Amniotic Band Syndrome | Limb Constriction | Variable Severity | Z-Plasty Release
- Amniotic band syndrome: Fibrous bands constrict developing limbs in utero, causing deformities
- Variable severity: From simple constriction rings to complete amputation
- Patterson classification: Grades 1-4 based on severity and distal changes
- Z-plasty release: Standard surgical technique for constriction bands
- Not hereditary: Sporadic condition, not genetic
- “Viva question: Classify this constriction band using Patterson system
- “Distinguish from other congenital limb deformities (symbrachydactyly, radial club hand)
- “Z-plasty technique: Multiple Z-plasties to lengthen and break up constriction
- “Complications: Recurrence, vascular compromise, need for multiple procedures
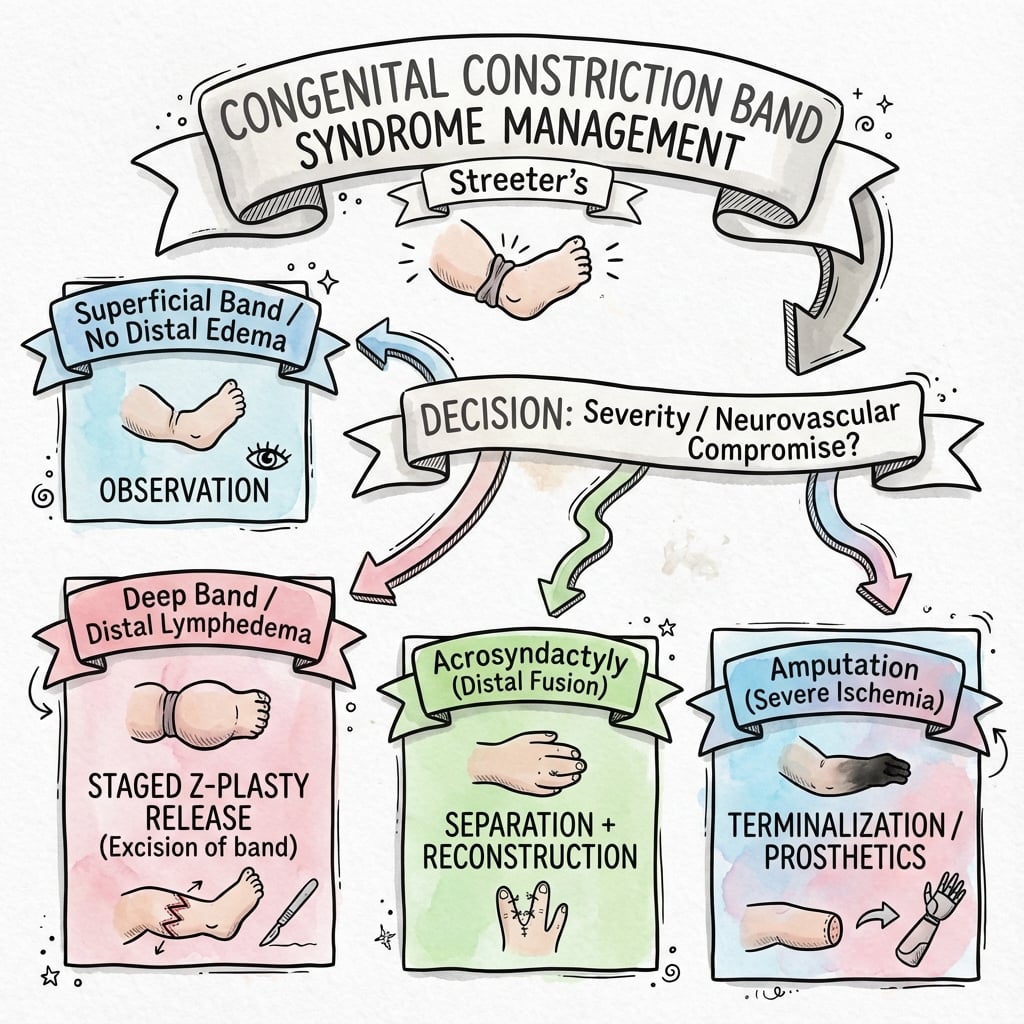
Grade 1-4 system based on severity. Grade 1 = simple ring, Grade 2 = ring with distal edema (URGENT release), Grade 3 = acrosyndactyly, Grade 4 = amputation. Classification guides urgency and surgical approach.
