Bicolumnar Concept | Anatomic Reduction Essential | ORIF vs TEA
- Bicolumnar anatomy - triangular architecture must be reconstructed
- Anatomic articular reduction is critical for good outcomes
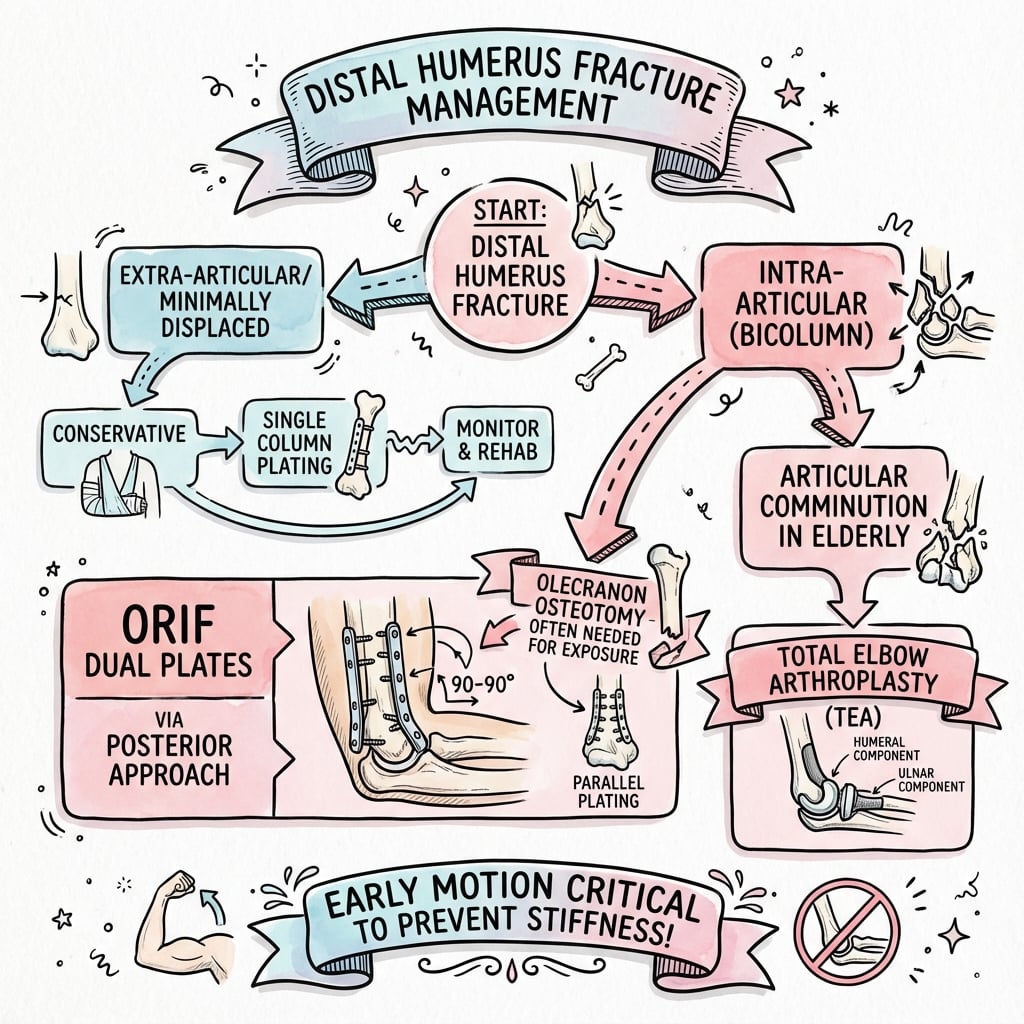
- Dual plate fixation (90-90 or parallel) is standard for Type C fractures
- Olecranon osteotomy provides best articular visualization
- Total elbow arthroplasty is an option in elderly, low-demand patients with comminution
- “Columns form an inverted triangle - both must be stabilized
- “Articular step more than 2mm increases arthritis risk significantly
- “Ulnar nerve transposition is routine with medial plating
- “TEA contraindicated in young active patients - reserved for elderly
Distal humerus forms an inverted triangle with medial and lateral columns supporting the trochlea. Both columns must be stabilized to restore the triangular arch for stable elbow function.
