Function, classification, timing and reconstruction
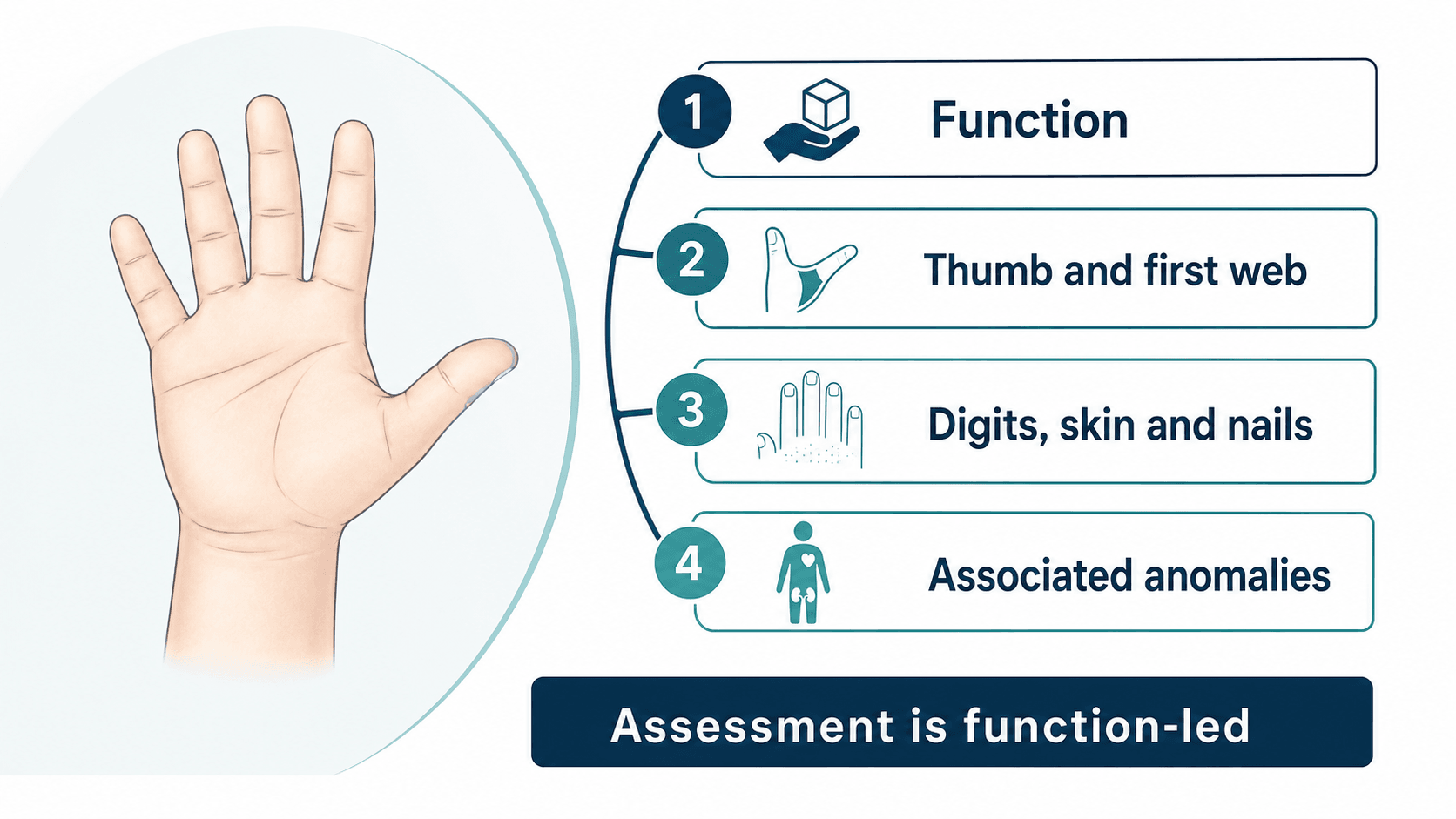
- Describe the anatomy before naming an operation: thumb, digits, web spaces, wrist, forearm, skin, nails, joints, tendons and function.
- Use the Oberg-Manske-Tonkin framework to organise congenital hand differences, but do not let classification replace clinical description.
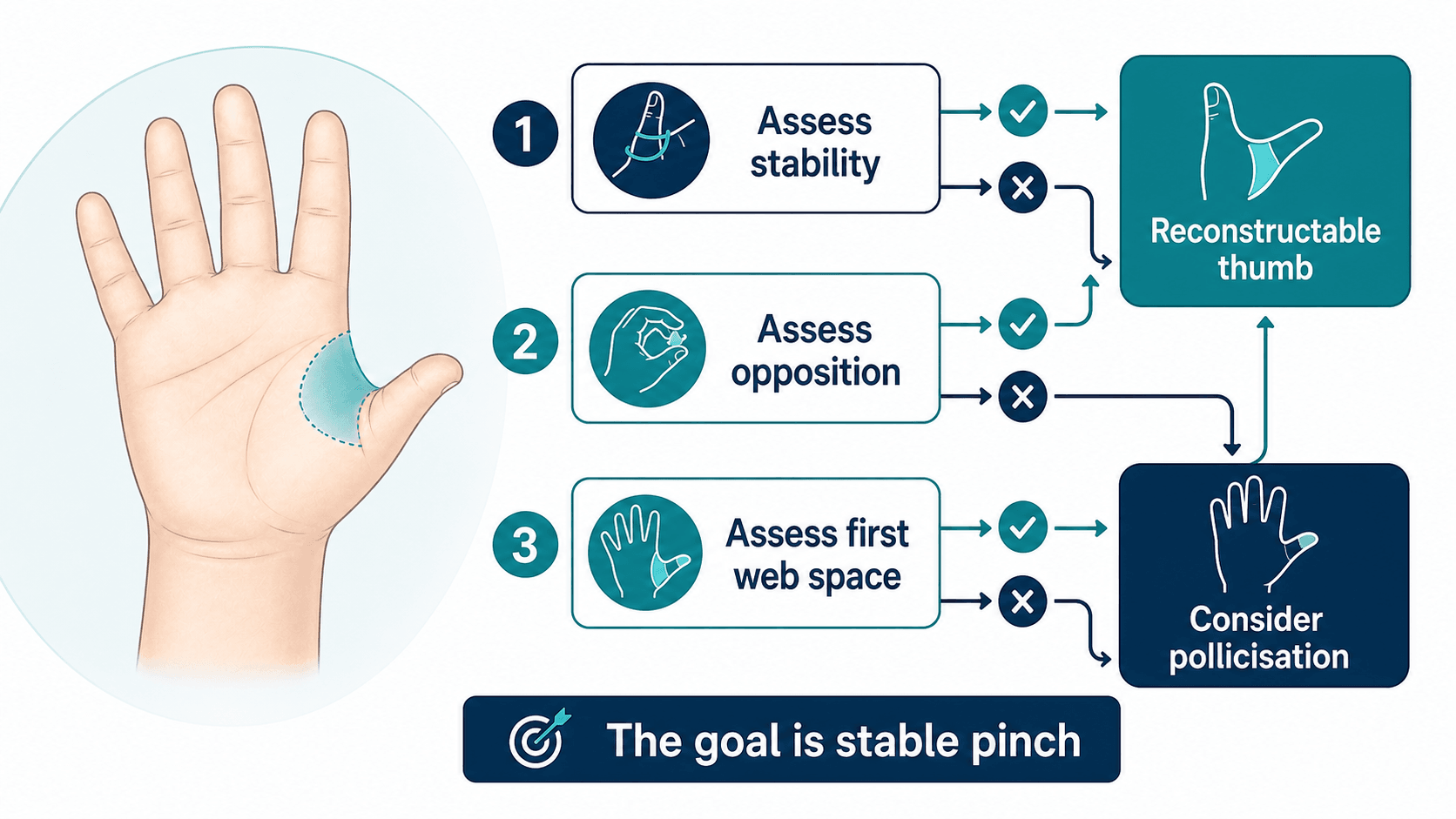
- Thumb function is the central decision point because opposition, stability and first web space determine pinch.
