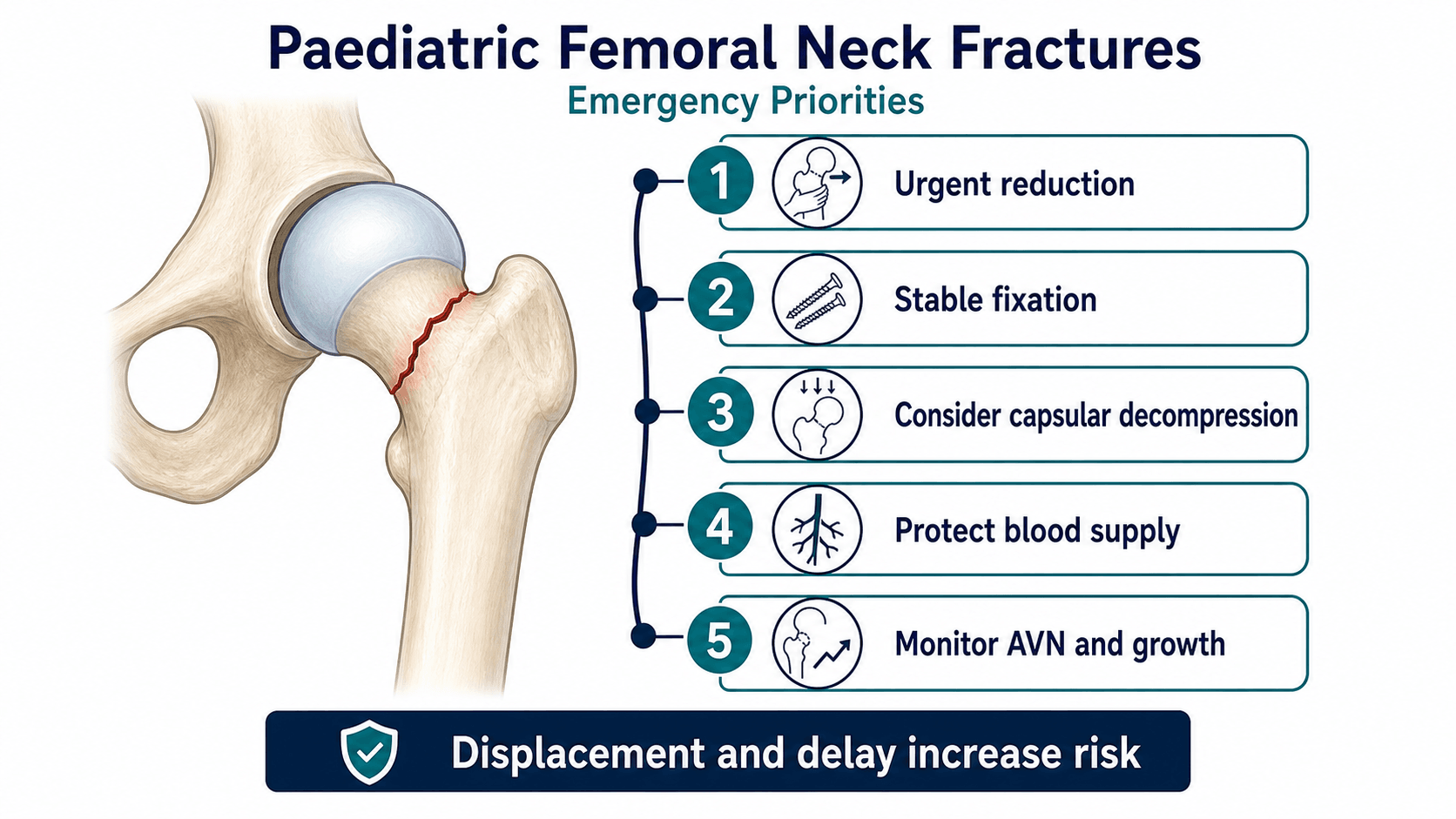
Rare injury, high complication burden, urgent anatomical reduction
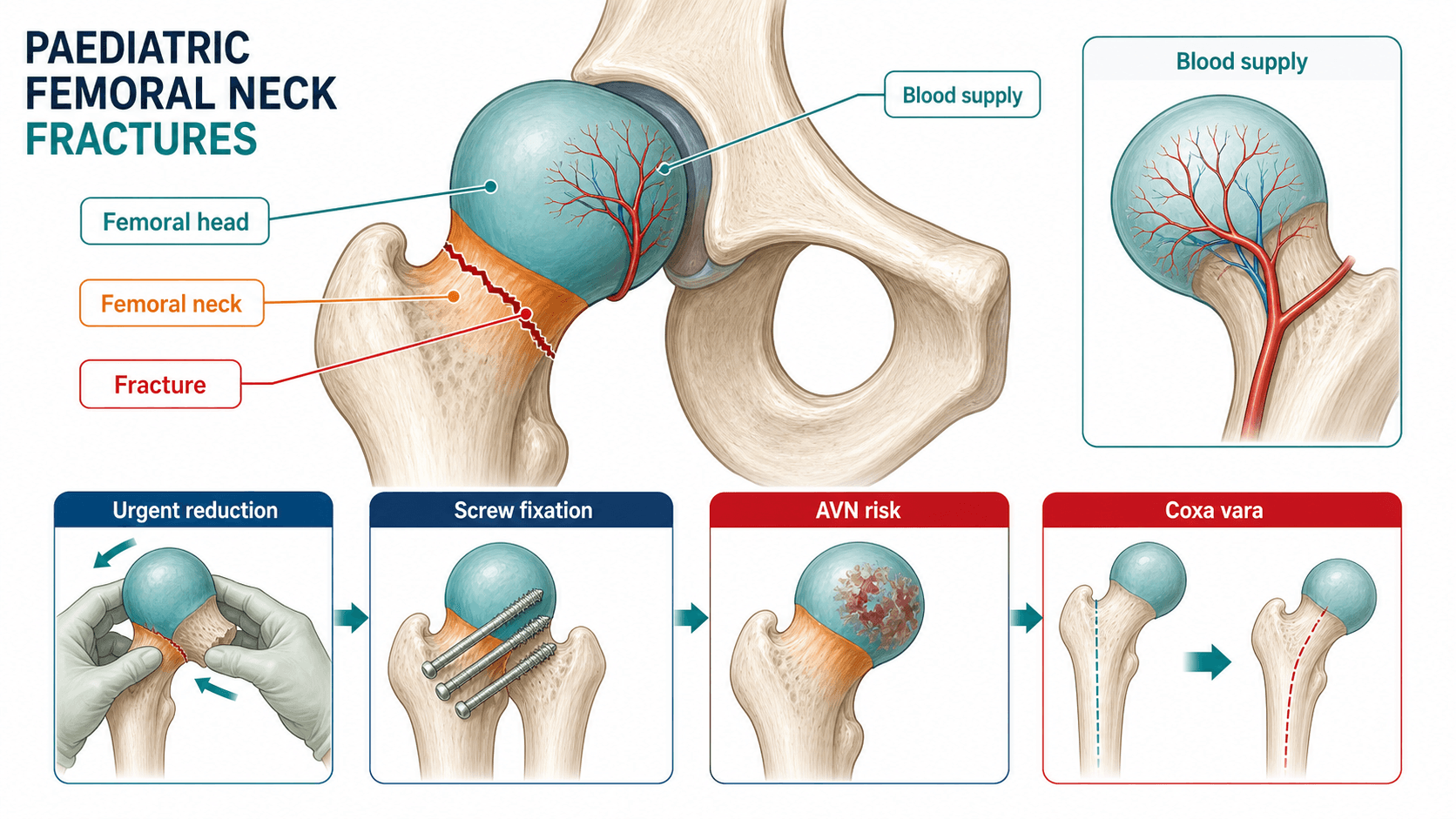
- Delbet type I transphyseal injuries have the greatest femoral-head perfusion concern.
- Displacement, intracapsular pressure, fracture location and reduction quality drive complication risk.
