Question | validity | effect size | applicability
- Critical appraisal is not a memory test of study designs. It is a structured judgement about whether a result should influence care.
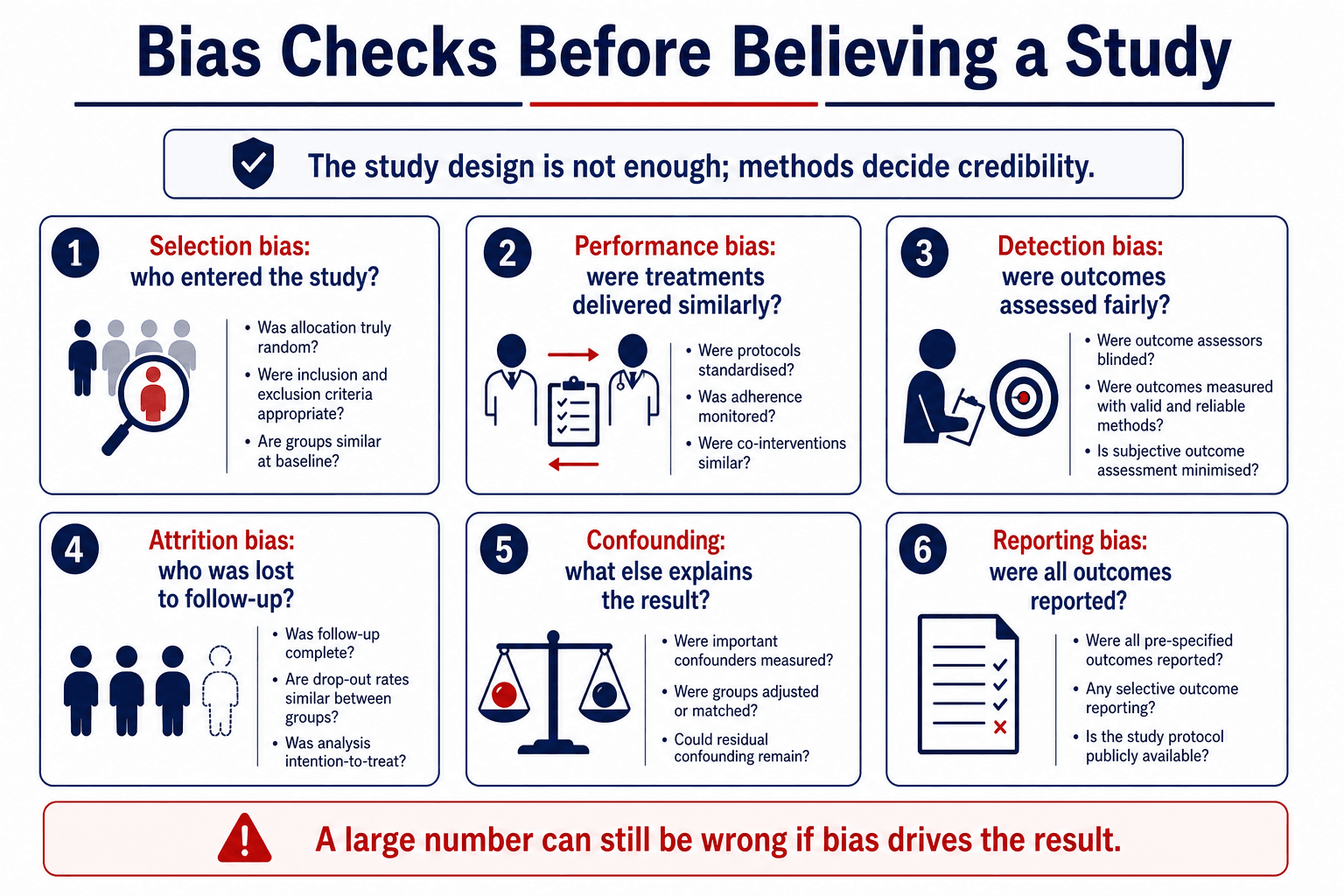
- A randomised trial can still be unreliable. Poor allocation concealment, missing data, crossover and selective reporting can destroy credibility.
