Direct, Capacitive and Inductive (PEMF) Coupling
- The rationale is that BONE is PIEZOELECTRIC: mechanical loading generates electrical STRESS-GENERATED POTENTIALS, with the CONCAVE (compression) surface becoming ELECTRONEGATIVE (associated with bone FORMATION) and the convex (tension) surface electropositive (resorption) - so applying an electrical/electromagnetic stimulus aims to mimic this and promote osteogenesis.
- There are THREE modalities of bone-growth stimulation. DIRECT CURRENT (DC) is INVASIVE: an electrode is implanted with the CATHODE at the fracture/fusion site, delivering a constant current that creates a local electronegative, low-oxygen, osteogenic environment. CAPACITIVE COUPLING (CC) is NON-INVASIVE: external skin electrodes (capacitor plates) on either side of the limb create an electric field across the bone. INDUCTIVE COUPLING / PULSED ELECTROMAGNETIC FIELD (PEMF) is NON-INVASIVE: an external coil generates a time-varying magnetic field that INDUCES an electric field in the tissue (Faraday's law), including combined-magnetic-field (CMF) devices.
- Only devices with SPECIFIC physical wave characteristics (pulse shape, frequency, amplitude) and an adequate daily EXPOSURE TIME are effective - it is not a generic effect - so the device parameters and patient COMPLIANCE (often hours per day for months) matter.
- At the cellular level, electrical/electromagnetic stimulation modulates calcium signalling and upregulates osteogenic growth factors (e.g. BMP, TGF-beta), osteoblast activity and angiogenesis, promoting bone formation across the fracture.
- INDICATIONS are mainly as an ADJUNCT in problem healing: established NON-UNIONS (the principal use), DELAYED unions, fractures at high non-union risk, as an adjunct to SPINAL FUSION (especially revision/high-risk), STRESS fractures, and early OSTEONECROSIS; reported union rates for non-union are in the order of ~80% in case series, but it does NOT replace adequate reduction, mechanical STABILITY and biology.
- It is generally SAFE and non-invasive (for CC/PEMF), avoiding the risks/costs of surgery, but the EVIDENCE is mixed and device-specific, it requires sustained patient compliance, and it will NOT heal a fracture that has a large gap, gross instability, an established synovial pseudarthrosis or interposed soft tissue - those need surgery; caution is advised with pacemakers/implanted electronic devices and in pregnancy.
- “Bone is piezoelectric: concave/compression side electronegative -> bone formation (the rationale).
- “Three modalities: Direct current (INVASIVE cathode), Capacitive coupling (external electrodes), Inductive coupling/PEMF (external coil, Faraday induction). CC and PEMF are non-invasive.
- “Main indication = NON-UNION (adjunct, ~80% union in series); also delayed union, fusion adjunct, osteonecrosis. Device-specific + compliance-dependent; not a substitute for stability/reduction/biology.
Implanted cathode at the fracture/fusion site -> local electronegative osteogenic environment. Used for non-union and spinal fusion.
Capacitive coupling (external skin electrodes) and inductive coupling/PEMF (external coil inducing current) - worn externally; rely on patient compliance.
Rationale & Mechanism
Bone generates electrical potentials when mechanically loaded - it is piezoelectric, producing stress-generated (streaming) potentials. The concave (compression) surface becomes ELECTRONEGATIVE, which is associated with bone formation, while the convex (tension) surface is electropositive and associated with resorption - an electrical correlate of Wolff's law. Electrical and electromagnetic stimulation aim to mimic this, creating an osteogenic environment that modulates calcium signalling and upregulates osteogenic growth factors (BMP, TGF-beta), osteoblast activity and angiogenesis, thereby promoting bone formation across a fracture or fusion. Only devices with specific waveforms and adequate daily exposure achieve this.
