Bimodal Distribution | Hoffa Fractures | Nail vs Plate Debate
- Hoffa fracture (coronal plane) is often missed on X-ray - CT mandatory for all articular fractures
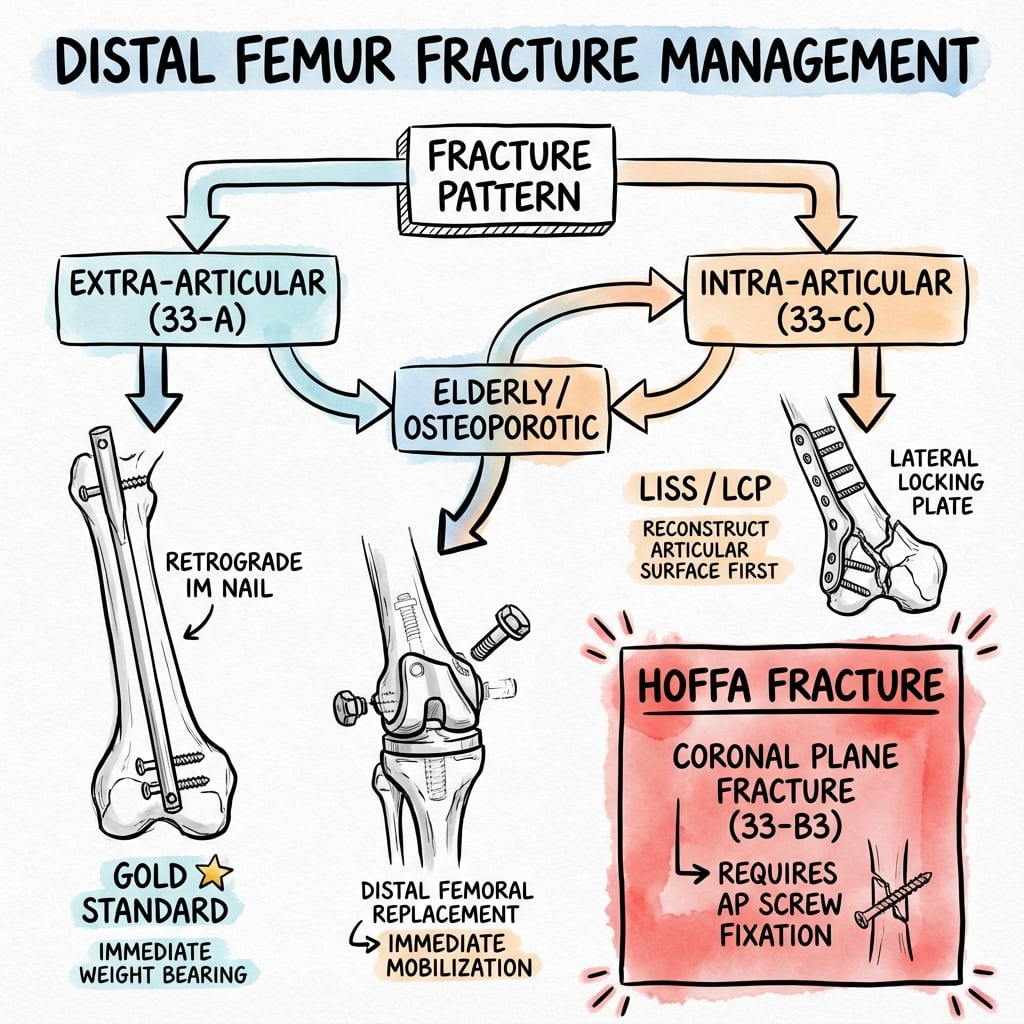
- Retrograde nail preferred for extra-articular (A) types - allows immediate weight bearing
- Lateral locking plate (LISS/LCP) workhorse for intra-articular (C) types
- Dual plating (medial + lateral) needed for comminuted medial column
- Distal femoral replacement (megaprosthesis) indicated for elderly independent ambulators with severe comminution
- “Look for the coronal plane fracture (Hoffa) in 33-B and 33-C types
- “Gastrocnemius causes recurvatum deformity (pulls distal fragment posterior)
- “Adductor magnus causes varus deformity
- “Quadriceps/hamstrings cause shortening
Clinical Imaging
Imaging Atlas




38% of intra-articular fractures have a coronal plane (Hoffa) component. Often missed on plain X-ray. CT is mandatory. Usually lateral condyle. Requires AP screws to fix.