Olecranon osteotomy provides best visualization of articular surface. Alternatives: triceps-splitting, paratricipital (Bryan-Morrey), TRAP. Choice depends on fracture pattern and soft tissue.
90-90 plating (posterolateral and medial) or parallel plating (both posterior). Both biomechanically sound. 90-90 may reduce hardware conflict. Minimum 2 screws per column.
Total Elbow Arthroplasty indicated in elderly (age 65 plus), low-demand patients with significant comminution. Contraindicated in young, active patients. Lifetime lifting restriction 5kg.
- Key Points
- Bimodal: young males (high energy) and elderly females (low energy)
- Key Points
- C3 most challenging: comminuted articular and metaphyseal
- Key Points
- Both columns must be fixed to shaft for stability
- Key Points
- Alternatives: triceps-splitting, paratricipital, TRAP
- Key Points
- Minimum 2 screws per column into shaft, interdigitate distally
- Key Points
- Lifetime 5kg lifting restriction - contraindicated in young active patients
- Key Points
- Ulnar neuropathy (10-15%), heterotopic ossification (5-15%), nonunion (2-10%)
- Key Points
- TEA: similar outcomes to ORIF in elderly but with activity restrictions
COLUMNSCOLUMNS - Bicolumnar Fixation Principles
Hook:COLUMNS reminds you to stabilize both columns for stable elbow reconstruction
TRAPTRAP - Triceps-Reflecting Approach
Hook:TRAP approach reflects triceps with anconeus - continuous sleeve, avoids osteotomy
TEATEA - Arthroplasty Indications
Hook:TEA for elderly patients, extensive damage, with low activity
9090-90 vs PARALLEL
Hook:Both configurations work - 90-90 reduces hardware conflict, parallel may be stronger distally
Overview and Epidemiology
Distal humerus fractures are challenging injuries requiring meticulous surgical technique for optimal outcomes. They represent a significant proportion of elbow fractures and have complex anatomy requiring reconstruction.
- Young males (20-40): High-energy trauma (MVA, falls from height, sports)
- Elderly females (age 65 plus): Low-energy falls, osteoporotic bone
- Fall directly onto elbow (most common)
- Fall on outstretched hand with elbow flexed
- High-energy direct trauma
- Sports injuries (football, rugby)
In elderly patients with osteoporotic bone, achieving stable fixation is challenging. The "bag of bones" concept of conservative treatment has largely been replaced by ORIF or primary TEA for better functional outcomes.
Anatomy and Pathophysiology
Bicolumnar anatomy:
The distal humerus forms an inverted triangle:
- Medial column: Supports medial trochlear ridge
- Lateral column: Supports capitellum and lateral trochlea
- Apex: Confluence of columns at metaphysis
- Base: Articular surface (trochlea plus capitellum)
The medial and lateral columns form a triangular arch that supports the articular surface. Surgical reconstruction must restore this architecture. Both columns must be independently fixed to the shaft for stability.
- Trochlea: Articulates with ulna, spool-shaped
- Capitellum: Articulates with radial head, hemispherical
- Coronoid fossa: Accommodates coronoid in flexion
- Olecranon fossa: Accommodates olecranon in extension
- Thin central bone: Very thin bone between fossae
- Carrying angle: 10-15 degrees valgus (arm extended, palm forward)
- Baumann angle: 70-80 degrees (angle of capitellum to humeral shaft)
- Anterior humeral line: Passes through middle third of capitellum
The ulnar nerve passes posterior to the medial epicondyle in the cubital tunnel. It is at risk during surgical exposure and with medial plate placement. Most surgeons perform anterior subcutaneous transposition as part of medial plating.