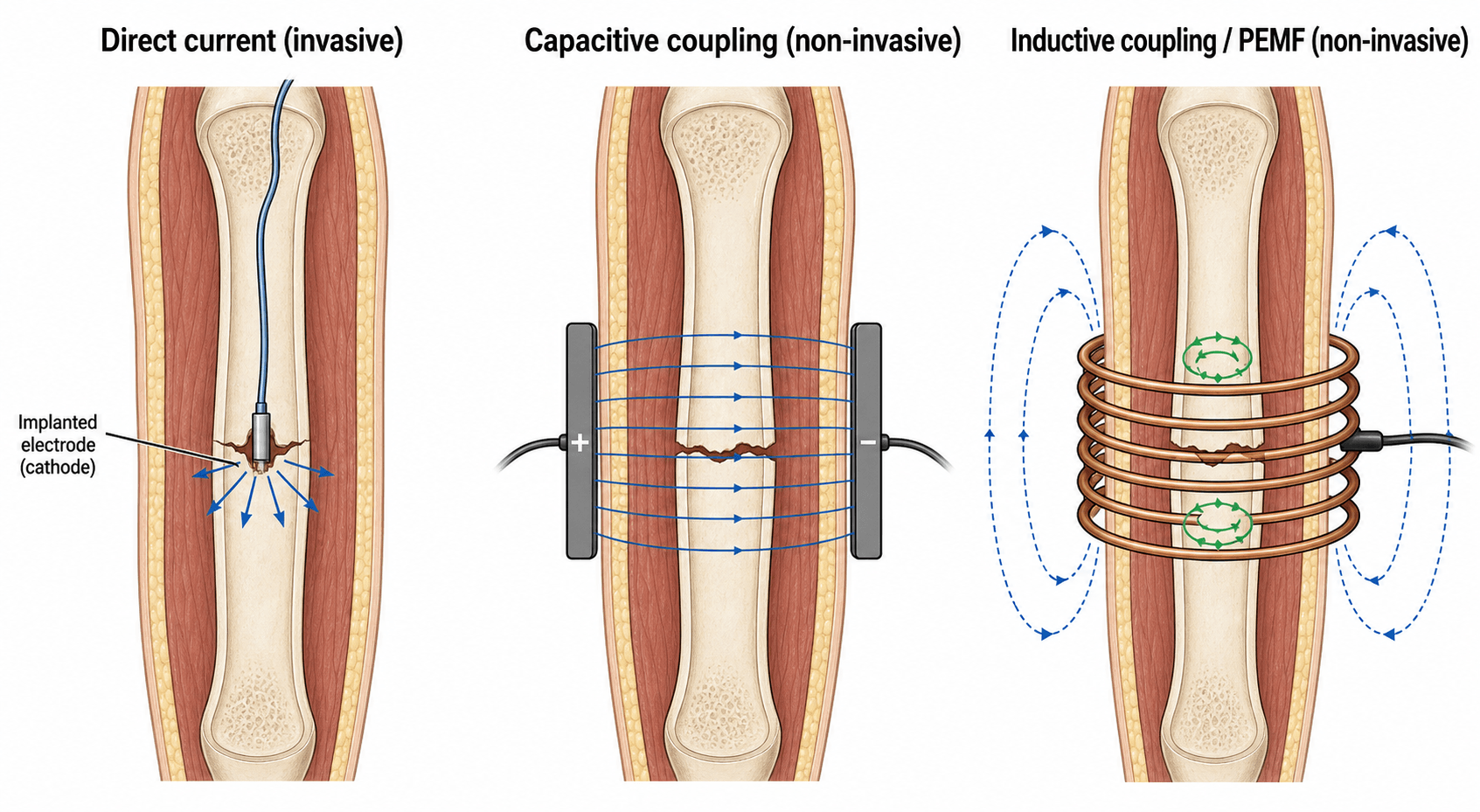
The Three Modalities
- Direct current (DC) - INVASIVE: an electrode is implanted with the cathode at the fracture or fusion site, delivering a constant current; the cathode creates an electronegative, relatively hypoxic, osteogenic microenvironment. Used for established non-unions and as a spinal-fusion adjunct.
- Capacitive coupling (CC) - NON-INVASIVE: two external skin electrodes (capacitor plates) are placed on opposite sides of the limb and connected to a generator, creating an electric field across the fracture.
- Inductive coupling / PEMF - NON-INVASIVE: an external coil placed around the limb produces a time-varying magnetic field that, by Faraday's law, induces an electric field/current within the bone; combined magnetic field (CMF) is a related device. The non-invasive devices are worn for several hours daily over weeks-to-months, so compliance is essential.
- Invasive?
- Yes (implanted cathode)
- How it works
- Constant current -> electronegative osteogenic environment
- Invasive?
- No (skin electrodes)
- How it works
- Electric field across the fracture
- Invasive?
- No (external coil)
- How it works
- Magnetic field induces current (Faraday's law)
The Biophysics: Streaming Potentials and the Osteogenic Cathode
- Stress-generated potentials have two origins. Classical piezoelectricity is a property of the oriented collagen-apatite lattice - deforming the crystal generates charge, and it is demonstrable even in dry bone. Streaming potentials are the dominant mechanism in wet/living bone: load drives interstitial fluid through the canalicular network, and the moving charged ions stream past the negatively-charged bone matrix, generating a potential (the same fluid shear is sensed by osteocytes - the cellular mechanotransduction is developed in our Osteocytes & Mechanotransduction topic). Both make the loaded/concave/compression surface electronegative and osteogenic.
- Why the implanted cathode is osteogenic (the electrochemistry). At the cathode, electrochemical reduction consumes local oxygen (lowering oxygen tension), generates hydroxyl ions (raising pH toward alkaline) and produces hydrogen peroxide - a low-oxygen, alkaline, electronegative microenvironment that favours osteoblastic bone formation and, via peroxide-driven VEGF/angiogenesis, new vessels. This is exactly the "electronegative, relatively hypoxic, osteogenic" niche the topic describes, and it is why the cathode (not the anode) is placed at the fracture.