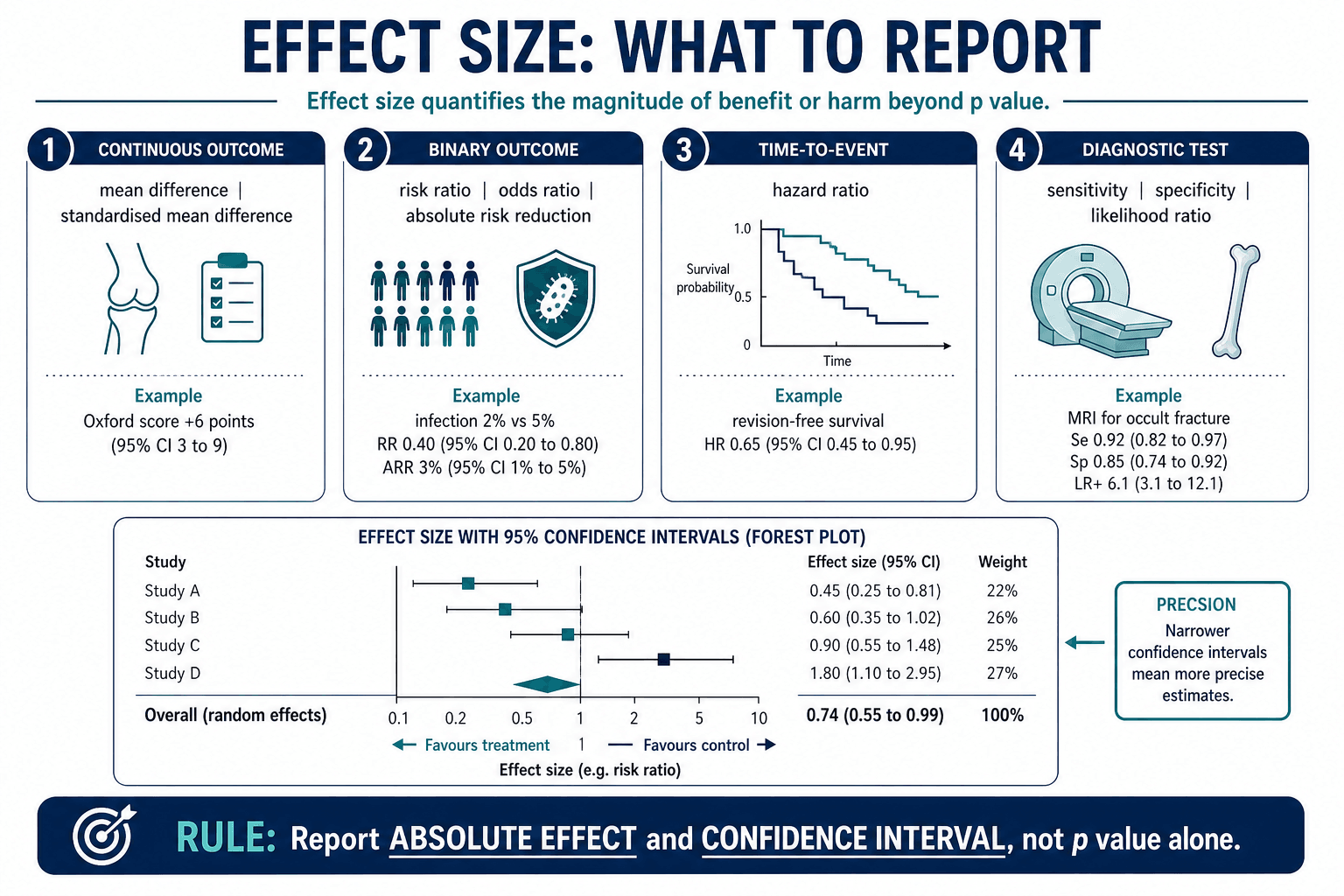
- A significant p value is not enough. Report effect size, absolute risk, confidence interval and clinical importance.
- Different questions need different designs. RCTs suit treatment efficacy; cohort studies suit prognosis; diagnostic studies need a reference standard.
- Evidence-based practice combines evidence, clinical expertise and patient values. It is not blind obedience to a paper.
- “Start journal club by stating the PICO in one sentence.
- “Always separate internal validity from external applicability.
- “For binary outcomes, ask for absolute risk reduction and number needed to treat or harm.
- “A clinically trivial difference can be statistically significant in a large study.
- “A negative study may be underpowered rather than proof of no difference.
A p value answers whether the observed difference is compatible with chance under a statistical model. It does not tell you whether the effect is large enough to matter, whether harms are acceptable, or whether the result applies to your patient.
PAPERRead A Paper
Hook:Do not finish the PAPER until you know whether it should change practice.
BIASEDBias Screen
Hook:A BIASED paper can have a beautiful p value.
CARESApply Evidence
Hook:Evidence CARES only when it changes a real decision safely.
Overview
Evidence-based orthopaedics means using the best available research, clinical judgement and patient values to make decisions. It does not mean automatically following the newest paper, the biggest trial, the loudest conference presentation or the most quoted meta-analysis.
The practical question is always:
This is internal validity. Ask whether the methods protected the result from bias, confounding, measurement error and missing data.