Not symbrachydactyly (missing central rays), not radial club hand (radial deficiency), not Poland syndrome (pectoralis absence). Constriction bands are asymmetric, irregular, and may affect multiple limbs.
Multiple Z-plasties are used to lengthen the constriction and break up the ring. Usually 2-4 Z-plasties around the circumference. Release must be complete to prevent recurrence and allow normal growth.
Grade 2 (with edema): Urgent release to prevent vascular compromise. Grade 1: Can wait until child is older (6-12 months) if no symptoms. Grade 3: Staged release and digit separation. Grade 4: No release needed, prosthetic fitting.
- Clinical Features
- Simple constriction ring, no symptoms
- Distal Changes
- None - normal distal limb
- Management
- Observe or Z-plasty if symptomatic
- Clinical Features
- Constriction ring with distal swelling
- Distal Changes
- Lymphedema, may have vascular compromise
- Management
- URGENT Z-plasty release
- Clinical Features
- Constriction with digit fusion
- Distal Changes
- Acrosyndactyly, webbed digits
- Management
- Staged release and separation
- Clinical Features
- Intrauterine amputation
- Distal Changes
- Missing distal segment
- Management
- Prosthetic fitting, no release
BANDConstriction Band Features - BAND
Hook:BAND syndrome - Bands are Asymmetric, Not hereditary, Distal changes vary!
RELEASEZ-Plasty Release - RELEASE
Hook:RELEASE the constriction - Release completely, Elevate flaps, Length gained, Edema resolves!
Overview and Epidemiology
Congenital constriction bands (also called amniotic band syndrome or constriction ring syndrome) is a condition where fibrous bands from the ruptured amnion constrict developing limbs or digits in utero, causing deformities ranging from simple constriction rings to complete intrauterine amputation.
Epidemiology:
- Reported prevalence varies widely with ascertainment — Australian population-based registries report 2.03 per 10,000 births (about 1 in 4,900; Bower 1993), while a UK tertiary series cited approximately 1 in 15,000 (Homer 2015). Higher figures (up to ~1 in 1,200) appear in older literature but reflect liveborn-only or less stringent case definitions.
- Sporadic condition — not hereditary or genetic; essentially no recurrence risk for future pregnancies (key counselling point)
- No sex predilection (equal male-to-female distribution in registry data)
- Risk associations: young maternal age (less than 25 years) and primiparity (Bower 1993, Syvanen 2021)
- Frequently multiple bands affecting more than one limb
- Most common on fingers, toes, arms, and legs; upper limb most frequently involved in surgical series
- Asymmetric, non-anatomical pattern (helps distinguish from genetic/longitudinal limb-deficiency conditions)
Congenital constriction bands can cause significant functional impairment and cosmetic concerns. Early recognition and appropriate classification (Patterson system) guides treatment urgency. Grade 2 bands with distal edema require urgent release to prevent vascular compromise and tissue loss. Understanding the classification system is essential for surgical planning.
Etiology:
- Ruptured amnion: Amnion tears early in pregnancy
- Fibrous bands: Amniotic bands wrap around developing limbs
- Constriction: Bands constrict blood flow and growth
- Variable severity: Depends on timing and tightness of constriction
- Not genetic: Sporadic, not inherited
- Maternal factors: Trauma, infection, drug use (controversial)
- Early amnion rupture: More severe if occurs early in pregnancy
- Multiple gestations: Slightly increased risk
- Most cases: No identifiable risk factor (idiopathic)
Natural History:
- Grade 1: Usually stable, may cause cosmetic concerns or mild functional limitations
- Grade 2: Progressive if not released - edema worsens, may lead to tissue loss
- Grade 3: Digits remain fused, need surgical separation
- Grade 4: No progression (already amputated), need prosthetic management
Clinical Presentation

Pathophysiology and Mechanisms
Pathophysiology
The Constriction Mechanism:
Amnion tears early in pregnancy (often first trimester):
- Amniotic fluid leaks, amnion separates from chorion
- Fibrous bands form from torn amnion
- Bands float in amniotic fluid and can wrap around developing fetus
- Constriction occurs as fetus grows
Severity depends on:
- Timing of amnion rupture (earlier = more severe)
- Tightness of band constriction
- Location of constriction (digits vs limb)
- Duration of constriction before birth
- May cause vascular compromise, lymphatic obstruction, or complete amputation
Effects of Constriction:
- Consequence
- Obstruction
- Clinical Finding
- Distal lymphedema (Grade 2)
- Consequence
- Compression
- Clinical Finding
- Venous congestion, swelling
- Consequence
- Severe compression
- Clinical Finding
- Tissue ischemia, amputation (Grade 4)
- Consequence
- Restriction
- Clinical Finding
- Distal hypoplasia, shortening
- Consequence
- Fusion
- Clinical Finding
- Acrosyndactyly (Grade 3)
Grade 2 constriction bands with distal edema indicate lymphatic obstruction and potential vascular compromise. These require urgent Z-plasty release to prevent progression to tissue loss or amputation. Do not delay surgery - the edema indicates active obstruction that may worsen.