Other structures:
- Radial nerve: Travels in spiral groove, passes anterior at lateral column level
- Brachial artery: Anterior to joint, at risk with anterior approaches
- Median nerve: Travels with brachial artery
Classification Systems
AO/OTA Classification (standard)
- Description
- Extra-articular
- Pattern
- Supracondylar
- Description
- Apophyseal avulsion
- Pattern
- Epicondyle fracture
- Description
- Simple metaphyseal
- Pattern
- Transverse or oblique
- Description
- Multifragmentary metaphyseal
- Pattern
- Comminuted supracondylar
- Description
- Partial articular
- Pattern
- Unicondylar
- Description
- Lateral sagittal
- Pattern
- Lateral condyle
- Description
- Medial sagittal
- Pattern
- Medial condyle
- Description
- Coronal (capitellar/trochlear)
- Pattern
- Shear fractures
- Description
- Complete articular
- Pattern
- Bicolumnar
- Description
- Simple articular, simple metaphyseal
- Pattern
- T or Y pattern
- Description
- Simple articular, comminuted metaphyseal
- Pattern
- Articular simple, column comminution
- Description
- Comminuted articular and metaphyseal
- Pattern
- Most complex
Type C fractures are the most common pattern requiring surgical reconstruction. The articular block is separated from both columns, requiring reconstruction of the joint and stable fixation to the shaft.
13-ABCAO Distal Humerus Classification
Hook:13-ABC: A=Away, B=Bit, C=Complete - simple way to remember AO classification!
Clinical Presentation and Assessment
History:
- Mechanism (fall, direct trauma, high vs low energy)
- Age and activity level
- Hand dominance
- Pre-injury function and comorbidities
- Occupation (implications for TEA consideration)
Physical examination:
- Significance
- Fracture confirmed
- Action
- Splint, ice, elevate
- Significance
- Impending open fracture
- Action
- Urgent reduction, consider early surgery
- Significance
- Open fracture
- Action
- Antibiotics, debridement, staged treatment
- Significance
- Nerve injury (15-20%)
- Action
- Document, monitor, consider early exploration
- Significance
- Vascular injury
- Action
- Urgent reduction, angiography
- Significance
- Impending compartment syndrome
- Action
- Urgent fasciotomies
Neurovascular examination:
- Ulnar nerve: sensation little finger, FDI strength, Froment sign
- Radial nerve: wrist/finger extension, sensation dorsal first web
- Median nerve: sensation thumb/index, thenar strength
- Brachial artery pulse, capillary refill
Pre-operative ulnar nerve injury occurs in 15-20% of distal humerus fractures. Document carefully before surgery. Most are neurapraxia and recover. Persistent or worsening symptoms may require exploration.
Associated injuries:
- Ipsilateral forearm fractures (floating elbow)
- Olecranon fractures
- Proximal ulna fractures
Differential diagnosis:
- Distinguishing features
- Supracondylar tenderness, bicolumnar deformity, articular crepitus
- Key investigation
- AP/lateral plus traction views; CT for articular pattern
- Distinguishing features
- Anterior elbow pain, block to flexion, double-arc sign on lateral
- Key investigation
- CT essential - often missed on plain films
- Distinguishing features
- Lateral tenderness, painful rotation, positive fat-pad sign
- Key investigation
- AP/lateral plus radiocapitellar view
- Distinguishing features
- Posterior tenderness, loss of active extension, palpable gap
- Key investigation
- Lateral radiograph
- Distinguishing features
- Gross instability, dislocation on imaging
- Key investigation
- CT plus stress views
- Distinguishing features
- Obvious deformity, olecranon prominent posteriorly
- Key investigation
- AP/lateral pre- and post-reduction
- Distinguishing features
- Child, extension-type deformity, anterior interosseous nerve at risk
- Key investigation
- AP/lateral - assess anterior humeral line, Baumann angle
- Distinguishing features
- Effusion with normal alignment, raised fat pad
- Key investigation
- Repeat film at 10-14 days or CT/MRI if suspicion persists
Investigations
- AP elbow - Assess column involvement, carrying angle
- Lateral elbow - Assess anterior/posterior displacement, articular involvement
- Oblique views - May help delineate fracture pattern
- AP and lateral with longitudinal traction
- Reduces overlap, better defines fracture pattern
- Useful for surgical planning
CT with 3D reconstruction is essential for surgical planning in all Type C fractures. It defines articular involvement, identifies small fragments, and helps plan fixation strategy. Do not operate without adequate imaging.