This is applicability. Ask whether the patient, intervention, comparator, outcome, surgeon skill and health system match your clinical decision.
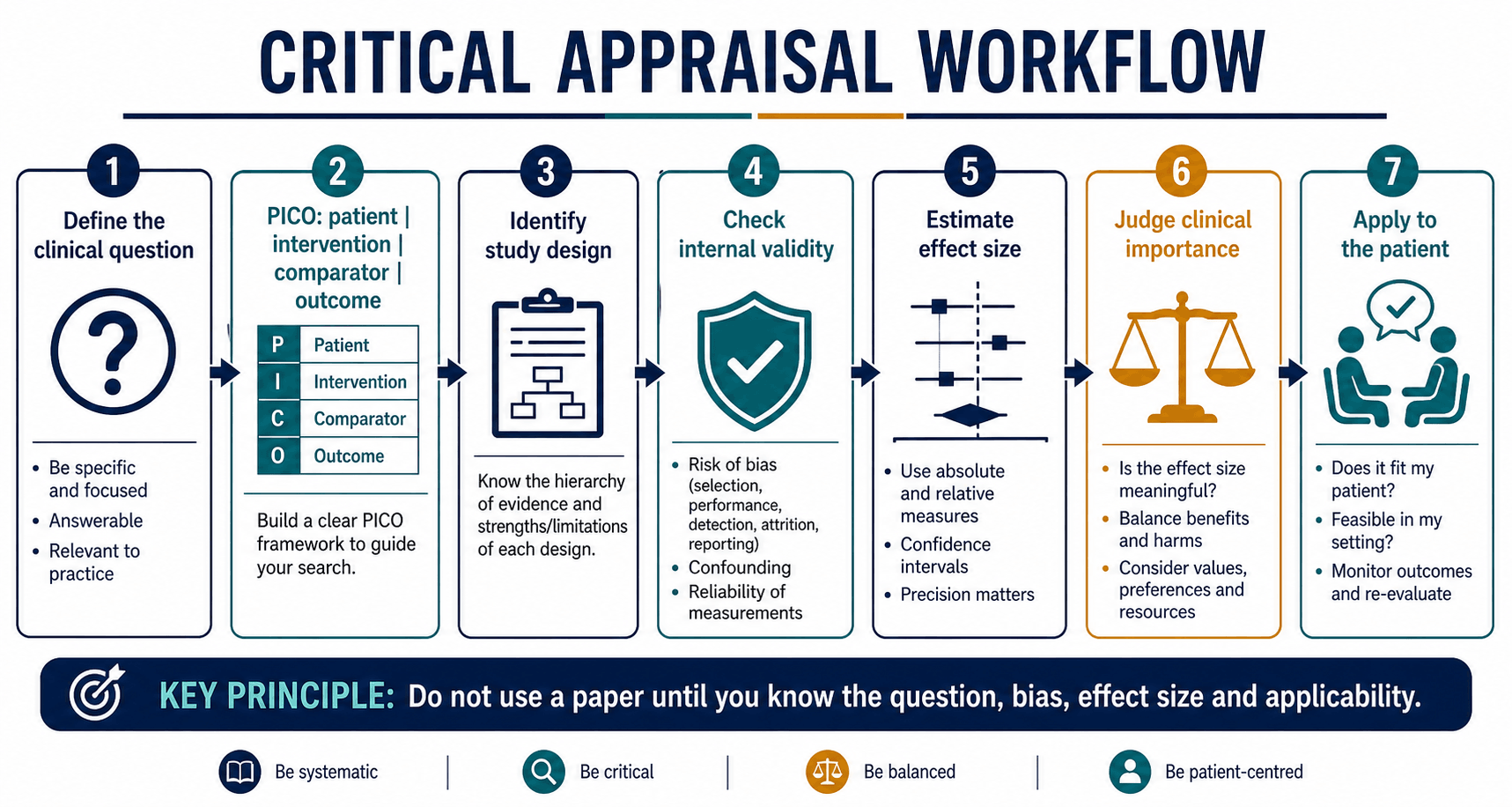
Begin by saying: "This paper asks whether intervention X compared with Y improves outcome Z in patients like this, and the key question is whether the methods and effect size are strong enough to change practice."
Concepts and Study Design
PICO before methods
PICO prevents vague appraisal. A paper about "fixation is better" is not appraisable until you define the patient, intervention, comparator and outcome.
- Question
- Who exactly is being treated?
- Example
- Older adults with displaced intracapsular femoral neck fracture who were ambulatory before injury.
- Question
- What is the treatment, implant or pathway?
- Example
- Total hip arthroplasty through a specified approach.
