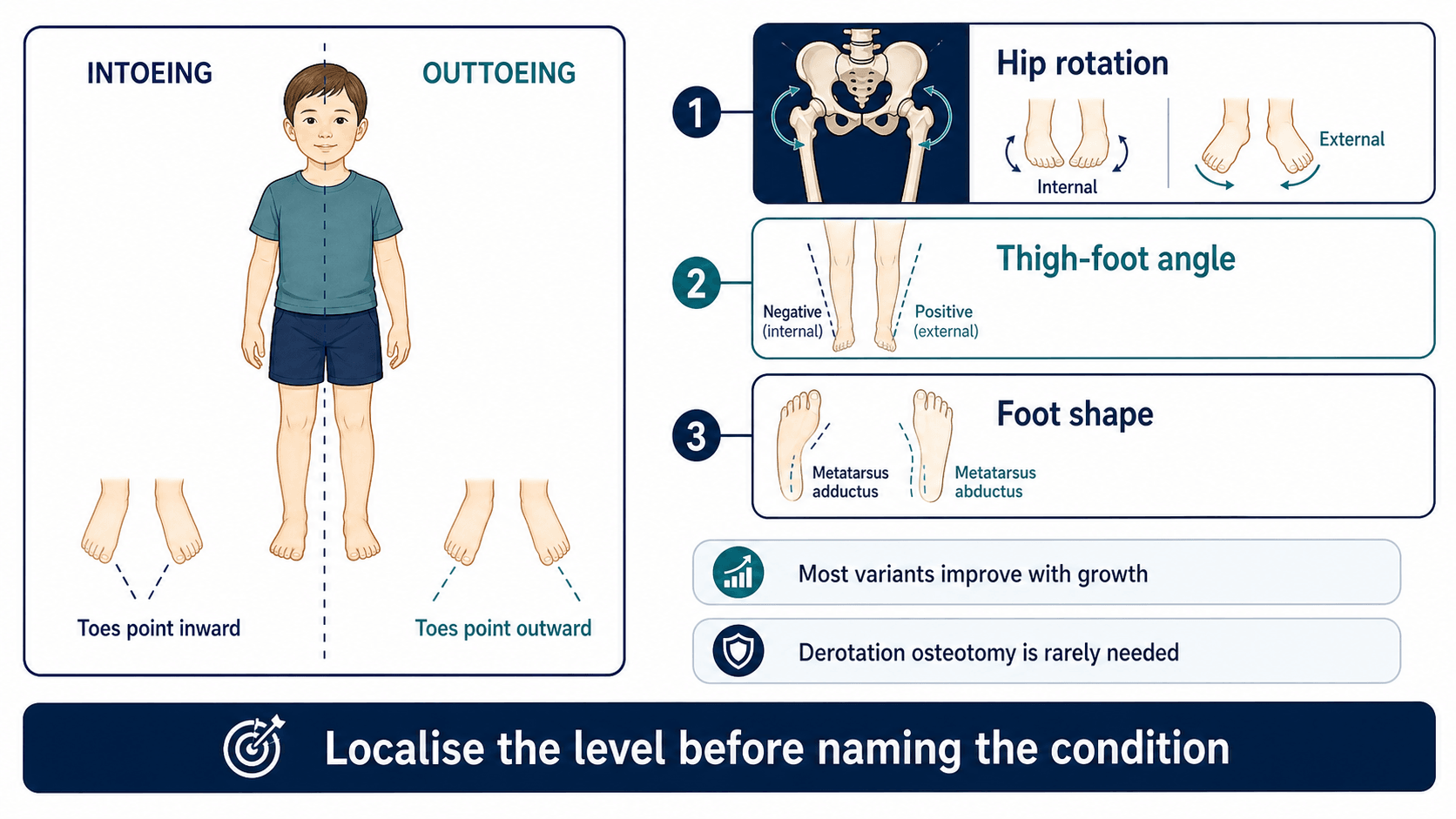
Localise the rotational level before reassuring or escalating
- The three classic in-toeing causes are metatarsus adductus, internal tibial torsion and femoral anteversion.