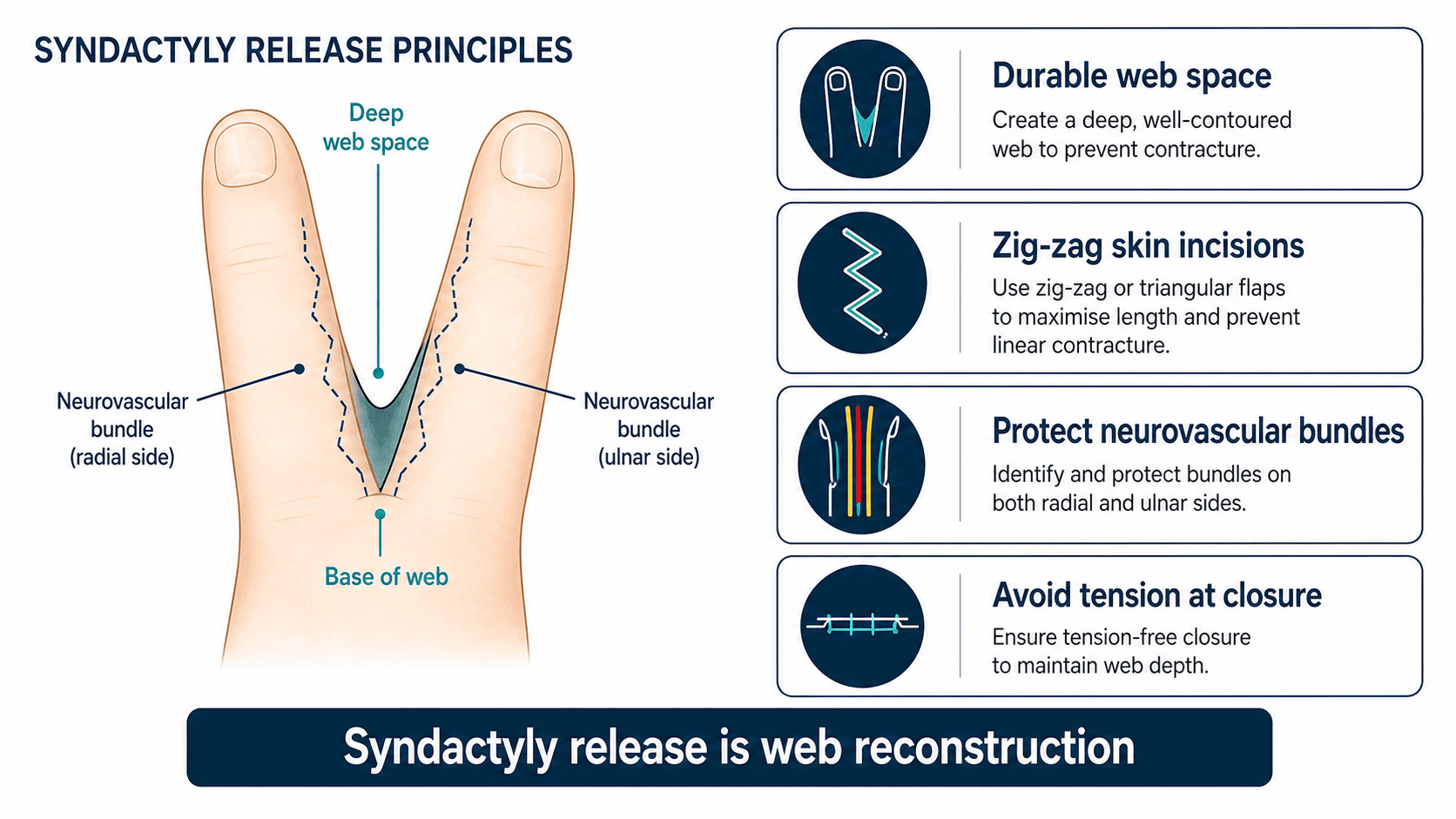
- Syndactyly release is web reconstruction; timing depends on border digits, growth tethering, complexity and skin cover.