- A displaced intracapsular femoral neck fracture in a child needs urgent senior paediatric orthopaedic planning.
- Closed reduction is acceptable only if anatomical; open reduction is safer than accepting varus or rotational malreduction.
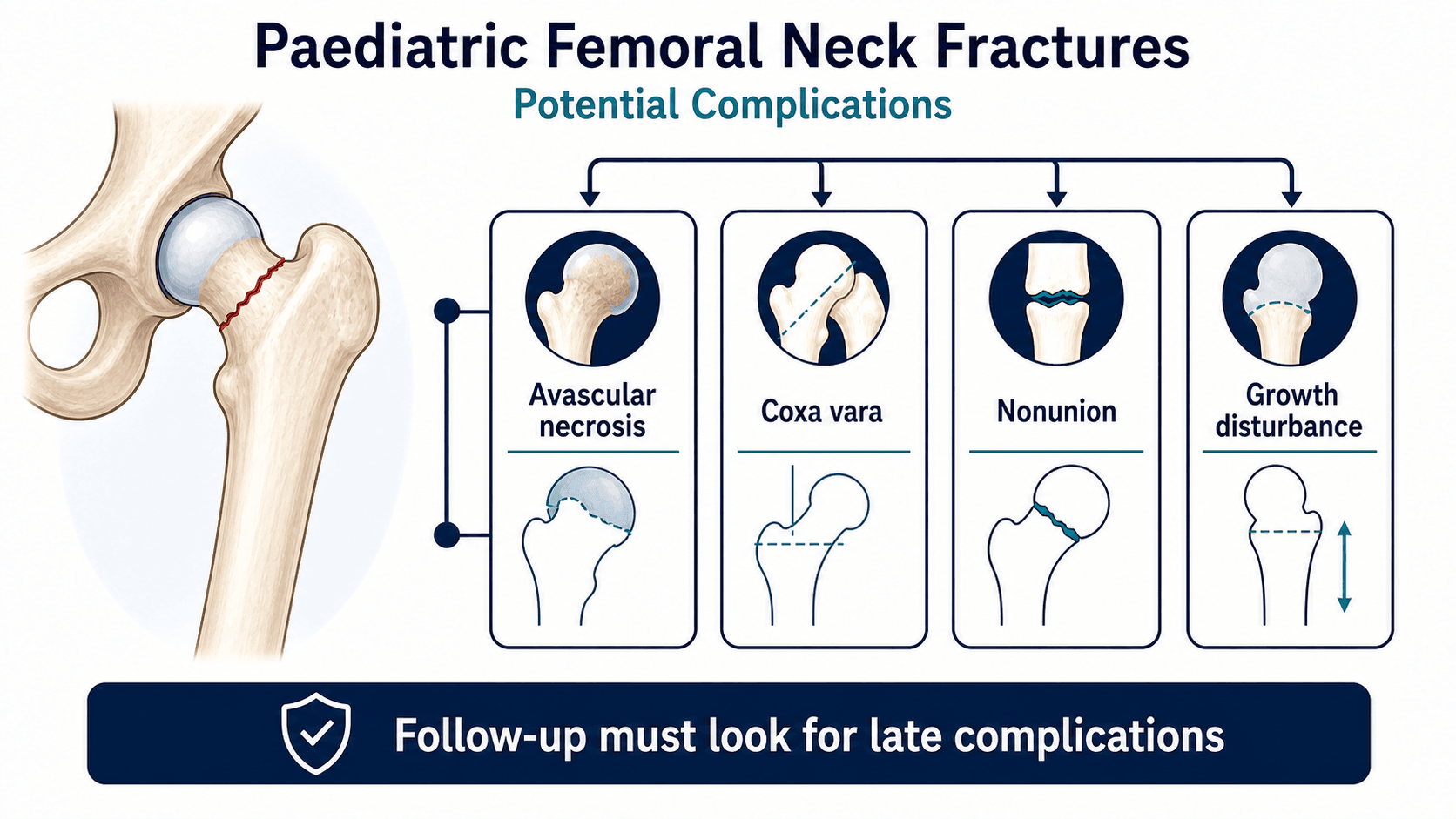
- Follow-up must continue after union because avascular necrosis and growth disturbance may declare late.