Gastrocnemius flexes distal fragment (Recurvatum). Adductors cause Varus. Quadriceps causes Shortening. Reduction must overcome these forces (flex knee to relax gastroc).
High 1-year mortality (30%). Goal is immediate weight bearing. Fixation failure is common in osteoporosis. Consider Distal Femoral Replacement (DFR) if fixation dubious.
Popliteal artery is tethered at hiatus and trifurcation. Displaced fractures (recurvatum) can injure artery. Check pulses and ABI.
| Age/Function | Fracture Type | Treatment | Pearl |
|---|---|---|---|
| Young / Active | Extra-articular (33-A) | Retrograde IM Nail | Allows immediate load bearing, less soft tissue strip |
| Young / Active | Intra-articular (33-C) | Lateral Locking Plate (LCP) | Anatomic articular reduction is priority |
| Any Age | Hoffa Fracture (33-B) | AP Screws + Buttress Plate | Must fix coronal component separately |
| Elderly / Osteoporotic | Comminuted Intra-articular | Distal Femoral Replacement | Immediate WB, avoid non-union/failure |
| Periprosthetic | Loose Implant | Revision Arthroplasty | Fixation will fail if implant loose |
GRASDeforming Forces
Hook:The GRAS pulls the femur into a deformed position!
HOFFAHoffa Fracture Features
Hook:HOFFA fractures are Hidden One-condyle Flexion Articular injuries!
LALSurgical Goals
Hook:Restore LAL to get the femur back to normal!
Overview and Epidemiology
Distal femur fractures are challenging due to comminution, osteoporosis, and intra-articular extension. The examiner will test your decision-making between nailing (A-type) vs plating (C-type) vs arthroplasty (elderly), and your ability to spot and manage the Hoffa fragment.
- Bimodal: Young males (high energy) and Elderly females (low energy)
- Osteoporosis is major factor in elderly
- Periprosthetic fractures increasing with TKA volume
- High energy: Axial load with varus/valgus
- Low energy: Simple fall (spiral pattern)
- Dashboard injury: Axial load through a flexed knee
Anatomy
The distal femur is trapezoidal - wider posteriorly. The lateral surface is inclined 10 degrees (not vertical) - plates must match this or risk malalignment. The Blumensaat's line indicates slope of intercondylar notch.
Distal Femur Anatomy
- Flares from cylinder to condyles
- Lateral wall inclined 10 degrees (slopes medial)
- Anterior wall inclined 25 degrees (trochlea)
- Medial condyle extends more distal (plus distal joint angle)
- Gastrocnemius: Posterior condyles (flexes fragment)
- Adductor Magnus: Adductor tubercle (varus force)
- Quadriceps: Patella (shortening)
- Hamstrings: Proximal tibia (shortening)
Classification Systems
AO/OTA Classification (33)
| Type | Description | Subtypes | Treatment |
|---|---|---|---|
| 33-A | Extra-articular | A1: Simple, A2: Wedge, A3: Comminuted | Retrograde Nail or Plate |
| 33-B | Partial Articular | B1: Lateral (Hoffa), B2: Medial, B3: Anterior | Screw fixation + Buttress |
| 33-C | Complete Articular | C1: Simple/Simple, C2: Simple/Multi, C3: Multi/Multi | Lateral Locking Plate |
Type B3 (coronal shear) is the Hoffa. Lateral condyle (Letenneur I-III) most common. Need to fix with countersunk screws from anterior to posterior (or vice versa) perpendicular to fracture line.

Clinical Assessment
- Deformity: Usually shortened and externally rotated
- Skin: Check posterolateral (open spikes) and anterior (contusion)
- Vascular: Pulses, ABI - high index of suspicion
- Nerves: Peroneal/Tibial nerve exam
- Pre-injury function: Independent vs housebound (guides arthroplasty decision)
- TKA History: Implant type, time since surgery
- Comorbidities: Optimize for surgery
Look for ipsilateral tibial shaft or plateau fracture ("floating knee"). This is a high-energy injury with significantly increased complications (fat embolism, vascular injury, compartment syndrome). Fix femur first usually.