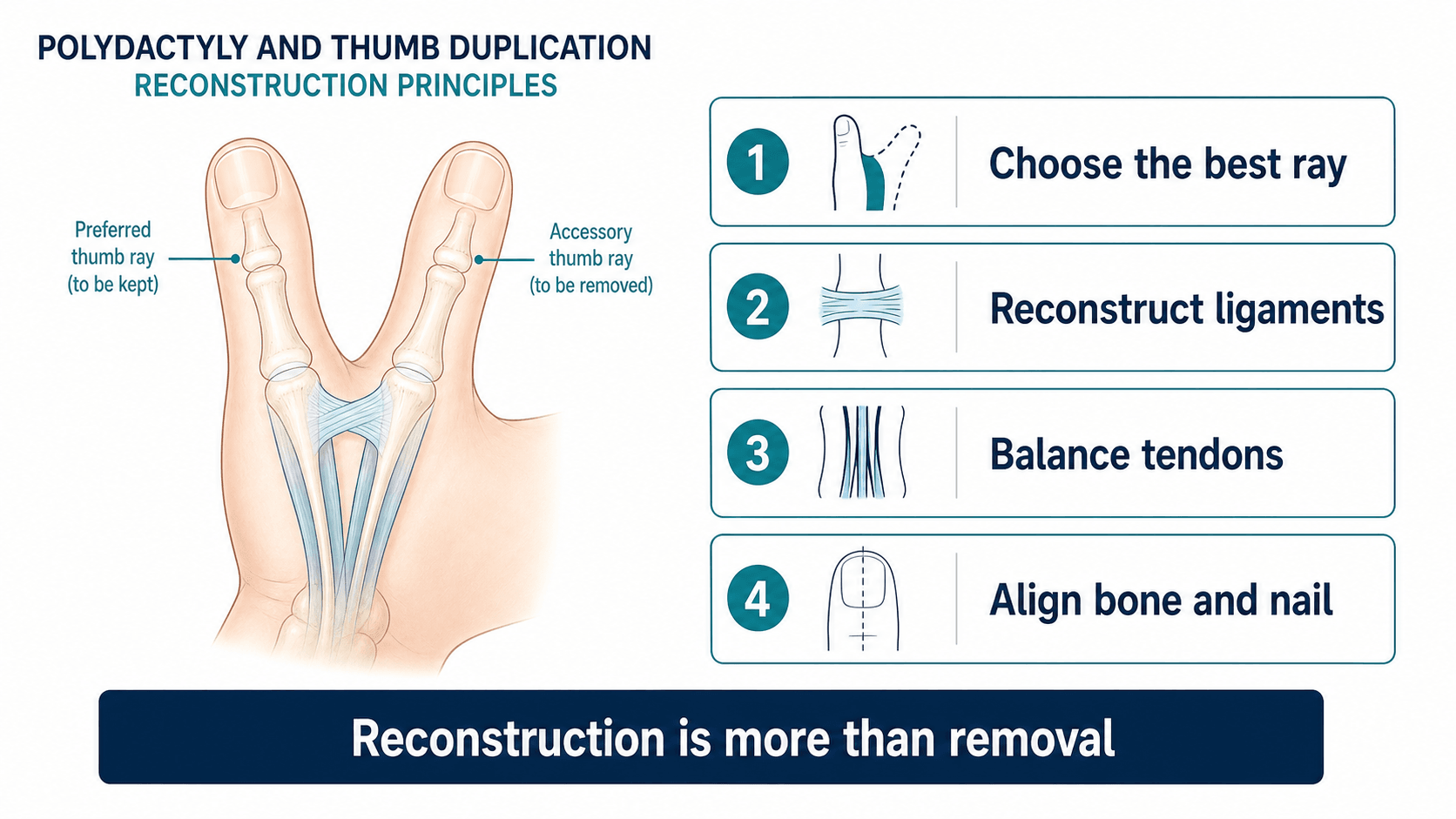
- Polydactyly reconstruction is not simple amputation; the retained ray often needs ligament, tendon, bone and nail alignment.
- Screen for associated anomalies when the pattern suggests radial deficiency, syndromic syndactyly, bilateral disease or multi-system involvement.
- “Watch the child play before looking at the X-ray; spontaneous use often defines the real problem.
- “Border-digit syndactyly is released earlier because unequal digit lengths can tether growth and create angular deformity.
- “A small duplicated digit may carry collateral ligament, tendon or nail-fold anatomy needed for the retained digit.
- “A floating or unstable hypoplastic thumb may be less functional than an index finger pollicisation.
- “Families need a staged plan: diagnosis, development, surgery, therapy, scars, possible revision and realistic functional goals.
Parents may first ask about appearance, but congenital hand surgery is judged by function, sensibility, growth, scars, revision risk and the child's ability to use the hand in daily life.
Images and Diagrams

| Question | Practical answer | Why it matters |
|---|---|---|
| First assessment step? | Observe spontaneous hand use. | The child often demonstrates the functional priority. |
| Most important structure? | Thumb and first web space. | Opposition and stable pinch drive hand utility. |
| Classification system? | Oberg-Manske-Tonkin plus condition-specific systems. | Organises diagnosis without replacing description. |
| Timing principle? | Operate when function or growth will benefit. | Avoid both delayed tethering and premature scarring. |
| Safety issue? | Associated systemic patterns. | Radial and syndromic patterns may need cardiac, renal, haematology or genetics review. |
HANDAssessment Sequence
Hook:HAND keeps the assessment function-led rather than operation-led.
PINCHThumb Function
Hook:PINCH is the practical thumb hypoplasia checklist.
WEBSyndactyly
Hook:WEB keeps syndactyly timing and surgical design linked.
