SI Joint Fracture-Dislocation (Day Classification)
- A 'crescent fracture' is a fracture-dislocation of the SACROILIAC (SI) JOINT and is a recognised subset of pelvic-ring injuries caused by a LATERAL COMPRESSION force: the SI joint is disrupted and the injury extends proximally as a fracture of the POSTERIOR ILIAC WING, leaving a crescent-shaped fragment of ilium still attached to the sacrum by the intact posterior SI ligaments.
- It is the posterior lesion of a LATERAL-COMPRESSION pelvic-ring injury (Young-Burgess LC, with an associated anterior ring/rami injury); it is typically ROTATIONALLY unstable but VERTICALLY stable (the strong posterior SI ligaments on the crescent fragment resist vertical migration).
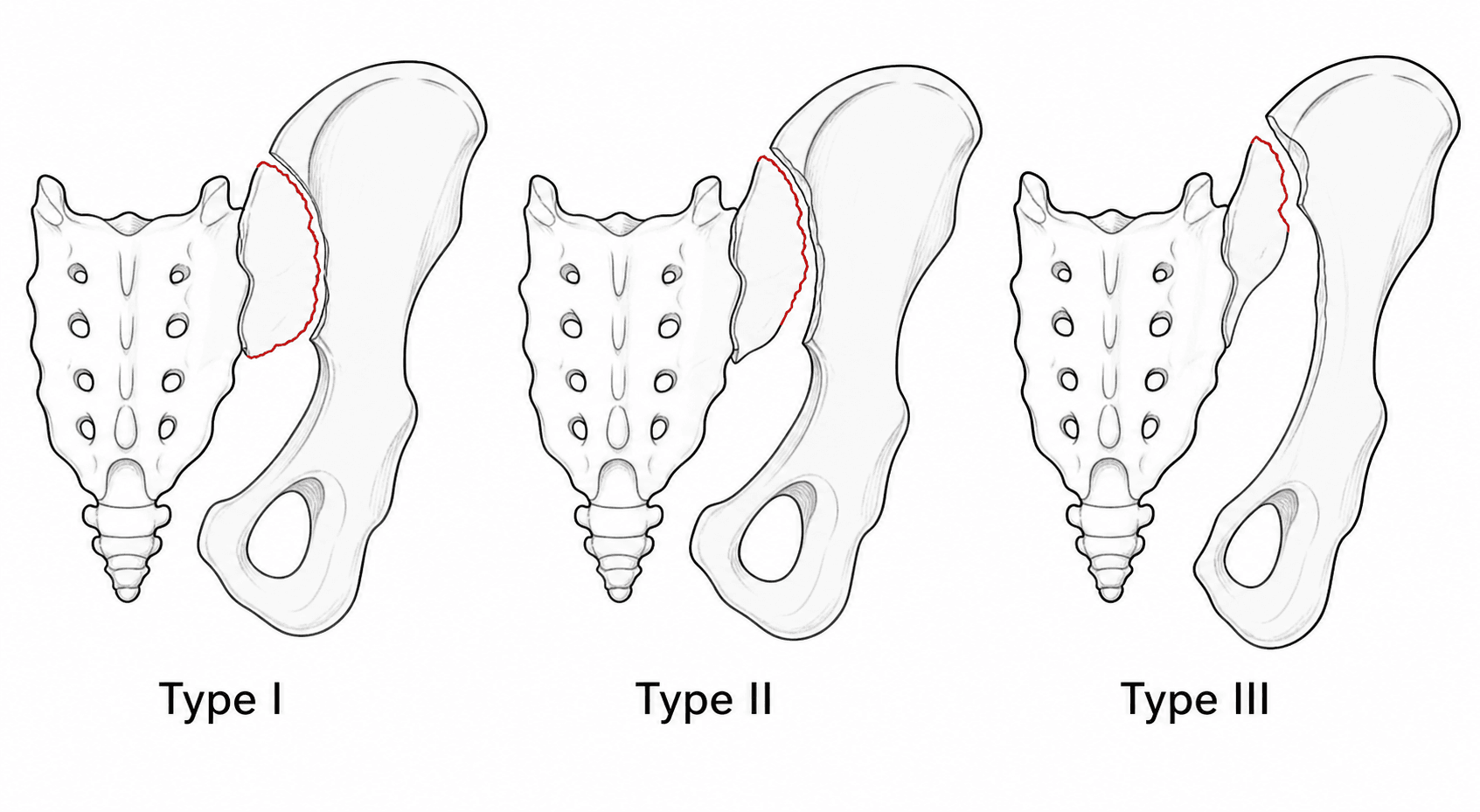
- The DAY CLASSIFICATION grades it by the SIZE of the crescent fragment and the PROPORTION of the SI joint that is dislocated: Type I = LARGE crescent / dislocation up to one-third (inferior); Type II = intermediate crescent / one- to two-thirds dislocated; Type III = SMALL crescent / most of the joint dislocated.
