Preaxial deficiency | Thumb function | Systemic screening | Wrist reconstruction | Recurrence
- Radial longitudinal deficiency ranges from thumb and carpal deficiency with a near-normal radius to complete absence of the radius.
- Systemic screening is essential because Fanconi anaemia, Holt-Oram syndrome, VACTERL association, TAR syndrome and renal or cardiac anomalies may be more important than the wrist deformity.
- Thumb hypoplasia must be classified separately from radius deficiency because pinch and grasp often depend more on the thumb than on the wrist angle.
- Elbow motion matters: a child with a stiff elbow may not gain much function from a straight wrist if the hand still cannot reach the mouth or face.
- Centralisation and radialisation can improve hand position, but recurrence, stiffness and distal ulna physeal problems must be expected and discussed.
- Pollicisation is usually preferred for absent, floating or non-reconstructable thumbs; stable milder thumbs may be reconstructed.
- “Start with the child, not the wrist: screen for systemic disease before planning elective reconstruction.
- “State the radius type and the thumb type separately.
- “Do not treat TAR like typical absent-radius-plus-absent-thumb disease: TAR usually has absent radii with thumbs present.
- “A straight wrist without a useful thumb is not a complete functional reconstruction.
- “Severe rigid deformity may need soft-tissue distraction before wrist realignment.
- “Recurrence is common because growth, soft-tissue imbalance and absent radial support persist.
The wrist may look dramatic, but the dangerous mistakes are medical: missing Fanconi anaemia, thrombocytopenia, cardiac disease, renal anomalies or a syndromic pattern; and functional: ignoring the thumb, elbow or bilateral hand use.
Overview/Epidemiology
Radial longitudinal deficiency is a congenital failure of formation affecting the radial side of the upper limb. Severe cases are often called radial club hand.
The condition can involve:
- radius: short, hypoplastic, partly absent or completely absent;
- radial carpus: deficient support under the hand;
- thumb: mild hypoplasia through to complete absence;
- soft tissues: contracted radial skin, abnormal tendons and abnormal vessels;
- proximal limb: short ulna, bowed ulna, elbow stiffness, weak biceps or shoulder involvement.
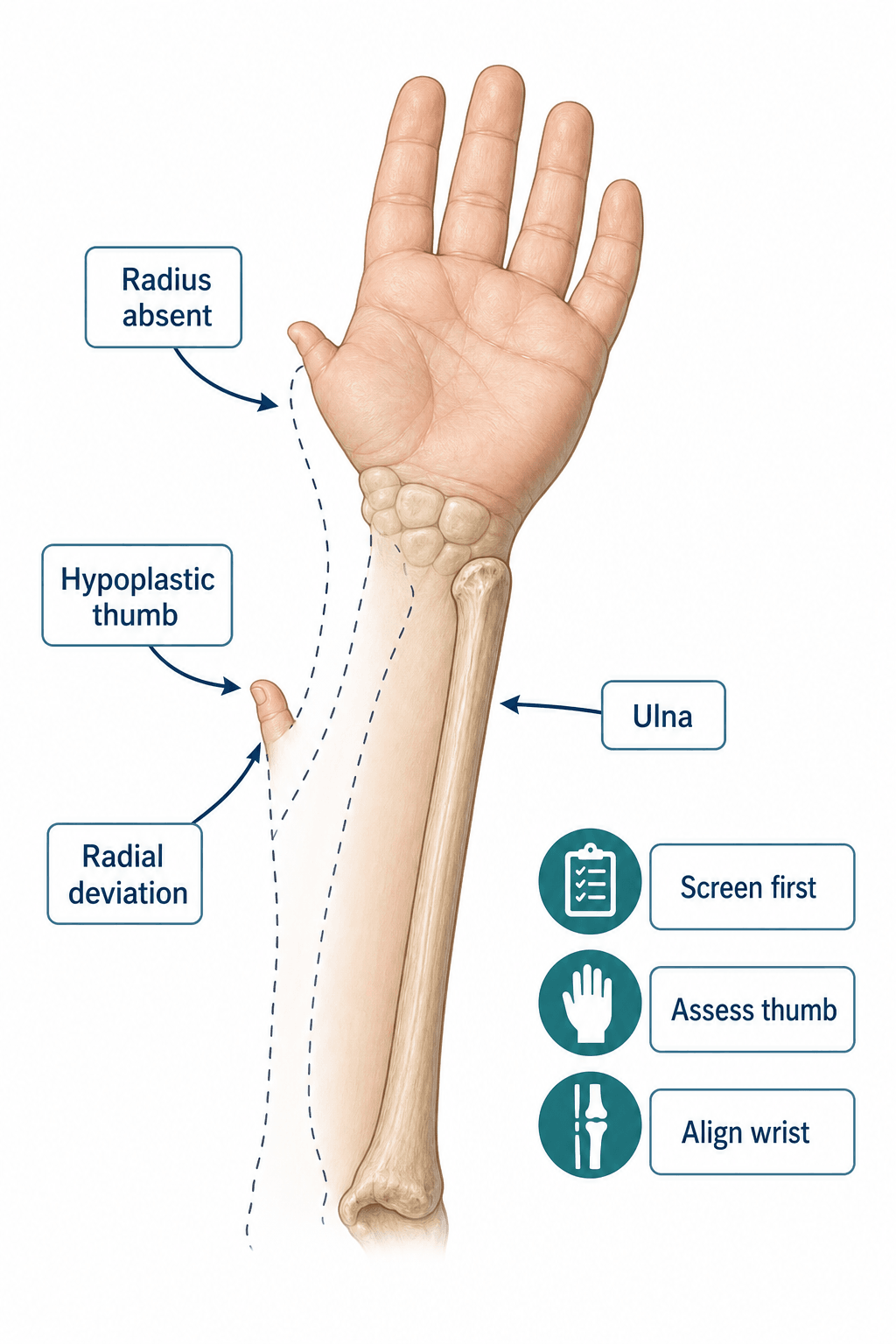
The deformity is usually obvious at birth: a shortened forearm, a bowed ulna, radial deviation of the wrist and a small or absent thumb. The visible wrist deformity does not fully define the child. The same developmental field can be associated with systemic disease and with major functional loss from thumb deficiency, elbow stiffness and bilateral involvement.
