Electrochemical Degradation | Metal Ion Release | ALVAL | Implant Failure
- Corrosion is electrochemical degradation of metal in physiological environment
- Passivation layer (TiO2, Cr2O3) protects implants - breakdown causes corrosion
- MACC (mechanically-assisted crevice corrosion) is key mechanism at modular junctions
- ALVAL (aseptic lymphocyte-dominated vasculitis-associated lesion) from metal hypersensitivity
- MoM hip failures primarily from taper corrosion, not bearing surface wear
- “Body fluid is corrosive: 0.9% NaCl, pH 7.4, 37°C, proteins
- “Mixed metal couples (CoCr/Ti) have higher galvanic corrosion than matched materials
- “Serum metal ions: Cobalt and chromium levels monitor MoM hips
- “Taper assembly: clean, dry, single impaction reduces fretting corrosion
Oxidation-reduction reaction. Metal loses electrons (oxidation: M → M+ + e-) at anode. Electrons flow to cathode where reduction occurs (O2 + 2H2O + 4e- → 4OH-). Passivation layer prevents this.
Mechanically-Assisted Crevice Corrosion is primary failure mode in modular hip implants. Micro-motion disrupts passivation + crevice environment creates low pH = accelerated corrosion.
Type IV delayed hypersensitivity to metal ions. Aseptic lymphocyte-dominated vasculitis causes soft tissue destruction (pseudotumor). Cobalt and chromium ions from corrosion products.
Avoid mixed metals (match CoCr with CoCr), proper taper assembly (clean/dry/single impaction), use highly polished surfaces, consider ceramic heads to eliminate taper corrosion.
Overview and Electrochemistry
Corrosion is the electrochemical degradation of metallic materials in their environment. In orthopaedic implants, this occurs when metals are exposed to the aggressive physiological environment: aqueous solution with chloride ions (0.9% NaCl), pH 7.4, temperature 37°C, and organic molecules.
The body is a hostile environment for metals:
- Chloride ions (aggressive anions) attack passivation layers
- Proteins and amino acids affect electrochemical reactions
- Cyclic mechanical loading creates stress and micro-motion
- Oxygen gradients develop in crevices and gaps
Understanding corrosion mechanisms is essential because metal ion release can cause:
- Implant mechanical failure - material loss weakens structure
- Metal hypersensitivity - Type IV delayed hypersensitivity (ALVAL)
- Local tissue toxicity - soft tissue necrosis and pseudotumor
- Systemic metal elevation - unclear long-term effects
Electrochemical Principles
Metal loses electrons and goes into solution as ions:
M → M^n+ + ne^-
This is the corrosion reaction. Metal atoms become ions in solution (metal ion release).
Electrons are consumed in reduction reaction:
O2 + 2H2O + 4e^- → 4OH^-
Oxygen is reduced to hydroxyl ions. This completes the electrochemical circuit.
Passivation: The Key Defense
All orthopaedic metals (titanium, stainless steel, cobalt-chromium) rely on a thin oxide layer for corrosion resistance:
- Titanium: Forms TiO2 layer (very stable, rapid self-healing)
- Stainless steel: Forms Cr2O3 layer (chromium oxide)
- Cobalt-chromium: Forms Cr2O3 layer (chromium oxide)
This passivation layer is typically 2-10 nm thick and prevents metal from contacting the corrosive environment. Corrosion occurs when passivation is disrupted.
Titanium forms a tenacious TiO2 passivation layer that is extremely stable and self-healing - if scratched, it reforms in milliseconds in the presence of oxygen. This makes titanium highly corrosion-resistant despite being a reactive metal thermodynamically. CoCr relies on Cr2O3 which is less robust.
The Polarisation Curve and the Breakdown Potential
Every section of this topic returns to one idea - corrosion occurs when passivation is disrupted. The electrochemistry that decides whether the passive film holds is the anodic polarisation curve, which plots corrosion current against electrode potential:
- Active region: at low potential the bare metal dissolves freely (high current).
- Passive region: as potential rises a protective oxide film forms and the current drops to a very low, near-constant value - the metal is protected across a wide "passive window".
- Breakdown (pitting) potential: above a critical potential the passive film breaks down locally and the current rises sharply again - this is where pitting and crevice corrosion initiate.
- Transpassive region: at very high potential the oxide itself dissolves and general corrosion resumes.
The wider the passive window and the higher the breakdown potential, the more corrosion-resistant the alloy - which is why titanium (very high, self-healing breakdown potential) outperforms stainless steel, whose lower breakdown potential makes it the most pitting-prone of the implant alloys.
Two modifiers the body imposes:
- Chloride ions lower the breakdown potential - they adsorb at film defects and prevent re-passivation, so the safe passive window narrows in physiological saline.
- Galvanic area effect: when dissimilar metals are coupled, a large cathode driving a small anode concentrates the entire galvanic current onto a tiny area, so a small exposed region (for example a small de-passivated patch within a taper crevice) corrodes very rapidly. A small-anode with large-cathode geometry is the worst case.
An alloy is protected only while its working potential stays within the passive window, below the breakdown (pitting) potential. Titanium has a very high, self-healing breakdown potential; stainless steel's is the lowest, so it pits most readily. Chloride lowers the breakdown potential, and an unfavourable large-cathode with small-anode area ratio concentrates corrosion - together these explain why localised breakdown happens in crevices and at mixed-metal couples.