- The classification GUIDES the surgical approach and fixation: a LARGE crescent (Type I) is reduced and fixed largely as an ILIAC-WING fracture (ORIF, e.g. via an anterior or posterior iliac approach, with plates/screws), whereas a SMALL crescent (Type III) behaves like a pure SI DISLOCATION and is best stabilised with ILIOSACRAL (sacroiliac) SCREWS.
- The PRINCIPAL GOAL of surgery is ACCURATE and STABLE REDUCTION of the SI joint; many crescent fractures can be managed by CLOSED (or open) reduction and PERCUTANEOUS ILIOSACRAL SCREW fixation - in one series percutaneous iliosacral screws were used in about 60% after reduction.
- Because it is a high-energy pelvic-ring injury (lateral compression), assess for ASSOCIATED injuries (anterior ring fractures, visceral/urogenital injury, head/chest/abdominal injuries) and follow pelvic-trauma resuscitation principles; outcomes are good with accurate reduction, though confounded by the associated high-energy injuries.
- “Crescent fracture = lateral-compression SI joint fracture-dislocation with a posterior iliac crescent fragment held to the sacrum by intact posterior SI ligaments (rotationally unstable, vertically stable).
- “Day classification by crescent size: large (I) -> treat as an iliac fracture (ORIF); small (III) -> treat as an SI dislocation (iliosacral screws); intermediate (II) -> address both.
- “Goal = accurate stable reduction of the SI joint; many are amenable to closed reduction + percutaneous iliosacral screws.
Most of the posterior support is on the iliac fragment (held by intact posterior SI ligaments). Treat it like an iliac-wing fracture - ORIF of the crescent achieves SI-joint stability.
Little ilium remains attached; the injury behaves like a near-complete SI joint dislocation. Stabilise the SI joint itself with iliosacral (sacroiliac) screws after reduction.
Mechanism & Anatomy
The crescent fracture results from a lateral compression force applied to the pelvis. Posteriorly, this disrupts the sacroiliac joint and the injury propagates as a fracture through the posterior iliac wing, splitting off a crescent-shaped fragment of ilium that remains attached to the sacrum via the strong, intact posterior sacroiliac ligaments. Because those posterior ligaments stay attached to the crescent fragment, the injury is generally vertically stable but rotationally unstable. It is the posterior component of a Young-Burgess lateral-compression pelvic-ring injury and is usually accompanied by an anterior ring (pubic rami) injury.
The Day Classification
- Crescent fragment
- Large
- SI joint dislocated
- Up to ~one-third (inferior)
- Implication
- Iliac fracture dominates -> ORIF of the ilium
- Crescent fragment
- Intermediate
- SI joint dislocated
- About one- to two-thirds
- Implication
- Mixed -> reduce/fix fracture and joint
- Crescent fragment
- Small
- SI joint dislocated
- Most of the joint (not all)
- Implication
- Behaves as SI dislocation -> iliosacral screws
The Day classification is useful because it directs the approach and reduction technique. The larger the crescent (Type I), the more the posterior stability resides in the iliac fragment, so fixing the iliac fracture restores the SI joint; the smaller the crescent (Type III), the more the injury is a joint dislocation, so iliosacral screw fixation across the SI joint is needed. Type II sits in between. (Some crescents do not fit neatly into the three types, and the scheme has been proposed for expansion.)