Radial longitudinal deficiency is the most common longitudinal deficiency of the upper limb. Severe radial club hand is rare, often quoted around 1 in 100,000 live births, and bilateral involvement is common, reported in roughly half to two-thirds of cases in many teaching references. Reported severity varies by referral population because mild thumb-dominant cases and severe syndromic bilateral cases are not captured in the same way.
For clinical learning, the useful epidemiology is pattern recognition: severe radial deficiency is more likely to be syndromic, bilateral disease is more likely to have systemic associations, and increasing radius severity tends to correlate with increasing thumb deficiency.
Pathophysiology
The radius and thumb belong to the preaxial or radial developmental column. When this column is deficient, the structures on the radial side of the limb are underdeveloped or absent.
The developmental biology is linked to limb-bud patterning of the radial or anterior side of the limb, including the apical ectodermal ridge and sonic hedgehog signalling pathways described in teaching references. Most isolated cases are sporadic, but the clinician must not assume an isolated problem until syndromic disease has been excluded.
The deformity is created by three linked problems:
- Anatomy
- The radius and radial carpus do not support the hand.
- Clinical consequence
- The carpus collapses radially around the distal ulna.
- Anatomy
- Radial skin, tendons, fascia and neurovascular structures may be short.
- Clinical consequence
- Correction may be limited by skin, nerve and vessel tension.
- Anatomy
- The thumb may be hypoplastic, unstable, floating or absent.
- Clinical consequence
- A straight wrist still fails function if pinch is not reconstructed.
The radial artery may be small or absent, radial-sided tendons may be abnormal, carpal bones may be absent or fused, and the ulna is often short and bowed. The elbow may be stiff or unstable. The biceps may be absent or weak in severe limb involvement, which directly affects hand-to-mouth function and surgical planning.
Radius, radial carpus and thumb should be considered together. Classifying only the radius misses the major functional determinant: the thumb.
Radial longitudinal deficiency does not just lack the radial bone column; the radial-side vessels and nerves are themselves abnormal, and this dictates safe surgery. The radial artery is frequently absent or hypoplastic, so the hand is supplied mainly by an enlarged ulnar artery, often with a persistent median artery as a dominant contributor — any plan involving free tissue transfer, distraction or aggressive radial dissection must account for this (do not assume a normal radial artery; assess the vascular pattern with Doppler when it matters). Critically, the median nerve typically lies abnormally radial and superficial in the forearm and wrist, often the most radial neural structure, so it is the structure most at risk during radial soft-tissue release and centralisation — it can be mistaken for a radial-sided tendon or fibrous band and divided, and it commonly supplies the radial skin because the radial-nerve sensory contribution is deficient. The operative lesson: identify and protect the median nerve first on the radial side, and never divide a radial "cord" until you are certain it is not nerve.
Classification

Classification should answer two questions separately: how severe is the radial deficiency, and can the thumb become a useful thumb?
The classic Bayne and Klug system grades radius severity:
- Type I: Mild deficiency with a short distal radius or deficient distal radial epiphysis.
- Type II: Hypoplastic radius with deficient distal and proximal radial epiphyses.
- Type III: Partial absence of the radius, usually distal absence.
- Type IV: Complete absence of the radius; this is the classic severe radial club hand pattern.
Modified systems (James and colleagues) add Type N for thumb hypoplasia with a normal radius and carpus, and Type 0 for radial carpal deficiency with normal radius length. These additions matter because thumb hypoplasia and radial carpal deficiency can belong to the same preaxial spectrum even when the radius appears near normal.
At the level of overall congenital limb classification, radial longitudinal deficiency sits within the Oberg-Manske-Tonkin (OMT) dysmorphology-based system, which the International Federation of Societies for Surgery of the Hand has adopted in place of the older Swanson/IFSSH scheme and which underpins modern registries such as CoULD. For day-to-day reconstructive decisions, the radius (Bayne-Klug) and thumb (modified Blauth) grades remain the working tools.
Do not say "Type IV radius, therefore centralise." Radius type describes anatomy; it does not by itself decide surgery. The thumb, elbow, wrist flexibility, systemic diagnosis, family goals and adaptive function decide treatment.
Associated Conditions
Associated disease is common enough that screening is part of the diagnosis. A child with radial deficiency should not be treated as an isolated hand problem until systemic conditions have been considered.
- Pattern to recognise
- Radial ray anomaly, thumb hypoplasia, short stature or other congenital anomalies.
- Why it matters
- Bone marrow failure may not be obvious at birth; CBC can be normal early, so genetics or haematology may arrange chromosomal breakage testing when suspected.
- Pattern to recognise
- Radial ray upper-limb anomaly with congenital heart disease or conduction disease.
- Why it matters
- Requires cardiac assessment before elective reconstruction.