Two mechanisms behind "stress-generated potentials": piezoelectricity (collagen-apatite lattice, present in dry bone) and streaming potentials (charged fluid moving through wet bone - the dominant, physiological one). At the implanted cathode, oxygen is consumed and pH rises (low-oxygen, alkaline, electronegative) → osteogenic
- so the cathode goes at the fracture.
Choosing the Right Non-union: Where Stimulation Fits
- Good candidate (stimulate): a non-union that is aligned, with stable fixation / no gross motion, a small or no gap, no infection, no established synovial (true) pseudarthrosis and no interposed soft tissue - i.e. the mechanics are adequate and the biology just needs a nudge - in a patient who can comply with hours-per-day wear for months.
- Poor candidate (operate instead): an atrophic non-union with poor biology needing graft, gross instability / inadequate fixation, a large gap or bone loss, a deformity needing correction, infection (needs debridement), an established synovial pseudarthrosis, or interposed soft tissue - these need surgery to fix the deficient element.
- The "diamond concept" frame: healing needs mechanical stability + an osteoconductive scaffold + osteogenic cells + osteoinductive growth factors (with host vascularity). Electrical stimulation - like LIPUS - addresses mainly the biological/osteoinductive vertex; it cannot substitute for a missing mechanical vertex or for absent scaffold/cells, so correct the deficient vertex (revision fixation, grafting) rather than relying on a stimulator alone. (Non-union classification/management is developed in our Nonunion Management topic, and the ultrasound adjunct in our LIPUS topic.)
Stimulate the non-union whose mechanics are already adequate (aligned, stable, small gap, no infection, no synovial pseudarthrosis) and whose biology just needs a nudge; operate when a vertex of the diamond concept is missing (instability, large gap, atrophic biology, infection). Electrical stimulation and LIPUS feed the biological vertex only - they do not fix mechanics.
Mnemonics & Memory Aids
DCI
Hook:Three modalities = DCI: Direct (invasive), Capacitive, Inductive.
NEGATIVE
Hook:Think 'NEGATIVE': the electronegative environment drives bone formation.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is the rationale for electrical stimulation of bone, and what are the modalities available?”
“When would you use bone-growth stimulation, and what are its limitations?”
Rationale
- Bone is piezoelectric -> stress-generated potentials
- Concave/compression side electronegative -> bone formation
- Stimulation modulates calcium/growth factors (BMP, TGF-beta)/osteoblasts
Modalities
- Direct current (DC): INVASIVE implanted cathode at fracture/fusion
- Capacitive coupling (CC): non-invasive external electrodes (electric field)
- Inductive coupling / PEMF (CMF): non-invasive external coil (Faraday induction)
Indications
- Non-union (main), delayed union, high-risk fractures
- Spinal fusion adjunct, stress fractures, early osteonecrosis
- Non-union union rates ~80% in series (device-specific, compliance-dependent)
Limits & cautions
- Not a substitute for reduction/stability/biology (gap/pseudarthrosis -> surgery)
- Mixed/device-specific evidence; requires sustained compliance
- Caution: pacemakers/implanted devices, pregnancy
Indications, Evidence & Limits
- Indications: principally established NON-UNIONS, plus delayed unions, fractures at high non-union risk, an adjunct to spinal fusion (especially revision/high-risk), stress fractures, and early osteonecrosis.
- Evidence: supportive in non-union series (union rates around 80%), and it avoids the risks and costs of surgery; but the literature is mixed, the effect is device-specific (only certain waveforms work), and it depends on sustained patient compliance.
- It does NOT replace the fundamentals: adequate reduction, mechanical stability and biology - a large gap, gross instability, interposed soft tissue or an established synovial pseudarthrosis needs surgery, not a stimulator.
- Cautions: care with pacemakers/implanted electronic devices and in pregnancy; ensure correct device selection and application.
Evidence & Key Studies
Biophysical stimulation with PEMFs in fracture healing: from bench to bedside
- Pulsed electromagnetic field (PEMF) therapy promotes fracture repair, but only devices with specific physical wave features (pulse shape, frequency, amplitude) are effective.
- Preclinical studies defined a dose-response relationship and the minimum exposure time required.
- PEMFs are used for acute fractures at non-union risk, non-unions, osteotomies, stress fractures and osteonecrosis.
Outcomes of fracture non-union treated with combined magnetic field bone growth stimulation
- In 25 evaluable patients with established fracture non-union treated with a combined magnetic field bone-growth stimulator, the union rate was 84% with a mean time to union of 6.6 months.
- Combined magnetic field stimulation is a viable non-operative option for established non-union, avoiding the risks/costs of surgery.
- The authors note that larger studies are needed to define efficacy conclusively.
The device-specific efficacy of PEMF (requiring particular waveforms and exposure) and its indications come from the cited Vicenti review, and the ~84% non-union union rate with combined magnetic field stimulation from the cited Sibanda series. The piezoelectric/stress-generated-potential rationale and the three modalities (direct current, capacitive coupling, inductive coupling/PEMF) are standard, well-established teaching. (See also our Bone Healing, Nonunion Management and Osteonecrosis topics.)