Non-Langerhans Cell Histiocytosis
- ERDHEIM-CHESTER DISEASE (ECD) is a RARE NON-LANGERHANS CELL HISTIOCYTOSIS - a proliferation of foamy histiocytes that are CD68-POSITIVE and CD1a/Langerin-NEGATIVE (the immunophenotype that separates it from Langerhans cell histiocytosis) - driven by MAPK-pathway mutations, with BRAF V600E in about HALF and the remainder carrying MAP2K1, NRAS/KRAS/ARAF or PIK3CA, placing it on the spectrum of clonal MYELOID neoplasms. It has a marked MALE predominance (39 men to 14 women in a 53-patient multicentre cohort).
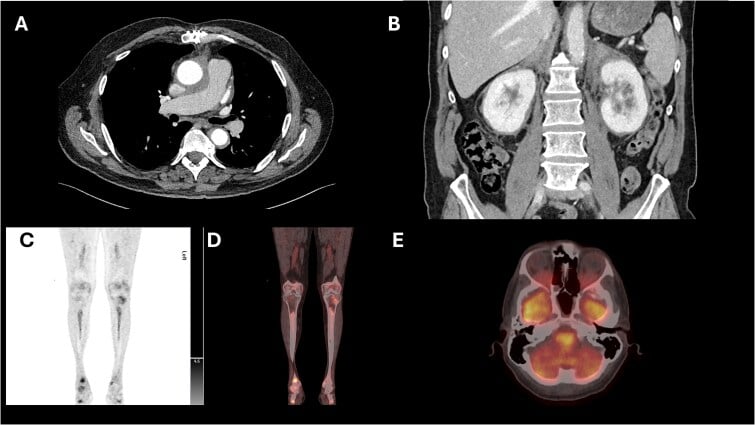
- Its SKELETAL HALLMARK is BILATERAL, SYMMETRIC OSTEOSCLEROSIS of the METADIAPHYSES of the LONG BONES, particularly the LOWER LIMBS (distal femur, proximal/distal tibia), commonly causing bone pain; a radionuclide BONE SCAN shows symmetric increased uptake in the distal long bones, a near-pathognomonic pattern that often first suggests the diagnosis to the orthopaedic surgeon/radiologist.
- ECD is a MULTISYSTEM disease, and the extraskeletal manifestations are protean and can be life-threatening: CARDIOVASCULAR (periaortic soft-tissue sheathing - the 'coated aorta' - and pericardial/myocardial infiltration), RETROPERITONEAL (perinephric infiltration - the 'hairy kidney' - with ureteric obstruction), CNS, ORBITAL (exophthalmos), PITUITARY (diabetes insipidus), cutaneous (xanthelasma) and pulmonary involvement.
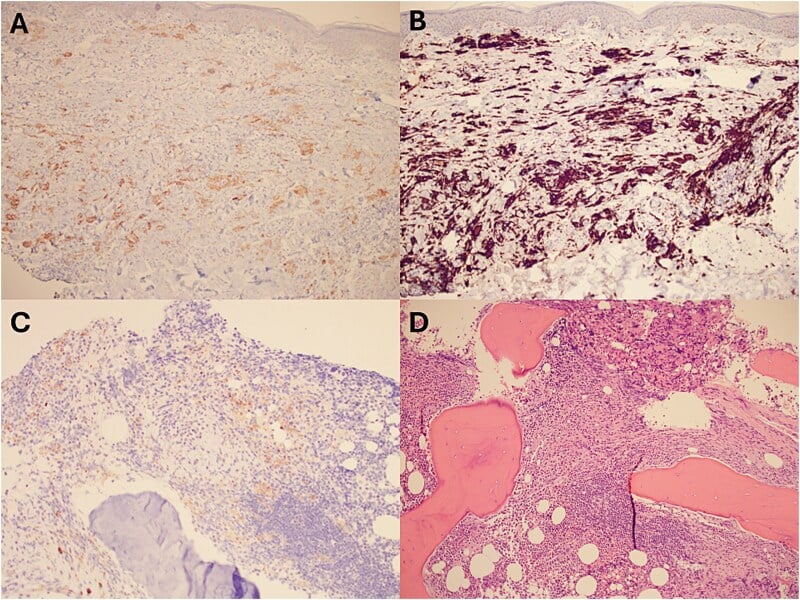
- DIAGNOSIS combines the characteristic clinical/imaging pattern with a BIOPSY showing foamy CD68+/CD1a-negative histiocytes (often with Touton giant cells and fibrosis) and MOLECULAR/BRAF testing; PET imaging is often more informative than CT/MRI in revealing the widespread FDG-avid skeletal and soft-tissue lesions, and a bone-marrow/bone biopsy can be valuable.