- Pattern to recognise
- Vertebral, anal, cardiac, tracheo-oesophageal, renal and limb anomalies.
- Why it matters
- Life-threatening neonatal issues may take priority over hand reconstruction.
- Pattern to recognise
- Absent radii, usually bilateral, with thumbs usually present and thrombocytopenia.
- Why it matters
- Platelet count and haematology planning are central; the present thumb is the clue.
- Pattern to recognise
- No systemic diagnosis after appropriate screen.
- Why it matters
- Management can focus more directly on function, thumb and wrist position.
Practical screening usually includes a full paediatric assessment, renal ultrasound, echocardiogram and complete blood count with platelet count. Genetics and haematology review are added when the pattern suggests Fanconi anaemia, TAR syndrome, Holt-Oram syndrome, VACTERL association or another syndromic diagnosis. Fanconi assessment may require chromosome breakage testing with agents such as diepoxybutane or mitomycin C, because marrow failure may evolve after infancy.
Differentiating the syndromic causes
The most exam-relevant decision is distinguishing the radial-ray syndromes from one another, because they carry very different systemic risks and treatment timing. The thumb is the single most useful discriminator: in TAR syndrome the thumbs are characteristically present despite absent radii, whereas Fanconi anaemia and Holt-Oram syndrome typically involve the thumb.
- Radius / thumb pattern
- Absent radii, usually bilateral, with thumbs present.
- Inheritance / gene
- Autosomal recessive; RBM8A.
- Key systemic clue
- Neonatal thrombocytopenia that often improves with age; cow's milk intolerance.
- Decisive test
- Platelet count and haematology review.
- Radius / thumb pattern
- Radial ray and thumb hypoplasia or aplasia; short stature.
- Inheritance / gene
- Mostly autosomal recessive; FANC genes.
- Key systemic clue
- Progressive marrow failure (may be normal at birth); cancer predisposition; cafe-au-lait spots.
- Decisive test
- Chromosomal breakage test (DEB / mitomycin C).
- Radius / thumb pattern
- Radial ray with thumb anomaly (often triphalangeal or absent thumb).
- Inheritance / gene
- Autosomal dominant; TBX5.
- Key systemic clue
- Congenital heart disease and conduction defects.
- Decisive test
- Echocardiogram, ECG and TBX5 testing.
- Radius / thumb pattern
- Limb (radial) defect as one component; thumb pattern similar to general cohort.
- Inheritance / gene
- Sporadic; non-Mendelian.
- Key systemic clue
- Vertebral, anal, cardiac, tracheo-oesophageal, renal anomalies.
- Decisive test
- Spine imaging, echocardiogram, renal ultrasound, assessment for atresias.
- Radius / thumb pattern
- Radial deficiency without systemic disease.
- Inheritance / gene
- Usually sporadic.
- Key systemic clue
- Normal screen.
- Decisive test
- Diagnosis of exclusion after appropriate screen.
Bilateral absent radii with thumbs present is TAR until proven otherwise. Check the platelet count urgently before any procedure.
Clinical Presentation
- Typical findings
- Short forearm, bowed ulna, radial deviation of the hand, small or absent thumb.
- Clinical meaning
- Recognise radial longitudinal deficiency and start systemic screening.
- Typical findings
- Complete absent radius, rigid radial deviation, tight radial skin, wrist unable to passively correct to neutral.
- Clinical meaning
- Early splinting may help, but definitive reconstruction may need staged soft-tissue preparation.
- Typical findings
- Thumb hypoplasia, radial carpal deficiency, subtle forearm shortening or weak pinch.
- Clinical meaning
- The thumb may be the main functional problem even when the wrist looks acceptable.
- Typical findings
- Difficulty with pinch, grasp, dressing, feeding, writing, hygiene, brace tolerance or cosmetic concern.
- Clinical meaning
- Treatment should be judged by independence and function, not appearance alone.
- Typical findings
- Fixed radial deviation, stiff wrist, limited elbow motion, absent pinch and established adaptive ulnar grasp.
- Clinical meaning
- Reconstruction must prove it will improve function rather than disrupt adaptation.
Bilateral involvement deserves special attention because the child may rely on adaptive grasp and compensatory shoulder or trunk movement. In severe cases the hand may lie almost perpendicular to the forearm, but visual severity still has to be interpreted against actual function.
History
The history should explain the child's safety, associated diagnoses and functional priorities before any wrist or thumb operation is discussed.
- Ask about
- Prenatal ultrasound, birth history, neonatal admissions and feeding problems.
- Why it matters
- May reveal syndromic or life-threatening associated disease.
- Ask about
- Cardiac symptoms, renal issues, infections, bruising, platelet problems, previous haematology or genetics review.
- Why it matters
- Guides Fanconi, TAR, Holt-Oram and VACTERL workup.
- Ask about
- Unilateral or bilateral involvement, other limb anomalies, spine, anorectal or tracheo-oesophageal anomalies.
- Why it matters
- Bilateral disease and extra-limb anomalies increase syndromic suspicion.
- Ask about
- Hand-to-mouth movement, grasping objects, splint tolerance and skin problems.
- Why it matters
- Shows whether early positioning is helping or harming function.
- Ask about
- Pinch, grasp, cutlery, dressing, toileting, writing, sport, pain, fatigue, teasing and brace tolerance.
- Why it matters
- Defines the real treatment goal.
Families may understandably focus on appearance. The clinical discussion should translate appearance into function: reach, pinch, grasp, hygiene, play, writing and independence.
Examination
Examine the whole child first, then both upper limbs. The hand is assessed last only because its function depends on the proximal limb and systemic diagnosis.