- “A painful log roll after high-energy trauma is enough to demand hip-specific imaging.
- “Do not force frog lateral positioning in a painful or unstable fracture; use a safe lateral view.
- “Implant choice matters, but the principles are more important: anatomical reduction, stable fixation and no joint penetration.
- “Coxa vara is often a sign of malreduction, fixation failure, non-union or growth disturbance rather than a minor radiographic detail.
Do not reassure the family simply because the fracture looks small. The femoral head may be threatened by vascular disruption, intracapsular pressure and growth-plate injury even when the initial radiograph does not look dramatic.
Images and Diagrams

- Answer
- A fracture through the paediatric proximal femur from physis to intertrochanteric region.
- Clinical use
- Classify by Delbet level and displacement.
- Answer
- The femoral-head blood supply and proximal femoral physis are vulnerable.
- Clinical use
- Counsel about AVN, growth disturbance and late deformity.
- Answer
- Urgent anatomical reduction and stable fixation when displaced or unstable.
- Clinical use
- Avoid varus, rotation, joint penetration and delay.
- Answer
- AVN, coxa vara, non-union, physeal arrest and limb-length difference.
- Clinical use
- Do not discharge after early union alone.
NECKCore Priorities
Hook:NECK keeps the management sequence simple: no delay, exact reduction, capsule pressure and keep watching.
DELBETClassification Logic
Hook:DELBET keeps classification tied to risk and treatment.
WATCHFollow-up Priorities
Hook:WATCH reminds the reader that union is not the endpoint.
Overview/Epidemiology
Paediatric femoral neck fractures are rare compared with adult hip fractures, but they are treated with a different level of urgency because the biology is different. The child has an open physis, a cartilage-rich proximal femur, a vulnerable femoral-head blood supply and many years of growth remaining. A well-aligned fracture can heal quickly; a poorly reduced or vascularly compromised fracture can leave the child with avascular necrosis, coxa vara, non-union, limb-length difference and early hip degeneration.
Most injuries follow high-energy trauma: road trauma, fall from height, sports collision or crush injury. A low-energy femoral neck fracture is not routine trauma until proven otherwise. It should trigger consideration of bone cyst, tumour-like lesion, metabolic bone disease, endocrine disease, infection, non-accidental injury in the right age group, or medication-related bone fragility.
The practical clinical sequence is:
- Identify the fracture and associated injuries.
- Classify with Delbet type and displacement.
- Decide whether the fracture is intracapsular and whether decompression is relevant.
- Restore an anatomical reduction.
- Stabilise the fracture without violating the joint.
- Protect weight bearing.
- Follow for union, femoral-head shape, neck-shaft angle and growth.
Pathophysiology
The proximal femur in a child is not a smaller adult hip. The proximal femoral physis contributes to growth, the greater trochanter has its own apophysis, and the femoral head relies heavily on vessels that run near the femoral neck.
- Clinical issue
- Articular segment at risk of avascular necrosis and collapse.
- Management implication
- Counsel early and follow long after fracture union.
- Clinical issue
- Displacement can directly injure femoral-head blood supply.
- Management implication
- Anatomical reduction and avoidance of repeated forceful manipulation matter.
- Clinical issue
- Delbet I and II injuries may raise pressure within the capsule.
- Management implication
- Capsular decompression should be considered in senior planning for displaced intracapsular fractures.
- Clinical issue
- Threatened in transphyseal injuries and by fixation choices.
- Management implication
- Balance physeal protection against the need for stable fixation.
- Clinical issue
- Vertical or varus fracture lines create shear and instability.
- Management implication
- Do not accept varus malreduction or inadequate fixation.
- Clinical issue
- Progressive varus reflects collapse, malunion, non-union or growth disturbance.
- Management implication
- Measure during follow-up rather than only checking union.
The reason this injury is treated urgently is not that children fail to unite. The reason is that the femoral head can lose perfusion, the neck can collapse into varus and the physis can arrest.