The whole topic assumes the extrinsic (amniotic band) theory, but an examiner will expect you to name the classic two competing theories of amniotic band sequence:
- Extrinsic theory (Torpin): the dominant, widely accepted model. Early rupture of the amnion (with an intact chorion) exposes the fetus to mesodermic fibrous strands floating in the chorionic cavity; these mechanically entangle and constrict developing parts, producing rings, lymphoedema, acrosyndactyly and amputation. It explains the asymmetric, non-anatomical, "anything-anywhere" pattern and the negligible recurrence risk.
- Intrinsic theory (Streeter): proposes a primary germ-plasm/developmental defect (an intrinsic abnormality of the embryonic disc or a localised vascular disruption) that produces both the bands and the tissue defects, with the bands a by-product rather than the cause. It is invoked for cases with associated internal/visceral and CNS anomalies that are hard to explain by simple constriction.
- A vascular-disruption mechanism is often cited as a unifying contributor (compromised perfusion of the developing part).
- Terminology: the constellation is also called the ADAM complex (Amniotic Deformity, Adhesions, Mutilations) and "amniotic band sequence" - reflecting that the visible bands are one part of a wider sequence.
Exam point: lead with the extrinsic (Torpin) amniotic-rupture theory as the accepted explanation for the constriction/limb deformities, but be able to contrast it with Streeter's intrinsic theory (better explains associated internal/CNS defects) and know the synonym ADAM complex.
Classification Systems
Patterson Classification (Most Commonly Used)
- Description
- Simple constriction ring
- Distal Changes
- None - normal distal limb/digit
- Treatment
- Z-plasty if symptomatic, observe if mild
- Urgency
- Elective
- Description
- Constriction with distal lymphedema
- Distal Changes
- Swelling, venous congestion, may have vascular compromise
- Treatment
- URGENT Z-plasty release
- Urgency
- Urgent
- Description
- Constriction with distal fusion
- Distal Changes
- Acrosyndactyly (digits fused at tips), webbed
- Treatment
- Staged release and digit separation
- Urgency
- Elective but early
- Description
- Intrauterine amputation
- Distal Changes
- Missing distal segment (finger, toe, limb)
- Treatment
- Prosthetic fitting, no surgical release
- Urgency
- N/A
The Patterson classification directly determines treatment urgency and approach. Grade 1 can be observed or treated electively. Grade 2 requires urgent release. Grade 3 needs staged procedures. Grade 4 needs prosthetics, not release. Always classify before planning treatment.
GRADEPatterson Classification - GRADE
Hook:GRADE the constriction - Grade 1 is simple, Grade 2 is urgent, Grade 3 needs separation, Grade 4 is amputation!
Clinical Assessment
History:
- Prenatal history: Maternal trauma, infection, drug use?
- Birth history: Normal delivery? Any complications?
- Family history: Other congenital anomalies? (Usually negative - not genetic)
- Progression: Is constriction getting worse? (Grade 2 may progress)
- Symptoms: Pain, swelling, functional limitations?