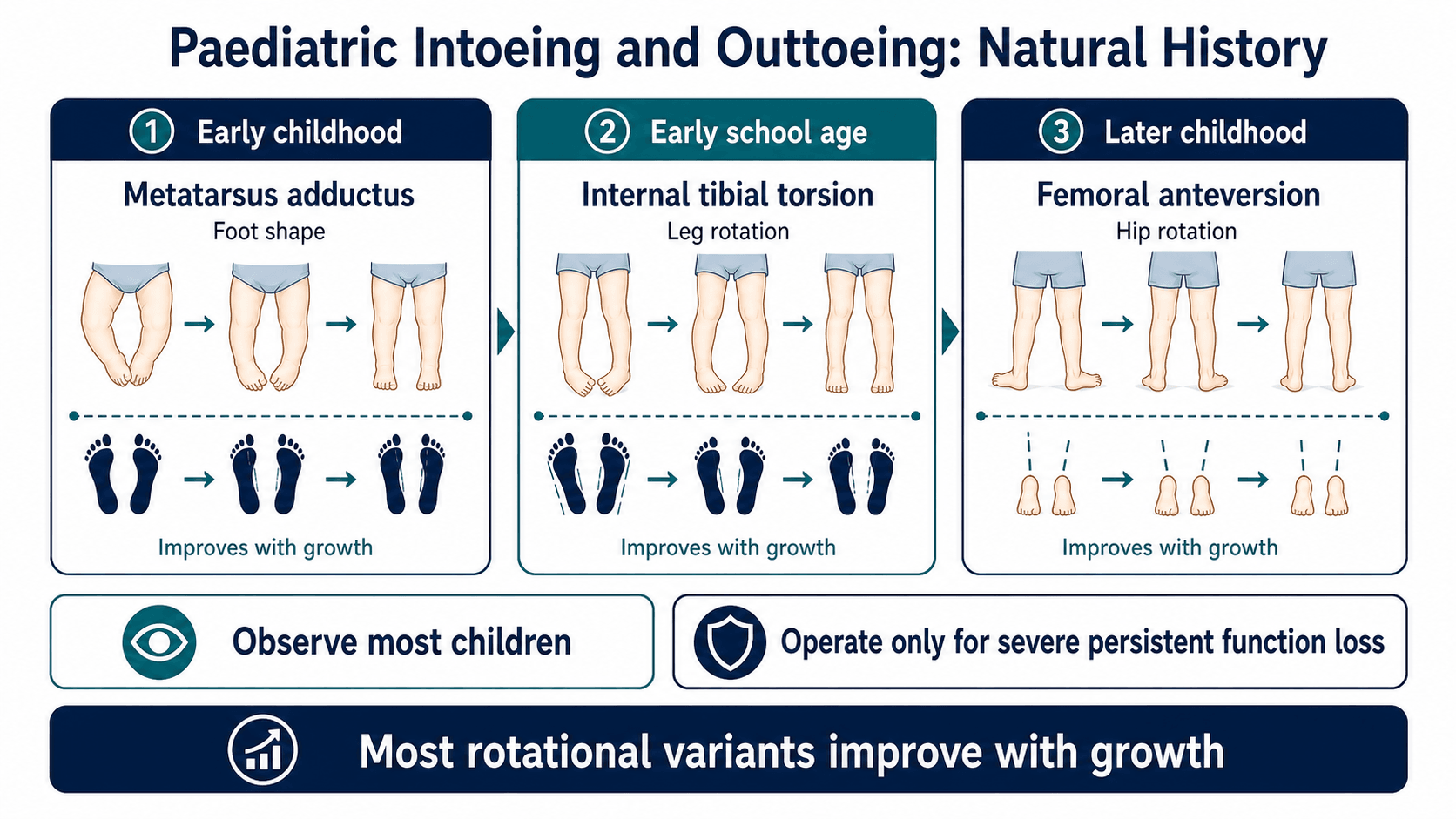
- Most painless symmetric developmental in-toeing improves with growth and does not need braces or special shoes.
- Patella direction during gait helps separate femoral from tibial contribution.
- Painful adolescent out-toeing requires hip assessment and imaging when SUFE or other hip pathology is possible.
- Derotation osteotomy is reserved for selected older children with severe persistent functional deformity.
- “Watch the child walk before putting them on the couch.
- “Name the level: foot, tibia, femur, hip or neuromuscular.
- “W-sitting is associated with femoral anteversion but is not itself an indication for surgery.
- “Reassurance is only safe after pain, asymmetry, progression and neurological signs have been considered.
Typical developmental in-toeing is painless, often symmetric and often improving. Pain, limp, asymmetry, neurological signs, progression or adolescent out-toeing should change the diagnostic pathway.
Images and Diagrams
- Likely level
- Foot
- Clinical meaning
- Metatarsus adductus; assess flexibility.
- Likely level
- Tibia
- Clinical meaning
- Internal tibial torsion.
- Likely level
- Femur
- Clinical meaning
- Femoral anteversion.
- Likely level
- Hip until proven otherwise
- Clinical meaning
- Assess for SUFE or other hip pathology.
WALKClinic Flow
Hook:WALK keeps the clinical assessment sequence practical.
FITCommon In-toeing Levels
Hook:FIT helps localise painless developmental in-toeing.
PAINEscalation Clues
Hook:PAIN prevents unsafe reassurance.
Overview/Epidemiology
Rotational concerns are one of the commonest reasons children are referred to orthopaedics. Parents may describe in-toeing, out-toeing, tripping, unusual running, shoe wear, W-sitting or cosmetic concern. The clinician's job is to identify whether this is a normal developmental variant, a structural rotational deformity causing function problems, a painful hip problem, or a neuromuscular gait issue.
Most typical in-toeing is painless and improves with growth. The common developmental sequence is metatarsus adductus in infancy, internal tibial torsion in toddlers and femoral anteversion in preschool or early school-age children. This timeline is useful, but it is not a substitute for examination.
Reassurance should be specific. Families should hear which level is responsible, what natural history is expected, why braces or special shoes are not useful for typical torsion, and what symptoms should prompt reassessment.