Principles and Mechanisms of Corrosion
Galvanic Corrosion
Galvanic Corrosion Mechanism
Occurs when two dissimilar metals are in electrical contact in an electrolyte. The less noble (more anodic) metal corrodes preferentially.
Galvanic series in physiological saline (most noble to least noble):
- Platinum (most noble - least corrodes)
- Cobalt-chromium alloys
- Titanium alloys
- Stainless steel 316L
- Magnesium (least noble - most corrodes)
- Anode (Corrodes)
- Titanium stem
- Cathode (Protected)
- CoCr head
- Clinical Example
- Modular hip taper junction
- Anode (Corrodes)
- Stainless steel
- Cathode (Protected)
- CoCr
- Clinical Example
- Mixed implants (rare)
- Anode (Corrodes)
- Neither (matched)
- Cathode (Protected)
- Neither (matched)
- Clinical Example
- Preferred combination
Key principle: The larger the potential difference between metals (farther apart in galvanic series), the greater the corrosion rate of the anodic metal.
This principle explains why galvanic corrosion occurs at modular taper junctions in hip implants.
Crevice Corrosion
Definition: Localized corrosion within shielded areas (crevices, gaps) where oxygen is depleted.
Crevice Corrosion Development
Crevice exists between surfaces (modular taper, plate-bone interface). Initially passive.
Oxygen consumed in crevice faster than it can diffuse in. Oxygen gradient develops - low inside crevice.
Metal oxidation continues: M → M^n+ + ne^-. Hydrolysis: M^n+ + H2O → MOH + H^+. Produces H^+ ions. pH drops to 3-4 in crevice.
Low pH dissolves protective oxide layer. Chloride ions migrate into crevice (charge balance). Acidic chloride environment is highly aggressive.
Corrosion accelerates and becomes self-sustaining. Metal ion release increases. Crevice pH stays low (autocatalytic).
Clinical sites of crevice corrosion:
- Modular taper junctions (head-neck, neck-stem)
- Screw-plate interfaces
- Plate-bone interfaces
- Modular knee tibial tray interfaces
MACC: Mechanically-Assisted Crevice Corrosion
When micro-motion is superimposed on crevice corrosion, the result is MACC:
- Micro-motion continuously disrupts passivation layer
- Fresh metal exposed to aggressive crevice environment
- Mechanical wear debris plus corrosion products
- Synergistic effect: corrosion rate much higher than either alone
MACC is the primary mechanism of modular taper corrosion in hip implants.
MACC is the leading cause of modular hip taper failures. Risk factors: large femoral heads (higher torque), offset head position (increased moment arm), patient factors (high BMI, activity). Prevention: proper assembly technique, avoid mixed metals, consider ceramic heads.
Pitting Corrosion
Highly localized breakdown of passivation creating small pits that propagate deep into metal.
- Passivation layer has microscopic defect (inclusion, scratch)
- Chloride ions adsorb at defect site
- Local passivation breakdown creates micro-anode
- Pit propagates inward (autocatalytic like crevice)
- Small surface opening, deep penetration
- Can act as stress concentration site for fatigue crack initiation
Cl^- is small anion that penetrates oxide layer and prevents re-passivation.
- Less common than fretting/crevice in orthopaedics
- Can occur on stainless steel more than Ti or CoCr
- Pits act as stress risers → fatigue crack initiation
- Surface finishing reduces susceptibility
Fretting Corrosion
Combined mechanical wear and corrosion from small amplitude oscillatory motion between surfaces.
- Micro-motion between surfaces (typically less than 100 microns)
- Passivation layer abraded away mechanically
- Fresh metal exposed to corrosive environment
- Oxidizes rapidly, forms debris
- Debris trapped between surfaces (third-body wear)
- Cycle repeats - synergistic mechanical + chemical degradation
- Pure Wear
- Mechanical removal
- Pure Corrosion
- Chemical dissolution
- Fretting Corrosion
- Synergistic mech + chem
- Pure Wear
- Yes (sliding)
- Pure Corrosion
- No
- Fretting Corrosion
- Yes (micro-motion)
- Pure Wear
- Not relevant
- Pure Corrosion
- Critical
- Fretting Corrosion
- Repeatedly disrupted
- Pure Wear
- Metallic particles
- Pure Corrosion
- Oxide/ions
- Fretting Corrosion
- Oxide particles + ions
- Pure Wear
- Linear with cycles
- Pure Corrosion
- Time-dependent
- Fretting Corrosion
- Accelerated (synergy)
- Modular tapers: Fretting corrosion is dominant wear mode
- Polyethylene backside: Fretting between poly and tibial tray
- Screw-plate interfaces: Micro-motion causes fretting
- Cerclage wires: Fretting against bone or plate
Black debris (metal oxide particles) characteristic of fretting corrosion.
This completes the description of fretting mechanisms in orthopaedic implants.
Environmentally-Assisted Cracking: Stress Corrosion Cracking and Corrosion Fatigue
The four types above describe metal loss; a further category describes cracking that occurs when mechanical stress and the corrosive environment act together. These environmentally-assisted cracking mechanisms cause sudden, often brittle, implant fracture rather than gradual material loss.