- PUT A NUMBER ON THE PROGNOSIS AND NAME WHAT DRIVES IT. In a 53-patient multicentre cohort with biopsy-proven ECD, CNS INVOLVEMENT was an independent predictor of DEATH (hazard ratio 2.51, 95% CI 1.28-5.52, p=0.006) - so the neurological examination and brain imaging matter more to the prognosis than the extent of the bone disease. In the same multivariate analysis, INTERFERON-ALPHA was an independent predictor of SURVIVAL (hazard ratio 0.32, 95% CI 0.14-0.70) - the first treatment ever shown to improve survival in ECD.
- It must be DISTINGUISHED from Langerhans cell histiocytosis (CD1a/Langerin-positive, lytic 'punched-out' lesions rather than symmetric sclerosis) and from other causes of osteosclerosis (osteoblastic metastases, sclerosing dysplasias, myelofibrosis, renal osteodystrophy) - the symmetric distal long-bone sclerosis with the multisystem features and immunophenotype is the key.
- MANAGEMENT has been TRANSFORMED by TARGETED THERAPY: BRAF inhibitors (e.g. vemurafenib/dabrafenib) for BRAF V600E-mutant disease, and MEK inhibitors for the MAPK pathway more broadly, can produce dramatic responses; treatment is delivered by a specialist multidisciplinary team addressing the affected organ systems - the orthopaedic role is largely RECOGNITION of the characteristic bone disease and biopsy. BE PRECISE ABOUT WHAT 'TRANSFORMED' MEANS: the BRAF and MEK inhibitors are supported by striking RESPONSE data (metabolic response on PET, symptom resolution) and regulatory approval, but no randomised trial has shown that they improve SURVIVAL. The only agent with a demonstrated survival benefit remains INTERFERON-ALPHA, and even that is a Cox-adjusted observational finding rather than a trial result. Both statements can be true at once, and the distinction is the exam point.
- “ECD = rare NON-LANGERHANS histiocytosis: foamy CD68+ , CD1a-/Langerin- histiocytes; MAPK-pathway driven (BRAF V600E).
- “Skeletal hallmark = BILATERAL SYMMETRIC OSTEOSCLEROSIS of long-bone metadiaphyses (lower limbs) -> symmetric distal-long-bone uptake on bone scan (near-pathognomonic).
- “Multisystem: 'coated aorta' (periaortic), 'hairy kidney' (perinephric), CNS, orbit, diabetes insipidus, xanthelasma. PET informative; biopsy + BRAF testing. Targeted BRAF/MEK inhibitors transformed treatment. Distinguish from LCH (CD1a+, lytic).
- “Prognosis: CNS involvement is the independent predictor of DEATH (HR 2.51, n=53) - examine the nervous system and image the brain, don't just count bones. Interferon-alpha independently predicted SURVIVAL (HR 0.32); no RCT shows a survival benefit for BRAF/MEK inhibitors, whose approval rests on response data.
Bilateral, symmetric osteosclerosis of the metadiaphyses of the lower-limb long bones with symmetric bone-scan uptake = Erdheim-Chester disease (foamy CD68+/CD1a- histiocytes, BRAF V600E).
Multisystem: 'coated aorta', 'hairy kidney', CNS/orbit, diabetes insipidus. PET + biopsy
- BRAF testing. BRAF/MEK inhibitors transformed treatment.