- Multiple sites: Check all limbs and digits
- Distal swelling: Indicates Grade 2, needs urgent assessment
- Color changes: Blue/purple distal to band suggests vascular compromise
- Progressive constriction: May indicate active band tightening
- Multiple severe bands: May be part of more complex syndrome
Physical Examination:
Systematic Examination
- Constriction rings: Visible grooves or indentations around limb/digit
- Distal changes: Swelling (Grade 2), fusion (Grade 3), amputation (Grade 4)
- Color: Normal, pale, or blue/purple (vascular compromise)
- Multiple sites: Check all limbs, fingers, toes
- Asymmetric pattern: Helps distinguish from genetic conditions
- Band depth: Superficial or deep constriction
- Distal pulses: May be diminished in Grade 2
- Edema: Pitting edema distal to band (Grade 2)
- Temperature: Cool distal to band suggests vascular compromise
- Sensation: May be normal or decreased
- Distal joints: May have limited motion if constriction is tight
- Digit function: Assess grip, pinch if fingers affected
- Limb function: Assess overall function if arm/leg affected
- Capillary refill: Should be less than 2 seconds
- Pulses: Distal pulses may be diminished
- Doppler: If available, assess arterial flow
- Urgency: If vascular compromise suspected, urgent release needed
Grade 2 constriction bands with distal edema indicate active lymphatic obstruction and potential vascular compromise. These require urgent surgical consultation and Z-plasty release. Delaying treatment may lead to tissue loss or progression to amputation. Do not wait for scheduled clinic - arrange urgent assessment.
The classification and surgery above are limb-focused, but amniotic band sequence is a sequence, and the band that constricts a limb can entangle or be swallowed by other developing parts. A complete assessment of the affected newborn looks beyond the obvious ring:
- Atypical (non-anatomical) facial clefts: bands can cause oblique/transverse facial clefts that do NOT follow the normal embryological cleft-lip/palate lines - a key clue that a cleft is band-related rather than a typical orofacial cleft.
- CNS and cranial defects: encephalocele, anencephaly and asymmetric/atypical skull defects can occur when bands involve the head.
- Body-wall defects / limb-body-wall complex (LBWC): the severe end of the spectrum, with thoraco-abdominoschisis, scoliosis and short cord - usually lethal and distinct from isolated peripheral bands.
- Secondary deformities: bands proximally can produce a secondary (non-idiopathic) clubfoot or other postural deformities distal to the constriction, which behave and are treated differently from idiopathic clubfoot.
Exam point: in any baby with a constriction band, examine all limbs and the face/skull and trunk - the presence of atypical facial clefts, cranial defects or a body-wall defect both confirms the diagnosis (asymmetric, non-anatomical pattern) and signals a more severe sequence; isolated limb bands carry a far better prognosis than limb-body-wall complex.
Investigations
Imaging:
- AP and lateral views: Assess bone structure, any underlying anomalies
- Distal hypoplasia: May see shortened or underdeveloped bones
- Fusion: In Grade 3, may see bony fusion of digits
- Not diagnostic: Clinical diagnosis, X-rays confirm extent
- Vascular assessment: If Grade 2 with edema, assess arterial flow
- Lymphatic obstruction: May see dilated lymphatics
- Not routine: Usually clinical diagnosis sufficient
Other Investigations:
- Indication
- All cases
- Findings
- Constriction ring, distal changes
- Clinical Use
- Primary diagnostic method
- Indication
- All cases
- Findings
- Bone structure, hypoplasia, fusion
- Clinical Use
- Confirm extent, plan surgery
- Indication
- Grade 2 with edema
- Findings
- Arterial flow assessment
- Clinical Use
- Assess vascular compromise
- Indication
- If multiple anomalies
- Findings
- Usually normal (not genetic)
- Clinical Use
- Rule out syndromes
Congenital constriction bands are a clinical diagnosis. The presence of a constriction ring with or without distal changes is diagnostic. Imaging confirms the extent but is not required for diagnosis. The Patterson classification is based on clinical findings, not imaging.
Differential Diagnosis
The defining feature of amniotic band sequence is an acquired, asymmetric, non-anatomical constriction with normal proximal anatomy. Genuine longitudinal/transverse limb deficiencies are intrinsic developmental field defects and follow predictable anatomical patterns.