- Stress corrosion cracking (SCC)
- Sustained (static) tensile stress
- Corrosion fatigue
- Cyclic (fluctuating) stress
- Stress corrosion cracking (SCC)
- Corrosive medium plus stress crack the passive film at a susceptible site
- Corrosion fatigue
- Corrosion removes the fatigue limit - cracks initiate at lower stress and earlier
- Stress corrosion cracking (SCC)
- Branching brittle crack (inter- or transgranular)
- Corrosion fatigue
- Transgranular fatigue crack, often pit-initiated
- Stress corrosion cracking (SCC)
- Historical stainless-steel implant fractures in the chloride environment
- Corrosion fatigue
- Stem/plate fatigue failure accelerated by pitting or crevice attack
Key points:
- Stress corrosion cracking requires three things together: a susceptible alloy, a specific corrosive environment (chloride), and a sustained tensile stress. The crack tip is both mechanically and chemically driven, so failure can occur well below the normal yield strength.
- Corrosion fatigue is the synergy of cyclic loading and corrosion: in a corrosive medium a metal loses its true fatigue (endurance) limit, so the S-N curve keeps falling and the implant can fail at a stress that would be safe in air. A corrosion pit or a fretting scar acts as the stress raiser that initiates the fatigue crack. (The pure mechanical S-N behaviour and fatigue limit are developed in the dedicated fatigue-failure topic.)
Pitting and fretting do not only release metal ions - each pit or fretting scar is a stress concentrator. Under cyclic load in the chloride-rich body environment that defect initiates a corrosion-fatigue crack, and the metal behaves as if it has no fatigue limit. This is the mechanistic link between localised corrosion and the rare but catastrophic complication of implant (stem, plate or modular-neck) fracture.
Metal Ion Release and Biological Effects
Metal Ion Release Mechanisms
When corrosion occurs, metal ions are released into surrounding tissues and systemic circulation.
- Normal Serum Level
- Less than 1 ppb
- Threshold for Concern
- Greater than 5 ppb
- Source of Elevation
- CoCr implant corrosion, MoM bearing
- Normal Serum Level
- Less than 1 ppb
- Threshold for Concern
- Greater than 5 ppb
- Source of Elevation
- CoCr implant corrosion
- Normal Serum Level
- Less than 5 ppb
- Threshold for Concern
- No established threshold
- Source of Elevation
- Ti implant corrosion (rare)
- Normal Serum Level
- Less than 1 ppb
- Threshold for Concern
- Greater than 5 ppb
- Source of Elevation
- Stainless steel corrosion
Routes of distribution:
- Local tissues - highest concentration, direct toxicity
- Regional lymph nodes - metal particles transported by macrophages
- Systemic circulation - ions absorbed into bloodstream
- Distant organs - liver, spleen, kidney accumulation
Biological Effects
Local tissue effects:
- Metallosis: Macroscopic metal staining of tissues (black/gray discoloration)
- Aseptic lymphocytic vasculitis-associated lesion (ALVAL): Type IV hypersensitivity
- Pseudotumor: Soft tissue mass with necrosis, not true neoplasm
- Osteolysis: Particle-induced bone resorption
ALVAL Pathophysiology:
ALVAL represents a Type IV delayed hypersensitivity reaction to metal ions:
ALVAL Development
Corrosion releases Co and Cr ions into tissues.
Metal ions bind to proteins, creating metal-protein complexes (haptens).
Antigen-presenting cells present hapten to T-cells. T-cells become sensitized (priming phase).
Continued metal release re-exposes sensitized T-cells.
T-cells recruit macrophages and lymphocytes. Perivascular lymphocytic infiltration. Tissue destruction and necrosis.
- Perivascular lymphocytic infiltration
- Aseptic fibrinoid necrosis
- Diffuse lymphocytic infiltrate
- Absence of infection
- Pain (most common)
- Soft tissue mass (pseudotumor on imaging)
- Instability or dislocation (soft tissue destruction)
- Elevated serum metal ions (Co and Cr)
Monitor all MoM hip patients with serum cobalt and chromium levels annually. Threshold for concern: greater than 7 ppb for either metal. MRI for soft tissue evaluation if elevated or symptomatic. Consider revision if progressive elevation or pseudotumor.
Systemic Effects
- Cobalt: Potential cardiomyopathy, thyroid dysfunction at very high levels
- Chromium: Theoretical carcinogenic risk (Cr^6+ form)
- Nickel: Known allergen, hypersensitivity common
Most patients with moderate metal elevation (5-10 ppb) do not have systemic symptoms, but long-term data limited.
This section completes the discussion of metal ion biological effects.