The Disease & Its Hallmarks
ECD is a rare non-Langerhans cell histiocytosis - foamy histiocytes that are CD68-positive and CD1a/Langerin-negative - driven by MAPK-pathway mutations, most commonly BRAF V600E. Its skeletal hallmark is bilateral symmetric osteosclerosis of the metadiaphyses of the long bones (especially the lower limbs), with symmetric increased uptake on bone scan - a near-pathognomonic pattern. It is a multisystem disease: periaortic 'coated aorta', perinephric 'hairy kidney', CNS, orbital (exophthalmos), pituitary (diabetes insipidus), skin (xanthelasma) and lung. Diagnosis combines the pattern with biopsy (foamy CD68+/CD1a- histiocytes, Touton giant cells) and BRAF/molecular testing, with PET highly informative; management has been transformed by BRAF/MEK inhibitors.
- Erdheim-Chester disease
- Non-Langerhans (foamy histiocytes)
- Langerhans cell histiocytosis
- Langerhans cells (Birbeck granules)
- Erdheim-Chester disease
- CD68+ , CD1a-/Langerin-
- Langerhans cell histiocytosis
- CD1a+ , Langerin/CD207+ , S100+
- Erdheim-Chester disease
- Bilateral symmetric osteoSCLEROSIS (long-bone metadiaphyses, legs)
- Langerhans cell histiocytosis
- LYTIC 'punched-out' lesions (skull, axial)
- Erdheim-Chester disease
- MAPK pathway (BRAF V600E common)
- Langerhans cell histiocytosis
- BRAF V600E also common
- Erdheim-Chester disease
- 'Coated aorta', 'hairy kidney', CNS, orbit, DI
- Langerhans cell histiocytosis
- Variable (single-system to multisystem)
Classification, the LCH Overlap, and the Mutation Spectrum
- The classification and the LCH overlap. In the 2016 Revised Classification of Histiocytoses (five groups: L, C, R, M, H), ECD sits in the "L" (Langerhans) group alongside LCH - the two share a clonal MAPK-driven myeloid-dendritic origin and can co-occur (about 15-20% of ECD patients have concurrent LCH - "mixed histiocytosis"), so the sharp ECD-versus-LCH split is a diagnostic contrast rather than a difference of origin. (The "R" group is Rosai-Dorfman disease; "H" is haemophagocytic lymphohistiocytosis.)
- A clonal myeloid neoplasm. ECD arises from a clonal myeloid progenitor (mutated haematopoietic stem/progenitor cells) - it behaves as an inflammatory myeloid neoplasm, and a subset have an associated myeloid malignancy (MDS/CMML).
- The fuller mutation spectrum. BRAF V600E is found in about half; the rest carry other activating MAPK/ERK mutations - MAP2K1 (MEK1), NRAS/KRAS/ARAF, and PIK3CA - which is why MEK inhibitors work in BRAF-wild-type disease.
Q: Where does ECD sit in the histiocytosis classification, and what is its mutation spectrum?
A: In the 2016 Revised Classification (L, C, R, M, H groups), ECD is in the "L" (Langerhans) group alongside LCH - they share a clonal MAPK-driven myeloid-dendritic origin and co-occur in ~15-20% ("mixed histiocytosis"). ECD is a clonal myeloid neoplasm (± associated MDS/CMML). Mutations: BRAF V600E in ~half; the rest have MAP2K1 (MEK1), NRAS/KRAS/ARAF, or PIK3CA - hence MEK inhibitors work in BRAF-wild-type disease.
Diagnosis & Management
- Imaging: symmetric distal long-bone osteosclerosis with symmetric bone-scan uptake; PET for the full extent (often more informative than CT/MRI); CT/MRI for organ involvement ('coated aorta', 'hairy kidney', CNS/orbit).
- Biopsy: foamy CD68+/CD1a-negative histiocytes (Touton giant cells, fibrosis); BRAF V600E/molecular testing.
- Distinguish from: Langerhans cell histiocytosis (CD1a+, lytic) and other causes of osteosclerosis.
- Treatment (transformed): BRAF inhibitors (BRAF V600E-mutant) and MEK inhibitors (MAPK pathway); interferon-alpha historically; specialist multidisciplinary care for the affected organs.
- Orthopaedic role: recognise the characteristic bone disease and obtain biopsy; manage bone pain.