Pathophysiology
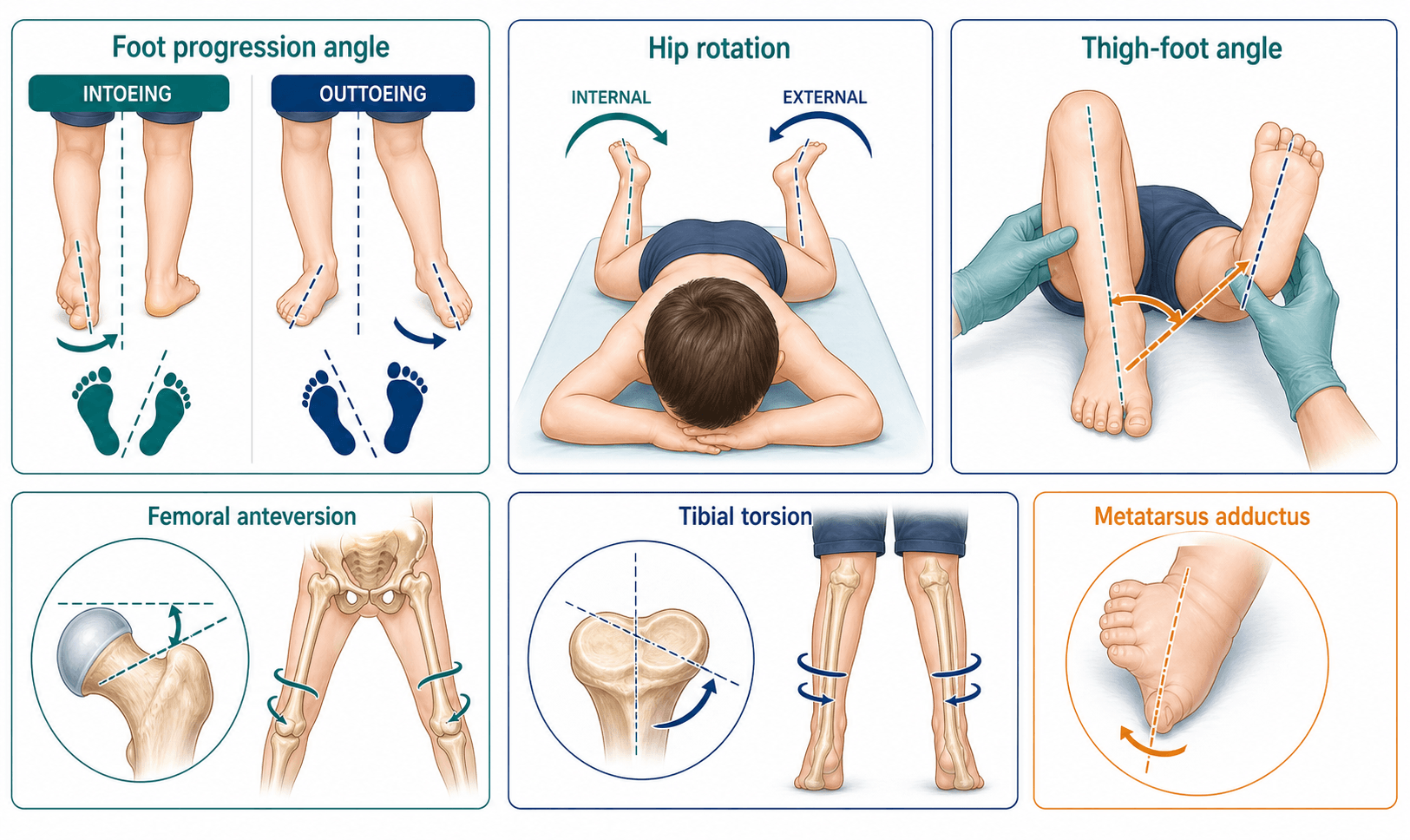
The foot progression angle is the visible result of multiple segments. A foot can point inward because the forefoot is adducted, the tibia is internally rotated, the femur is anteverted, or the child has neuromuscular tone and motor-control issues. The patella is a key clue because it reflects femoral orientation more than foot orientation.
Metatarsus adductus is a foot-shape problem, often related to intrauterine packaging. Flexible forms often improve. Rigid forms require more careful foot assessment.
Internal tibial torsion is common in toddlers. During gait, the patella may face forward while the feet point inward. Many children improve as tibial rotation changes with growth.
Femoral anteversion produces increased hip internal rotation and reduced external rotation. During gait, the patellae point inward, and W-sitting is common. Most cases improve gradually, but severe persistent anteversion can cause tripping, cosmetic concern and functional limitations.
External tibial torsion and femoral retroversion can cause out-toeing. External tibial torsion may become more apparent with growth and may contribute to patellofemoral symptoms. Painful adolescent out-toeing is a different problem: the hip must be considered first, especially SUFE.
Classification
- Metatarsus adductus: curved lateral border of the foot, forefoot adduction and abnormal heel bisector.
- Internal tibial torsion: patella forward but feet point inward; measured with thigh-foot angle.
- Femoral anteversion: patellae point inward, hip internal rotation is increased and external rotation is reduced.
- Neuromuscular in-toeing: tone, weakness, asymmetry or lever-arm dysfunction changes the pattern.
Clinical Presentation
History
Ask what the family sees during real activity. A child may walk acceptably in clinic but trip when tired, run awkwardly or struggle with sport. Establish age of onset, whether the pattern is improving, symmetry, pain, functional limitation and developmental context.