Overview/Epidemiology
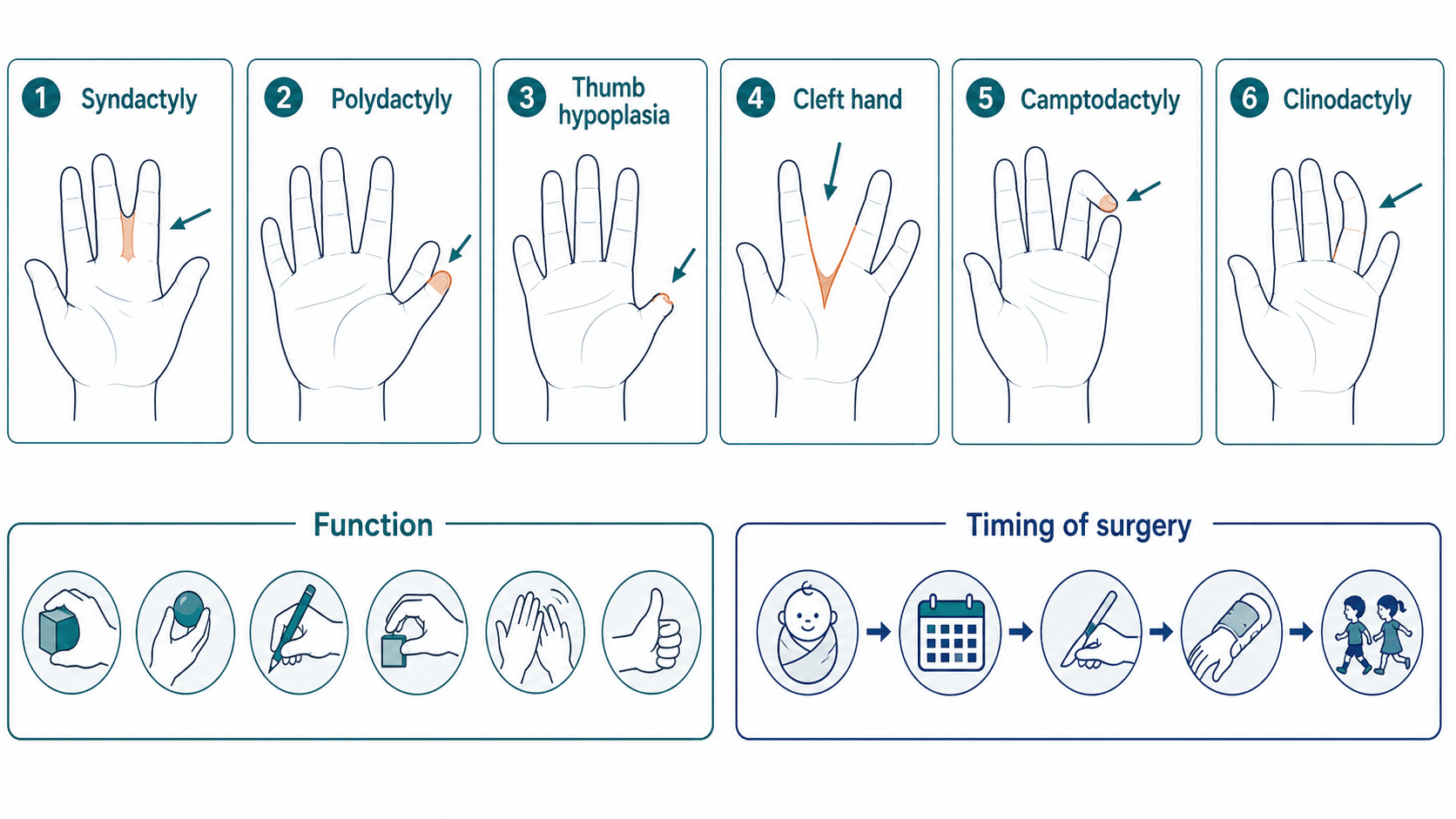
Congenital hand differences range from a small extra digit to complex bilateral syndromic limb deficiency. The presentation may be a newborn with an obvious anomaly, a toddler with delayed function, or a child referred for a specific problem such as syndactyly, thumb hypoplasia, clinodactyly or camptodactyly.
The consultation has two simultaneous tasks. First, explain the visible difference in language that parents can understand. Second, identify the functional and safety implications: Is the thumb useful? Are digits tethered? Is there enough skin for reconstruction? Is the pattern isolated, or does it suggest cardiac, renal, haematological, vertebral or genetic associations?
Most decisions are not urgent on the day of birth, but early referral matters. Families need counselling, the child may need therapy, and some conditions have timing windows. Border-digit syndactyly and severe thumb deficiency are examples where delaying assessment can reduce the quality of later function.
Pathophysiology
Upper limb development depends on coordinated patterning in several directions. The clinical value is practical: the developmental mechanism predicts what else may be abnormal besides the visible digit.
| Mechanism | Typical hand pattern | What to check clinically |
|---|---|---|
| Failure of formation | Absent or hypoplastic structures such as radial deficiency, absent thumb or central ray deficiency. | Forearm, wrist, thumb, elbow motion and associated systemic anomalies. |
| Failure of separation or differentiation | Syndactyly, synostosis, camptodactyly and complex fusions. | Skin shortage, neurovascular sharing, joint motion and growth tethering. |
| Duplication | Polydactyly and thumb duplication. | Which ray has the best nail, joint, tendon, collateral ligament and alignment. |
| Dysplasia or abnormal tissue growth | Macrodactyly, abnormal soft tissue, nail or skeletal overgrowth. | Progression, nerve symptoms, soft-tissue bulk and recurrence risk. |
| Amniotic constriction sequence | Constriction rings, distal swelling, acrosyndactyly or amputations. | Lymphoedema, vascularity, distal function and staged release need. |
The anatomy is rarely just bone. Tendons, intrinsic muscles, digital nerves, vessels, collateral ligaments, nail folds and skin cover may all be abnormal. That is why congenital hand surgery is reconstructive surgery, not simply removal, release or straightening.
Classification
The Oberg-Manske-Tonkin system is useful because it organises congenital upper-limb differences into developmental groups. In clinical teaching, however, classification must be followed by a concrete anatomical description. A clear description is often more useful than a label alone.