Anatomy of Corrosion Sites
Key Anatomical Sites of Implant Corrosion
Most critical corrosion site in modern THA
- Morse taper connection between femoral head and stem
- Contact area: 50-150 mm² depending on design
- Crevice geometry creates ideal environment for MACC
- Micro-motion disrupts protective oxide layer
Anatomy:
- Taper angle typically 5°40' (Morse taper)
- Roughness affects seating and corrosion
- Material couple (CoCr/Ti) critical factor
Modular neck systems
- Additional taper connection for neck modularity
- Double modular systems have two corrosion sites
- Higher failure rates led to some recalls
Key anatomy:
- Neck angle and offset adjustability
- Increased corrosion debris with two tapers
- Greater surface area for metal ion release
Implant Regions Prone to Corrosion
- Corrosion Type
- Crevice + fretting (MACC)
- Clinical Significance
- Primary failure site in modular THA
- Corrosion Type
- Crevice + fretting
- Clinical Significance
- Hardware loosening, pain
- Corrosion Type
- Fretting + third-body wear
- Clinical Significance
- Osteolysis, loosening
- Corrosion Type
- Tribocorrosion
- Clinical Significance
- Metal ion release, ALVAL
- Corrosion Type
- Pitting (rare)
- Clinical Significance
- Usually minor clinical impact
FRACS Viva Point: "Why is the head-neck taper the most important corrosion site?" Answer: Crevice geometry + micro-motion creates MACC environment. The combination of oxygen depletion in the crevice (low pH 3-4), cyclic loading causing micro-motion, and mixed metal couples maximizes corrosion.
Understanding anatomical sites of corrosion helps identify at-risk implants and plan revision surgery.
Classification
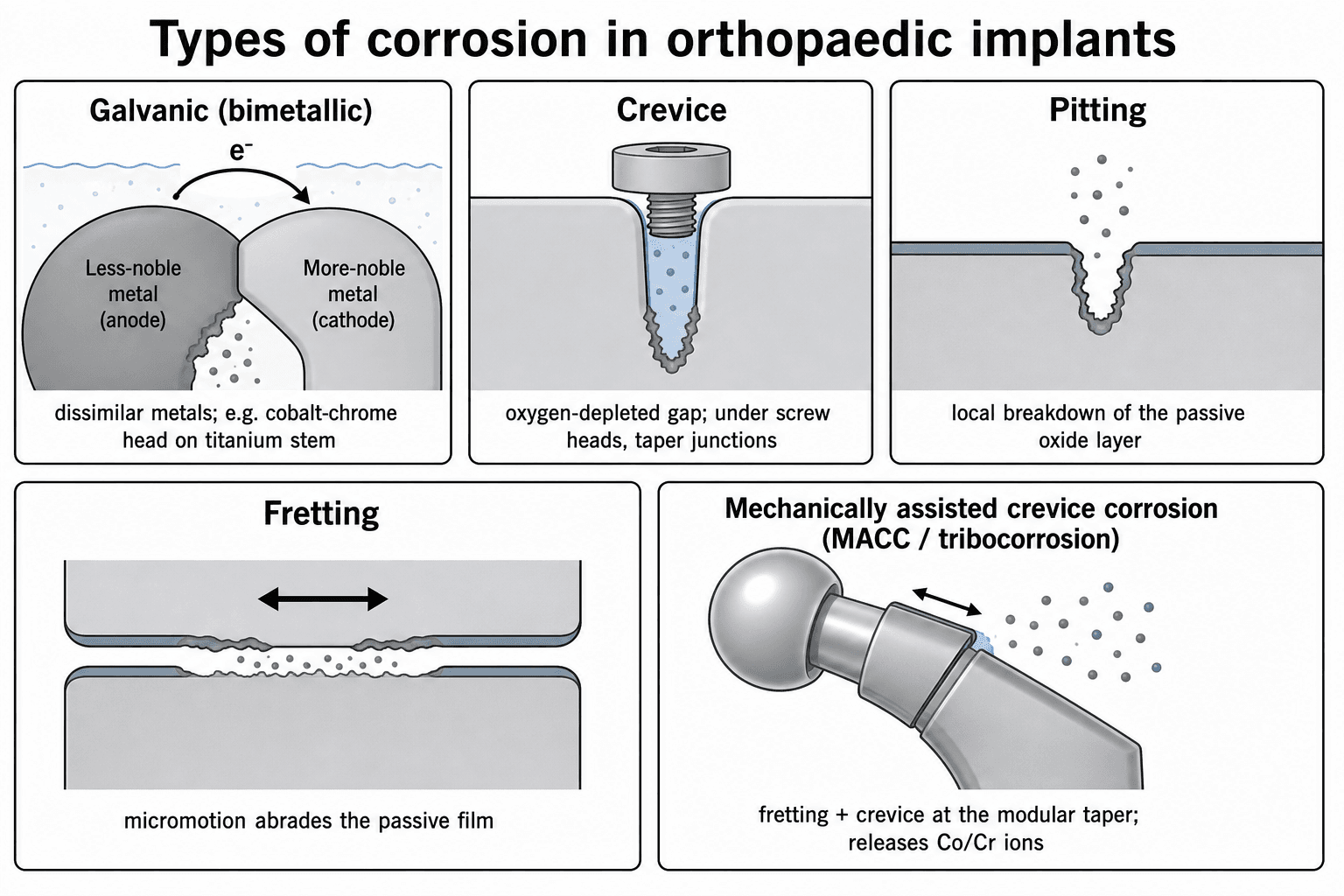
Four Major Types of Corrosion
Corrosion when two dissimilar metals contact in an electrolyte
- Less noble metal = anode (corrodes)
- More noble metal = cathode (protected)
- Electron flow from anode to cathode
- CoCr head on Ti stem
- Ti is less noble, corrodes at junction
- Mixed metal couples show worse outcomes
Localized corrosion within shielded areas
- Oxygen depleted in crevice
- pH drops to 3-4 (autocatalytic)
- Chloride concentration increases
- Passivation layer dissolves
- Modular taper junctions
- Screw-plate interfaces
- Under bone cement mantle
Highly localized passivation breakdown
- Chloride ions attack defects
- Small surface pit, deep penetration
- Self-propagating once initiated
- Stainless steel implants (most susceptible)
- Surface contamination sites
- Rare in Ti and CoCr
Mechanical wear + chemical corrosion
- Micro-motion disrupts oxide layer
- Fresh metal exposed and oxidizes
- Cyclic process with each loading cycle
- Modular tapers under load
- Polyethylene liner backside
- Screw-plate motion
MACC - The Key Mechanism
Mechanically-Assisted Crevice Corrosion (MACC) combines crevice + fretting corrosion. This is the PRIMARY failure mechanism at modular hip tapers. Micro-motion disrupts passivation within the crevice environment, accelerating metal dissolution.