Classification
The Delbet classification describes fracture location. It is useful because location correlates with femoral-head perfusion risk and fixation strategy. It should always be paired with displacement, reduction quality, child age and associated injuries.
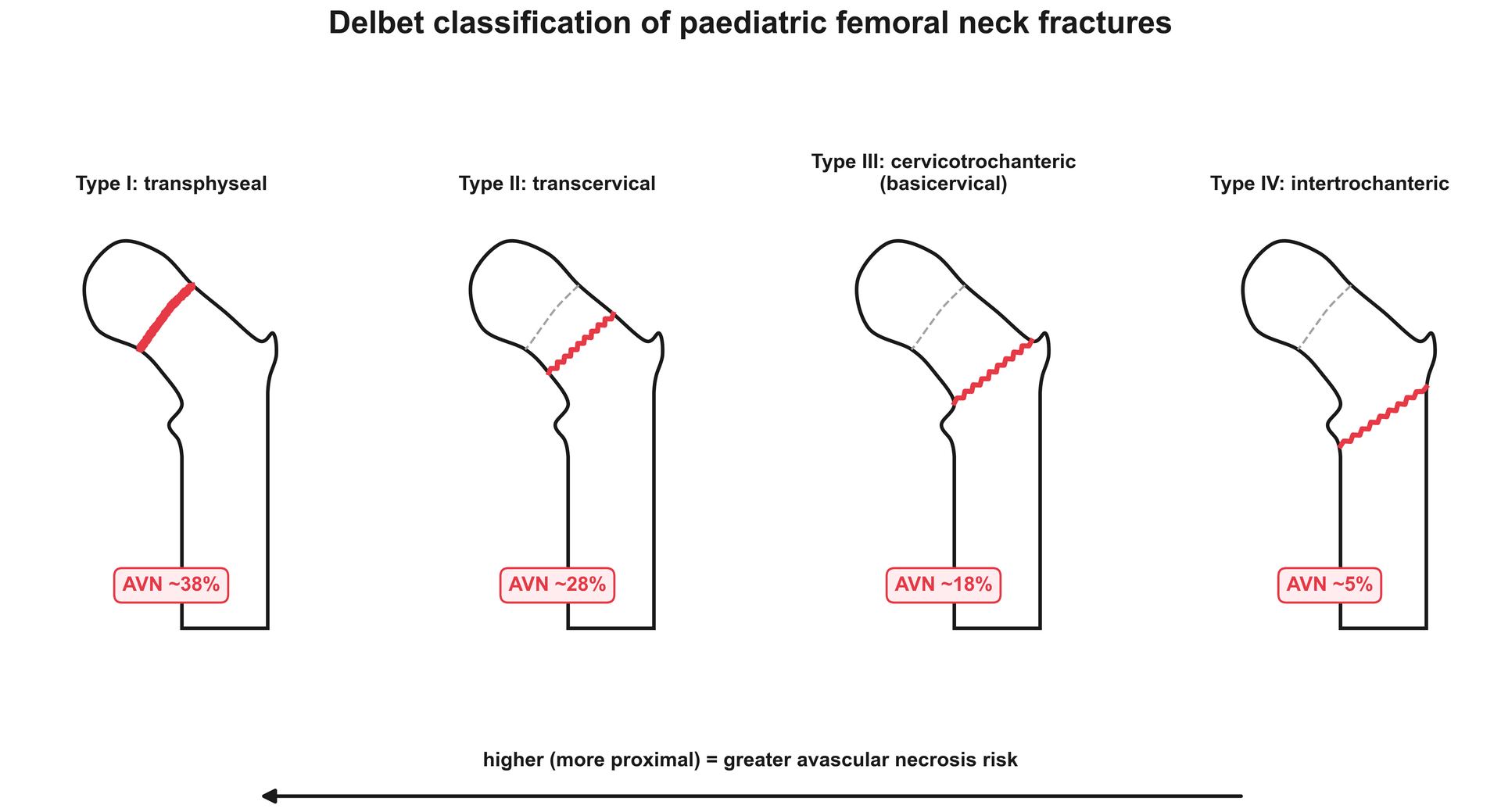
- Type I is transphyseal, through the proximal femoral physis. It may occur with traumatic hip dislocation. It has the greatest avascular necrosis concern because the injury is closest to the femoral head and physis.
- Type II is transcervical, through the femoral neck. It is the classic high-risk paediatric femoral neck fracture and is usually treated operatively when displaced.
- Type III is basicervical or cervicotrochanteric, at the base of the femoral neck. The AVN risk is lower than type I and II, but coxa vara and fixation stability remain major concerns.
- Type IV is intertrochanteric. It is extracapsular and has lower AVN risk than intracapsular patterns, but displacement, comminution and child size still matter.
- Fracture level
- Transphyseal
- Main concern
- Highest femoral-head perfusion and growth-plate concern
- Management implication
- Urgent senior care; reduction and stabilisation are time-sensitive.
- Fracture level
- Transcervical
- Main concern
- High AVN, non-union and displacement risk
- Management implication
- Anatomical reduction and stable fixation are central.
- Fracture level
- Basicervical
- Main concern
- Varus collapse and fixation failure
- Management implication
- Stability and neck-shaft angle monitoring matter.
- Fracture level
- Intertrochanteric
- Main concern
- Mechanical stability more than femoral-head perfusion
- Management implication
- Treat displacement and instability; AVN vigilance is still required.