- Key Feature
- Circumferential groove with normal proximal limb
- Symmetry / Pattern
- Asymmetric, non-anatomical, often multiple limbs
- Discriminator from Bands
- Visible ring; distal lymphoedema, acrosyndactyly or amputation; sporadic
- Key Feature
- Short/absent central digits, often nubbins
- Symmetry / Pattern
- Unilateral, follows a developmental gradient
- Discriminator from Bands
- No constriction ring; transverse/central deficiency; Poland-spectrum association
- Key Feature
- Radial deviation, absent/hypoplastic radius and thumb
- Symmetry / Pattern
- May be bilateral; syndromic (VACTERL, TAR, Holt-Oram)
- Discriminator from Bands
- Longitudinal axis deficiency, not a ring; warrants systemic work-up
- Key Feature
- Fusion from the web base distally, normal length
- Symmetry / Pattern
- Often bilateral, familial, web extends proximally
- Discriminator from Bands
- Acrosyndactyly fuses only at the tips with a proximal fenestration; band syndactyly is sporadic
- Key Feature
- Cord or trunk involvement, major visceral defects
- Symmetry / Pattern
- Severe, often lethal
- Discriminator from Bands
- Bands extend beyond limbs; not isolated peripheral rings
The classic discriminator examiners probe: acrosyndactyly (Patterson Grade 3) shows distal-tip fusion with a proximal sinus/fenestration that a probe can pass through, reflecting an extrinsic band rather than a failure of separation. True congenital syndactyly fuses from the web space distally with no proximal opening. The presence of constriction rings elsewhere on the limb seals the diagnosis of amniotic band sequence.
Management Algorithm
Management by Patterson Grade
Treatment Protocol by Grade
Simple constriction ring, no distal changes:
- Observation: If mild and asymptomatic, may observe
- Z-plasty release: If constriction is deep, causing symptoms, or cosmetic concern
- Timing: Can wait until child is 6-12 months old (easier anesthesia)
- Technique: 2-4 Z-plasties around circumference to lengthen and break up ring
Constriction with distal lymphedema:
- URGENT Z-plasty release: Do not delay - edema indicates active obstruction
- Timing: Within days to weeks, depending on severity
- Technique: Complete release with multiple Z-plasties
- Post-op: Monitor for resolution of edema, may need compression
Constriction with acrosyndactyly:
- Stage 1: Z-plasty release of constriction bands
- Stage 2: Digit separation (usually 3-6 months later)
- Technique: Release bands first, then separate fused digits
- Multiple procedures: May need several stages for complex cases
Intrauterine amputation:
- No surgical release: Nothing to release - already amputated
- Prosthetic fitting: When child is ready (usually 12-18 months)
- Early fitting: Important for development and acceptance
- Psychological support: Family counseling about prosthetic options
Grade 2 constriction bands with distal edema require urgent surgical release. The edema indicates lymphatic obstruction that may progress to vascular compromise and tissue loss. Do not delay treatment - arrange urgent surgical consultation and release within days to weeks depending on severity.
Surgical Technique

Z-Plasty Technique (Standard for Constriction Bands)
Principle: Multiple Z-plasties around the circumference lengthen the constriction and break up the ring, preventing recurrence.
Z-Plasty Release Steps
Mark constriction ring: Identify the full extent of constriction Plan Z-plasties: Usually 2-4 Z-plasties around circumference Z-plasty design: 60-degree angles optimal for length gain (75% increase) Flap size: Adequate to ensure vascularity (usually 5-10mm limbs)
Incision: Make Z-plasty incisions through constriction ring Elevate flaps: Raise skin and subcutaneous tissue as flaps Preserve vascularity: Maintain adequate blood supply to flaps Release deep tissues: May need to release fascia if constriction is deep
Transpose flaps: Rotate flaps to interdigitate (Z-plasty pattern) Lengthen circumference: Z-plasty increases length by 75% (60-degree angles) Break up ring: Multiple Z-plasties prevent recurrence Ensure complete release: No residual constriction
Suture flaps: Close Z-plasty incisions Drains: Usually not needed Dressing: Non-constrictive, allow for swelling Splint: May use splint to protect repair
Z-plasty lengthens tissue by interdigitating triangular flaps. 60-degree angles provide 75% length gain. Multiple Z-plasties around the circumference ensure complete release and prevent recurrence. The technique breaks up the constriction ring while maintaining vascularity of the flaps.