Classification helps identify specific corrosion mechanisms and guide prevention strategies.
Investigations
Serum Metal Ion Testing
- Normal: Less than 1 ppb (μg/L)
- Elevated: 2-7 ppb - increased surveillance
- Concerning: Greater than 7 ppb - further investigation
- Critical: Greater than 20 ppb - revision often indicated
- Fasting sample (some foods contain metals)
- Trace element tube (metal-free)
- Recent activity may elevate levels
- Fasting morning sample
- Metal-free (trace element) tube
- Avoid contamination from needle hub
- Laboratory with validated assay (ICP-MS)
- MoM hips: Annual minimum
- Symptomatic: At presentation
- Post-revision: 3, 12 months
Imaging for Corrosion-Related Pathology
- Findings
- Osteolysis, implant migration, loosening
- Role
- First-line, baseline comparison
- Findings
- Pseudotumor, soft tissue necrosis, fluid collection
- Role
- Gold standard for ALVAL
- Findings
- Fluid collections, pseudotumor
- Role
- Screening, guided aspiration
- Findings
- Bone detail with metal suppression
- Role
- Osteolysis assessment
FRACS Viva Point: "What is MARS MRI?" Answer: Metal Artifact Reduction Sequence MRI uses specialized pulse sequences and post-processing to reduce metal artifact, allowing visualization of periprosthetic soft tissues to detect ALVAL, pseudotumor, and fluid collections.
Serum metal ions and MARS MRI are the cornerstone investigations for suspected corrosion-related pathology.

Management

Management Algorithm for Corrosion-Related Pathology
- Annual clinical review
- Annual metal ion levels
- Radiographs every 2 years
- Patient education on symptoms
- Symptoms develop
- Metal ions rise progressively
- Imaging abnormalities appear
- 6-monthly clinical review
- MARS MRI to assess soft tissues
- More frequent metal ion monitoring
- Progressive elevation of ions
- Imaging shows pseudotumor
- Patient high-demand, long life expectancy
Indications for Revision Surgery
- Strength
- Strong
- Timing
- Elective revision planned
- Strength
- Strong
- Timing
- Semi-urgent revision
- Strength
- Strong
- Timing
- Before bone loss worsens
- Strength
- Moderate-strong
- Timing
- Revision recommended
- Strength
- Moderate
- Timing
- Close surveillance vs revision
Delay increases complexity. Early revision before extensive soft tissue or bone destruction improves outcomes. Waiting for severe symptoms often means worse tissue damage.
Management depends on symptoms, metal ion levels, imaging findings, and patient factors.
Surgical Technique
Revision Surgery for Corrosion-Related Failure
- Taper corrosion with well-fixed stem
- Good bone stock
- No extensive tissue destruction
- Dislocate hip, remove head
- Clean taper thoroughly (dry)
- Inspect taper for damage
- New ceramic head on clean, dry taper
- Or sleeve adapter if taper damaged
- Loose stem
- Severe taper damage/fracture
- Extensive osteolysis
- Pseudotumor with bone destruction
- Extended approach for exposure
- Thorough debridement of necrotic tissue
- Revise acetabulum if affected
- New stem with modular options
- Bone grafting if needed
Soft Tissue Management
- Action
- Complete excision
- Rationale
- Remove source of inflammation
- Action
- Thorough debridement
- Rationale
- Remove reactive tissue
- Action
- Lavage, debride what possible
- Rationale
- May not fully remove all staining
- Action
- Debride back to viable tissue
- Rationale
- Document for prognosis
FRACS Viva Point: "How do you manage the taper at revision?" Answer: If taper undamaged: clean thoroughly, dry completely, place ceramic head with single firm impaction. If taper damaged: use a sleeve adapter system or revise the stem.
Careful debridement and appropriate component selection are essential for successful revision.