- All intra-articular fractures (Type B and C)
- Surgical planning for ORIF
- Coronal shear fractures (capitellar/trochlear)
- Comminuted patterns
- Rarely indicated acutely
- May be useful for soft tissue assessment in delayed presentations
Management Algorithm
- Patient Factors
- Any age
- Treatment
- Posterior plating, no osteotomy needed
- Patient Factors
- Any age
- Treatment
- Lag screws plus or minus buttress plate
- Patient Factors
- Young, active, good bone
- Treatment
- Dual plate ORIF via olecranon osteotomy
- Patient Factors
- Young patient
- Treatment
- Dual plate ORIF - accept some complexity
- Patient Factors
- Elderly (age 65 plus), low demand
- Treatment
- Consider primary TEA
- Patient Factors
- Any patient
- Treatment
- Staged: debridement, spanning ex-fix, then definitive
The topic notes the "bag of bones" approach has been "largely replaced," but a complete answer recognises it still has a defined, legitimate place - and examiners probe whether you will operate on everyone:
- What it is: deliberate non-operative management of a comminuted distal humerus fracture - a brief period of immobilisation followed by early active motion, accepting that the elbow may heal as a malunion or a painless, mobile fibrous pseudarthrosis ("functional flail" elbow) rather than an anatomically reduced joint.
- Who it is for now: the frail, very elderly, non-ambulatory or severely demented patient, or one medically unfit for the prolonged anaesthesia of a complex ORIF/TEA - patients in whom the morbidity of surgery outweighs the functional gain, especially if the arm is mainly a "helper" or used with a frame/wheelchair.
- Why consider it: it avoids the substantial wound, infection and hardware complications of operating on osteoporotic comminution in a fragile patient; surprisingly acceptable functional outcomes and good pain relief are reported when early motion is allowed, because even a lax elbow can be functional for low demands.
- The trade-off: expect reduced strength, some instability and deformity; it is a demand-matched compromise, not a reconstruction - so reserve it for the genuinely high-risk-for-surgery patient and counsel accordingly. For the fit elderly with an unreconstructable joint, primary TEA remains the better functional option.
Exam point: don't reflexively operate on every distal humerus fracture - in the frail, low-demand or medically unfit patient, non-operative ("bag of bones") treatment with early motion is a legitimate, morbidity-sparing choice that can yield a functional (if lax) elbow.
Surgical Technique
Olecranon Osteotomy - gold standard for Type C fractures
- Posterior midline incision
- Identify and protect ulnar nerve
- Chevron or transverse osteotomy 2cm from tip
- Predrill for later tension band or plate fixation
- Reflect olecranon proximally with triceps attached
- Provides excellent articular visualization
Direct posterior split - adequate for Type A, limited articular view.
Elevate triceps off columns - maintains continuity, limited articular view.
Triceps-anconeus pedicle flap - maintains blood supply, avoids osteotomy.
The osteotomy is typically fixed with tension band wire or plate fixation. Plate fixation may have lower hardware removal rates. Pre-drilling before osteotomy ensures accurate reduction.


A favourite operative-technique question: even a perfectly reduced, solidly fixed distal humerus can be mechanically blocked if hardware intrudes into the olecranon and coronoid/radial fossae - the thin "bare area" between the columns where the olecranon (in extension) and the coronoid and radial head (in flexion) must seat:
- Posterior - olecranon fossa: a screw tip or a plate contoured too distally that crosses the olecranon fossa blocks terminal extension (the olecranon hits hardware) - and intra-articular screws into the trochlear notch cause pain/arthrosis.
- Anterior - coronoid and radial fossae: hardware or a too-long screw filling these fossae blocks flexion (the coronoid/radial head cannot seat).
- How to avoid it: contour plates to the supracondylar ridges and stop short of the fossae; choose distal screw lengths and trajectories that pass between/around the fossae (the interdigitating articular screws should run within the bone of the columns/trochlea, not across the empty fossae); and check a full flexion-extension arc and orthogonal fluoroscopy intra-operatively before closing - if there is a mechanical block, reposition the offending screw.
- Why it matters: this is a mechanical (hardware) cause of stiffness that is distinct from capsular/HO stiffness and is fully preventable - and it is a common reason an early arc is lost despite "good" fixation.
Exam point: distal-humerus stiffness is not only soft-tissue - screws or plate in the olecranon, coronoid or radial fossae mechanically block the arc; keep hardware out of the fossae and test the full arc under fluoroscopy before closure.