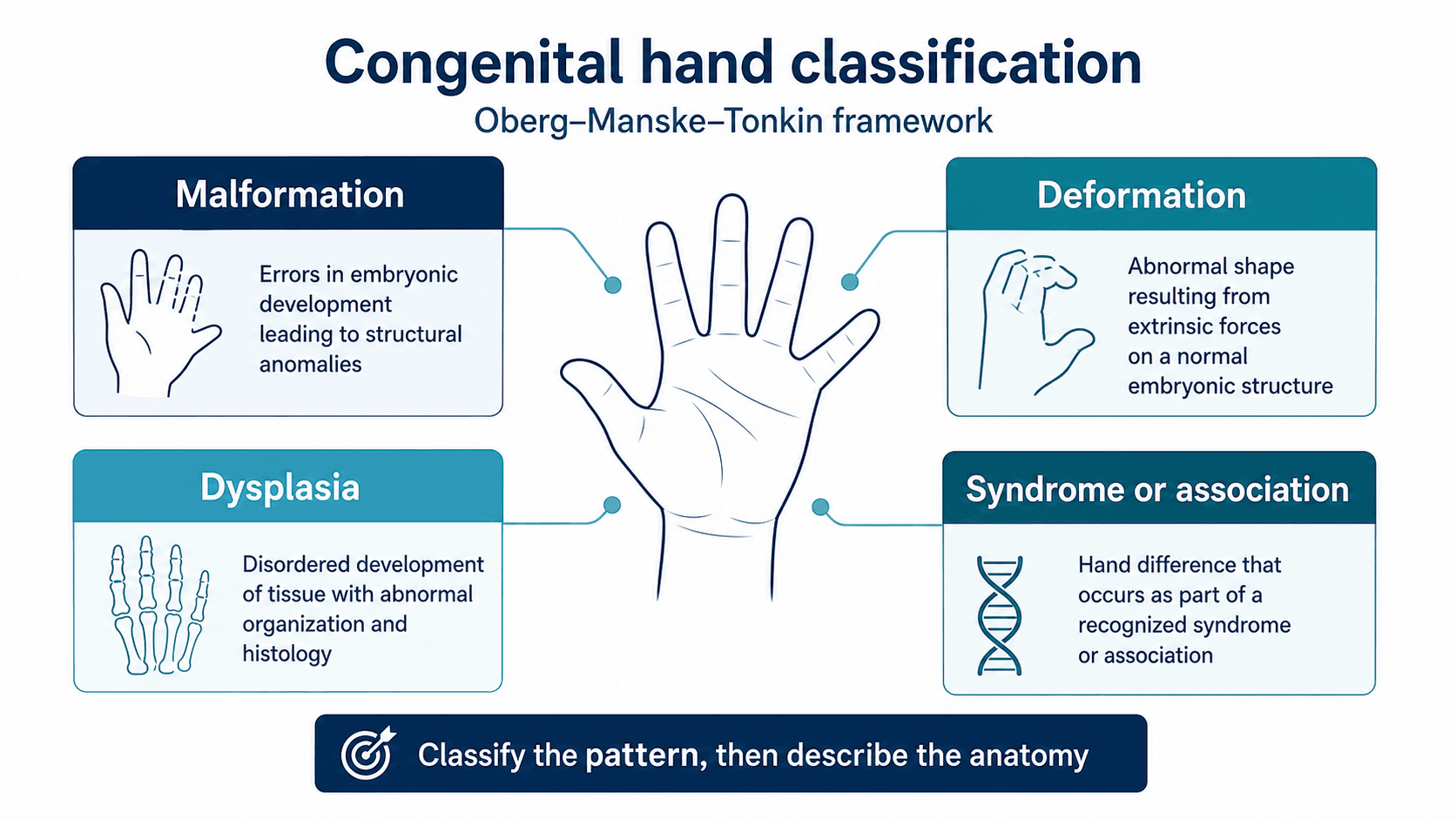
- Malformations: absent, duplicated, separated or hypoplastic parts.
- Deformations: a formed part is bent, contracted or positioned abnormally.
- Dysplasias: abnormal tissue growth or quality, such as macrodactyly.
- Syndromes: hand findings are part of a wider multi-system condition.
Clinical Presentation
Newborn presentation
Many congenital hand differences are visible at birth. Parents may be distressed and need clear, calm explanation. The first response should not be to name an operation. Explain that hand function depends on the thumb, digits, skin, joints, tendons, nerves and how the child learns to use the limb.
Later presentation
Some children present later because function becomes more obvious with development. A toddler may avoid pinch, struggle with grasp, catch a flexed finger, have progressive web tethering, or show increasing angular deformity as the digits grow. School-age children may present with writing difficulty, sport limitations, pain from a prominent duplicated ray, or concern about appearance and peer interaction.
History
| Domain | Ask specifically | Why it matters |
|---|---|---|
| Pattern and onset | Prenatal scans, birth finding, unilateral or bilateral involvement and progression. | Separates isolated anomaly from broader developmental pattern. |
| Family and pregnancy | Family history, consanguinity where relevant, pregnancy exposures and syndromic clues. | Guides genetics referral and recurrence counselling. |
| Associated systems | Feeding, cardiac history, renal anomalies, vertebral issues, haematological problems and other limb findings. | Prevents unsafe elective surgery when systemic disease is possible. |
| Function | Grasping blocks, holding utensils, dressing, toileting, writing, play, sport and bimanual tasks. | Defines the treatment goal better than appearance alone. |
Examination
Observe spontaneous use first. Then examine both upper limbs from shoulder to fingertip.
| Area | Assess | Decision it informs |
|---|---|---|
| Thumb and first web | Presence, stability, opposition, thenar function and web depth. | Reconstruction versus pollicisation, and pinch potential. |
| Digits and nails | Number, length, webbing, nail folds, duplicated parts and growth tethering. | Timing of syndactyly or duplication reconstruction. |
| Joints and tendons | Passive motion, active motion, stability, contracture and tendon balance. | Whether surgery can improve function without causing stiffness. |
| Skin, vessels and nerves | Skin shortage, scars, vascularity and sensibility where testable. | Flap/graft planning, staged surgery and safety. |
| Wrist and forearm | Wrist position, forearm length and elbow motion. | Identifies longitudinal deficiency and associated treatment limits. |
A child reaching for a toy often demonstrates opposition, grasp, release and bimanual strategy better than a formal command.
Investigations
Plain radiographs are the main investigation when skeletal anatomy will change treatment. Include the hand and often the wrist and forearm, especially when thumb hypoplasia or radial deficiency is suspected. In infants, some anatomy is cartilaginous, so repeat imaging later may be more informative.
Ultrasound or MRI is rarely first-line, but can be useful in selected complex cases if tendons, vessels, soft tissue or a mass-like component will change surgery. Genetic, cardiac, renal or haematological investigations should be targeted to the pattern rather than ordered indiscriminately.
| Clinical question | Investigation | Decision it informs |
|---|---|---|
| What bones are present? | Hand, wrist and forearm radiographs. | Defines duplicated, fused, absent or hypoplastic skeleton. |
| Is the thumb reconstructable? | Clinical assessment plus radiographs. | Assesses CMC, MCP, first web and thenar function. |
| Could this be syndromic? | Targeted paediatric, genetics, cardiac, renal or haematology review. | Prevents unsafe elective surgery before systemic assessment. |
| What function should treatment improve? | Therapy assessment and functional observation. | Sets realistic goals and post-operative therapy plan. |
Major Conditions
Syndactyly
Syndactyly is failure of separation between adjacent digits. It may be incomplete or complete. It may be simple when only soft tissue is involved, complex when bone or nail structures are fused, and complicated when additional skeletal anomalies exist. The ring-small finger web is commonly affected, but border-digit involvement is more urgent because unequal digit lengths can tether growth.