Complications
Complications of Implant Corrosion
- Soft tissue necrosis around implant
- Pseudotumor (solid or cystic mass)
- Abductor muscle destruction
- Femoral nerve compression (rare)
- Osteolysis from debris
- Periprosthetic bone loss
- May compromise revision fixation
- Cardiomyopathy (cobalt cardiomyopathy)
- Thyroid dysfunction
- Neurological symptoms (peripheral neuropathy)
- Visual and hearing impairment
- Usually greater than 50-100 ppb
- May be reversible with revision
- Cardiac monitoring recommended
Complication Severity
- Incidence
- 5-30% of MoM hips
- Severity
- Moderate to severe
- Incidence
- 5-15% (corrosion-related)
- Severity
- Moderate
- Incidence
- Less than 1%
- Severity
- Potentially severe
- Incidence
- Less than 1%
- Severity
- Severe - requires revision
- Incidence
- 10-20%
- Severity
- Variable
Exam Viva Point: "What are the systemic effects of cobalt toxicity?" Answer: Cardiomyopathy, hypothyroidism, peripheral neuropathy, and visual/hearing impairment. Usually occurs with very high serum cobalt levels (greater than 50-100 ppb) and may be reversible after revision surgery.
Complications range from local tissue destruction to rare but serious systemic toxicity.
Postoperative Care
Post-Revision Surveillance Protocol
- 3 months: Baseline after revision
- 12 months: Assess decline
- Annually: Until levels normalize
- Rapid initial decline (first 3-6 months)
- Gradual normalization over 1-2 years
- May not return to normal in all patients
- 6 weeks: Wound check, weight-bearing
- 3 months: Function assessment
- 6 months: Metal ions, radiographs
- 12 months: Comprehensive review
- Annually: Ongoing surveillance
- Hip function (Oxford Hip Score)
- Stability (dislocation precautions)
- Symptoms (pain, clicking)
Rehabilitation Considerations
- Focus
- Protected weight-bearing, precautions
- Special Considerations
- Extended hip precautions if abductor damage
- Focus
- Strengthening, gait training
- Special Considerations
- Focus on abductor rehabilitation
- Focus
- Progressive loading, function
- Special Considerations
- May need abductor brace if weak
- Focus
- Return to activities
- Special Considerations
- Some permanent limitations expected
Exam Viva Point: "How do you follow up a patient after revision for ALVAL?" Answer: Serial metal ion levels (3, 12 months then annual), clinical review for function and stability, imaging if symptoms, and extended hip precautions due to abductor compromise.
Close surveillance ensures early detection of complications and guides rehabilitation.
Outcomes
Outcomes After Revision for Corrosion
- Mean 50-70% reduction at 12 months
- Normalization (less than 2 ppb) in most patients
- Some patients have persistent elevation
- Rate of decline varies
- Extent of initial metallosis
- Completeness of debridement
- New implant bearing choice
- Oxford Hip Score: Significant improvement
- Harris Hip Score: Mean improvement 20-30 points
- Patient satisfaction: 70-85%
- Often do not reach primary THA levels
- Abductor weakness limits function
- Some persistent pain common
Outcome Predictors
- Better Outcome
- Minimal pseudotumor
- Worse Outcome
- Extensive destruction
- Better Outcome
- Intact abductors
- Worse Outcome
- Necrotic/absent abductors
- Better Outcome
- Minimal osteolysis
- Worse Outcome
- Severe bone loss
- Better Outcome
- Early (before extensive damage)
- Worse Outcome
- Late (symptomatic, severe ALVAL)
- Better Outcome
- Moderately elevated
- Worse Outcome
- Very high (greater than 50 ppb)
Exam Viva Point: "What determines outcome after revision for ALVAL?" Answer: Pre-revision tissue destruction (especially abductor status), bone stock, timing of revision (earlier is better), and completeness of debridement. Patients with extensive destruction have worse functional outcomes.
Early revision before extensive tissue destruction optimizes outcomes.
Clinical Implications and Prevention
Failed Metal-on-Metal Hips
Taper corrosion, NOT bearing surface wear in most modern MoM failures.
- Taper shows severe MACC with debris
- Bearing surfaces often well-preserved
- Mixed metal couples (CoCr/Ti) show worse corrosion
- Large head diameter increases taper mechanical stress
- Large femoral head diameter (greater than 36mm)
- Increased offset (higher moment arm on taper)
- High patient BMI and activity level
- Mixed metal couples (CoCr on Ti)
- Poor taper assembly (contamination, multiple impacts)
Taper Assembly Technique
Critical steps to minimize MACC:
Rationale:
- Clean and dry: Contaminants prevent full seating and increase micro-motion
- Single impaction: Multiple impacts damage taper surface
- Adequate force: Ensures taper engagement and minimizes micro-motion
- Matched materials: CoCr on CoCr eliminates galvanic component
Prevention Strategies
- Mechanism
- Eliminates metal taper corrosion
- Effectiveness
- Excellent
- Considerations
- Fracture risk (historical concern, rare with modern ceramics)
- Mechanism
- Eliminates galvanic corrosion
- Effectiveness
- Good
- Considerations
- CoCr on CoCr preferred over CoCr on Ti
- Mechanism
- Reduces taper mechanical stress
- Effectiveness
- Good
- Considerations
- Alternative bearing, not directly addressing corrosion
- Mechanism
- Reduces moment arm on taper
- Effectiveness
- Moderate
- Considerations
- May increase dislocation risk in some patients
- Mechanism
- Minimizes micro-motion
- Effectiveness
- Essential
- Considerations
- Clean, dry, single impaction - surgeon dependent
Material selection considerations:
- Titanium stems: Excellent corrosion resistance but weaker at taper when coupled with CoCr
- CoCr stems: Stronger taper but heavier, more stiff
- Ceramic heads: Eliminate taper corrosion but historical fracture concern
- Modern approach: Ceramic head on Ti stem is popular compromise
This completes the prevention strategies discussion.