Clinical Presentation
History
A typical child presents after high-energy trauma with severe hip or groin pain and inability to bear weight. Some children describe thigh or knee pain, so a hip injury can be missed if the assessment stops at the knee.
- Ask specifically
- Road trauma, fall height, sports collision, crush injury or direct lateral hip blow.
- Why it matters
- Most true paediatric femoral neck fractures are high-energy; low-energy injury needs pathology workup.
- Ask specifically
- Ability to stand, transfer or bear weight.
- Why it matters
- Inability to weight bear supports urgent hip imaging and protected handling.
- Ask specifically
- Groin, lateral hip, thigh or knee pain.
- Why it matters
- Hip fracture can present as knee pain.
- Ask specifically
- Previous limp, night pain, fever, weight loss or known bone lesion.
- Why it matters
- Suggests pathological fracture, tumour, infection or metabolic bone disease.
- Ask specifically
- Head, chest, abdomen, pelvis, femoral shaft, knee and neurological symptoms.
- Why it matters
- High-energy trauma can produce competing injuries and missed ipsilateral femoral shaft fracture.
- Ask specifically
- Timing of injury, transfer and any delay in presentation.
- Why it matters
- Frames urgency, counselling and complication risk discussion.
Examination
Examine the child using trauma principles before focusing on the hip. A displaced femoral neck fracture is painful; repeated log rolling or forced positioning is unnecessary.
- Assess
- Trauma survey, haemodynamics, head, chest, abdomen, pelvis and other limb injuries.
- Why it matters
- Do not let the hip fracture distract from polytrauma.
- Assess
- Shortening, external rotation, guarding and severe pain with gentle movement.
- Why it matters
- Supports displaced proximal femur injury and need for protected handling.
- Assess
- Groin tenderness, proximal femur tenderness and pain with gentle log roll.
- Why it matters
- Confirms hip source when pain is reported in thigh or knee.
- Assess
- Femoral shaft swelling, knee injury and distal femoral physeal tenderness.
- Why it matters
- Avoid missed associated shaft or distal injury.
- Assess
- Open injury, crush trauma or threatened skin.
- Why it matters
- Changes antibiotic, debridement and fixation timing.
- Assess
- Distal perfusion, motor function and sensation.
- Why it matters
- Documents baseline in high-energy trauma.
A child with a painful knee after trauma can still have a hip fracture. Hip examination and pelvis imaging are essential when the mechanism is high energy or weight bearing is impossible.
Investigations
Initial imaging
Obtain an AP pelvis and a safe lateral view of the injured hip. In a painful fracture, do not force frog lateral positioning. A cross-table lateral or other safe lateral projection is preferable. The AP pelvis gives the contralateral hip for comparison and helps identify associated pelvic injury.
Image the whole femur when the mechanism is high energy, when thigh pain is present or when ipsilateral shaft fracture is possible. A femoral shaft fracture can distract attention from a proximal femoral injury, and the reverse is also true.
When CT helps
CT is useful when fracture anatomy is unclear, when reduction planning is difficult, when displacement is subtle, or when an associated pelvic or acetabular injury is suspected. CT should answer a management question; it should not delay urgent treatment of an obvious displaced fracture.
When MRI or laboratory work helps
MRI, blood tests and broader workup are considered when the mechanism is low energy, when there was preceding pain, when X-ray shows a lesion, or when infection or tumour is possible. MRI can also help later if avascular necrosis is suspected before radiographic collapse is obvious.
- Investigation
- AP pelvis and safe lateral hip view
- What it changes
- Confirms Delbet level and displacement.
- Investigation
- Whole femur, pelvis and trauma imaging as indicated
- What it changes
- Prevents missed shaft, pelvic, abdominal or head injury.
- Investigation
- CT when it will change planning
- What it changes
- Improves reduction and fixation planning.
- Investigation
- MRI, labs and lesion workup
- What it changes
- Changes biopsy caution and definitive management.
- Investigation
- Serial X-rays, MRI if concern persists
- What it changes
- Detects late perfusion and shape complications.
Differential Diagnosis
A child with a painful, non-weight-bearing hip after trauma is not always a femoral neck fracture. The differential matters because each alternative has a different urgency, imaging pathway and pitfall. The dangerous traps are the slipped capital femoral epiphysis (SCFE) mislabelled as a transphyseal fracture, and the low-energy "fracture" that is really a pathological lesion.
- Discriminating features
- Fracture follows clear high-energy trauma; SCFE is usually atraumatic or trivial trauma in an older, often overweight or endocrine-predisposed child with chronic groin or knee pain.
- Key pitfall
- Forcing reduction of an unrecognised acute-on-chronic SCFE as if it were a fracture can precipitate osteonecrosis.
- Discriminating features
- Low-energy mechanism, preceding limp or night pain, lytic or expansile lesion (unicameral bone cyst, aneurysmal bone cyst, non-ossifying fibroma, fibrous dysplasia) or permeative malignant pattern.
- Key pitfall
- Stabilising or biopsying through the wrong approach before staging a possible malignancy.
- Discriminating features
- Fever, raised inflammatory markers, refusal to weight bear without clear trauma; effusion on ultrasound.
- Key pitfall
- Attributing an irritable hip to minor trauma and missing joint sepsis.
- Discriminating features
- Fixed deformity, empty acetabulum on radiograph; may coexist with a Delbet I injury.
- Key pitfall
- Missing an associated transphyseal fracture during or after relocation.