Differential Diagnosis
| Diagnosis | Distinguishing Features | Confirming Investigation |
|---|---|---|
| Distal femur fracture | Supracondylar deformity, recurvatum, crepitus, axial pain | AP/lateral radiograph plus CT for articular extension |
| Tibial plateau fracture | Tenderness below joint line, valgus/varus instability, effusion | Knee radiograph and CT; check for floating knee |
| Patella fracture | Anterior tenderness, palpable gap, loss of active extension | Lateral knee radiograph, skyline view |
| Periprosthetic fracture (around TKA) | Prior TKA, fracture above femoral component | Radiograph; assess implant fixation status |
| Pathological fracture (metastasis/myeloma) | Low-energy mechanism, prior pain, lytic lesion, known primary | Radiograph, MRI, bloods, staging if no known primary |
| Knee dislocation / multiligament injury | Gross instability, dimple sign, high vascular risk | Reduction, ABI/CTA, examination under anaesthesia |
Investigations
Imaging Protocol
AP and Lateral of femur and knee. Traction view can help define phenotype. Full length femur to rule out ipsilateral hip/shaft.
Current standard of care for ALL distal femur fractures. 38% have coronal (Hoffa) fractures missed on X-ray. Helps plan articular reduction screw trajectory.
If pulses asymmetric or ABI less than 0.9. Low threshold due to popliteal tethering.
A traction X-ray (manually applied traction) in ED often reveals the fracture pattern better than the initial comminuted mess. Helps determine if the articular block is reconstructable.


Management Algorithm
In elderly patients, the goal is immediate full weight bearing. Fixation that requires restricted weight bearing (NWB) has high mortality and failure rates. If fixation cannot support FWB, choose Distal Femoral Replacement (arthroplasty).
Surgical Approaches
| Approach | Indication | Interval | Nerve at Risk |
|---|---|---|---|
| Lateral Parapatellar | Standard for ORIF | Vastus lateralis / Rectus | Superior lateral genicular artery |
| Swashbuckler | Complex articular | Lat parapatellar + Snip | Superior medial genicular |
| Medial Subvastus | Medial plate | Vastus medialis / Adductors | Saphenous nerve |
| Trans-tendinous | Nail entry | Split patellar tendon | Infrapatellar branch saphenous |
The Swashbuckler approach is a modified lateral parapatellar approach with a lateral quadriceps snip. It allows the patella to subluxate medially, giving complete exposure of the articular surface while preserving blood supply.
Surgical Technique
Lateral Locked Plating - ORIF
Patient Positioning:
- Supine on radiolucent table
- Bump under ipsilateral hip for neutral rotation
- Knee slightly flexed over radiolucent triangle
Approach:
- Lateral approach through iliotibial band
- Preserve soft tissue attachments to bone
- MIPO technique for extra-articular fractures
- Direct exposure for intra-articular fractures
Articular Reduction:
- K-wires for provisional fixation
- Anatomic articular reduction (step-off under 2mm)
- Lag screws (outside plate footprint) for condylar splits
- Confirm under fluoroscopy
Plate Application:
- Anatomic distal femur locking plate
- Submuscular plate insertion for shaft
- Confirm alignment before proximal fixation
- Avoid varus malreduction (most common error)
Locking Screws:
- Locking screws in metaphysis and distal fragment
- Mix of locking and cortical proximally
- Leave 2-3 empty holes at fracture for flexibility
Anatomic articular reduction and stable fixation are essential for good outcomes.
Complications
| Complication | Rate | Risk Factors | Management |
|---|---|---|---|
| Non-union | 5-10% | Bridge plating too stiff, smoking, open | Dual plating + Bone graft |
| Malunion (Valgus/Varus) | 10-20% | Poor intra-op alignment | Osteotomy if symptomatic |
| Infection | 3-5% | Open fracture, OR time, Obesity | Debridement, hardware removal |
| Knee Stiffness | Common | Prolonged immobilization | Arthroscopic lysis of adhesions |
| Implant Failure | 5% | Early WB on weak fixation | Revision to DFR or nail |
| Prominent Hardware | 10-20% | Iliotibial band irritation | Removal after union |

Postoperative Care and Rehabilitation
Rehab Protocol
Immediate ROM is critical to prevent adhesions. CPM machine often used. Toe-touch weight bearing (unless nail/DFR).
X-ray check. Advance weight bearing if callus visible.
Full weight bearing. Quad strengthening. Returns to baseline 6-12 months.
Nail: WBAT usually allowed. DFR: WBAT allowed. Plate: TDWB/PWB (15kg) for 6-12 weeks until callus. This restriction is why plating is less ideal for frail elderly.