Complications
- Incidence
- 15-50%
- Prevention/Management
- Early motion, stable fixation, CPM
- Incidence
- 10-15%
- Prevention/Management
- Anterior transposition, careful handling
- Incidence
- 5-15%
- Prevention/Management
- Prophylaxis (indomethacin or XRT), early motion
- Incidence
- 2-10%
- Prevention/Management
- Stable fixation, bone graft if needed
- Incidence
- 3-5%
- Prevention/Management
- Adequate fixation, protected loading
- Incidence
- 1-3%
- Prevention/Management
- Prophylactic antibiotics, good soft tissue handling
- Incidence
- 5-10%
- Prevention/Management
- Adequate fixation, consider plate over TBW
- Incidence
- 10-20%
- Prevention/Management
- Anatomic reduction, minimize step-off
Stiffness:
- Most common complication
- Goal: functional arc 30-130 degrees
- Prevention: stable fixation allowing early motion
- Treatment: physiotherapy, dynamic splinting, arthroscopic or open release
The functional arc for most activities of daily living is 30-130 degrees flexion and 50 degrees pronation-supination. This is the minimum acceptable outcome. Patients should be counseled that some stiffness is expected.
- Transposition is routine with medial plating
- New symptoms may develop post-operatively
- Most neurapraxias recover over 6-12 months
- Persistent symptoms may require revision transposition
- More common with delayed surgery, head injury, severe trauma
- Prophylaxis: indomethacin 75mg/day for 2 weeks or single-dose XRT
- May require excision if limiting motion (wait 12 plus months)
Postoperative Care and Rehabilitation
Post-ORIF protocol:
- Posterior splint at 90 degrees
- Elevation, ice
- Wound check at 48 hours
- Gentle finger motion
- Remove splint for supervised motion
- Begin active assisted ROM
- Focus on flexion-extension first
- Continue finger and wrist motion
- Progressive active ROM
- Night splinting if developing flexion contracture
- Dynamic splinting if significant stiffness
- No resistive exercises
- Begin gentle strengthening
- Progressive loading as tolerated
- Continue ROM exercises
- Full strengthening
- Return to most activities
- Heavy lifting/sport when healed
Key rehabilitation principles:
- Stable fixation is essential for early motion
- Continuous passive motion (CPM) may be helpful
- Balance between motion and healing
- Patient education about expected stiffness
- Long-term therapy often required
The goal is early motion to prevent stiffness. Stable fixation that allows early ROM produces better outcomes than rigid immobilization. If fixation is not stable enough for motion, it is not adequate.
Outcomes and Prognosis
Expected outcomes by treatment:
- Good/Excellent Outcomes
- 90-95%
- Key Points
- Anatomic reduction, early motion
- Good/Excellent Outcomes
- 75-85%
- Key Points
- More stiffness, higher complication rate
- Good/Excellent Outcomes
- 85-90%
- Key Points
- Reliable pain relief, restrictions required
- Good/Excellent Outcomes
- 50-60%
- Key Points
- Stiffness, malunion, poor function
Prognostic factors:
- Patient age and bone quality
- Fracture complexity (C3 worse than C1)
- Quality of reduction (articular step-off)
- Adequacy of fixation
- Associated injuries
- Compliance with rehabilitation
In comparable elderly populations, ORIF and TEA produce similar functional outcomes at 2 years. ORIF has higher re-operation rates for hardware issues. TEA has lifetime restrictions but reliable pain relief. Patient selection is key.
Guidelines, Registries & Global Practice
Global epidemiology (PubMed-backed):
- Figure
- 5.7 per 100,000 per year
- Source
- Robinson, Edinburgh (PMID 12499966)
- Figure
- Bimodal; near-equal male:female overall
- Source
- Robinson (PMID 12499966)
- Figure
- Simple fall
- Source
- Robinson (PMID 12499966)
- Figure
- 90.6%
- Source
- Robinson (PMID 12499966)
The elderly, low-energy ("fragility") fracture is the fastest-growing subgroup worldwide as populations age, and these patients drive the ORIF-versus-TEA debate.