- What to examine
- Dysmorphic features, short stature, bruising, cardiac signs, spine anomalies, abdominal or anorectal scars, renal clues and other limb deficiencies.
- Decision it informs
- Identifies systemic disease and surgical risk.
- What to examine
- Shoulder range, elbow flexion and extension, biceps function, hand-to-mouth reach.
- Decision it informs
- Decides whether wrist realignment will improve reach or remove compensation.
- What to examine
- Forearm length, ulna bowing, ulnar head position, radiohumeral or radioulnar abnormality.
- Decision it informs
- Defines reconstructive platform and growth expectations.
- What to examine
- Direction and severity of deviation, flexion posture, passive correctability, radial skin tightness and active wrist control.
- Decision it informs
- Separates supple deformity from rigid deformity that may need distraction.
- What to examine
- Thumb size, first web, sensibility, CMC/MCP stability, thenar bulk, opposition and active motion.
- Decision it informs
- Decides reconstruction versus pollicisation.
- What to examine
- Index mobility, sensibility, finger motion, grip pattern and ulnar-digit function.
- Decision it informs
- Confirms suitability for pollicisation and expected hand function.
- What it means
- Improved wrist position may not improve reach.
- Management consequence
- Set realistic goals; avoid wrist-only planning.
- What it means
- The child may have limited active elbow flexion.
- Management consequence
- Be cautious about wrist realignment if it reduces adaptive hand-to-mouth positioning.
- What it means
- Soft tissues can be corrected more safely.
- Management consequence
- Stretching, splinting and realignment may be easier.
- What it means
- Skin, nerve and vessel stretch risk is higher.
- Management consequence
- Consider staged distraction or modified reconstruction.
- What it means
- Thumb can potentially be preserved.
- Management consequence
- Web deepening, stabilisation and opponensplasty may be appropriate.
- What it means
- Poor native pinch potential.
- Management consequence
- Index pollicisation is usually the functional option.
It is unsafe to plan a wrist operation before checking for cardiac disease, renal anomalies, platelet problems, Fanconi anaemia risk, VACTERL features, elbow flexion, biceps function and thumb reconstructability. These are not optional extras; they determine whether surgery is safe and whether it will help.
Investigations
Radiographs

Obtain AP and lateral radiographs of the hand, wrist and forearm. Include the elbow if elbow motion is abnormal or the proximal forearm anatomy is unclear. In infants, remember that carpal and epiphyseal anatomy is partly cartilaginous, so classification may need repeat radiographs as ossification progresses.
Radiographs should define:
- Radius presence, length and distal physis.
- Ulna length, bowing and distal physis.
- Carpal alignment and radial carpal deficiency.
- Thumb metacarpal and phalanges.
- Elbow and proximal forearm abnormalities when clinically relevant.
Medical workup
The basic screen is chosen to answer safety questions before elective reconstruction:
- What it looks for
- Thrombocytopenia, anaemia or evolving marrow disease.
- Decision it affects
- TAR syndrome, Fanconi concern, bleeding risk and timing of surgery.
- What it looks for
- Fanconi anaemia, usually through genetics or haematology.
- Decision it affects
- Anaesthetic planning, marrow surveillance, cancer risk and whether elective reconstruction is appropriate.
- What it looks for
- Structural heart disease and conduction disease, especially Holt-Oram pattern.
- Decision it affects
- Anaesthetic safety and perioperative planning.
- What it looks for
- Renal agenesis, ectopia, reflux-associated anatomy or other renal anomalies.
- Decision it affects
- Medical care, syndromic diagnosis and operative timing.
- What it looks for
- VACTERL-associated anomalies.
- Decision it affects
- Neonatal priorities may completely override hand reconstruction.
Additional tests
Ultrasound may help in borderline thumb hypoplasia by assessing CMC stability and cartilaginous structures, but treatment is still based on clinical function, stability and reconstructability. CT and MRI are not routine for most infants, but may be used selectively for complex anatomy or revision planning.
Radial longitudinal deficiency is increasingly detected before birth on routine antenatal ultrasound (a short, radially deviated forearm with an absent or hypoplastic radius). An antenatal finding should not be treated as an isolated limb problem: it is a prompt to search for associated anomalies (detailed fetal cardiac, renal and spinal imaging for Holt-Oram, VACTERL and related patterns) and to offer genetic counselling and testing — considering Holt-Oram (autosomal dominant, TBX5), TAR (autosomal recessive, RBM8A) and Fanconi anaemia, with karyotype/targeted testing or chromosome-breakage testing as the pattern suggests. This lets the family be counselled before delivery, the birth be planned in an appropriate unit, and the newborn screening pathway (echocardiogram, renal ultrasound, full blood count) be arranged from day one rather than after a delayed referral. Recurrence-risk counselling depends entirely on the underlying diagnosis — high for an autosomal dominant syndrome such as Holt-Oram, low for a truly sporadic isolated case.
Images and Radiology
- High-yield answer
- A preaxial deficiency involving radius, radial carpus, thumb and radial soft tissues.
- Why it matters
- Explains why the deformity is more than a bent wrist.
- High-yield answer
- Rare; severe radial club hand is often quoted around 1 in 100,000 live births, with bilateral disease in roughly half or more of cases.
- Why it matters
- The exact number varies by definition, but the rarity and bilateral pattern are useful for recognition and counselling.
- High-yield answer
- Heart, kidneys, blood count and syndromic/genetic associations.
- Why it matters
- Systemic disease may change timing, anaesthetic safety and prognosis.