Ask about:
- In-toeing or out-toeing during walking, running or fatigue.
- Tripping, falling, shoe wear, sport limitation or cosmetic concern.
- Pain location: hip, knee, shin, ankle or foot.
- Asymmetry, worsening or sudden change.
- W-sitting, sitting preferences and family history.
- Pregnancy, birth history, milestones and prematurity.
- Neurological symptoms, known cerebral palsy or developmental delay.
Examination
Observe from the front, side and behind. Estimate foot progression angle during natural walking, not just when the child is concentrating. Watch patella direction: inward-facing patellae suggest femoral anteversion, while forward-facing patellae with inward feet suggest tibial torsion.
Measure:
- Hip internal and external rotation, usually prone or supine.
- Thigh-foot angle prone with knees flexed to 90 degrees.
- Foot shape, lateral border, heel bisector and flexibility.
- Coronal alignment, limb length and knee tracking.
- Tone, reflexes, selective motor control, strength and balance when atypical.
- Hip range and obligatory external rotation in painful out-toeing adolescents.
The useful answer is not "the child in-toes". The useful answer is "this is painless symmetric internal tibial torsion" or "this is femoral anteversion with no red flags".
Measuring the Rotational Profile and Normal Values
The rotational profile (Staheli) is the structured set of bedside measurements that localises the deformity to foot, tibia or femur and compares the child against age-related norms - the whole point is to measure rather than treat all in-toeing alike. Each component is simple, free and reproducible.
- How it is taken
- Angle between the long axis of the foot and the line of walking, estimated over several gait cycles
- Approximate normal
- About +10 degrees out-toed (broad range roughly -3 to +20)
- Abnormal means
- Negative (in-toed) or excessively positive overall result of all segments
- How it is taken
- Prone, knees flexed 90 degrees, let the legs fall in and out; record internal and external rotation
- Approximate normal
- Internal and external each broadly up to about 60-70 degrees
- Abnormal means
- Internal rotation high (often over 70) with reduced external rotation suggests increased femoral anteversion; the reverse suggests retroversion
- How it is taken
- Prone, knee flexed 90 degrees, ankle neutral; angle between the thigh axis and the foot axis
- Approximate normal
- About +10 degrees external (range roughly -5 to +30, increasing with age)
- Abnormal means
- Internal (negative) angle indicates internal tibial torsion; large positive indicates external tibial torsion
- How it is taken
- Prone, angle between the thigh axis and a line through both malleoli; isolates the ankle/distal tibia
- Approximate normal
- Increases (laterally) through childhood
- Abnormal means
- Used alongside TFA to confirm tibial torsion and exclude a foot contribution
- How it is taken
- Line bisecting the heel pad on the sole; note where it exits the toes
- Approximate normal
- Passes through the 2nd-3rd toe web
- Abnormal means
- Lateral to this = metatarsus adductus: mild through the 3rd toe, moderate 3rd-4th, severe 4th-5th
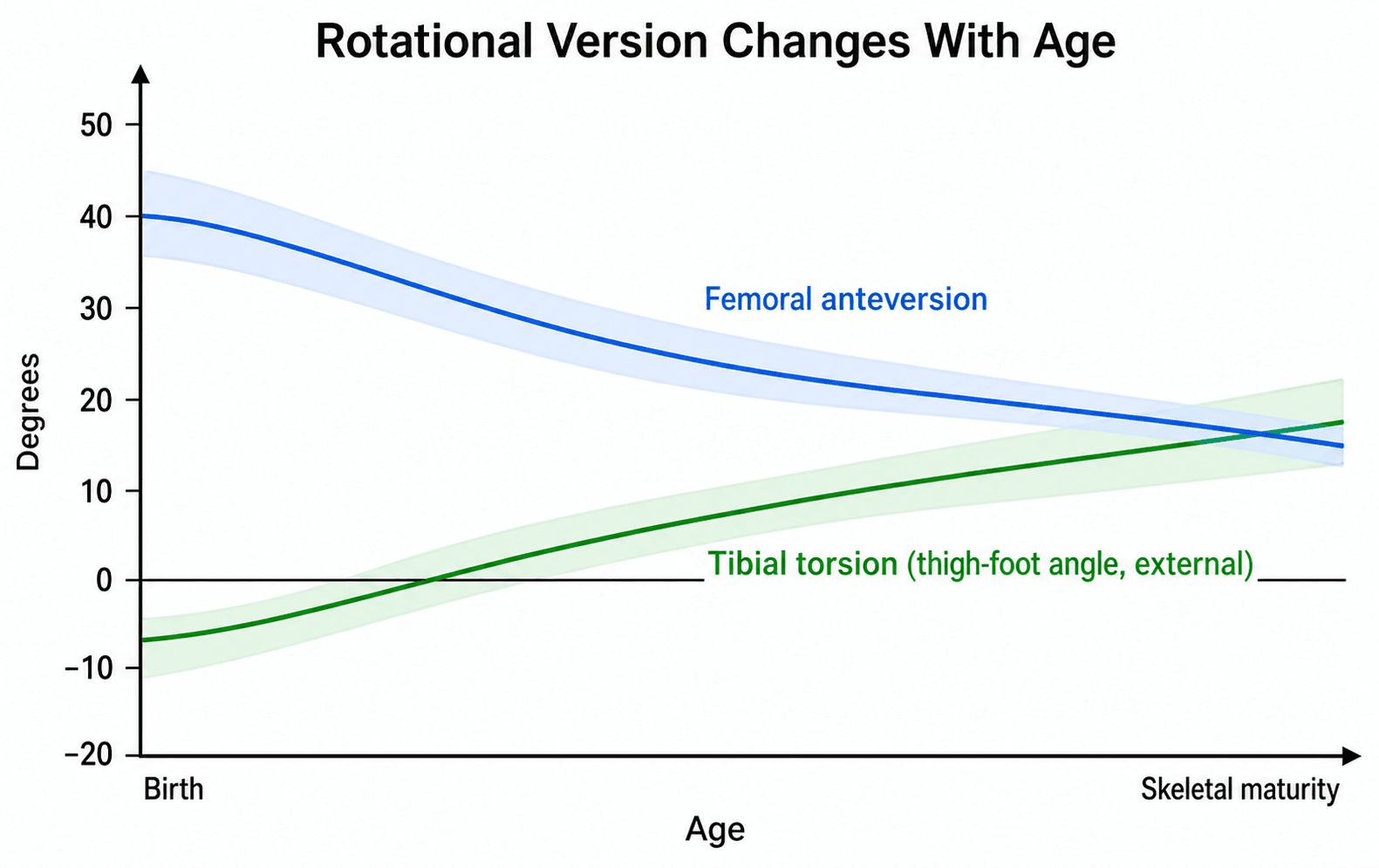
Version is age-dependent, which is why the profile is read against norms: femoral anteversion falls from roughly 30 to 40 degrees at birth to about 15 degrees by skeletal maturity, while the tibia rotates progressively externally, so the same measurement can be normal at one age and abnormal at another.