- Discriminating features
- Localised lateral tenderness, intact neck-shaft architecture, avulsed apophysis.
- Key pitfall
- Over-treating a benign avulsion as an unstable neck fracture.
- Discriminating features
- Mechanism inconsistent with injury, age under walking, delayed presentation, other injuries of differing ages.
- Key pitfall
- Failing to safeguard while focusing only on the fracture.
Both cross the proximal femoral physis. The history (clear high-energy trauma versus atraumatic chronic symptoms), the child's age and habitus, and the contralateral hip usually separate them. Treating an acute slip with forceful reduction is a recognised route to osteonecrosis.
Management
- Practical action
- Analgesia, trauma assessment, non-weight bearing and safe positioning.
- Avoid
- Repeated painful examination or forced frog lateral positioning.
- Practical action
- AP pelvis, safe lateral hip, whole femur when needed and Delbet/displacement classification.
- Avoid
- Calling it simply a hip fracture without defining the risk.
- Practical action
- Urgent anatomical reduction; open reduction if closed reduction is not anatomical.
- Avoid
- Accepting varus, rotation or translation to avoid an incision.
- Practical action
- Use fixation that holds reduction and avoids joint penetration.
- Avoid
- Prioritising physeal avoidance over stability in a dangerous unstable fracture.
- Practical action
- Consider aspiration, capsulotomy or decompression in displaced intracapsular injuries.
- Avoid
- Ignoring a tense intracapsular haematoma in senior planning.
- Practical action
- Protected weight bearing, serial imaging and long-term AVN/growth follow-up.
- Avoid
- Discharging after early union.
The first step is analgesia, trauma assessment and immobilisation. Keep the child non-weight bearing. Involve senior paediatric orthopaedics early, especially if the fracture is displaced, intracapsular, transphyseal, pathological or part of polytrauma.
- Resuscitate and assess associated injuries.
- Provide adequate analgesia and avoid repeated painful manipulation.
- Keep the limb protected and non-weight bearing.
- Obtain appropriate imaging without unsafe positioning.
- Classify Delbet type and displacement.
- Plan urgent reduction and fixation for displaced or unstable fractures.
If the choice is between a neat closed reduction that is not anatomical and an open reduction that is anatomical, the safer orthopaedic answer is to restore anatomy.
Specific Scenarios
- Confirm the fracture with high-quality AP and lateral imaging.
- Treat as high risk even when displacement is absent.
- Many paediatric femoral neck fractures still undergo fixation because secondary displacement is dangerous.
- Protect weight bearing and monitor closely if a non-operative pathway is chosen for a very selected stable pattern.
- Counsel about AVN and late deformity.
Complications and Follow-up
- What it looks like
- Pain, stiffness, sclerosis, fragmentation, collapse or loss of femoral-head sphericity.
- Why it matters
- Can declare late and may occur despite fracture union.
- What it looks like
- Falling neck-shaft angle from malreduction, fixation failure, non-union, physeal injury or collapse.
- Why it matters
- Shortens the limb, weakens abductors and may need osteotomy.
- What it looks like
- Persistent fracture line, pain, implant failure or varus progression.
- Why it matters
- Often reflects shear, poor reduction, unstable fixation or biological compromise.
- What it looks like
- Varus, rotation or translation after healing.
- Why it matters
- Produces limp, pain and abductor dysfunction.
- What it looks like
- Premature closure, proximal femoral growth disturbance or limb-length difference.
- Why it matters
- Growth consequences may outlast fracture healing.
- What it looks like
- Collapse, incongruity and altered proximal femoral mechanics.
- Why it matters
- Explains why surveillance often extends beyond union.
When avascular necrosis does occur, grade it with the Ratliff classification, which describes the pattern and predicts prognosis: Type I - total head involvement (the whole capital epiphysis is avascular; the commonest and worst pattern, typically from a Delbet I/II injury disrupting the lateral epiphyseal vessels); Type II - partial or localised segmental involvement of part of the head; and Type III - an area limited to the femoral neck between the fracture line and the physis, sparing the epiphysis (the best prognosis). Ratliff type correlates with the long-term Harris hip score and osteoarthritis risk, so naming it guides counselling and the aggressiveness of intervention (containment, osteotomy or salvage). Quote it alongside the Delbet-type-specific AVN incidence (roughly 38/28/18/5% for Delbet I-IV).
A specific growth sequela the examiner expects is relative (greater) trochanteric overgrowth. If the proximal femoral capital physis arrests (from the injury, from fixation crossing it, or after AVN) while the greater trochanteric apophysis keeps growing, the trochanter ends up relatively high - shortening the abductor lever arm and the femoral neck (coxa breva) and producing abductor weakness and a Trendelenburg gait even when the neck-shaft angle is acceptable. It is distinct from coxa vara (a true reduction in the neck-shaft angle), though the two often coexist. Recognition matters because management differs: a young child with remaining growth can be treated with greater trochanteric epiphysiodesis to let the head and neck "catch up", whereas an established deformity in the older child needs trochanteric transfer (distal-lateral advancement) to restore the abductor moment arm. So in follow-up, measure the articulotrochanteric distance, not just the neck-shaft angle.
Decision-Making in Practice
Paediatric femoral neck fracture is an emergency because the femoral head blood supply is vulnerable and complications are common. The treatment plan should be built around timing, displacement, Delbet type, reduction quality, fixation stability, capsular pressure and long-term surveillance for avascular necrosis.