Complications
- Incidence
- 5-10%
- Risk Factors
- Incomplete release, inadequate Z-plasties
- Management
- Revision Z-plasty
- Incidence
- Common in Grade 3-4
- Risk Factors
- Early constriction, growth restriction
- Management
- Accept or lengthening procedures
- Incidence
- Rare but serious
- Risk Factors
- Tight constriction, delayed release
- Management
- Urgent release, may need amputation
- Incidence
- Variable
- Risk Factors
- Severity, location, multiple bands
- Management
- Therapy, adaptive devices
- Incidence
- Common
- Risk Factors
- Visible constriction rings, amputations
- Management
- Reassurance, revision surgery if severe
Grade 2 bands can progress to Grade 4 if not treated. Distal edema indicates active obstruction that may worsen. Urgent release prevents progression to tissue loss or amputation. Do not delay treatment for Grade 2 constriction bands.
Postoperative Care and Rehabilitation
Postoperative Protocol
- Dressing: Non-constrictive, allow for swelling
- Elevation: If limb affected, elevate to reduce edema
- Wound care: Monitor for infection, keep clean and dry
- Splint: May use splint to protect repair
- Suture removal: 10-14 days post-operatively
- Scar management: Begin scar massage when healed
- ROM exercises: Gentle range of motion if joints affected
- Monitor: Check for recurrence, wound healing
- Scar management: Continue massage, silicone sheets if needed
- Functional therapy: If digits/limbs affected, occupational/physical therapy
- Monitor growth: Ensure normal growth distal to release
- Follow-up: Clinical assessment for recurrence
- Annual follow-up: Monitor for recurrence, growth
- Functional assessment: Ensure normal development
- Cosmetic concerns: Address if significant
- Additional procedures: If needed for Grade 3 separation or recurrence
Rehabilitation:
- Scar management: Essential to prevent contracture
- Functional therapy: If digits or limbs affected
- Adaptive devices: May be needed for severe cases
- Psychological support: Important for children and families
Outcomes
- Good to excellent results in 90-95% with appropriate Z-plasty release
- Recurrence rate 5-10% (usually from incomplete release)
- Functional outcomes depend on severity and location
- Grade 1: Excellent outcomes with release
- Grade 2: Good outcomes if released urgently
- Grade 3: Variable outcomes, may need multiple procedures
- Grade 4: Prosthetic outcomes generally good with early fitting
- Severity: Grade 1-2 have better outcomes than Grade 3-4
- Timing of release: Earlier release (especially Grade 2) has better outcomes
- Complete release: Incomplete release leads to recurrence
- Location: Fingers and toes generally have better outcomes than limbs
Early release of Grade 2 constriction bands prevents progression and improves outcomes. Delaying release allows edema to worsen and may lead to tissue loss. Grade 1 bands can be released electively, but Grade 2 requires urgent attention.
Guidelines, Registries & Global Practice
No formal society guideline (AAOS / BOA / NICE / EFORT) addresses amniotic band sequence specifically — the condition is too rare and heterogeneous for guideline development, and the evidence base is Level III-IV. Practice is therefore guided by classification (Patterson), case-series experience, and registry epidemiology rather than graded recommendations.