If the patellae point inward during gait, the rotation is femoral (anteversion). If the patellae face forward but the feet still point inward, the rotation is tibial. The thigh-foot angle then confirms the tibial component and the prone hip-rotation arc confirms the femoral component.
Investigations
Typical painless symmetric in-toeing is a clinical diagnosis and usually does not require imaging. Imaging is for red flags, painful presentations, atypical asymmetry, neuromuscular assessment, suspected hip pathology or surgical planning.
- Investigation
- No routine imaging
- Decision it informs
- Clinical diagnosis, reassurance and review triggers.
- Investigation
- AP pelvis and lateral hip radiographs
- Decision it informs
- Excludes SUFE or other hip pathology.
- Investigation
- CT or MRI rotational profile
- Decision it informs
- Quantifies femoral and tibial version for planning.
- Investigation
- Video, gait analysis and relevant imaging in selected cases
- Decision it informs
- Links torsion to lever-arm dysfunction and treatment planning.
- Investigation
- Standing alignment radiographs
- Decision it informs
- Separates rotational and coronal contributors.
Rotational CT should not be ordered just because a toddler in-toes. It should answer a specific treatment question, usually in an older child with severe persistent functional torsion or complex deformity.
Differential Diagnosis
The differential is best worked through by level (foot, tibia, femur, hip, neuromuscular control), then by whether the picture is benign developmental variation or a pathological signal. The table below distils the discriminating features that separate look-alikes at each level.
- Discriminating feature
- Curved (convex) lateral foot border, forefoot adduction, abnormal heel bisector; hindfoot normal
- Typical age
- Infant
- What separates it from look-alikes
- Deformity is in the foot only; hip rotation and thigh-foot angle are normal.
- Discriminating feature
- Patella faces forward but feet point inward; internal (negative) thigh-foot angle
- Typical age
- Toddler (1 to 3 years)
- What separates it from look-alikes
- Foot and hip are normal; the rotation is in the tibial segment.
- Discriminating feature
- Patellae point inward; hip internal rotation increased and external rotation reduced; W-sitting
- Typical age
- Child 3 to 10 years
- What separates it from look-alikes
- Patella direction (inward) distinguishes it from tibial torsion where patella faces forward.
- Discriminating feature
- Asymmetry, tone, brisk reflexes, toe-walking, lever-arm dysfunction
- Typical age
- Any age
- What separates it from look-alikes
- Abnormal neurology and gait quality; not a smooth symmetric developmental pattern.
- Discriminating feature
- Forefoot adduction with hindfoot valgus (skewfoot) or cavus/equinus residua
- Typical age
- Infant to child
- What separates it from look-alikes
- Mid- and hindfoot deformity, often rigid; needs dedicated foot assessment and weight-bearing radiographs.
- Discriminating feature
- Bilateral out-toeing in the new walker that resolves with growth
- Pain or red flag
- None
- Action
- Reassure and review.
- Discriminating feature
- Feet point outward with patella forward; external (positive) thigh-foot angle
- Pain or red flag
- May cause patellofemoral pain
- Action
- Observe; consider osteotomy only if severe and symptomatic.
- Discriminating feature
- Increased hip external rotation, reduced internal rotation
- Pain or red flag
- Linked to SCFE risk
- Action
- Examine hip; image if painful.
