Diathermy Principles & Safety
- ELECTROSURGERY (diathermy) works by passing HIGH-FREQUENCY (radiofrequency) ALTERNATING CURRENT through tissue, generating HEAT where the current density is high; the effect depends on the WAVEFORM - a continuous waveform CUTS by vaporising cells, an interrupted (damped) waveform COAGULATES by desiccation, fulguration sprays current to char a surface, and BLEND combines cutting with haemostasis.
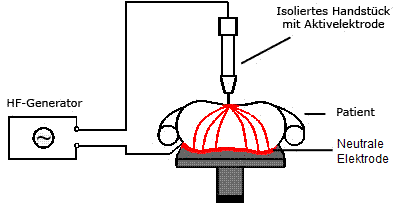
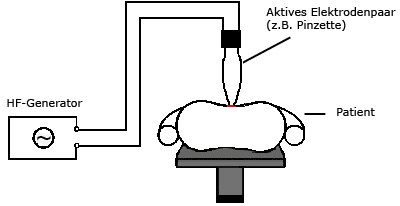
- MONOPOLAR diathermy passes current from a small ACTIVE electrode THROUGH the patient to a large RETURN (dispersive/plate) electrode: the small active tip has HIGH current density (the surgical effect) and the large return pad has LOW current density (so it does not burn) - it is versatile but depends on correct return-electrode application; BIPOLAR confines the current BETWEEN the two forceps tips, needs NO return electrode and passes NO current through the rest of the patient.
- BIPOLAR is therefore SAFER near nerves, near or on implants, in patients with pacemakers, and in DIGITS/appendages with end-arterial supply (avoiding the historic teaching against monopolar on a digit/penis), but it only coagulates a small volume; MONOPOLAR is more versatile (cut and coagulate) but carries the risks of current passing through the body.
- RETURN-ELECTRODE safety is fundamental in monopolar use: the dispersive pad must be correctly sized and applied over well-perfused muscle close to the operative site, must NOT be cut down for a child (reducing its area raises current density and risks a pad-site burn), and poor contact causes BURNS - while CURRENT DIVERSION can cause ALTERNATIVE-SITE burns (e.g. at ECG electrodes or skin contact points).
- PACEMAKER/ICD precautions matter: monopolar diathermy can interfere with cardiac implantable devices (inhibition, inappropriate shocks), so bipolar is preferred where possible, short bursts are used, the return electrode is positioned so the current path avoids the device, and the device team is involved (with magnet/programming as advised); SURGICAL FIRE (the fire triad - oxidiser, fuel, ignition source) and SURGICAL SMOKE (a respiratory/biological hazard requiring evacuation) are further safety considerations.
- THE KNOWLEDGE GAP HAS BEEN MEASURED, AND THE NUMBERS ARE THE POINT. In a surgeon survey, about 58 PERCENT scored at an unsafe level of understanding of electrosurgical devices; NEARLY HALF said they would cut a dispersive electrode down to fit a child (which raises current density at the pad and risks a burn); MOST believed the harmonic scalpel was a form of bipolar cautery when it is ULTRASONIC (mechanical vibration generating frictional heat); and A MAJORITY did not know how to handle an operating-room fire. Other gaps were the correct current mode for coagulating a vessel and where to place the dispersive electrode. This is a single questionnaire study, not a measure of actual harm, but it identifies precisely the items examiners ask - and is why structured training (the Fundamental Use of Surgical Energy, FUSE) is advocated.
- “Diathermy = high-frequency AC -> heat at high current density. Cut = continuous waveform (vaporise); coagulation = interrupted waveform (desiccate); fulguration = spray/char; blend = both.
- “MONOPOLAR = current through patient to a large RETURN (dispersive) electrode (high density at tip, low at pad). BIPOLAR = current only between forceps tips (no return electrode) - safer near nerves/implants/pacemakers and in DIGITS.
- “Safety: correct return-electrode placement (never cut it down for a child), alternative-site burns, pacemaker/ICD precautions (prefer bipolar, short bursts), surgical fire (oxidiser+fuel+ignition), surgical-smoke evacuation. Harmonic scalpel = ULTRASONIC, NOT bipolar cautery. The gap is measured, not asserted: ~58% of surveyed surgeons scored unsafe, ~half would cut a child's dispersive pad, most thought harmonic was bipolar cautery, and a majority could not manage an OR fire.
Monopolar: current through the patient to a large return/dispersive electrode (effect at the small tip). Bipolar: current only between the forceps tips - no return electrode; safer near nerves/implants/pacemakers and in digits.
Correct return-electrode placement (never cut it down for a child); alternative-site burns; pacemaker/ICD precautions (prefer bipolar); surgical fire & smoke. Harmonic = ultrasonic, not bipolar cautery.