- Assess
- Displacement, pain, transfer time and theatre access
- Management consequence
- Early reduction and stable fixation are prioritised
- Assess
- Delbet I to IV, Pauwels angle and comminution
- Management consequence
- Transphyseal and transcervical injuries have high complication concern
- Assess
- Anatomic alignment on AP and lateral imaging
- Management consequence
- Poor reduction increases AVN, nonunion and coxa vara risk
- Assess
- Age, size, physis, fracture line and stability
- Management consequence
- Screws, pins or plate constructs are selected to hold reduction safely
- Assess
- AVN, coxa vara, nonunion, premature physeal closure and leg length
- Management consequence
- Long surveillance is mandatory
- Practical position
- Rare; only selected nondisplaced stable injuries with specialist oversight.
- Reason
- Secondary displacement is dangerous and follow-up must be reliable.
- Practical position
- Use when closed reduction is not anatomical.
- Reason
- An incision is preferable to residual varus, rotation or translation.
- Practical position
- Discuss explicitly for displaced intracapsular injuries.
- Reason
- Evidence is debated, but pressure and vascular concerns are clinically important.
- Practical position
- Protect fixation until union, then restore motion and gait.
- Reason
- Fixation failure, coxa vara and stiffness are preventable follow-up targets.
- Practical position
- Warn family that AVN and growth disturbance may declare late.
- Reason
- Normal early radiographs do not end care.
Clinical Reasoning Notes
- Say clearly
- This is a paediatric femoral neck fracture, not an adult hip fracture.
- Why it matters
- Signals different vascular, growth and fixation risks.
- Say clearly
- Delbet type plus displacement, verticality and associated injuries.
- Why it matters
- Delbet type alone is incomplete.
- Say clearly
- Displaced intracapsular patterns are urgent because of femoral-head perfusion risk.
- Why it matters
- Prevents routine-list thinking.
- Say clearly
- Anatomical reduction, stable fixation, capsule pressure management where indicated and long surveillance.
- Why it matters
- Keeps decision-making focused on avoidable complications.
- Say clearly
- Age, skeletal maturity, polytrauma, low-energy mechanism, associated shaft/pelvic injury and closed-reduction quality.
- Why it matters
- Explains why the same Delbet type may need different treatment.
Common pitfalls
- Treating the injury like an adult neck-of-femur fracture.
- Saying "hip fracture" without naming Delbet type.
- Forgetting to ask why a low-energy fracture happened.
- Accepting varus reduction.
- Avoiding open reduction when closed reduction is poor.
- Focusing on implant type but not reduction quality.
- Missing joint penetration on postoperative imaging.
- Stopping follow-up once the fracture unites.
Counselling points
Families need a clear explanation that this is rare and serious. The fracture can heal but still develop late femoral-head or growth problems. They should understand the need for repeat imaging, protected weight bearing, monitoring for pain or stiffness, and longer follow-up than many other childhood fractures.
Guidelines, Registries and Global Practice
There is no single randomised trial or dedicated international guideline for this rare injury; practice is built from cohort series, two meta-analyses and society fracture-management principles. The picture below is a global synthesis rather than any one country's protocol.
Global epidemiology
- Paediatric femoral neck fractures represent less than 1 percent of all paediatric fractures and roughly 1 percent of hip fractures across age groups.
- Bimodal mechanism: high-energy trauma (road traffic, falls from height) in most series, with a smaller pathological-fracture group.
- Delbet type II (transcervical) is the most common pattern; type I (transphyseal) is the rarest but carries the highest osteonecrosis risk.
- Pooled osteonecrosis rates by Delbet class are approximately 38, 28, 18 and 5 percent for types I to IV respectively (Moon and Mehlman), with contemporary cohorts reporting overall AVN around 23 to 29 percent.
- Emphasis
- Anatomical reduction and stable internal fixation; spica supplementation in young children; implant sized to the child.
- Practical takeaway
- Stability plus anatomy is the universal core principle.
- Emphasis
- Urgent treatment of displaced fractures, consideration of capsular decompression, and prolonged AVN surveillance.
- Practical takeaway
- Treat displaced intracapsular injuries as emergencies and watch the head long term.
- Emphasis
- Senior decision-making, network transfer to a paediatric orthopaedic centre, and clear complication counselling.
- Practical takeaway
- Escalate early; these are not routine list cases.
- Emphasis
- Reduction quality as the dominant modifiable factor; honest acknowledgement that timing and decompression evidence is weak.
- Practical takeaway
- Frame timing and decompression as rational but unproven.
Registry and high- versus limited-resource practice
- Unlike adult hip fractures, this injury is too rare for dedicated arthroplasty-style registries; evidence comes from single-centre cohorts and the pooled meta-analyses above. National paediatric trauma networks (rather than implant registries) are the practical data source.
- High-resource settings: rapid imaging, sub-specialist paediatric orthopaedic cover, image-intensifier-guided reduction and fixation, and structured multi-year AVN surveillance.
- Limited-resource settings: delayed presentation is common and a recognised cause of established non-union and coxa vara in toddlers; valgus osteotomy with minimal fixation is a described salvage where early anatomical fixation was not feasible.
- Regardless of setting, the modifiable lever is the same — achieve and hold an anatomical reduction and follow the head for years.
Controversies and Areas of Uncertainty
Much of this topic is taught as if it were settled. It is not. A consultant-level answer names where the evidence is genuinely conflicting and then states a defensible position.