- Discriminating feature
- Obligate external rotation on hip flexion (Drehmann sign), limp, hip/thigh/knee pain
- Pain or red flag
- Major red flag
- Action
- Non-weight bearing; urgent AP and frog-lateral pelvis radiographs.
- Discriminating feature
- Unilateral change after fracture or osteotomy
- Pain or red flag
- Asymmetric
- Action
- Compare sides; rotational imaging if surgery considered.
Miserable Malalignment Syndrome
Miserable malalignment syndrome (also called malicious malalignment) is the combination of increased femoral anteversion and external tibial torsion, often with genu valgum and pes planus. It is the reason the rotational profile must always be read at every level before planning surgery, and why an isolated single-level correction can fail.
The two torsions point in opposite directions, so they partly cancel at the foot: the foot progression angle can look near-normal even though both segments are markedly abnormal. The mismatch is instead concentrated at the knee, producing the classic appearance of inward-facing ("squinting") patellae with the feet pointing straight ahead or out, an increased dynamic Q-angle and a laterally directed quadriceps vector.
- Finding
- Increased femoral anteversion plus external tibial torsion (± genu valgum, pes planus)
- Why it matters
- Two opposite torsions, so the FPA can be deceptively normal
- Finding
- Adolescent, often female, with anterior knee pain or patellar instability
- Why it matters
- Overlaps with patellofemoral pain - the torsion is the underlying driver
- Finding
- Squinting (inward-facing) patellae with feet forward or out-toed
- Why it matters
- Distinguishes it from isolated single-level torsion
- Finding
- Severe symptomatic cases need double-level (femoral and tibial) derotation osteotomy
- Why it matters
- Correcting only one level leaves residual deformity and can worsen symptoms
Before recommending a derotation osteotomy, complete the whole rotational profile. A near-normal foot progression angle does not exclude severe deformity, because a coexisting opposite tibial torsion can mask femoral anteversion. Missing miserable malalignment leads to under-correction or a worse patellofemoral result after isolated single-level osteotomy.
Management
- Typical management
- Observation, parental stretching or casting depending flexibility and severity.
- When to escalate
- Rigid severe deformity, skin crease, failed improvement or associated foot disorder.
- Typical management
- Observation, normal activity and explanation that braces or special shoes do not untwist the tibia.
- When to escalate
- Older child with severe persistent functional limitation after expected improvement window.
- Typical management
- Observation and reassurance when painless and symmetric.
- When to escalate
- Severe persistent in-toeing with tripping, functional limitation, marked cosmetic concern in an older child, or neuromuscular lever-arm dysfunction.
- Typical management
- Assess knee symptoms, patellar tracking and neuromuscular context.
- When to escalate
- Patellofemoral pain or instability, brace intolerance, progressive external foot progression or major lever-arm dysfunction.
- Typical management
- Treat as hip pathology until proven otherwise.
- When to escalate
- Immediate pelvis and lateral hip imaging if SUFE is possible; keep non-weight bearing when suspicious.
Typical painless in-toeing is managed with explanation, normal activity and observation. The explanation should be anatomical and practical: identify the level, explain expected improvement and list red flags. Braces, twister cables and special shoes do not reliably remodel typical femoral or tibial torsion and should not be presented as corrective treatment.
- Femoral derotation
- Severe persistent femoral anteversion or retroversion causing functional gait limitation after natural improvement is unlikely.
- Tibial derotation
- Severe tibial torsion causing functional limitation, patellofemoral symptoms, brace difficulty or neuromuscular lever-arm dysfunction.
- Femoral derotation
- Clinical hip rotation plus CT or MRI version when surgery is being planned.
- Tibial derotation
- Thigh-foot angle, transmalleolar axis and CT/MRI torsion when surgical planning requires precision.
- Femoral derotation
- Usually proximal or subtrochanteric femoral osteotomy depending surgeon preference and fixation strategy.
- Tibial derotation
- Usually distal tibial osteotomy for isolated tibial torsion, with fibular osteotomy when required.
- Femoral derotation
- Plate or intramedullary fixation depending age, bone size and osteotomy level.
- Tibial derotation
- Plate, pins, screws or external fixation depending technique and soft-tissue risk.
- Femoral derotation
- Malrotation, non-union, hardware irritation, hip or knee symptoms and missed combined torsion.
- Tibial derotation
- Compartment syndrome, peroneal nerve injury, malrotation, non-union and hardware symptoms.
Complications
Early
- Over-investigation of normal variants.
- Anxiety from vague reassurance.
- Braces or special shoes prescribed as if they correct torsion.
- Missed SUFE in painful adolescent out-toeing.
- Missed neurological diagnosis in asymmetric or progressive gait.
Late
- Persistent severe torsion with tripping or sport limitation.
- Patellofemoral symptoms, especially with external tibial torsion.
- Lever-arm dysfunction in neuromuscular disease.
- Surgical complications after derotation osteotomy.
- Residual cosmetic concern despite normal function.
Good reassurance is not "they will grow out of it" in isolation. Good reassurance names the level, explains the expected change and gives clear review triggers.