How It Works: Waveforms, Monopolar & Bipolar
Electrosurgery passes high-frequency alternating current through tissue, producing heat where current density is high. The waveform determines the effect: a continuous waveform cuts (vaporises cells), an interrupted waveform coagulates (desiccates/seals), fulguration sprays current to char, and blend combines them. Monopolar diathermy passes current from a small active electrode through the patient to a large return (dispersive) electrode - high current density (the effect) at the tip, low density (no burn) at the pad - and is versatile but needs correct return-electrode application. Bipolar confines current between the two forceps tips, needs no return electrode, and passes no current through the rest of the patient, making it safer near nerves, implants, pacemakers and in digits, though it only coagulates a small area.
- Monopolar
- Active tip -> through patient -> return (dispersive) electrode
- Bipolar
- Between the two forceps tips only
- Monopolar
- Required (large dispersive pad)
- Bipolar
- Not required
- Monopolar
- Cut + coagulate; wide effect
- Bipolar
- Coagulation of small volume only
- Monopolar
- Higher risk (current through body)
- Bipolar
- Safer (current confined)
- Monopolar
- Traditionally avoided
- Bipolar
- Preferred (end-arterial safety)
Safety & Other Energy Devices
- Return (dispersive) electrode: correctly sized and applied over well-perfused muscle near the site; never cut it down for a child (raises current density -> burn); poor contact -> pad-site burn.
- Alternative-site burns: from current diversion (e.g. at ECG electrodes/skin contact); minimise contact points.
- Pacemaker/ICD: prefer bipolar, short bursts, position the return so the current path avoids the device, involve the device team (magnet/programming as advised).
- Surgical fire: the fire triad (oxidiser - O2; fuel - drapes/alcohol prep; ignition - diathermy) - allow alcohol prep to dry, manage oxygen, know how to handle an OR fire.
- Surgical smoke: a respiratory/biological hazard - use smoke evacuation.
- Other devices: harmonic scalpel = ultrasonic (mechanical vibration/frictional heat, NOT bipolar cautery); advanced bipolar vessel sealers; RFA and microwave ablation differ in mechanism.
Three of these have a specifically orthopaedic edge. Alcohol-based skin preparation runs downwards and pools beneath a limb, under drapes and beneath a tourniquet cuff, where it neither evaporates nor is visible, so the fuel side of the fire triad is a limb-surgery problem as much as an airway one - the prep must be allowed to dry and pooled fluid removed before the diathermy is switched on. The current path matters more in limb surgery too: in monopolar use the return electrode should sit so the path does not run along the operated limb through a tourniquet or across a metallic implant, since current concentrating at a small metal contact raises local current density. And bipolar is the sensible default when working around a nerve, an existing prosthesis or a digit, where the confined current path removes the question entirely. The related perioperative pages are tourniquet use and surgical site infection prevention.
When surgeons were surveyed on this, about 58 percent scored at an unsafe level of understanding, and the specific failures were consistent enough to predict both the theatre error and the exam question. First, devices are confused: the harmonic scalpel is an ultrasonic device that cuts and coagulates by mechanical vibration generating frictional heat - it is not a form of bipolar electrocautery - and mixing these up leads to wrong assumptions about safety near pacemakers and implants. Most of the surveyed surgeons made exactly this error. Second, the return (dispersive) electrode in monopolar surgery is frequently mishandled - nearly half said they would cut one down to fit a child - and it must be correctly sized and applied over well-perfused muscle close to the operative field, and it must never be cut down to fit a child, because reducing its surface area raises the current density and risks a pad-site burn; poor contact and current diversion likewise cause burns at the pad or at alternative sites. Third, patient factors are overlooked - monopolar diathermy can interfere with pacemakers and defibrillators, so bipolar is preferred with short bursts and a current path that avoids the device, and the surgical-fire triad (oxidiser, fuel, ignition source) and the biohazard of surgical smoke must be actively managed - and a majority of those surveyed did not know how to handle an operating-room fire. Structured training such as the Fundamental Use of Surgical Energy programme exists precisely to close these gaps. The survey is a questionnaire of knowledge, not a measure of how often patients are actually harmed; no study quantifies the incidence of diathermy burns or surgical fires in orthopaedic practice, so no such rate is given here.
Why High Frequency, and How the Heat Is Made
- The frequency and why. Diathermy uses radiofrequency alternating current, about 300 kHz to several MHz - deliberately above the roughly 100 kHz ceiling of neuromuscular and cardiac excitability. At mains frequency (50/60 Hz) the current would stimulate nerve and muscle (the Faradic effect - electrocution, arrhythmia); at radiofrequency the cell membranes cannot depolarise fast enough to follow it, so the current heats tissue without stimulating it.
- How the heat is made. Heating is resistive (Joule) heating - proportional to the square of the current density - so it concentrates at the small active electrode (high density → intense local heat) and is negligible at the large dispersive pad (low density).
- The temperature thresholds. Around 60°C proteins denature and vessels seal (coagulation); around 100°C intracellular water boils and cells explode (vaporisation/cutting); higher still, tissue chars (fulguration/eschar).
Q: What frequency does diathermy use, and why must it be high?