Guidelines, Registries & Global Practice
Global Epidemiology of Corrosion-Related Failure
Implant corrosion is relevant wherever modular metal hip components are used, which is virtually universal. Two clinical phenotypes dominate: adverse reactions to metal debris (ARMD) from metal-on-metal (MoM) bearings, and head-neck taper corrosion (trunnionosis) in metal-on-polyethylene hips. The National Joint Registry of England and Wales demonstrated that stemmed MoM articulations fail at high rates that rise with head diameter, with young women receiving large-diameter heads at greatest risk.[Smith 2012] Pseudotumour develops in approximately 1% of MoM resurfacing patients within 5 years, with female sex and small components as key risk factors.[Pandit 2008]
What the major joint registries show:
- Stemmed large-head MoM THA has markedly higher revision than ceramic-on-ceramic or ceramic/metal-on-polyethylene
- Revision risk rises with head diameter for MoM (opposite to ceramic-on-ceramic)
- These signals drove global abandonment of large-head MoM by the early 2010s
- MoM bearings now represent a very small fraction of primary THA worldwide
Current global position:
- Higher revision than standard THA overall
- Better in young active men with large femoral heads; poor in women and small components
- Now confined to selected high-volume centres and specific designs
- Registry data (NJR, AOANJRR, NZJR) consistently show sex- and size-dependent outcomes
Surveillance Recommendations - Side by Side
- Core Recommendation
- Annual review of all MoM hips for implant life; blood Co/Cr and MARS MRI if symptomatic or ions elevated
- Evidence Basis
- Registry + retrieval evidence
- Core Recommendation
- Symptom-driven follow-up; metal ion testing and cross-sectional imaging for symptomatic patients
- Evidence Basis
- Expert/regulatory consensus
- Core Recommendation
- Risk-stratified surveillance; lower thresholds for large-head and symptomatic patients
- Evidence Basis
- Consensus, level IV-V
- Core Recommendation
- Co or Cr around 7 ppb (approximately 119 nmol/L) prompts further investigation
- Evidence Basis
- Cohort/registry correlation
Exam Viva Point: "What does registry evidence show about MoM hips?" Answer: National registries (NJR, AOANJRR, others) showed high, head-size-dependent revision rates for stemmed MoM THA, especially in young women with large heads. This evidence drove the global withdrawal of large-head MoM and underpins mandatory surveillance of existing implants.[Smith 2012]
Registry and retrieval evidence converted MoM corrosion from a theoretical concern into a worldwide device-safety issue.
MCQ Practice Points
Q: What provides corrosion resistance to titanium implants? A: TiO2 passivation layer (titanium oxide). This thin (2-10 nm) oxide layer forms spontaneously and is self-healing. It prevents titanium metal from contacting the corrosive environment.
Q: What is MACC and where does it occur? A: Mechanically-Assisted Crevice Corrosion - synergistic combination of micro-motion (disrupts passivation) and crevice environment (low pH, chloride). Primary failure mode at modular hip tapers.
Q: In a CoCr head on Ti stem taper, which metal corrodes? A: Titanium - Ti is less noble than CoCr in the galvanic series, so Ti acts as anode and corrodes preferentially. CoCr acts as cathode and is protected.
Q: What type of hypersensitivity reaction is ALVAL? A: Type IV delayed hypersensitivity (T-cell mediated). Metal ions bind proteins forming haptens, leading to T-cell sensitization and lymphocytic tissue infiltration.
Q: What serum cobalt or chromium level warrants concern in MoM hips? A: Greater than 5-7 ppb for either metal. Levels above this threshold associated with increased corrosion/wear and revision risk. Normal is less than 1 ppb.
Q: What is the pH inside a crevice undergoing crevice corrosion? A: pH 3-4 (highly acidic) - Metal hydrolysis produces H+ ions and oxygen depletion prevents neutralization. This low pH dissolves the passivation layer.
Q: What is the characteristic appearance of fretting corrosion debris? A: Black debris - mixture of metal oxide particles (FeO, TiO2, Cr2O3) from repeated disruption of passivation and oxidation. Distinguishes fretting from pure wear.
At a Glance
Corrosion is the electrochemical degradation of orthopaedic implants in the physiological environment (0.9% NaCl, pH 7.4, 37°C, proteins), occurring when the protective passivation layer (TiO₂, Cr₂O₃) breaks down. Four major corrosion types exist: Galvanic (dissimilar metal couples, e.g., CoCr/Ti), Crevice (oxygen depletion in gaps creating acidic pH 3-4), Pitting (localized passivation breakdown from chloride ions), and Fretting (micro-motion disrupting oxide layer). MACC (mechanically-assisted crevice corrosion) at modular taper junctions is the primary failure mechanism in modern hip implants, as micro-motion disrupts passivation within the crevice environment. Metal ion release leads to ALVAL (aseptic lymphocyte-dominated vasculitis-associated lesion), a Type IV delayed hypersensitivity reaction causing pseudotumor formation—serum cobalt and chromium levels monitor MoM hip patients. Prevention strategies include avoiding mixed metal couples, proper taper assembly (clean, dry, single impaction), polished surfaces, and ceramic femoral heads to eliminate head-taper corrosion.