Guideline and consensus positions (side-by-side):
- Position on distal humeral fractures
- Anatomic articular reduction plus dual-column plate fixation (parallel or perpendicular) for displaced bicolumnar fractures; early motion
- Evidence level
- Expert consensus / technique
- Position on distal humeral fractures
- Open fractures: early IV antibiotics, combined ortho-plastics debridement, staged definitive fixation with soft-tissue cover
- Evidence level
- Consensus standard
- Position on distal humeral fractures
- Operative fixation for displaced/articular fractures; primary TEA reserved for selected elderly with unreconstructable comminution
- Evidence level
- Limited / consensus
- Position on distal humeral fractures
- Supports shared decision-making between ORIF and TEA in the elderly; distal humeral hemiarthroplasty considered investigational
- Evidence level
- Consensus
No single high-level society guideline mandates ORIF versus TEA; the McKee RCT (PMID 18823799) remains the anchor evidence and all guidance is consistent with selective primary TEA.
Registry evidence:
- Finding
- TEA survival 92% / 81% / 71% / 61% at 5/10/15/20 years
- Source
- Krukhaug (PMID 29332662)
- Finding
- Post-traumatic sequelae and uncemented ulnar fixation are the main revision risks
- Source
- Krukhaug (PMID 29332662)
National joint registries (Norwegian Arthroplasty Register, AOANJRR, UK NJR) consistently show elbow arthroplasty durability below that of hip and knee replacement, which underpins the lifelong activity restriction and the avoidance of TEA in younger, higher-demand patients.
Practice variation:
- High-volume elbow/upper-limb units perform more primary TEA and more complex C3 reconstructions; smaller units more often transfer or default to ORIF.
- Parallel-plate use is more common in North American practice, perpendicular (90-90) in parts of Europe and Asia; functional outcomes are equivalent (TRON study, PMID 36527504), with the main difference being symptomatic hardware removal.
- In ageing health systems worldwide, the rising fragility-fracture burden is increasing demand for both ORIF and selective primary TEA; national registries including the AOANJRR track elbow arthroplasty outcomes.
Be ready to argue ORIF versus TEA with their indications, contraindications and the supporting evidence (McKee RCT, Norwegian Register). Show you can apply the same principles across health systems rather than quoting any single national tariff.
MCQ Practice Points
Q: What is the bicolumnar concept in distal humerus fractures? A: The distal humerus forms an inverted triangular architecture with medial and lateral columns that support the articular surface (trochlea and capitellum). Both columns must be reconstructed and fixed to the shaft for stable elbow function.
Q: Which surgical approach provides the best visualization of the distal humerus articular surface? A: Chevron olecranon osteotomy. This elevates the olecranon with the triceps attached, providing direct visualization of the entire articular surface. Alternative approaches (triceps-splitting, paratricipital) have limited articular visualization.
Q: In 90-90 plating of the distal humerus, where are the plates positioned? A: Medial plate on the medial column and posterolateral plate on the lateral column, positioned approximately 90 degrees apart. Alternative is parallel plating with both plates on the posterior surface.
Q: What are the indications for primary TEA in distal humerus fractures? A: Age 65 plus years, low-demand patient, severe articular comminution (C3 pattern) that cannot be reconstructed, and pre-existing arthritis (especially rheumatoid). Contraindicated in young, active patients.
Q: What is the most common complication following distal humerus fracture fixation? A: Elbow stiffness (15-50%). The goal is to achieve a functional arc of 30-130 degrees. Prevention includes stable fixation allowing early motion and appropriate physiotherapy.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old right-hand dominant carpenter falls from a ladder, landing on his elbow. X-rays show a Type C2 distal humerus fracture (simple articular, comminuted metaphysis). The ulnar nerve is intact. Describe your management.”
“A 78-year-old woman with osteoporosis and rheumatoid arthritis falls at home. CT shows a Type C3 distal humerus fracture with severe articular comminution. She lives alone but is independent. What are your treatment options?”
“A 35-year-old male motorcyclist has a Type C3 distal humerus fracture with severe soft tissue injury and skin loss posteriorly. The wound is contaminated. The hand is well perfused but he has ulnar nerve palsy. How do you manage this?”