Global epidemiology and registry evidence:
- Region
- Australia
- Key Datum
- Prevalence 2.03 per 10,000 births; maternal age under 25 and primiparity associated
- Evidence Level
- III (registry case-control)
- Region
- Europe (Finland)
- Key Datum
- Population case-control; primiparity and first-trimester beta-blocker/progestogen associations
- Evidence Level
- III
- Region
- Europe (multi-country)
- Key Datum
- Surveillance platform tracking limb-reduction and amniotic-band defects across populations
- Evidence Level
- III (surveillance)
- Region
- USA
- Key Datum
- Multi-site case-control; secondhand-smoke association with ABS-limb body wall complex
- Evidence Level
- III
- Region
- UK
- Key Datum
- Tertiary surgical series; ~1 in 15,000; upper-limb predominance
- Evidence Level
- IV (case series)
Practice variation and global access:
- Managed in paediatric orthopaedic/plastic hand units with multidisciplinary limb-deficiency clinics
- Antenatal ultrasound increasingly detects bands and threatened limbs; selected fetoscopic release offered in a few fetal-surgery centres (Cincinnati, European units) for progressive limb or cord constriction
- Microsurgical toe-to-hand transfer and prosthetics available for severe loss
- Frequently diagnosed only postnatally (limited antenatal screening) — case reports from Somalia and Burkina Faso illustrate first documented presentations
- Emphasis on simple band release / Z-plasty under local or topical anaesthesia where theatre access is limited
- Prosthetic provision and staged reconstruction often constrained; early simple release of threatening Grade 2 bands remains the priority intervention
- Patterson classification as the shared language
- Urgent release of bands with distal lymphoedema/vascular threat
- Single- or two-stage circumferential excision with opposing flaps (Z-plasty or Y-to-V) preferred over piecemeal release
- Sporadic aetiology — reassurance regarding negligible recurrence risk
- Patient selection for fetoscopic release (limb salvage vs PPROM risk) is undefined
- Optimal timing of acrosyndactyly separation (early neonatal vs 3-6 months) is debated
- Best technique to avoid residual hourglass deformity after circumferential release
- Whether maternal medication associations are causal or confounded
- Key documentation: Patterson grade, vascular/lymphoedema assessment, timing rationale (urgent vs elective)
- Consent: staged approach for Grade 3, recurrence/hourglass-deformity risk, likely need for multiple procedures
- Common pitfalls: missing the urgency of a distally oedematous band; incomplete release leading to recurrence
Key documentation points:
- Patterson classification (Grade 1-4) clearly documented
- Assessment of urgency (especially Grade 2)
- Discussion of treatment plan and staging if Grade 3
- Family counseling about prognosis and need for multiple procedures
- Timing of surgery (urgent vs elective)
Don't Delay Grade 2: Missing the urgency of Grade 2 constriction bands with distal edema is a serious issue. These require urgent release, and delay may lead to tissue loss or amputation.
MCQ Practice Points
Q: A newborn has a constriction ring around a finger with swelling of the fingertip. What is the Patterson grade and management? A: Grade 2 - constriction with distal lymphedema. This requires URGENT Z-plasty release to prevent progression to tissue loss. The edema indicates active lymphatic obstruction that may worsen if not treated promptly.
Q: How many Z-plasties are typically needed for constriction band release? A: Usually 2-4 Z-plasties around the circumference. Multiple Z-plasties ensure complete release and prevent recurrence. The Z-plasties should have 60-degree angles for optimal length gain (75% increase).
Q: How do you distinguish constriction bands from symbrachydactyly? A: Constriction bands are asymmetric, irregular, and may affect multiple limbs. Symbrachydactyly is central ray deficiency (missing middle fingers), usually bilateral and more symmetric. Constriction bands have visible constriction rings, while symbrachydactyly has absent rays.
Q: Which Patterson grade requires urgent surgical release? A: Grade 2 (constriction with distal lymphedema) requires urgent release. The edema indicates active lymphatic obstruction that may progress to vascular compromise and tissue loss. Grade 1 can be observed or treated electively, Grade 3 is staged, Grade 4 needs prosthetics.
Q: How do you prevent recurrence after Z-plasty release? A: Complete release with multiple Z-plasties around the entire circumference. Incomplete release allows the constriction to reform as the child grows. Using 2-4 Z-plasties with 60-degree angles ensures adequate lengthening and breaks up the constriction ring completely.
Q: How do you manage Grade 3 constriction bands with acrosyndactyly? A: Staged approach: Stage 1 is Z-plasty release of constriction bands, allowing 3-6 months for healing. Stage 2 is digit separation, creating web spaces and separating fused digits while preserving neurovascular bundles. Multiple procedures may be needed for complex cases.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A newborn is noted to have a constriction ring around the middle finger with swelling of the fingertip. The constriction is deep and the distal finger is edematous.”
“Walk me through the Z-plasty release technique for a constriction band.”
“A 6-month-old has multiple constriction bands affecting several fingers. Some fingers are fused at the tips (acrosyndactyly), and one finger has a constriction ring with distal swelling.”