Polydactyly and thumb duplication
Polydactyly is an extra digit or ray. It may be preaxial, central or postaxial. Thumb duplication is commonly discussed with Wassel classification, but management depends on the function of the retained thumb: alignment, nail, joint stability, collateral ligaments, tendon insertions and first web space.
Thumb hypoplasia
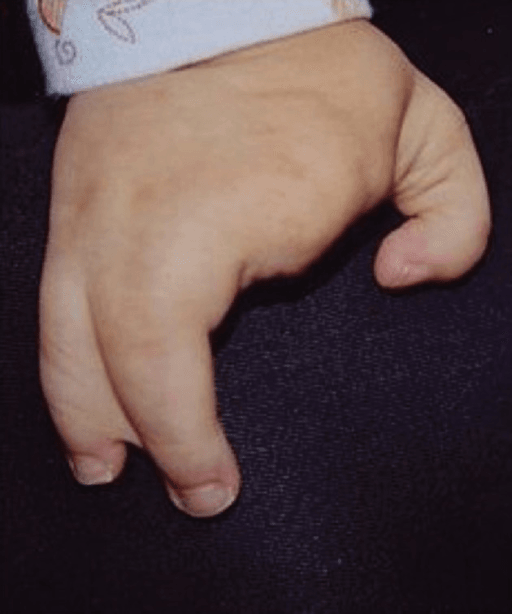
Thumb hypoplasia ranges from mild small thumb to absent or floating thumb. Mild forms may need observation or first-web release. Reconstructable thumbs may need web deepening, opponensplasty and MCP stabilisation. Severe unstable or floating thumbs often function better after index pollicisation than after attempted preservation of a non-functional thumb.
Symbrachydactyly
Symbrachydactyly is usually sporadic and unilateral. It includes short digits, absent phalanges, nubbins, central deficiency and variable thumb involvement. The main task is counselling and functional support. Surgery may improve pinch space, length or grasp in selected children, but it cannot create a normal hand. Prosthetic, adaptive and therapy options should be discussed without framing them as inferior to surgery.
Cleft hand
Cleft hand is a central deficiency with absent central ray or rays and variable syndactyly. Some children have excellent function despite a dramatic appearance. Surgery is considered for first web narrowing, transverse bones, progressive deformity, unstable pinch, syndactyly or functional limitations. The plan should protect the thumb-index pinch space.
Camptodactyly, clinodactyly and trigger thumb
| Condition | Clinical focus | Usual treatment logic |
|---|---|---|
| Camptodactyly | PIP flexion deformity, flexibility, progression and functional limitation. | Observe or splint mild flexible cases; consider surgery only for severe or progressive functional contracture. |
| Clinodactyly | Coronal-plane curvature, often from delta phalanx, plus function and cosmesis. | Usually observe; corrective osteotomy is reserved for severe deformity or functional interference. |
| Congenital trigger thumb | IP flexion, palpable Notta nodule, reducibility, age and duration. | Many early cases are observed; persistent fixed triggering may need A1 pulley release. |
Management Principles
Management begins with honest counselling. The family should understand the diagnosis, what function is present, what treatment can improve, and what surgery cannot change. Many children benefit from therapy, adaptive strategies and observation. Surgery is chosen when it improves function, prevents deformity, supports development or solves a specific practical problem.
| Problem | Timing logic | Main treatment decision |
|---|---|---|
| Border-digit syndactyly | Earlier planning because unequal digit lengths can tether growth. | Release the web with durable commissure reconstruction and safe skin cover. |
| Central simple syndactyly | Often can wait until the child is larger and tissue handling is safer. | Release when function, growth, family goals and surgical safety align. |
| Thumb hypoplasia | Early assessment because pinch development and radial deficiency screening matter. | Reconstruct a stable thumb if possible; pollicise when the thumb is absent, floating or non-reconstructable. |
| Thumb duplication or polydactyly | Plan once anatomy, nail, joint stability and tendon balance are defined. | Build the best single ray; do not simply amputate the smaller part. |
| Camptodactyly or clinodactyly | Observe mild flexible deformity; intervene for progression or function. | Splint, therapy or osteotomy/release only when the deformity justifies stiffness and scar risk. |
| Bilateral complex differences | Stage surgery so the child keeps useful function during recovery. | Protect feeding, toileting, mobility, play and family care capacity. |
Observation is appropriate when function is good, deformity is mild, or surgery is unlikely to improve the hand. Therapy supports range, splinting, sensory use, bimanual skill and post-operative recovery. Adaptive tools may be more useful than surgery for some tasks.
Operative Concepts
| Operation | Core technical idea | Major pitfall |
|---|---|---|
| Syndactyly release | Create a durable commissure, separate digits with zig-zag incisions, protect neurovascular bundles and close without tension using flaps or full-thickness graft when needed. | Linear scars, inadequate skin, web creep, vascular compromise and stiffness. |
| Polydactyly reconstruction | Build one straight, stable, sensate digit by choosing the best skeletal, ligament, tendon and nail components. | Treating it as simple amputation and leaving instability, malalignment or nail deformity. |
| Pollicisation | Rotate, shorten and reposition the index finger while preserving neurovascular supply and balancing tendons to create opposition. | Trying to preserve a floating non-functional thumb when pollicisation would give better pinch. |
| Contracture or deformity surgery | Reserve surgery for progressive or functionally important deformity and combine with therapy. | Creating stiffness or recurrence by operating on mild flexible deformity. |
Complications
Early complications
- Skin graft loss or flap edge necrosis.
- Vascular compromise after complex digit separation.
- Infection or wound breakdown.
- Scar sensitivity and pain.
- Stiffness after immobilisation.
- Family distress if expectations were not clear.
Late complications
- Web creep after syndactyly release.
- Scar contracture and limited motion.
- Angular deformity or instability after polydactyly reconstruction.
- Poor pinch after inadequate thumb reconstruction.
- Growth-related recurrence.
- Need for revision surgery.
- Dissatisfaction if appearance was over-promised.
In congenital hand surgery, a technically successful operation that creates stiffness, poor sensibility or unstable pinch is not a functional success.