The orthopaedic and radiological importance of Erdheim-Chester disease is recognition: the bilateral, symmetric osteosclerosis of the metadiaphyses of the lower-limb long bones, with symmetric increased uptake on bone scan, is a near-pathognomonic pattern that should prompt the diagnosis and a search for multisystem involvement, rather than being dismissed as nonspecific sclerosis. This matters because ECD is a multisystem, potentially life-threatening disease (cardiovascular, retroperitoneal, CNS), and because it is now a treatable one: it is a non-Langerhans histiocytosis driven by MAPK-pathway mutations - most commonly BRAF V600E - and targeted BRAF and MEK inhibitors have transformed its management, so confirming the diagnosis on biopsy (foamy CD68-positive, CD1a-negative histiocytes) with BRAF testing, distinguishing it from Langerhans cell histiocytosis and from other causes of osteosclerosis, and referring to a specialist multidisciplinary team can dramatically change outcome.
Targeted Therapy, Monitoring and Prognosis
- The targeted agents. Vemurafenib (a BRAF inhibitor) was the first agent approved specifically for BRAF V600E-mutant ECD (2017); dabrafenib (± trametinib) is also used, and the MEK inhibitor cobimetinib is approved for ECD (2022), including BRAF-wild-type disease. Interferon-alpha (± pegylated) was the historical first-line, with anakinra, sirolimus and others in selected cases.
- Monitoring. Response is assessed by PET (metabolic response), which is often rapid and dramatic on a BRAF inhibitor.
- Prognosis. Historically poor, and the numbers come from a 53-patient multicentre cohort: CNS involvement was an independent predictor of death (hazard ratio 2.51, 95% CI 1.28-5.52), while interferon-alpha independently predicted survival (hazard ratio 0.32, 95% CI 0.14-0.70). Cardiovascular involvement is the other major cause of death. Targeted therapy has changed practice on the strength of response data; no randomised trial has shown a survival benefit for a BRAF or MEK inhibitor, so the honest statement is that the disease is now treatable rather than that survival is proven to be longer.
Q: What are the specific targeted agents for ECD, how is response monitored, and what determines prognosis?
A: Vemurafenib (BRAF inhibitor) was the first agent approved for BRAF-V600E ECD (2017); dabrafenib ± trametinib also used; the MEK inhibitor cobimetinib is approved (2022, including BRAF-wild-type). Interferon-alpha was the historical first-line (± anakinra/sirolimus) and remains the only agent with a demonstrated survival benefit - hazard ratio 0.32 in a 53-patient multivariate cohort analysis, though observational. Response is monitored by PET (metabolic - often rapid/dramatic). The main adverse prognostic factor is CNS involvement (hazard ratio 2.51), with cardiovascular disease the other major cause of death. Targeted therapy is supported by response data and approval, not by a randomised survival trial - state that distinction rather than saying survival is proven to be longer.
What Actually Predicts Survival - and What 'Transformed' Means
The skeletal pattern is what brings the patient to an orthopaedic clinic, but it is not what determines whether they survive. In a multicentre cohort of 53 patients with biopsy-proven ECD followed from 1981 to 2010, multivariate Cox analysis identified central nervous system involvement as an independent predictor of death, with a hazard ratio of 2.51 (95% CI 1.28 to 5.52, p=0.006). The practical consequence is that a patient whose symmetric long-bone sclerosis has just been recognised needs a neurological examination and brain imaging, not only a skeletal survey - and that the presence or absence of CNS disease, rather than how many bones are involved, is what shapes the conversation about outlook. The cohort was also strikingly male, 39 men to 14 women.
In the same multivariate analysis, treatment with interferon-alpha was an independent predictor of survival - hazard ratio 0.32 (95% CI 0.14 to 0.70, p=0.006) - the first time any treatment had been shown to improve survival in ECD. It is an observational cohort with 87 percent of patients treated, so confounding by indication cannot be excluded and the authors said a randomised trial would be needed. But it is more than the label "historical" implies.
Vemurafenib (approved 2017 for BRAF V600E-mutant ECD) and cobimetinib (approved 2022, including BRAF-wild-type) produce rapid metabolic responses on PET and symptom resolution, and they are the modern standard. What they do not yet have is a randomised demonstration of improved survival. Saying the disease is now treatable is right; saying targeted therapy is proven to prolong life overstates the evidence.