- High-yield answer
- Thumb stability, first web space, opposition, finger motion, sensibility and elbow motion.
- Why it matters
- Wrist alignment alone does not restore pinch or reach.
- High-yield answer
- Place the hand in a more useful position on the ulna while preserving skin, neurovascular structures and growth.
- Why it matters
- The goal is function and care, not a perfectly straight radiograph.
- High-yield answer
- Recurrent radial deviation, stiffness and short ulna.
- Why it matters
- Families need long-term expectations before surgery.
RADIUSAssessment Sequence
Hook:RADIUS keeps the answer wider than the wrist.
THUMBThumb Decision
Hook:THUMB keeps the treatment focused on pinch.
SAFESystemic Screen
Hook:SAFE prevents a cosmetic wrist-only answer.
Non-Operative Treatment
Non-operative treatment starts early and continues even if surgery is planned. It has two aims: protect current function and prepare the limb for safer future reconstruction if surgery becomes useful.
- What it involves
- Explain the diagnosis, associated screening, realistic function and recurrence risk.
- What it achieves
- Prevents a cosmetic-only understanding of treatment.
- What it involves
- Regular radial soft-tissue stretching within comfort.
- What it achieves
- Maintains supple tissue and may improve later correction.
- What it involves
- Resting or corrective splints to improve wrist position without skin pressure.
- What it achieves
- Improves positioning and may prepare soft tissues; it does not create a radius.
- What it involves
- Grasp practice, bimanual use, adaptive play, feeding and later school tasks.
- What it achieves
- Builds practical hand use rather than just alignment.
- What it involves
- Monitor radial skin, splint pressure, hygiene and irritation.
- What it achieves
- Prevents avoidable wounds in a limb with abnormal soft tissue.
- What it involves
- Encourage safe adaptive grasp and independence, especially in bilateral disease.
- What it achieves
- Protects the child's current abilities while decisions mature.
Observation is appropriate for mild radius deficiency, good function, high medical risk, well-adapted bilateral hands, or families who do not want reconstruction. Observation is not neglect if the child is functioning well and systemic screening has been completed.
The wrist position may look abnormal, but treatment is chosen by what the child can do: reaching the mouth, grasping, pinching, hygiene, play and later writing. A brace and therapy can be the right treatment when function is good.
Observation is unsafe if it means ignoring systemic screening, progressive skin problems, loss of useful grasp, severe brace intolerance or a thumb that cannot provide pinch.
Management Framework
Management is staged. The sequence is screening, therapy, thumb planning, wrist planning and long-term follow-up. The decision is made from function and safety, not from appearance alone.
- Decision
- Is there cardiac, renal, haematological or syndromic disease?
- Management
- Complete paediatric, cardiology, renal, genetics and haematology workup as indicated before elective reconstruction.
- Decision
- What does the child need the hand to do?
- Management
- Define reach, pinch, grasp, hygiene, writing, bilateral use and adaptive strategies.
- Decision
- Is the thumb stable and reconstructable?
- Management
- Reconstruct milder thumbs; pollicise absent, floating or non-reconstructable thumbs.
- Decision
- Is wrist position limiting function and can it be corrected safely?
- Management
- Stretch and splint early; consider distraction, centralisation or radialisation in selected severe deformity.
- Decision
- How will correction be maintained?
- Management
- Night splints, therapy, surveillance and revision only when function justifies it.
Complete the medical screen before elective reconstruction. CBC and platelet count, renal ultrasound, echocardiography, paediatric review and genetics or haematology input are used according to the clinical pattern.
- Usual direction
- Observation, splinting and therapy.
- Rationale
- Surgery may add stiffness or scarring without improving independence.
- Usual direction
- Delay elective reconstruction until medically safe.
- Rationale
- Hand surgery is not urgent if systemic disease is unsafe.
- Usual direction
- Plan pollicisation rather than repeated weak thumb salvage.
- Rationale
- A stable opposable thumb is more useful than preserving a non-functional ray.
- Usual direction
- Consider centralisation, radialisation or staged distraction.
- Rationale
- Wrist position may be worth correcting when it changes practical use.
- Usual direction
- Be cautious about wrist realignment.
- Rationale
- Straightening the wrist can reduce the child's compensatory reach.
Thumb Treatment
Thumb treatment is often the most important functional decision. In practical terms, the question is: can this thumb become a stable sensate post for opposition, or is the index finger a better future thumb?
- Typical treatment direction
- Observation or minor support if function is good.
- Reasoning
- The thumb is small but usually stable.
- Typical treatment direction
- First web deepening, MCP stabilisation and opponensplasty when needed.
- Reasoning
- The thumb can often be made stable and opposable.
- Typical treatment direction
- Reconstruction if the CMC joint is stable and soft tissues are adequate.
- Reasoning
- The base can support pinch if the deficient components are corrected.
- Typical treatment direction
- Usually pollicisation.
- Reasoning
- An unstable or absent CMC base makes durable reconstruction unreliable.
- Typical treatment direction
- Index pollicisation.
- Reasoning
- A floating or absent thumb cannot provide stable opposition.
Reconstructable thumb
Milder thumbs are treated by correcting the components that prevent pinch:
- first web narrowing: first web release or deepening;
- MCP instability: ligament reconstruction or joint stabilisation;
- weak opposition: opponensplasty, commonly using FDS or abductor digiti minimi depending anatomy and surgeon preference;
- tendon imbalance: tendon transfer or balancing;
- deficient extension or flexion: reconstruct selectively if it changes function.