GCPFTypes of Corrosion
Hook:Get Careful, Prevent Failure - know your corrosion types!
CHAMPSFactors Accelerating Corrosion
Hook:CHAMPS accelerate corrosion - control these factors!
ALVALALVAL Features
Hook:ALVAL describes the pathology of metal hypersensitivity reactions!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Examiner asks: Describe the four main types of corrosion in orthopaedic implants and give a clinical example of each.”
“Patient with painful MoM hip has serum cobalt 45 ppb, chromium 38 ppb, and MRI shows large pseudotumor. Examiner asks about pathophysiology and management.”
“Examiner asks: You are performing primary THA with a CoCr head on titanium stem. Describe your taper assembly technique and explain the rationale.”
Electrochemistry Basics
- Corrosion = electrochemical degradation (oxidation-reduction)
- Anode: M → M^n+ + e^- (metal oxidizes, goes into solution)
- Cathode: O2 + 2H2O + 4e^- → 4OH^- (reduction)
- Passivation layer (TiO2, Cr2O3) prevents corrosion
- Body fluid aggressive: 0.9% NaCl, pH 7.4, chloride ions
Four Types of Corrosion
- GALVANIC: Dissimilar metals (CoCr/Ti) - less noble corrodes (Ti)
- CREVICE: Oxygen depletion → pH 3-4 → passivation dissolved
- PITTING: Localized chloride attack → small hole, deep penetration
- FRETTING: Micro-motion disrupts passivation + corrosion (synergy)
- MACC = Mechanically-Assisted Crevice Corrosion (taper failure mode)
ALVAL Pathophysiology
- Aseptic Lymphocyte-dominated Vasculitis-Associated Lesion
- Type IV delayed hypersensitivity to Co and Cr ions
- Metal ions + proteins = haptens → T-cell sensitization
- Perivascular lymphocytic infiltration, tissue necrosis
- Pseudotumor = soft tissue mass with necrosis (not tumor)
- Histology: lymphocytes, no bacteria (NOT infection)
Metal Ion Monitoring
- Normal: Co and Cr less than 1 ppb
- Concern threshold: greater than 5 ppb either metal
- Action threshold: greater than 7 ppb warrants investigation
- Annual surveillance for all MoM hips recommended
- Elevated levels: MRI for pseudotumor, consider revision
- Levels decline 6-12 months after revision (slow)
Taper Assembly (Prevent MACC)
- CLEAN: No debris on tapers
- DRY: No blood/fluid contamination (prevents full seating)
- SINGLE: One firm impaction (multiple damages surface)
- MATCH: CoCr on CoCr better than CoCr on Ti (no galvanic)
- CERAMIC: Ceramic head eliminates taper corrosion risk
Prevention Strategies
- Avoid mixed metals (galvanic corrosion)
- Proper taper assembly critical
- Ceramic heads eliminate metal taper corrosion
- Avoid large heads (reduce taper mechanical stress)
- Polish surfaces (reduce stress concentrations for pitting)
Evidence Base
Goldberg, Gilbert, Jacobs et al - Multicentre Retrieval Study of Modular Taper Interfaces
- Retrieval analysis of 231 modular hip implants attributing in-vivo taper corrosion to mechanically-assisted crevice corrosion (MACC)
- Mixed-alloy couples corroded more than similar-alloy couples: moderate-to-severe head corrosion in 42% of mixed versus 28% of similar-alloy tapers
- Implantation time and neck flexural rigidity were predictors of corrosion and fretting
- Larger-diameter (stiffer) necks may reduce fretting, balanced against range-of-motion loss
Langton et al - Early Failure of Metal-on-Metal Bearings from Adverse Reaction to Metal Debris
- Series of 660 MoM resurfacings/large-head THRs: 3.4% (17 hips, all ASR) revised for adverse reaction to metal debris (ARMD)
- ARMD patients had significantly higher blood and joint chromium and cobalt ion concentrations than asymptomatic patients (all p less than 0.001)
- ARMD associated with smaller components and higher acetabular anteversion
- Explants from ARMD revisions showed greater bearing wear, supporting excess wear as a driver
Willert et al - Metal-on-Metal Bearings and Hypersensitivity (ALVAL)
- Landmark description of a lymphocyte-dominated immunological reaction (ALVAL) in revised second-generation MoM hips
- Histology: diffuse and perivascular T and B lymphocyte infiltrates, high endothelial venules, fibrin exudation, macrophages and necrosis - distinct from infection
- Only few metal particles seen, supporting hypersensitivity rather than purely particle-volume-driven reaction
- Patients re-revised to another MoM articulation had no symptom relief
These three studies establish the electrochemical mechanism (MACC) and the hypersensitivity basis (ALVAL) of corrosion-related implant failure.