Outcomes and Prognosis
Union and Function
| Method | Union Rate | Time to Union | Key Considerations |
|---|---|---|---|
| Retrograde nail | 85-95% | 12-16 weeks | Early WB, good for extra-articular |
| Lateral locking plate | 85-90% | 16-20 weeks | Protected WB needed, versatile |
| Dual plating | 80-90% | 16-24 weeks | For unstable medial column |
| Distal femoral replacement | N/A | N/A | Salvage or severe comminution in elderly |
Prognostic Factors
Extra-articular fracture pattern. Good bone quality. Anatomic reduction achieved. Early ROM and rehabilitation. Non-smoker.
Complex articular involvement (C3). Severe osteoporosis. Varus malreduction. Delayed surgery or infection. Open fracture.
Functional Outcomes
Most patients achieve functional independence and return to baseline mobility. Knee stiffness is the most common functional problem, particularly with prolonged immobilization. Arthrofibrosis may require manipulation or arthroscopic lysis of adhesions. Long-term post-traumatic arthritis is common with intra-articular injuries, with some patients requiring eventual arthroplasty.
Evidence Base and Key Trials
Femur-LISS vs Distal Femoral Nail (Prospective Comparative)
- Prospective comparison of LISS plate vs distal femoral nail (two groups of 16, n=32)
- No significant difference in epidemiology, fracture type, infection or malalignment
- Lysholm-Gillquist scores equivalent at 1 year (plate 110 vs nail 103 degrees ROM)
- Both minimally invasive implants superior to the condylar blade plate for infection and axial malalignment
Retrograde Nail vs Locking Plate (Meta-analysis)
- Systematic review and meta-analysis of 16 studies (6 RCTs), 936 patients (467 nail, 477 plate)
- Significantly fewer non-unions and deep infections in the retrograde nail group
- Locking plate group achieved better postoperative knee range of motion
- No difference in union time, overall complications, re-operation rate or surgical duration
Cochrane Review: Interventions for Distal Femur Fractures
- Seven trials, 444 adults; all small and at substantial risk of bias
- Largest trial (n=126) found no significant difference between nail and locking plate at 1 year
- Trend toward better function (SMFA) and quality of life (EQ-5D) favouring nail, confidence intervals crossed null
- Evidence graded very low; a definitive pragmatic multicentre RCT is the stated priority
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 78-year-old female presents after a fall on stairs. Knee is swollen and painful. X-ray shows distal femur fracture (33-A2).”
“A 30-year-old motorcyclist has a C3 distal femur fracture. CT shows a displaced coronal plane (Hoffa) fracture of the lateral condyle.”
“45-year-old male, 6 months post-LISS plating of open distal femur fracture. Pain on WB. X-ray shows broken plate.”
MCQ Practice Points
Q: Which femoral condyle is most commonly involved in a Hoffa fracture? A: Lateral Condyle - The lateral condyle is involved in 70-85% of cases due to the valgus vector of force in a flexed knee.
Q: Which muscle is responsible for the recurvatum (hyperextension) deformity of the distal fragment? A: Gastrocnemius - It originates on the posterior femoral condyles and flexes the distal fragment.
Q: On current evidence, what advantages does retrograde nailing have over locking plate fixation for amenable distal femur fractures? A: Lower non-union and infection rates - meta-analysis (Aggarwal 2022) found significantly fewer non-unions and deep infections with the nail, although locking plates achieved better knee range of motion. No adequately powered RCT has settled the debate (Cochrane 2015, TrAFFix 2019).
Q: A medial locking screw placed too long is at risk of injuring which structure? A: Femoral Vessel (at Hunter's canal) - If placed in the proximal part of the plate. Distally, the popliteal vessels are posterior and central.
Q: What defines an AO 33-C3 distal femur fracture? A: Complete articular fracture with multifragmentary articular component - The 33 designates distal femur, C indicates complete articular involvement, and 3 denotes comminution of the articular surface.
Q: In an AO 33-C fracture, what is the correct order of reduction? A: Articular first, then metaphyseal - First reconstruct the articular surface anatomically, then reduce the articular block to the shaft. "Fix the joint to the shaft."