Assessment & Management
- Pelvic radiographs (AP, inlet/outlet) and CT (defines the crescent size, SI-joint dislocation and any sacral/anterior-ring injury - essential for Day typing and planning)
- Treat as a high-energy pelvic-ring injury: resuscitation, assess haemodynamics, and screen for associated visceral/urogenital, head, chest and abdominal injuries
- Examine neurology (lumbosacral plexus/roots) and skin (Morel-Lavallée lesion)
Accurate and stable reduction of the SI joint is the principal goal - restoring the posterior ring to allow weight-bearing and prevent malunion/chronic pain. The Day type selects the approach and whether to fix the fracture (ilium) or the joint (iliosacral screws) - or both.
- Type I (large crescent): open reduction and internal fixation of the iliac fracture (anterior or posterior iliac approach; plates and/or lag screws) - this re-establishes SI-joint stability.
- Type III (small crescent): behaves like an SI dislocation - closed (or open) reduction and percutaneous ILIOSACRAL (sacroiliac) SCREW fixation across the SI joint.
- Type II (intermediate): a combination - reduce the joint and stabilise both the fracture and the SI joint as needed (often iliosacral screws +/- iliac fixation). Many crescent fractures are amenable to closed reduction and percutaneous iliosacral screw fixation, and in selected stable patterns non-operative management or external fixation has a role; the choice is individualised to the fracture type and the patient.
The Iliosacral Screw: Corridor, Reduction-First & Sacral Dysmorphism
- Reduce first - the screw does not reduce the joint: a percutaneous iliosacral screw fixes a reduced SI joint, it does not achieve the reduction, and it cannot be placed safely through a malreduced joint (a malreduction throws the bony corridor out of line and pushes the screw towards neural structures). So obtain an accurate closed (or open) reduction first, then fix.
- Stay in the osseous corridor: the screw runs from the lateral ilium, across the SI joint, into the S1 (and sometimes S2) vertebral body, and must remain entirely within bone. The structures just outside the corridor are the L5 nerve root (crossing the ala superiorly), the S1 foramen and roots, and the sacral canal - an extraosseous screw injures them. A transiliac-transsacral screw (passing through both ilia and across S1) needs a corridor wide enough to accept it.
- Beware the dysmorphic sacrum: a substantial minority have upper-sacral dysmorphism (an acute alar slope, mammillary bodies, a residual S1 disc, a "tongue-in-groove" SI joint and a raised colliculus) that narrows and angulates the S1 corridor, so a transsacral S1 screw may be impossible - use an oblique S1 and/or an S2 corridor instead. Recognise it on the preoperative outlet view and CT.
- Confirm with imaging: true inlet and outlet fluoroscopic views plus a strict lateral sacral view (the iliac cortical density and alar slope) - or navigation - confirm the screw stays in bone.
Iliosacral screw rules: reduce the SI joint first (the screw fixes, it does not reduce, and won't go safely through a malreduction); keep it in the osseous corridor (L5 root over the ala, S1 foramen and canal are just outside); and screen for sacral dysmorphism (narrow/angulated S1 corridor) where an S2 or oblique corridor is safer - confirmed on inlet/outlet and a true lateral sacral view.
The L5 Root and the Price of Malreduction
- The L5 nerve root is the structure at risk: it runs over the sacral ala, roughly a finger-breadth (around 2 cm) medial to the SI joint, where it joins the lumbosacral trunk between the ala and the L5 transverse process. It is vulnerable to the original fracture displacement and, intra-operatively, to an anterior SI-joint plate, reduction clamp or a misdirected screw - so identify and protect it in any anterior approach (the full plexus anatomy is in our Lumbosacral Plexus Anatomy topic).