Patterson Classification
- Grade 1: Simple ring, no distal changes = elective release
- Grade 2: Ring with distal edema = URGENT release
- Grade 3: Ring with acrosyndactyly = staged release and separation
- Grade 4: Intrauterine amputation = prosthetic fitting
Key Clinical Features
- Asymmetric, irregular constriction rings
- Not hereditary - sporadic condition
- 50% have multiple bands
- Variable severity from simple ring to amputation
Surgical Technique
- Z-plasty release: 2-4 Z-plasties around circumference
- 60-degree angles for optimal length gain (75%)
- Complete release essential to prevent recurrence
- Preserve flap vascularity
Treatment Urgency
- Grade 1: Elective (6-12 months)
- Grade 2: URGENT (days to weeks)
- Grade 3: Staged (release then separation)
- Grade 4: Prosthetic fitting (12-18 months)
Complications
- Recurrence: 5-10% if incomplete release
- Flap necrosis: Rare but serious
- Wound infection: 5%
- Scar contracture: 10-15%
Evidence Base
The amniotic band sequence literature is dominated by retrospective case series and narrative reviews (Oxford Level III-IV). No randomised trials exist, and is unlikely to, given the rarity and heterogeneity of the condition. The cards below combine the original classification, contemporary surgical-technique series, population-based epidemiology, and the emerging fetal-surgery evidence base.
Patterson — Original Classification of Congenital Ring Constrictions
- Foundational description distinguishing four presentations: simple ring; ring with distal deformity/lymphoedema; ring with distal fusion (acrosyndactyly); intrauterine amputation
- Established that bands and their distal sequelae, not heredity, drive the deformity
- Introduced multiple Z-plasty release as the operative principle
- Framework still in routine clinical and examination use over six decades later
Amniotic Constriction Bands — Case Series and Proposed Classification
- 37 children over 1993-2012 at a single tertiary paediatric centre; 28 underwent surgery, 9 managed non-operatively
- Upper-limb bands were the most common pattern and lower-limb the least; 17 of 37 had combined upper- and lower-limb involvement
- Cited an approximate incidence of 1 in 15,000 live births
- Highlighted lack of consensus nomenclature and proposed an upper-limb scheme incorporating anatomical location and band depth
Multiple Continuous Y-to-V-Plasties for Constriction Band Excision
- 7 patients, 10 involved extremities; band excision with continuous opposing Y-to-V-plasties in one or two stages
- All achieved primary wound healing with no band revision required
- Technique designed to avoid the residual hourglass deformity that can follow simple circumferential Z-plasty
- Post-operative lymphoedema in 2 patients resolved with compression; one neuropathic insensate foot ultimately required Syme amputation
Risk Factors and Prevalence of Amniotic Band-Associated Limb Deficiency
- Nationwide Finnish population-based case-control study, 106 cases versus 530 matched controls (births 1996-2008)
- Young maternal age (less than 25 years) increased risk (OR 1.72, 95% CI 1.06-2.80)
- Primiparity was an independent risk factor (adjusted OR 2.42, 95% CI 1.52-3.88)
- Novel associations with first-trimester maternal beta-blocker and progestogen use
Amniotic Band Syndrome — Australian Population-Based Prevalence
- Two Australian state birth-defect registries (Western and South Australia)
- Prevalence 2.03 per 10,000 births (approximately 1 in 4,900)
- Equal sex distribution; more common with maternal age under 25 years and in first births
- Limb-only defects in 24 cases, limb-body-wall in 4, craniofacial/complex in 12
Fetoscopic Release of Amniotic Bands — Systematic Review
- PRISMA systematic review: 17 studies, 37 fetuses undergoing fetoscopic band release (median 22 weeks)
- Fetal survival 89.2%; limb preserved and functional in 75.7%
- Preterm premature rupture of membranes in 51.3% — the dominant complication
- Strongest rationale where bands threaten the umbilical cord or a still-perfused limb
Prosthetic and Reconstructive Management of Limb Deficiency
- Early prosthetic fitting (around sitting/standing milestones) improves acceptance for congenital amputation
- Toe-to-hand transfer can restore prehension in adactylous constriction-band hands
- Multidisciplinary limb-deficiency clinics optimise function and family support
- Reconstruction is individualised to residual anatomy and functional goals
For severe upper-limb amniotic band sequence with multi-digit loss or acrosyndactyly, microsurgical second-toe (and double second-toe) transfer can create a sensate, mobile digit for tip-to-tip pinch. Series report viable, growing transfers (growth roughly 68-95% of the donor toe) but with mediocre active motion and a near-universal need for secondary procedures, so families must be counselled about staged, long-horizon reconstruction.