The aim is not simply to preserve five digits. The aim is a stable sensate thumb that can oppose the fingers. If the CMC joint is stable, the thumb has useful skin and sensibility, and the family accepts staged reconstruction, reconstruction is reasonable. If the base is unstable or absent, repeated reconstruction usually produces a weak thumb and delays better function.
Non-Reconstructable Thumb
Types IIIB, IV and V usually require index pollicisation. The family may worry that the operation removes a finger. The explanation should be functional: the index finger is repositioned to create a thumb-like post that can oppose the remaining fingers.
Timing is individualised, but pollicisation is commonly planned in infancy or early childhood, often around 12 to 18 months when the child is developing more complex grasp and before strong maladaptive pinch patterns become fixed. It may be delayed if medical screening is incomplete, the child is medically unfit, the index finger is unsuitable, or the family is not ready for the decision.
Principles of pollicisation:
- Position: supine, arm table, tourniquet, magnification and careful marking before exsanguination.
- Incisions and flaps: design dorsal and palmar flaps to create a broad first web and a sensate pulp-facing thumb.
- Planes: raise flaps carefully, preserve both neurovascular bundles to the index finger and mobilise tendons without devascularising the digit.
- At-risk structures: digital arteries, digital nerves, extensor mechanism, flexor sheath and skin bridge vascularity.
- Deformity correction: shorten the index metacarpal, rotate and pronate the digit, and place it in palmar abduction and opposition.
- Repair and balancing: stabilise the new thumb, rebalance flexors, extensors and intrinsics, and secure a thumb posture that can oppose the fingers.
- Aftercare: cast or splint protection, wound review, pin removal if used, then hand therapy for pinch, grasp and cortical relearning.
- Warnings: poor flap design, neurovascular injury, malrotation, web contracture or weak opposition can produce a thumb that looks acceptable but does not function.
In thumb hypoplasia, the decision between reconstruction and pollicisation depends heavily on whether the CMC joint can provide a stable base for opposition.
Wrist Reconstruction
Wrist reconstruction is considered when radial deviation and carpal malalignment limit function, care or brace positioning enough to justify surgery. The operation should not be described as simply "straightening the hand." It is an attempt to place the carpus in a more useful position on the distal ulna while protecting growth and soft tissues.
- Reasonable strategy
- Centralisation or radialisation may be considered.
- Key caution
- Protect the distal ulnar physis and counsel recurrence.
- Reasonable strategy
- Staged distraction before definitive reconstruction.
- Key caution
- Avoid acute nerve, vessel and skin tension.
- Reasonable strategy
- Radialisation may be preferred by some surgeons.
- Key caution
- Evidence is technique-dependent and mostly case-series based.
- Reasonable strategy
- Observation or very cautious reconstruction.
- Key caution
- Straightening the wrist may reduce hand-to-mouth function.
- Reasonable strategy
- Continue splinting, therapy and surveillance.
- Key caution
- Do not operate for radiographs alone.
Timing
Timing varies between centres. Classical reconstruction is often planned after medical screening and soft-tissue preparation, commonly around 6 to 12 months for severe deformity in centres that operate early. Surgery may be delayed or modified if the child has significant cardiac disease, thrombocytopenia, marrow disease, infection risk, poor soft tissue, severe elbow stiffness or excellent adaptive function without surgery.
The timing decision should also account for the thumb plan. If a child needs pollicisation, the wrist position may need to be improved enough to give the new thumb a useful platform. In bilateral disease, procedures are staged so the child is not left without a usable hand during recovery.
Centralisation
Centralisation places the carpus over the distal ulna. It is considered when the wrist is severely radially deviated, passively correctable or made correctable, and improved alignment is expected to help grasp, hygiene, splinting or thumb reconstruction.
Centralisation principles:
- Position: supine, arm on hand table, tourniquet, image intensifier available, and the whole upper limb prepared so elbow and wrist position can be assessed.
- Incision and approach: dorsal or dorsoradial approach depending surgeon preference and skin deficiency; plan skin so closure does not strangulate the radial side.
- Planes: release contracted radial soft tissues, identify abnormal tendons, preserve useful extensor and flexor units, and expose the carpus and distal ulna.
- At-risk structures: radial-sided neurovascular structures, ulnar neurovascular bundle, extensor tendons, skin flaps and especially the distal ulnar physis.
- Deformity correction: prepare a socket or receiving surface in the carpus as required, translate the carpus onto the distal ulna, correct radial deviation and avoid excessive acute tension.
- Repair and fixation: stabilise with K-wire fixation, commonly from carpus into ulna, and rebalance tendons such as ECU or radial wrist tendons according to local technique and anatomy.
- Aftercare: cast protection, pin care and removal, then long-term splinting and therapy to preserve finger motion and maintain position.
- Warnings: do not damage the distal ulnar physis; do not over-tighten skin or nerves; do not judge success by immediate radiographic straightness alone.
Radialisation
Radialisation places the hand slightly ulnar to the ulna and rebalances tendons to counter the tendency for recurrent radial deviation. Several modifications exist. The principle is to avoid simply balancing the carpus on the ulna in a way that recurrent radial pull can easily reverse.
Radialisation is considered by surgeons who want a mechanical bias against recurrence, especially in severe Type IV deformity or recurrence-prone wrists. The decision is centre- and surgeon-dependent because the evidence is mostly case series, but the concept is important: the hand is intentionally positioned to the ulnar side, and tendon transfers are used to create an ulnar correcting force.
Radialisation principles:
- Position and exposure are similar to centralisation.
- Correction is directed beyond simple neutral alignment, placing the carpus in a slight ulnarised position relative to the ulna.