- Accurate reduction is the long-term determinant: a malreduced SI joint leads to chronic posterior pelvic pain, SI nonunion and post-traumatic SI arthrosis, and pelvic malunion (limb-length and rotational deformity) - hence the goal is anatomical reduction; the high-energy associated injuries confound the reported functional scores (as Day noted).
- Mind the soft-tissue envelope: an overlying Morel-Lavallée lesion (a closed degloving over the flank/trochanter, with a real infection risk) influences the timing and the posterior approach to fixation (managed as in our Morel-Lavallée Lesion topic).
The L5 root crosses the ala about 2 cm medial to the SI joint - protect it from the fracture, the clamp and the anterior plate/screw. Long term, malreduction (not the bone loss) drives the morbidity: chronic posterior pelvic pain, SI nonunion/arthrosis and pelvic deformity - so reduce it accurately, and respect an overlying Morel-Lavallée lesion when timing surgery.
Mnemonics & Memory Aids
CRESCENT
Hook:A CRESCENT fracture: lateral compression, SI fracture-dislocation, classify on CT, type drives fixation.
DAY
Hook:DAY: bigger crescent = fix the fracture (ORIF); smaller crescent = fix the joint (SI screws).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has a lateral-compression pelvic injury with a posterior iliac fracture extending into the SI joint. What is this injury, what is the relevant anatomy, and how do you classify it?”
“How does the Day type guide your surgical management of a crescent fracture?”
What it is
- Lateral-compression SI joint fracture-dislocation; posterior iliac-wing fracture leaves a crescent fragment
- Crescent stays attached to the sacrum via intact posterior SI ligaments
- Rotationally unstable, vertically stable; Young-Burgess LC (+ anterior ring injury)
Day classification
- Type I: large crescent, <=1/3 SI dislocated (inferior)
- Type II: intermediate crescent, 1/3-2/3 dislocated
- Type III: small crescent, most of SI dislocated
Assessment
- Pelvic radiographs (AP/inlet/outlet) + CT (type it, plan)
- High-energy: resuscitate, screen visceral/urogenital/other injuries; assess neurology
- Goal = accurate, stable reduction of the SI joint
Fixation by type
- Type I: ORIF of the iliac fracture (anterior/posterior approach)
- Type III: percutaneous iliosacral (SI) screws (treat as SI dislocation)
- Type II: combination; many amenable to closed reduction + percutaneous iliosacral screws (~60%)
Evidence & Key Studies
Crescent fracture-dislocation of the sacroiliac joint: a functional classification
- Crescent fracture-dislocations are a lateral-compression pelvic-ring injury - SI joint disruption extending proximally as a posterior iliac-wing fracture.
- Describes three types: Type I (large crescent, dislocation no more than one-third of the SI joint, typically inferior), Type II (intermediate crescent, one- to two-thirds dislocated), Type III (small crescent, most of the joint dislocated).
- The principal goal is accurate, stable reduction of the SI joint; the classification guides the surgical approach and reduction technique, with good functional results.
Posterior iliac crescent fracture-dislocation: what morphological variations are amenable to iliosacral screw fixation?
- In 100 patients (16 Type I, 47 Type II, 37 Type III; 12 unclassifiable), the majority of crescent fracture-dislocations were amenable to closed reduction and percutaneous iliosacral screw fixation.
- Percutaneous iliosacral screw fixation was used in 60% of crescents after closed or open reduction.
- Suggests the Day classification be expanded to include variant injury patterns.
The lateral-compression mechanism, the crescent-fragment anatomy and the three-type classification come from the cited Day original paper, and the amenability to percutaneous iliosacral screw fixation (used in ~60%) from the cited Calafi & Routt series. The Young-Burgess lateral-compression context and the rotationally-unstable/vertically-stable behaviour are standard, well-established pelvic-trauma teaching. (See also our Pelvic Ring Injury and Sacral Fracture material.)