Decision-Making in Practice
Rotational assessment is mainly a clinical skill. Most children with intoeing or out-toeing have physiological variation that improves or becomes asymptomatic, but the clinician must identify asymmetry, progression, pain, neurological disease, slipped epiphysis, patellar instability, severe functional limitation or torsion that will not remodel.
- Interpretation
- Forefoot-driven intoeing in infancy
- Management consequence
- Observe, stretch or cast depending flexibility and severity
- Interpretation
- Toddler intoeing with inward thigh-foot angle
- Management consequence
- Usually observation; surgery only for severe persistent functional deformity
- Interpretation
- Older child intoeing, high hip internal rotation and W-sitting
- Management consequence
- Usually observation; derotation osteotomy only for severe persistent disability
- Interpretation
- Out-toeing, patellofemoral symptoms or lever-arm dysfunction
- Management consequence
- May worsen with growth and can require osteotomy when severe
- Interpretation
- Unilateral change, limp, hip pain, knee pain or neurological signs
- Management consequence
- Investigate for pathology rather than reassuring
A complete rotational profile records foot progression angle, hip rotation, thigh-foot angle, transmalleolar axis, heel bisector, foot shape and gait. The examination should be performed prone and walking, with comparison between sides. Radiographs are not needed for every intoeing child; they are used when there is pain, asymmetry, deformity outside the expected pattern, suspected hip pathology, neuromuscular disease or surgical planning.
Derotation osteotomy is a functional operation, not a cosmetic operation. Indications include severe persistent deformity causing tripping, pain, brace difficulty, patellofemoral instability, lever-arm dysfunction or major gait limitation after physiological improvement is no longer expected.
Clinical Reasoning Notes
Structured clinical approach
Start with the gait and localise:
- "The child has inward foot progression during gait."
- "The patellae face forward, so the main contribution appears tibial."
- "The thigh-foot angle confirms internal tibial torsion."
- "There is no pain, asymmetry, progression or neurological sign."
- "This is a developmental variant; I would reassure and avoid braces."
For a different child:
- "The adolescent has painful out-toeing and a limp."
- "I would not call this external tibial torsion without assessing the hip."
- "I would obtain AP pelvis and lateral hip imaging to exclude SUFE."
Common pitfalls
- Calling every in-toeing femoral anteversion.
- Measuring foot progression but not hip rotation or thigh-foot angle.
- Ignoring patella direction during gait.
- Ordering CT for a typical toddler.
- Missing adolescent SUFE.
- Prescribing braces as if they change bone version.
- Operating too young for cosmetic concern.
- Forgetting neurological screening in asymmetric cases.
Guidelines, Registries & Global Practice
Rotational concerns are among the most common reasons children are referred to orthopaedics worldwide, yet they generate little registry data because most are treated non-operatively. The clinically important point for any global exam is that named societies broadly agree on a conservative, profile-based approach, with surgery reserved for the rare severe symptomatic older child.
Global epidemiology
- In-toeing peaks in toddlers and preschoolers and is one of the commonest paediatric musculoskeletal referrals across all health systems.
- Internal tibial torsion is the commonest cause of in-toeing in toddlers; femoral anteversion predominates in children aged roughly 3 to 10 years; metatarsus adductus presents in infancy.
- Out-toeing is less common than in-toeing and tends to occur in older children; painful adolescent out-toeing carries a disproportionate risk burden because of SCFE.
- Femoral version decreases from around 30 to 40 degrees at birth to roughly 15 degrees by skeletal maturity, which underpins the natural-history counselling given everywhere.
Side-by-side guidance
- Imaging stance
- No routine imaging for typical in-toeing; image for atypical or painful cases.
- Treatment emphasis
- Reassurance and observation; braces, casts and special shoes not recommended for typical torsion.
- Imaging stance
- Clinical diagnosis for benign torsion; radiographs reserved for red flags and suspected hip pathology.
- Treatment emphasis
- Conservative management with clear safety-netting; specialist referral for pain, asymmetry or progression.
- Imaging stance
- Cross-sectional (CT or low-dose) version measurement when surgery is planned.
- Treatment emphasis
- Derotation osteotomy at the correct level for severe symptomatic deformity; precise correction and fixation.
- Imaging stance
- Selective imaging; emphasises rotational profile and gait assessment.
- Treatment emphasis
- Observation for physiological variants; multilevel planning and gait analysis for neuromuscular lever-arm dysfunction.
- Imaging stance
- CT confirmation of version before osteotomy in symptomatic anteversion.
- Treatment emphasis
- Derotation osteotomy effective in carefully selected symptomatic children (Naqvi et al.).
Registry and practice notes
- There is no dedicated international registry for paediatric rotational deformity because the overwhelming majority resolve without surgery; high-quality outcome data come from single-centre series and gait-analysis cohorts rather than arthroplasty-style registries.
- Where derotation osteotomy is performed, most published evidence is Level IV (case series), so practice variation in surgical thresholds is wide and driven by symptom severity and surgeon judgement.
High- versus limited-resource practice variation
- In well-resourced settings, instrumented 3D gait analysis and CT/MRI version measurement support surgical planning, especially in cerebral palsy single-event multilevel surgery.
- In limited-resource settings, the clinical rotational profile (foot progression angle, hip rotation, thigh-foot angle, heel bisector) remains the backbone; it is accurate, free and exam-relevant everywhere. Plain radiographs are universally available for the critical task of excluding SCFE in painful out-toeing.