Counselling and Follow-up
| Issue | How to explain it | Follow-up focus |
|---|---|---|
| Function first | Explain what the hand can already do and what treatment may realistically improve. | Pinch, grasp, release, bimanual skill and independence. |
| Appearance | Avoid promising a normal-looking hand; scars and residual difference are common. | Child confidence, peer concerns and family expectations. |
| Staged care | Some children need therapy, splints, one operation, revision or staged reconstruction. | Growth, web creep, angular deformity and therapy progress. |
| Risk | Discuss stiffness, scar sensitivity, graft problems, vascular risk and recurrence before elective surgery. | Early wound review and long-term functional review. |
Differential Diagnosis
The hand difference is often obvious; the exam skill is distinguishing patterns that look similar but carry different prognosis, screening needs and surgical plans. The two highest-stakes distinctions are isolated versus syndromic syndactyly, and a deficient central ray (cleft hand) versus transverse or symbrachydactyly deficiency.
| Diagnosis | Distinguishing features | Key action |
|---|---|---|
| Isolated simple syndactyly | Soft-tissue web only, normal nails and skeleton, no systemic features. | Plan web reconstruction; timing by border versus central. |
| Syndromic syndactyly (Apert, Poland) | Complex or complicated webs, craniofacial features (Apert) or absent pectoralis and limb hypoplasia (Poland). | Genetics and systemic assessment before staged surgery. |
| Thumb duplication / preaxial polydactyly | Extra radial digit with shared or duplicated joints; assess best ray. | Reconstruct retained ray, do not simply amputate. |
| Postaxial polydactyly | Extra ulnar digit; often familial, more common in African ancestry. | Excise with collateral ligament reconstruction if well-formed. |
| Thumb hypoplasia with radial deficiency | Small or absent thumb, radial wrist deviation, short forearm. | Mandatory cardiac, renal and haematology (Fanconi, TAR) screen. |
| Cleft hand (central deficiency) | Central V-shaped cleft, absent central ray, often good function. | Protect thumb-index pinch; operate for first-web or function. |
| Symbrachydactyly / transverse deficiency | Short or absent digits with nubbins, usually unilateral and sporadic. | Counsel; prosthetic or toe transfer in selected cases. |
| Amniotic constriction band sequence | Constriction rings, distal swelling, acrosyndactyly, normal proximal anatomy. | Assess vascularity; urgent release if circulation threatened. |
| Macrodactyly / overgrowth | Enlarged digit, may be progressive, nerve-territory distribution. | Monitor progression; debulking or epiphysiodesis if needed. |
| Camptodactyly / clinodactyly / trigger thumb | Isolated flexion or angular deformity without true deficiency or duplication. | Mostly observe; surgery only for progressive functional loss. |
Decision-Making in Practice
Congenital hand assessment should begin with function rather than appearance. The key questions are whether the child can pinch, grasp, release, oppose, feel, play, perform self-care and participate socially. Anatomy matters because it determines whether reconstruction can improve function without creating stiffness, scarring or repeated operations that add little value.
| Problem | Assessment focus | Treatment direction |
|---|---|---|
| Thumb absence or severe hypoplasia | Stability, active motion, first web, thenar function and family goals | Pollicisation when the thumb cannot become a useful post |
| Syndactyly | Border digits, complex bony union, nail involvement and growth asymmetry | Earlier release for border digits or progressive deformity; staged release for multiple webs |
| Polydactyly | Duplication pattern, joint stability, tendon balance and nail complex | Remove or reconstruct the less useful ray while preserving alignment and stability |
| Radial or ulnar deficiency | Wrist position, thumb function, elbow motion, forearm length and syndromic associations | Therapy, splintage and staged reconstruction depending severity and child function |
| Symbrachydactyly or transverse deficiency | Available sensate digits, web spaces, toe transfer suitability and prosthetic needs | Function-led reconstruction, prosthetics or observation |
Classification helps communication, but it should not replace a hand-by-hand functional plan.
| Principle | Practical meaning | Failure mode |
|---|---|---|
| Stable sensate pinch | Create or preserve a thumb or pinch post that the child can use. | Straight-looking hand with poor opposition or no stability. |
| First web space | Deepen or protect the web when thumb-index span limits pinch. | Good-looking thumb that cannot oppose because the web is narrow. |
| Growth and scars | Release tethering tissue early when growth will worsen deformity; avoid scars that contract across joints. | Web creep, angular deformity or recurrent contracture. |
| Staging | Stage procedures when blood supply, skin coverage or bilateral function makes one-stage surgery unsafe. | Vascular compromise or loss of independence during recovery. |
| Therapy | Plan splinting, motion and functional retraining before operating. | Technically correct surgery followed by stiffness and poor use. |
Controversies and Areas of Uncertainty
Even at consultant level, several decisions in congenital hand surgery remain genuinely contested. Examiners reward a candidate who can name the controversy, give both sides and then commit to a defensible position.
| Controversy | One side | Other side |
|---|---|---|
| Timing of syndactyly release | Early release (before 12-18 months) limits growth tethering of border webs and gives a longer remodelling period. | Later release allows larger structures, easier dissection and lower anaesthetic and vascular risk for non-border webs. |
| Reconstruct versus pollicise the Blauth IIIB thumb | An unstable carpometacarpal joint usually dooms reconstruction, so pollicisation gives more reliable pinch. | Some surgeons and families prefer to preserve a five-digit hand and accept a weaker but present thumb. |
| Graft versus graftless syndactyly closure | Full-thickness grafts reliably resurface defects and are the traditional standard. | Defatting, local flaps and dermal substitutes can avoid donor sites and graft pigmentation in selected webs. |
| Centralisation in radial longitudinal deficiency | Centralisation or radialisation improves wrist alignment and hand position. | High recurrence, ulnar growth arrest and stiffness lead some to favour soft-tissue distraction or vascularised transfers. |
| Bilhaut-Cloquet versus ablation-reconstruction for thumb duplication | Bilhaut preserves combined width and joint stability for symmetric duplicates. | It risks nail ridging and joint stiffness, so most use ablation of the smaller ray with reconstruction. |
Evidence Signals
OMT classification: dysmorphology-based framework
- The Oberg-Manske-Tonkin system separates malformations, deformations and dysplasias using dysmorphological concepts.
- Malformations are subgrouped by whether the hand alone or the whole limb is affected and by the axis of development involved.
- The framework is expandable so that future gene and chromosomal defects can be incorporated.