- The two positions
- Some series suggest earlier reduction protects the head; pooled meta-analysis (AlKhatib) found no significant timing effect, and Spence found a timing signal that was confounded by injury severity.
- Defensible practical stance
- Treat displaced Delbet I or II fractures expediently as best practice, but do not promise the family that an overnight operation prevents AVN.
- The two positions
- Open reduction allows anatomical reduction under vision; closed reduction avoids further surgical insult and was associated with lower AVN in long-term subgroups (Dong 2025).
- Defensible practical stance
- Aim for a closed anatomical reduction; convert to open only when closed reduction is not anatomical. Quality of reduction beats route.
- The two positions
- Biologically attractive (relieves tamponade on retinacular vessels); but Spence found decompression was not an independent predictor of AVN.
- Defensible practical stance
- Discuss explicitly for displaced intracapsular injuries; it is low-morbidity and biologically rational even though high-level proof is lacking.
- The two positions
- Avoiding the physis protects growth; crossing it may be unavoidable for stability in proximal Delbet I or II fractures.
- Defensible practical stance
- Accept controlled physeal crossing when stability demands it, then counsel about and monitor for growth arrest.
- The two positions
- Cannulated screws, paediatric hip screw or plate constructs each have advocates; no implant has been shown to change AVN or coxa vara rates.
- Defensible practical stance
- Choose by child size, fracture level and stability, not dogma; stability and reduction matter more than the device.
The strongest single message from the modern evidence is that reduction quality is the dominant surgeon-controlled determinant of outcome. Time, route and implant are secondary and contested.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child presents after a fall from height with a displaced transcervical femoral neck fracture. How do you manage it?”
“A child sustains a femoral neck fracture after a minor fall from standing height. What changes in your assessment?”
“The parents of a child with a displaced Delbet type II fracture ask whether operating tonight and decompressing the joint will save the femoral head. What do you tell them, and what does the evidence show?”
Classify
- Delbet I: transphyseal
- Delbet II: transcervical
- Delbet III: basicervical
- Delbet IV: intertrochanteric
- Always add displacement
Treat
- Trauma assessment
- Urgent senior review
- Anatomical reduction
- Stable fixation
- Consider decompression
Avoid
- Delay
- Varus reduction
- Joint penetration
- Missed shaft fracture
- Early discharge from surveillance
Follow
- Union
- AVN
- Coxa vara
- Non-union
- Physeal arrest and LLD
Evidence Signals
Moon and Mehlman: the landmark AVN meta-analysis defining Delbet risk
- Pooled 360 paediatric femoral neck fractures (25 Cincinnati cases plus 20 literature reports with patient-level data).
- Osteonecrosis rate fell stepwise by Delbet class: type I 38 percent, type II 28 percent, type III 18 percent, type IV 5 percent.
- On logistic regression, fracture type and age were the only independent predictors; type I, II and III were 15, 6 and 4 times more likely to develop AVN than type IV.
Early versus late treatment: time-to-surgery did not independently change AVN
- Six comparative studies, 231 paediatric femoral neck fractures.
- No statistically significant difference in osteonecrosis between treatment under 24 hours versus over 24 hours (OR 1.19, 95 percent CI 0.56 to 2.51), nor between open and closed reduction (OR 1.62, 95 percent CI 0.82 to 3.22).
- Displaced fractures (OR 3.81) and Delbet type I or II fractures (OR 2.43) carried significantly higher AVN risk.
Contemporary risk-factor meta-analysis: what predicts AVN in 1332 children
- Thirty-four studies, 1332 patients (1340 fractures) — the largest pooled paediatric dataset to date.
- Significant AVN predictors: age 12 years or older (RR 1.40), Delbet type I or II (RR 1.96), initial displacement (RR 2.98) and poor reduction quality (RR 2.43).
- In long-term (5 year or more) subgroups, delayed reduction increased AVN (RR 2.63) and closed reduction and internal fixation reduced AVN versus open reduction (RR 0.40).
Anatomical reduction outweighs every other variable for long-term outcome
- 26 surgically treated Delbet type II and III fractures followed into adulthood (mean 157 months).
- AVN occurred in 23 percent and correlated with non-anatomic reduction, poor early Ratliff grade, lower adult Harris hip score and later osteoarthritis.
- Non-anatomic reduction correlated with all three principal complications; coxa breva and limb-length discrepancy did not predict poor clinical outcome.
Evidence Base
Single-centre risk-factor analysis: displacement and location, not decompression, predicted AVN
- 70 patients followed to union; osteonecrosis occurred in 20 (29 percent), median time to diagnosis 7.8 months.
- Fracture displacement and fracture location were the independent multivariable predictors of osteonecrosis.
- Age, fixation type, mechanism, postoperative alignment, performance of reduction and capsular decompression were NOT predictive.
Comprehensive review of proximal femoral fractures in childhood
- Delbet classification both guides management and provides prognostic clues.
- Universal agreement that anatomic reduction and stable internal fixation, supplemented by spica in younger children, are essential for good outcomes.
- The role of capsular decompression, implant choice and configuration, and surgical timing remain genuinely debated.
Paediatric femoral neck fracture overview
- Confirms the Delbet system as the standard classification and its prognostic use.
- Lists osteonecrosis, non-union, coxa vara and premature physeal closure as the key complications to monitor.
- Reinforces radiographic and functional follow-up beyond union.