- Tendon balancing is a key part of the operation; available wrist and finger tendons are redirected to oppose radial deviation.
- Fixation and aftercare still require K-wires or equivalent fixation, casting, splinting and prolonged therapy.
- Warnings are the same as centralisation: skin compromise, stiffness, neurovascular stretch, distal ulna growth injury and recurrence.
Distraction-assisted correction
Severe rigid deformity may need preoperative distraction to reduce radial soft-tissue tension. This is most useful when the wrist cannot be brought near neutral without excessive skin, nerve or vessel tension.
Distraction is usually performed with an external fixator across the forearm and hand, gradually correcting the hand position before definitive centralisation or radialisation. It can make later realignment safer, but it adds pin-site infection risk, family burden, stiffness, pain, frame care and additional follow-up. It should be chosen because it makes reconstruction safer, not because it appears more technically impressive.
Other Surgical Options
- When it is considered
- Bowed ulna obstructs carpal repositioning or contributes to deformity.
- Why it is not routine
- It should serve a reconstructive goal, not cosmetic straightening alone.
- When it is considered
- Carpal repositioning would otherwise create unsafe tension.
- Why it is not routine
- The forearm is already short, so shortening must have a clear safety reason.
- When it is considered
- Selected severe shortening where length would improve reach or reconstructive platform.
- Why it is not routine
- Prolonged frame treatment, pin-site infection, regenerate problems and recurrence are common concerns.
- When it is considered
- Highly selected specialist reconstruction for wrist support or growth potential.
- Why it is not routine
- Specialised, uncommon and not standard first-line treatment in most centres.
Complications
- Complications
- Progressive radial deviation, short forearm, limited reach and weak or absent pinch.
- Clinical lesson
- Untreated severe disease can limit function, but not every visible deformity requires surgery.
- Complications
- Elbow stiffness, weak biceps and limited hand-to-mouth function.
- Clinical lesson
- Wrist reconstruction cannot compensate for poor reach.
- Complications
- Skin necrosis, wound breakdown, neurovascular stretch and splint pressure.
- Clinical lesson
- Correction must respect soft-tissue tension.
- Complications
- Pin-site infection, distal ulna physeal injury, under-correction, over-correction and recurrent radial deviation.
- Clinical lesson
- Protect the distal ulna and counsel recurrence through growth.
- Complications
- Weak pinch after poor thumb reconstruction, stiff fingers or adaptation difficulty after pollicisation.
- Clinical lesson
- Functional success depends on thumb, fingers and therapy, not just wrist alignment.
- Complications
- Need for repeat splinting, revision surgery or later reconstruction.
- Clinical lesson
- Families should expect surveillance through growth.
Recurrence after centralisation or radialisation is not always a technical error. It reflects absent radial support, growth and persistent soft-tissue imbalance.
Follow-Up and Counselling
Counselling should be honest and practical. The aim is a hand that is better positioned for use, hygiene, splinting and appearance, with the best possible pinch. A perfectly straight wrist is not the same as a good functional result.
Follow-up continues through growth.
- What to check
- Position, passive correction, recurrence, splint tolerance and skin.
- Why it matters
- Detects recurrence and splint-related problems early.
- What to check
- Ulna growth, distal ulnar physis and forearm length.
- Why it matters
- Growth changes alignment and may reveal physeal injury.
- What to check
- Elbow motion, biceps function, finger motion, thumb pinch, writing, hygiene and play.
- Why it matters
- Keeps follow-up focused on independence.
- What to check
- Appearance concerns, school function, brace burden and willingness for further procedures.
- Why it matters
- Revision should match a real functional or care goal.
- What to check
- Whether immobilisation or staged surgery would leave the child without a usable hand.
- Why it matters
- Staging must preserve independence.
- Useful answer
- No. Surgery may improve position, pinch platform and care, but it does not create a normal radius or normal growth.
- Why this is honest
- Prevents unrealistic expectations.
- Useful answer
- We first need to check the heart, kidneys, blood and syndromic causes, and we need to understand what the child can already do.
- Why this is honest
- Explains why screening is part of safe treatment.
- Useful answer
- If the thumb cannot become stable, using the index finger to make a new thumb usually gives better pinch.
- Why this is honest
- Frames pollicisation as function, not amputation.
- Useful answer
- Yes. Recurrence is common because the radius is absent or deficient and growth continues.
- Why this is honest
- Prepares the family for splints, surveillance and possible revision.
Decision Traps
- Why it is wrong
- Systemic disease may be life-threatening or change anaesthetic risk.
- Better answer
- Screen medically, then plan limb reconstruction.
- Why it is wrong
- Thumb stability and opposition drive pinch.
- Better answer
- Classify thumb hypoplasia and decide reconstruction versus pollicisation.
- Why it is wrong
- The child may need radial deviation to reach the mouth if elbow flexion is poor.
- Better answer
- Assess shoulder, elbow, biceps and adaptive reach before changing wrist position.
- Why it is wrong
- A straight wrist can still have poor pinch, reach or finger motion.
- Better answer
- Define functional goals before surgery.
- Why it is wrong
- Thumbs are usually present despite absent radii.
- Better answer
- Absent radius plus present thumb should prompt platelet and haematology thinking.
- Why it is wrong
- Recurrence through growth is common.
- Better answer
- Counsel about splints, surveillance and possible revision.
Why It Matters
Radial longitudinal deficiency is a high-yield congenital hand topic because it tests safe clinical priorities. The correct approach is not "straighten the wrist." The correct approach is to decide whether the child is medically safe, whether the thumb can provide pinch, whether the elbow and fingers can use any improved wrist position, and whether surgery will improve function enough to justify recurrence and stiffness risk.