Epidemiology of congenital upper-limb anomalies (OMT applied)
- 641 children with 653 anomalies were classified across three centres over one year; 74% were malformations.
- Among hand-plate malformations, radial polydactyly (15%) was most common, then symbrachydactyly (13%) and cleft hand (11%).
- All individuals could be classified with OMT, though Madelung deformity and symbrachydactyly needed clarification.
Clinical Reasoning Notes
Structured clinical approach
Start with the child's age, side, function and pattern. Then describe the anatomy: thumb, web spaces, number of rays, digits involved, joints, skin, nail and forearm. State whether the condition is isolated or syndromic. Finally, give a plan for investigation, counselling, therapy and timing.
Common pitfalls
- Starting with an operation instead of function.
- Saying "remove the extra digit" without reconstructing the retained ray.
- Treating all syndactyly with the same timing.
- Missing radial deficiency or haematology risk in thumb hypoplasia.
- Preserving a non-functional thumb when pollicisation would give better pinch.
- Ignoring the first web space.
- Promising normal appearance.
- Forgetting therapy and revision risk.
Integrated clinical approach
"I would assess the child in a paediatric hand clinic. I would first observe spontaneous function, then describe the thumb, digits, web spaces, skin, joints, tendons, sensibility and forearm. I would classify the pattern but base management on functional goals, growth and associated anomalies. Treatment may be observation, therapy, reconstruction or pollicisation, with timing chosen to support development while minimising stiffness, scarring and revision risk."
Evidence Base
Radial polydactyly: physical-characteristic classification
- Across 545 thumbs in 500 patients, ulnar-dominant duplication was most frequent (67.5%) and the hypoplastic type accounted for 14.5%.
- Excision with reconstruction was needed in 73.9% and simple excision in only 24.8%, confirming most duplicates require reconstruction not amputation.
- Stratifying by floating, symmetry, dominant side and joint angulation predicted the operation as well as the radiographic Wassel-Flatt system.
Syndactyly web reconstruction: dorsal flap technique
- 39 webs were reconstructed in 26 children using a hexagonal dorsal flap with mid-lateral closure; grafts were needed in only 2 complex or complicated cases.
- Web creep occurred in a single child after a self-induced postoperative infection, underscoring that closure technique and wound integrity drive outcome.
- Mean parental cosmetic and functional satisfaction scores were 87 and 92 of 100 at 1.3 years.
Pollicisation for thumb aplasia and severe hypoplasia
- 13 index pollicisations (Blauth IIIB, IV and V thumbs) were assessed at a mean 6.5 years; mean Percival score was 18 of 22.
- Pollicisation reliably created a sensate, mobile thumb with satisfactory strength and appearance in the majority of children.
- Transient psychosocial discomfort was reported, reinforcing the need for family counselling alongside the technical result.
Radial longitudinal deficiency: associations and treatment
- About two-thirds of children with radial longitudinal deficiency have an associated medical or musculoskeletal disorder, and one-third have a recognised syndrome.
- Centralisation and radialisation improve wrist position but carry high recurrence and ulnar growth-arrest rates.
- Microsurgical options (vascularised fibula or second-toe transfer) and management of the associated hypoplastic thumb are evolving alternatives.
Guidelines, Registries & Global Practice
Congenital hand surgery is delivered very differently across high- and limited-resource settings, but the functional principles are universal. There is no single global guideline; practice is shaped by specialist society reviews, classification consensus and national registries.
| Measure | Approximate figure | Source population / note |
|---|---|---|
| Overall congenital upper-limb anomaly birth prevalence | Roughly 1 to 2 per 1000 live births | Population registry estimates vary with ascertainment and minor-anomaly inclusion. |
| Polydactyly | Among the most common; postaxial more frequent in African ancestry, preaxial in East Asian and European ancestry | Ancestry-dependent distribution is a recognised exam point. |
| Syndactyly | Around 1 in 2000 to 3000 births | Often the ring-small or long-ring web; can be syndromic (Apert, Poland). |
| Radial longitudinal deficiency | Around 1 in 30,000 to 100,000 | Two-thirds have associated anomalies; mandatory systemic screen. |
| Body / framework | Emphasis | Practical implication |
|---|---|---|
| IFSSH / OMT classification (international) | Dysmorphology-based grouping adopted as the global standard since 2014. | Use OMT terminology in international exams and correspondence. |
| BSSH (UK) and ASSH (US) educational guidance | Function-led assessment, staged reconstruction and early referral for border-digit and thumb deficiency. | Refer neonatal anomalies early to a specialist congenital hand service. |
| AO / paediatric hand reconstructive principles | Reconstruct the retained ray; protect neurovascular bundles and the first web. | Avoid framing duplication surgery as simple amputation. |
| Genetics / paediatric haematology pathways | Screen radial deficiency for Fanconi anaemia (chromosomal breakage) and TAR before surgery. | Haematology clearance can change anaesthetic and surgical timing. |
| Domain | High-resource setting | Limited-resource setting |
|---|---|---|
| Diagnosis | Antenatal ultrasound, early genetics and multidisciplinary clinic. | Often first seen at walking age or school entry; late presentation common. |
| Reconstruction | Microsurgery, toe transfer and staged web reconstruction available. | Focus on high-impact, single-stage procedures and durable web release. |
| Therapy and prosthetics | Hand therapy, custom splints and myoelectric prostheses accessible. | Adaptive low-cost devices and family-led therapy emphasised. |
| Follow-up | Long-term growth and revision review routine. | Single definitive procedure prioritised where follow-up is uncertain. |
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A newborn is referred with an abnormal hand. How do you assess and counsel the family?”
“Why is border-digit syndactyly usually released earlier than central simple syndactyly?”
“A child has a very small unstable thumb. How do you decide between reconstruction and pollicisation?”
“A toddler has a duplicated thumb with two similar-sized radial digits. The family asks you to remove the extra one. How do you plan surgery?”
Assess
- Watch function
- Describe anatomy
- Thumb and web
- Whole upper limb
- Associated screen
Classify
- Malformation
- Deformation
- Dysplasia
- Syndrome
- Condition-specific system
Treat
- Observe
- Therapy
- Web reconstruction
- Ray reconstruction
- Pollicisation
Pitfalls
- Cosmetic-only plan
- No systemic screen
- Web creep
- Unstable retained ray
- Poor pinch