A: Radiofrequency alternating current, about 300 kHz to several MHz - above the roughly 100 kHz ceiling of neuromuscular/cardiac excitability. At mains 50/60 Hz the current would stimulate nerve/muscle (Faradic effect - electrocution/arrhythmia); at radiofrequency the membranes cannot follow it, so it heats without stimulating. Heat = resistive (Joule) heating (proportional to the square of the current density), concentrated at the small active tip. Thresholds: about 60°C protein denaturation/coagulation, about 100°C water boils/vaporisation-cutting.
The Energy Devices and Thermal Spread
- Ultrasonic (Harmonic). A piezoelectric transducer vibrates the blade at about 55 kHz; the mechanical friction denatures protein (coagulation, not electrical) and the vibration cuts - at a lower temperature than diathermy, with little lateral thermal spread and no electrical current through the patient (safe near pacemakers); it cuts and coagulates simultaneously and seals vessels up to about 5 mm.
- Advanced bipolar (vessel sealers, e.g. LigaSure). Feedback-controlled bipolar radiofrequency plus pressure fuses the collagen and elastin of the vessel wall into a permanent seal (vessels up to about 7 mm); the generator senses tissue impedance and stops when the seal is complete, limiting thermal spread.
- Thermal spread and ablation. Ultrasonic and advanced bipolar have the least lateral thermal spread (safest near nerves); monopolar the most. RFA and microwave ablation instead destroy a target (tumour, some bone lesions) by heat.
Q: How do the ultrasonic and advanced-bipolar energy devices work, and how do they compare on thermal spread?
A: Ultrasonic (Harmonic) = a piezoelectric blade vibrating at about 55 kHz - mechanical friction denatures protein (coagulation) and cuts, at lower temperature, little lateral thermal spread, no current through the patient (safe near pacemakers); seals vessels up to about 5 mm. Advanced bipolar (LigaSure) = feedback-controlled bipolar RF + pressure fusing collagen/elastin to seal vessels up to about 7 mm. Thermal-spread hierarchy: ultrasonic/advanced-bipolar least (safest near nerves), monopolar most. RFA/microwave = ablation of a target lesion.
Mnemonics & Memory Aids
DIATHERMY
Hook:DIATHERMY: Density, Interrupted=coag, Alternative-site burns, Two types (mono/bipolar), Harmonic=ultrasonic, Electrode (return), Rhythm devices, Make no fire/smoke, You need training.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is the difference between monopolar and bipolar diathermy, and what are the key safety issues?”
Principles
- High-frequency AC -> heat at high current density
- Cut = continuous waveform (vaporise); coagulation = interrupted (desiccate)
- Fulguration = spray/char; blend = cut + haemostasis
Monopolar vs bipolar
- Monopolar: active tip -> through patient -> large return (dispersive) electrode
- Bipolar: current only between forceps tips; no return electrode
- Bipolar safer near nerves/implants/pacemakers and in digits (small effect only)
Safety
- Return electrode over well-perfused muscle; never cut down for a child
- Alternative-site burns; pacemaker/ICD precautions (prefer bipolar, short bursts)
- Surgical fire triad (oxidiser+fuel+ignition); alcohol prep POOLS under a limb/tourniquet - let it dry
- Route the return so the current path avoids the tourniquet and any metallic implant
- Surgical-smoke evacuation
Other devices / gaps
- Harmonic scalpel = ultrasonic (NOT bipolar cautery)
- Advanced bipolar vessel sealers; RFA and microwave ablation differ in mechanism
- ~58% of surveyed surgeons scored unsafe; ~half would cut a child's pad; most thought harmonic was bipolar -> FUSE training
Evidence & Key Studies
Lack of awareness among surgeons regarding safe use of electrosurgery
- In a survey of surgeons, the majority (about 58%) had an unsafe level of understanding of electrosurgical devices; common gaps included the correct mode of current for coagulating vessels, correct placement of the dispersive (return) electrode, and identifying a safe device in patients with a pacemaker.
- Nearly half would inappropriately cut a dispersive electrode to fit a child, and most incorrectly believed the harmonic scalpel was a form of bipolar cautery; a majority did not know how to handle an operating-room fire.
- The findings highlight a high level of ignorance regarding basic electrosurgical equipment and the need for raising awareness and structured training (e.g. surgical-energy curricula).
The evidence that many surgeons have an unsafe understanding of electrosurgery - the 58 percent figure, and the specific gaps in the correct coagulation mode, dispersive (return) electrode placement, the error of cutting the dispersive electrode for a child, identifying pacemaker-safe devices, recognising that the harmonic scalpel is not bipolar cautery, and managing an operating-room fire - comes from the cited Malik survey. The underlying physics (high-frequency AC, cut vs coagulation waveforms), the monopolar/bipolar distinction, alternative-site burns, the fire triad, surgical-smoke hazards, and the ultrasonic mechanism of the harmonic scalpel and the nature of RF/ microwave devices are standard, well-established teaching (formalised in surgical-energy curricula such as FUSE). That survey measured knowledge, not harm: it does not establish how often burns or fires actually occur, and no study gives an incidence of diathermy burns, alternative-site burns or surgical fires specific to orthopaedic surgery, so no such figure is quoted. Nor is there a randomised comparison showing that any one energy device reduces blood loss, operating time or complications in orthopaedic procedures.