Screen for associated conditions: cardiac disease, renal anomalies, haematological disease and syndromic patterns.
A non-functional thumb may be a bigger disability than the wrist angle. Classify and plan the thumb separately.
Wrist reconstruction can improve position, but recurrence through growth is common.
Some children adapt well. Revision surgery should have a clear functional goal, not just a radiographic goal.
Guidelines, Registries and Global Practice
Radial longitudinal deficiency is rare, so there is no single high-level clinical practice guideline equivalent to those for common adult conditions. Practice is instead shaped by national specialist society teaching, multicentre registries and a body of mostly Level IV evidence. The result is genuine, defensible variation between centres rather than one mandated pathway, and a good exam answer acknowledges this.
Global epidemiology
Radial longitudinal deficiency is the most common congenital longitudinal deficiency of the upper limb. Severe radial club hand is rare, with classic teaching quoting an incidence in the order of 1 in 30,000 to 1 in 100,000 live births depending on definition and case ascertainment. Bilateral involvement is common, reported in roughly half to two-thirds of cases. Population-based birth-defect surveillance and large registries (for example the multinational CoULD registry) confirm the strong association between increasing radial severity and increasing thumb severity, and the higher syndromic burden of bilateral disease.
How major bodies frame the topic
- Position on RLD
- Mandatory systemic screen (renal ultrasound, echocardiogram, full blood count) for every child regardless of severity; thumb classified separately from radius; centralisation outcomes questioned in favour of selective use of radialisation, distraction and joint transfer.
- Evidence level
- Specialist review and registry data (Level IV-V).
- Position on RLD
- Management concentrated in supraregional paediatric hand units; emphasis on early therapy and splinting, multidisciplinary screening and individualised reconstruction; the OMT classification (Edinburgh and others contributing) used for registry and audit.
- Evidence level
- Consensus and unit experience.
- Position on RLD
- Endorses the Oberg-Manske-Tonkin dysmorphology-based classification as the international standard, replacing the Swanson/IFSSH system.
- Evidence level
- Expert consensus, periodically updated.
- Position on RLD
- Similar staged philosophy: screen, therapy, separate thumb and wrist planning; growing interest in growth-preserving techniques (vascularised joint transfer) in selected units.
- Evidence level
- Case series and centre experience.
- Position on RLD
- No condition-specific RLD guideline; care delivered through specialised commissioning of paediatric hand and limb-difference services rather than a discrete technology appraisal.
- Evidence level
- Service specification, not clinical trial guidance.
Registry evidence and practice variation
The CoULD (Congenital Upper Limb Differences) registry and similar databases provide the strongest contemporary data, confirming the radius-thumb severity correlation and syndromic associations rather than head-to-head surgical comparisons (per PubMed: Forman et al., 2020, JBJS Am, PMID 33086350). Because randomised data are absent, the choice between centralisation, radialisation, distraction-assisted correction and vascularised joint transfer is driven by surgeon training, available microsurgical expertise and family goals. High-income specialist centres increasingly favour growth-preserving and recurrence-resistant techniques, while in many settings the dominant unmet need is simply timely access to a paediatric hand service and to systemic screening.
When asked "what is the correct wrist operation," the safe consultant answer is that there is no single mandated procedure: the evidence is Level IV, registries describe associations not comparisons, and selection depends on flexibility, growth, recurrence risk, local expertise and family goals.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A newborn is referred with a short forearm, severe radial deviation of the wrist and an absent thumb.”
“A baby has bilateral absent radii on radiographs, but both thumbs are present.”
“A child with radial longitudinal deficiency has a very small unstable thumb attached by a soft-tissue bridge.”
“A child returns several years after wrist centralisation with recurrent radial deviation.”
“You decide that wrist reconstruction is appropriate. The examiner asks how centralisation is performed.”
Define
- Preaxial upper-limb deficiency
- Radius, radial carpus and thumb spectrum
- Severe cases called radial club hand
- Soft tissue, nerve, vessel and joint abnormalities also matter
Screen
- CBC and platelet count
- Chromosomal breakage testing when Fanconi suspected
- Renal ultrasound
- Echocardiogram
- Genetics or haematology when indicated
- Fanconi, Holt-Oram, VACTERL and TAR
Classify
- Bayne and Klug radius type
- Modified Type N/0 when relevant
- Blauth thumb type
- Unilateral versus bilateral
- Elbow and wrist flexibility
Treat
- Stretching, splinting and therapy
- Reconstruct stable milder thumbs
- Pollicise floating or absent thumbs
- Centralisation: carpus over ulna with soft-tissue release, fixation and tendon balancing
- Radialisation: ulnarised carpal position and tendon balancing to resist recurrence
- Distraction first if severe rigid soft-tissue contracture
Pitfalls
- Wrist-only answer
- No medical screen
- Missing TAR with present thumb
- Ignoring elbow stiffness
- No recurrence counselling
Evidence Base
Systemic screening is part of the diagnosis
- Radial longitudinal deficiency includes bone, muscle, nerve, vessel and joint abnormalities, all of which influence ultimate upper-extremity function.
- The striking limb deformity is often more obvious than the potentially life-threatening associated systemic conditions.
- All children presenting with radial longitudinal deficiency, regardless of severity, require renal ultrasound, echocardiogram and complete blood count to evaluate associated conditions including Fanconi anaemia, Holt-Oram syndrome and the VATER/VACTERL association.