Mnemonics & Memory Aids
ERDHEIM
Hook:ERDHEIM: Extra-skeletal multisystem, Rare non-Langerhans, Driven by BRAF, Histiocytes CD68+/CD1a-, Evaluate PET+biopsy, Inhibitors (BRAF/MEK), Metadiaphyseal symmetric sclerosis.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A bone scan shows symmetric increased uptake in the distal femora and tibiae, with corresponding osteosclerosis. What diagnosis should you consider and how is it managed?”
What it is
- Rare non-Langerhans cell histiocytosis
- Foamy histiocytes CD68+ , CD1a-/Langerin- (vs LCH which is CD1a+)
- MAPK-pathway driven (BRAF V600E common)
Skeletal hallmark
- Bilateral symmetric osteosclerosis of long-bone metadiaphyses (lower limbs)
- Symmetric increased uptake on bone scan (near-pathognomonic)
- Bone pain common
Multisystem features
- Cardiovascular: periaortic 'coated aorta'; pericardial/myocardial
- Retroperitoneal: perinephric 'hairy kidney' (ureteric obstruction)
- CNS, orbit (exophthalmos), pituitary (diabetes insipidus), skin (xanthelasma)
Diagnosis & treatment
- PET (extent) + CT/MRI (organs); biopsy (CD68+/CD1a-) + BRAF testing
- Distinguish from LCH (CD1a+, lytic) and other osteosclerosis causes
- BRAF/MEK inhibitors transformed treatment (response data; no survival RCT); MDT care
- Prognosis: CNS involvement HR 2.51 for death; interferon-alpha HR 0.32 for survival (n=53, observational)
Evidence & Key Studies
Erdheim-Chester disease: the role of PET imaging and bone-marrow biopsy in diagnosis
- Erdheim-Chester disease is an extremely rare non-Langerhans cell histiocytosis involving MAPK-pathway mutations, notably BRAF V600E.
- PET imaging was more informative than CT or MRI, identifying widespread FDG-avid skeletal and soft-tissue lesions; because of the skeletal lesions, bone-marrow/tissue biopsy was valuable and histopathology confirmed ECD with the BRAF V600E mutation.
- Multidisciplinary evaluation and targeted therapy with a BRAF inhibitor led to symptom resolution.
CNS involvement and treatment with interferon-alpha are independent prognostic factors in Erdheim-Chester disease: a multicenter survival analysis of 53 patients
- Multicentre prospective observational cohort of 53 patients with biopsy-proven ECD - 39 men and 14 women - followed between November 1981 and November 2010, with 46 (87 percent) receiving interferon-alpha or PEGylated interferon-alpha.
- On multivariate Cox analysis, central nervous system involvement was an independent predictor of death (hazard ratio 2.51, 95% CI 1.28 to 5.52, p=0.006), while treatment with interferon-alpha was an independent predictor of survival (hazard ratio 0.32, 95% CI 0.14 to 0.70, p=0.006) - the first treatment shown to improve survival in this disease.
- The authors state that definitive confirmation would require a randomised controlled trial. With 87 percent of the cohort treated, confounding by indication cannot be excluded, and the study predates the targeted-therapy era entirely.
ECD as a rare non-Langerhans cell histiocytosis involving MAPK-pathway (BRAF V600E) mutations, the superior diagnostic role of PET imaging in revealing widespread FDG-avid skeletal/soft-tissue lesions, the value of biopsy with BRAF confirmation, and the efficacy of targeted BRAF-inhibitor therapy come from the cited Al-Abdulmalek report. The skeletal hallmark (bilateral symmetric long-bone metadiaphyseal osteosclerosis), the CD68+/CD1a- immunophenotype, the multisystem features ('coated aorta', 'hairy kidney', CNS/ orbit, diabetes insipidus), and the distinction from Langerhans cell histiocytosis are standard, well-established teaching. The survival figures - the hazard ratios for CNS involvement and for interferon-alpha, and the sex distribution - come from the Arnaud cohort, which is observational and predates the targeted-therapy era. No randomised trial has shown that a BRAF or MEK inhibitor improves survival in ECD; their approval rests on response data. Nor is there a validated staging system, a surveillance interval, or a figure for what proportion of patients have skeletal involvement drawn from a defined cohort, so none is quoted here.