management
- Non-operative first: strapping/splinting, accommodative footwear, padding
- Surgery for persistent symptoms (tenotomy, capsulotomy, tendon transfer, osteotomy, phalangectomy, amputation)
- No gold-standard procedure - tailor to the pathology
Evidence & Key Studies
Prenatal diagnosis & genetic counselling of split-hand/split-foot malformation (SHFM3, 10q24.3): case report & review
- Split-hand/split-foot malformation (SHFM, ectrodactyly) is a congenital limb malformation affecting the central rays, extending to syndactyly, median clefts of the hands/feet, and aplasia/hypoplasia of phalanges, metacarpals and metatarsals (the 'lobster-claw' appearance).
- It is clinically and genetically heterogeneous (e.g. SHFM3 associated with 10q24 duplication) and may be isolated or syndromic, making prenatal diagnosis and genetic counselling important.
- Genetic counselling helps plan and manage affected pregnancies and families.
Fifth toe deformities: overlapping and underlapping toe
- The overlapping (overriding) fifth toe has the proximal phalanx dorsally subluxated and adducted at the fifth MTP joint; in children it often corrects with normal ambulation, so intervention is only needed for persistent symptomatic deformity, with non-operative measures (strapping, splinting, shoe modification) first.
- The underlapping ('curly') fifth toe has the proximal phalanx in varus and flexion (often with rotational malalignment) and commonly corrects with reassurance up to about age 6; non-operative care is the mainstay.
- Surgery (osteoclysis, percutaneous tenotomy, capsulotomy, syndactylisation, tendon transfer, phalangectomy, amputation) is reserved for persistent pain/footwear difficulty, and no gold-standard approach exists - surgery should be tailored to the specific pathology.
The definition and genetic heterogeneity of cleft foot/split-foot malformation (central-ray deficiency, 'lobster-claw', SHFM3/10q24, isolated vs syndromic) and the importance of genetic counselling come from the cited Lai report (with the cited Raza case report illustrating function-and-cosmesis-tailored surgical management of ectrodactyly, PMID 41013550); the descriptions and management of the overlapping and underlapping fifth-toe deformities (largely non-operative in children with surgery for persistent symptoms, and no gold-standard procedure) from the cited Talusan review. The EEC syndromic association and the assessment of the hands/associated anomalies are standard, well-established teaching. (See also our Polydactyly/Syndactyly and Paediatric Foot Deformities topics.)