- The one universal, resource-independent rule: painful adolescent out-toeing is a hip problem until pelvic radiographs prove otherwise.
Controversies and Areas of Uncertainty
- Surgical threshold for idiopathic anteversion. There is no agreed degree of version or foot progression angle that mandates surgery. Decisions rest on function and symptoms in an older child, and the evidence base is largely uncontrolled case series.
- Value of routine version imaging. CT quantifies version but adds radiation; low-dose CT, biplanar (EOS-type) imaging and MRI are increasingly preferred, but no single modality is universally mandated.
- Effectiveness of conservative devices. Twister cables, derotation braces and orthopaedic shoes are not supported for typical torsion; their continued use in some settings reflects parental expectation rather than evidence.
- Predictability of femoral derotation osteotomy. Outcomes are reported as more predictable in adults than children for neuromuscular internal-rotation gait, and recurrence or under-correction can occur; this informs timing and counselling.
- Miserable malalignment. Combined femoral anteversion and external tibial torsion can co-exist and partly cancel out clinically while still causing patellofemoral symptoms; isolated single-level correction may be insufficient and combined torsion must be actively excluded before surgery.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A three-year-old has painless symmetric in-toeing and trips occasionally. How do you assess and counsel?”
“An adolescent presents with painful out-toeing and a limp. What must you exclude?”
“A 10-year-old has marked in-toeing with inward-facing patellae, trips frequently when running and is teased at school. Hip internal rotation is 80 degrees and external rotation is 10 degrees. Parents ask for surgery. How do you decide?”
In-toeing
- Metatarsus adductus
- Internal tibial torsion
- Femoral anteversion
- Neuromuscular
Measure
- Foot progression
- Patella direction
- Hip rotation
- Thigh-foot angle
- Foot shape
Red Flags
- Pain
- Asymmetry
- Progression
- Neurology
- Adolescent out-toeing
Treat
- Reassure typical
- No special shoes
- Image red flags
- Gait analysis selected
- Derotation selected older child
Evidence Signals
Most rotational variations are benign but must be classified clinically
- In-toeing is usually metatarsus adductus in the infant, internal tibial torsion in the toddler and femoral anteversion in the child younger than 10 years.
- Out-toeing patterns largely result from external rotation hip contracture, external tibial torsion and external femoral torsion.
- A deliberate rotational profile assessment is needed to separate benign variation from true structural abnormality.
Normative rotational profile values guide management
- 1,000 normal lower extremities were studied to establish age-related normal values for the rotational profile.
- Out-toeing in infants, medial tibial torsion in toddlers and medial femoral torsion in young children are extremes of a normal developmental pattern.
- In the vast majority, these rotational variations fall within the broad range of normal and require no treatment.
Derotation osteotomy resolves in-toeing in selected symptomatic children
- 21 children (35 limbs, mean age 13.3 years) with symptomatic idiopathic femoral anteversion (mean version 40.8 degrees on CT) underwent proximal femoral derotation osteotomy.
- Foot progression angle improved from 15.2 degrees internal to 7.7 degrees external and tripping, falling and hip pain resolved in all patients.
- Knee pain failed to improve in 3 patients, underlining careful patient selection.
Evidence Base
Primary-care framework for lower extremity rotational and angular problems
- In-toeing is caused by metatarsus adductus, internal tibial torsion and femoral anteversion; out-toeing by external tibial torsion and femoral retroversion.
- Most children have rotational and angular findings within two standard deviations of the mean and resolve spontaneously with growth.
- Orthotics are not beneficial, radiographs are not routinely required, and surgery is rarely needed (typically over age 8 with severe functional deformity).
In-toeing is commonly over-treated with braces and special footwear
- The usual causes of in-toeing are excessive femoral anteversion, internal tibial torsion and metatarsus adductus.
- Because of poor understanding of natural history, in-toeing is commonly over-treated with braces or special footwear.
- Early diagnosis of pathological causes such as cerebral palsy and developmental dysplasia of the hip is essential.
Out-toeing and obligate external rotation should be presumed SCFE until excluded
- Any child with hip, thigh or knee pain, or with out-toeing, decreased internal rotation or obligate external rotation on flexion, should be presumed to have SCFE until proven otherwise.
- There is a high rate of diagnostic delay, allowing deformity progression and conversion of stable to unstable slips with higher avascular necrosis risk.
- Diagnosis is confirmed with AP and frog-lateral pelvis radiographs and treatment is urgent and surgical.
Drehmann sign reflects proximal femoral deformity and impingement in SCFE
- In 92 SCFE hips, a positive Drehmann sign (obligatory external rotation with hip flexion) correlated with higher alpha-angle and radiologic cam-type femoroacetabular impingement.
- Drehmann sign was present in 25 percent, 75 percent and 100 percent of mildly, moderately and poorly remodelled hips respectively.
- The sign is a valuable clinical marker of the anatomic change underlying out-toeing after SCFE.
AAOS family education on in-toeing
- Common causes of in-toeing include metatarsus adductus, tibial torsion and femoral anteversion.
- Most children improve without braces, casts or surgery.
- Persistent severe functional problems require specialist review.