BICOLUMNAR CONCEPT
- Inverted triangular architecture
- Medial column plus lateral column support articular surface
- Both columns must be fixed to shaft for stability
- Interdigitating screws in articular block
CLASSIFICATION
- AO Type A: extra-articular (supracondylar)
- AO Type B: partial articular (unicondylar)
- AO Type C: complete articular (bicolumnar)
- C3 equals comminuted articular and metaphyseal equals most challenging
SURGICAL APPROACHES
- Olecranon osteotomy: best articular visualization (gold standard)
- Triceps-splitting: simple patterns, limited view
- Paratricipital: TEA, some ORIF, no osteotomy
- TRAP: TEA, preserves triceps blood supply
PLATE CONFIGURATION
- 90-90: medial plus posterolateral plates (90 degrees apart)
- Parallel: both plates posterior surface
- Both configurations acceptable
- Minimum 2 screws per column into shaft
TEA INDICATIONS
- Age 65 plus (ideally age 75 plus)
- Low-demand patient
- Severe articular comminution (C3)
- Pre-existing arthritis (especially RA)
- Contraindicated in young, active patients
TRAPS AND PEARLS
- Always get CT for surgical planning
- Ulnar nerve transposition is routine with medial plating
- Early motion is essential to prevent stiffness
- Functional arc: 30-130 degrees flexion
- TEA requires lifetime 5kg lifting restriction
Evidence Base
- Multicentre RCT (42 patients randomised) comparing ORIF with primary semiconstrained TEA in patients older than 65 with displaced OTA 13C fractures
- TEA had significantly better Mayo Elbow Performance Score at 2 years (86 vs 73, p=0.015) and faster early DASH recovery
- 5 of 21 patients randomised to ORIF (24%) were converted to TEA intra-operatively because fixation could not be achieved
- Reoperation rates (TEA 12% vs ORIF 27%) were not statistically different (p=0.2)
- Describes the parallel-plate (both columns plated medially and laterally) principle-based approach to distal humeral fixation
- Distal screws should be as long as possible, pass through plates, engage as many articular fragments as possible, and interdigitate to lock the columns together
- Each screw should pass through a plate and engage a fragment on the opposite side that is also fixed to a plate
- Stability is sufficient to permit immediate intensive rehabilitation, with bone graft rarely required
- Retrospective comparison of 39 transolecranon exposures fixed with double screws versus tension-band wiring (TBW) for complex distal humeral fractures
- Significantly fewer all-cause revisions with double screws than with TBW (3/14 versus 14/25, p=0.049)
- Symptomatic implant removal was the commonest reason for revision and was more frequent after TBW
- Olecranon nonunion occurred only in the TBW group (4/25 versus 0/14)
- Multicentre study of 383 distal humeral fractures, propensity-matched to 50 perpendicular versus 50 parallel double-plate cases
- No significant difference in Mayo Elbow Performance Score at any time point between the two plate configurations
- Implant removal was significantly more frequent after parallel plating (50% versus 26.5%, p=0.023)
- Medial-lateral parallel plates lie under thin subcutaneous tissue, increasing symptomatic prominence
- Defined that apparent isolated capitellar fractures are often complex multi-fragment articular injuries with up to five components (capitellum-lateral trochlea, lateral epicondyle, posterior lateral column, posterior trochlea, medial epicondyle)
- All 21 fractures healed after open reduction and fixation with implants buried beneath the articular surface
- Mayo Elbow Performance Index excellent or good in 16 of 21; mean ulnohumeral arc 96 degrees
- Ten patients required a second operation, most commonly for contracture release
- Consecutive series of 320 adult distal humeral fractures from a defined catchment population; incidence 5.7 per 100,000 per year
- Bimodal age distribution with an almost equal male-to-female ratio; simple falls were the commonest mechanism overall
- Most fractures were extra-articular (OTA type A) or complete articular (OTA type C); 90.6% united within 12 weeks
- Union complications were higher after high-energy injury, open fractures and nonoperative treatment
- 838 primary total elbow arthroplasties reported to the Norwegian Arthroplasty Register 1994-2016
- Implant survival 92% at 5 years, 81% at 10 years, 71% at 15 years and 61% at 20 years
- A diagnosis of post-traumatic sequelae and uncemented ulnar fixation were the main risk factors for revision
- Aseptic loosening was the commonest revision cause; survivorship was poorer than for hip and knee arthroplasty