Guidelines, Registries & Global Practice
- Account for roughly 3-6% of all femoral fractures
- Bimodal: high-energy injuries in young men; low-energy fragility fractures in older women
- Incidence is rising with an ageing population and increasing total knee arthroplasty volume (periprosthetic fractures)
- 1-year mortality in elderly/periprosthetic cohorts is substantial (commonly reported 18-30%), comparable to hip fracture
- Anatomic articular reduction, then restore length/axis/rotation of the metaphysis
- Biological (soft-tissue sparing) fixation to protect union
- In frail elderly, prioritise constructs allowing immediate weight bearing
- Orthogeriatric co-management and early mobilisation (within 24-48 hours) reduce mortality
| Body | Region | Key Emphasis |
|---|---|---|
| AO Foundation | Global | Articular-block-then-shaft sequence; nail for extra-articular, locked plate/MIPO for articular; medial column support when deficient |
| AAOS | USA | Evidence-based perioperative optimisation; CT for articular extension; shared decision-making on fixation vs arthroplasty |
| BOA / BOAST | UK | Senior decision-making, early definitive fixation, orthogeriatric input for fragility fractures, mobilisation by next day |
| EFORT / European consensus | Europe | Acute distal femoral replacement as a valid option for comminuted osteoporotic and periprosthetic fractures |
Registry & systematic-review signals (arthroplasty for fracture):
- Distal femoral replacement (DFR) for acute fracture carries a higher revision rate than DFR for oncological reconstruction, with infection and aseptic loosening the leading failure modes.
- For periprosthetic fractures around a total knee replacement, fixation reliably fails if the femoral component is loose - revision arthroplasty is then mandatory regardless of bone stock.
- Pooled data (Senthilkumaran 2019) support acute knee arthroplasty in selected osteoporotic comminuted fractures, with 1-year mortality 18.4% and revision 3.4%.
- Routine CT, anatomic locking plates, retrograde nails and modular DFR readily available
- Increasing use of dual plating and acute arthroplasty for the comminuted elderly fracture
- Orthogeriatric pathways and early-mobilisation protocols standard
- CT may be unavailable - higher risk of missing the Hoffa fragment; rely on traction and stress views plus careful intra-operative assessment
- Conventional plates / condylar blade plates and SIGN-type nails used where premium locking implants are unaffordable
- DFR megaprostheses often inaccessible; fixation (even with restricted weight bearing) remains the default
Controversies and Areas of Uncertainty
Meta-analysis favours the nail for lower non-union and infection in amenable patterns, while plating gives better ROM and handles complex articular fractures. No adequately powered definitive RCT exists (Cochrane, TrAFFix) - the choice remains pattern- and surgeon-driven.
For the comminuted osteoporotic or periprosthetic fracture, DFR allows immediate weight bearing but carries higher infection/loosening risk; locked plating preserves bone but may demand protected weight bearing. Mortality is broadly equivalent (Hoellwarth).
When and how aggressively to add a medial plate is debated. Over-stiff lateral constructs (short working length) cause asymmetric callus and non-union; far-cortical locking and titanium plates aim to tune stiffness, but optimal screw density is unsettled.
Posterior-to-anterior screws are biomechanically stronger for the coronal fragment, but anterior-to-posterior (countersunk) screws are technically easier and avoid posterior dissection. The trade-off remains contested.
Key Anatomy
- Trapezoidal shape (wider posterior)
- Lateral wall inclined 10 degrees
- Popliteal artery tethered posteriorly
- Gastrocnemius causes Extension (Recurvatum)
Classification
- Type A: Extra-articular → Nail or Plate
- Type B: Partial articular → Screws
- Type C: Complete articular → Plate
- Hoffa: Coronal shear (Lateral more common than Medial)
Surgical Rules
- Reconstruct articular block first (anatomical)
- Attach block to shaft (functional alignment)
- Bridge plating for length/rotation
- Compression for articular surface
Implants
- Retrograde Nail: Load sharing, Early WB
- Lateral Locking Plate: Fixed angle, Buttress
- Dual Plate: For medial comminution
- DFR: For elderly/salvage
Complications
- Non-union (Medial instability)
- Malunion (Varus/Recurvatum)
- Infection (Open fracture)
- Knee Stiffness
Key Studies
- Nork 2005: 38% of 33-C have a coronal (Hoffa) fracture - CT mandatory
- Aggarwal 2022 meta-analysis: nail fewer non-unions/infections, plate better ROM
- Sanders 1991: dual plating for deficient medial buttress
- Hoellwarth 2018: DFR vs plating - equivalent mortality (periprosthetic)