- Question
- What is it being compared with?
- Example
- Hemiarthroplasty, non-operative treatment, another implant or another rehabilitation pathway.
- Question
- What matters and when?
- Example
- Reoperation, function, pain, dislocation, infection, mortality, revision, cost and patient-reported outcome at a defined time.
Match study design to question
- What To Check
- Random sequence, allocation concealment, blinding where possible, intention-to-treat and follow-up.
- Orthopaedic Trap
- Surgical trials may be hard to blind, so outcome assessment and crossover matter.
- What To Check
- Confounding control, selection bias, surgeon/implant learning curve and outcome definition.
- Orthopaedic Trap
- Registry survival may not capture pain, function or radiographic failure.
Superiority, equivalence and non-inferiority
Not every trial sets out to show one treatment is better. Orthopaedic device and technique studies are frequently non-inferiority trials: a new implant only needs to be "not meaningfully worse" than the gold standard while offering another advantage (lower cost, simpler technique, fewer complications).
- Question
- Is the new treatment better?
- How it is judged
- The confidence interval for the difference excludes zero (no difference)
- Question
- Is it neither better nor worse, within a margin?
- How it is judged
- The confidence interval lies entirely within plus or minus the equivalence margin
- Question
- Is it not meaningfully worse?
- How it is judged
- The worse-side limit of the confidence interval does not cross the pre-set non-inferiority margin
- The non-inferiority margin (delta) must be defined a priori and clinically justified - it is the largest loss of efficacy that would still be acceptable. Setting it too wide can let a genuinely inferior treatment "pass".
- The analysis population is reversed. In a superiority trial, intention-to-treat is conservative. In a non-inferiority trial, intention-to-treat is anti-conservative because crossover and non-compliance blur the groups together and falsely favour non-inferiority, so a per-protocol analysis must agree with intention-to-treat before non-inferiority is accepted.
- Assay sensitivity: a non-inferiority trial is only interpretable if the gold-standard comparator genuinely works in that setting; otherwise "non-inferior" may simply mean "both ineffective".
Q: Why is intention-to-treat analysis insufficient on its own in a non-inferiority trial? A: Intention-to-treat dilutes differences between groups, which is conservative when proving superiority but anti-conservative when proving non-inferiority - it makes a worse treatment look acceptably close. A non-inferiority conclusion should therefore be supported by both intention-to-treat and per-protocol analyses, with a clinically justified margin and demonstrated assay sensitivity.
Clinical Relevance
Internal validity: can I believe the result?
- Question To Ask
- Were patients allocated or selected in a way that created unfair groups?
- Orthopaedic Example
- Healthier patients receive surgery while frailer patients receive non-operative care.
- Question To Ask
- Were co-interventions and rehabilitation similar?
- Orthopaedic Example
- One ACL group receives more supervised physiotherapy than the other.
- Question To Ask
- Were outcomes assessed fairly and blindly?
- Orthopaedic Example
- Surgeon-assessed radiographic union favours their preferred implant.
- Question To Ask
- Who was lost to follow-up?
- Orthopaedic Example
- Painful failures do not return to clinic and are counted as successes.
- Question To Ask
- What else explains the result?
- Orthopaedic Example
- High-volume surgeons use one implant and low-volume surgeons use another.
- Question To Ask
- Were all prespecified outcomes reported?
- Orthopaedic Example
- The published paper reports range of motion but omits reoperation.
Effect size: what does the number mean?
- What To Translate
- Difference in points, degrees, millimetres or time.
- Decision Question
- Is it greater than the minimum clinically important difference?
- What To Translate
- Relative change plus absolute baseline risk.
- Decision Question
- How many events are actually prevented or caused?
- What To Translate
- Event rate difference between groups.
- Decision Question
- What is the number needed to treat or harm?
- What To Translate
- Relative event rate over time.
- Decision Question
- Are proportional hazards plausible and follow-up long enough?
- What To Translate
- Test performance against reference standard.
- Decision Question
- How does the result change post-test probability?
Applicability: should I use it?
A valid result still may not apply. Check:
- Patient match: age, frailty, bone quality, comorbidity, activity level and pathology severity.
- Intervention match: implant, surgical approach, rehabilitation protocol and perioperative care.
- Surgeon/system match: volume, learning curve, imaging access, theatre resources and follow-up capability.
- Outcome match: patient-reported outcomes, revision, reoperation, complications, cost and survivorship.
- Time horizon: short-term function may conflict with long-term revision risk.
Registry studies often excel at large-scale implant survivorship and rare revision outcomes. Randomised trials better test efficacy in controlled populations. Neither replaces the other.
Differential: easily confused concepts
The commonest appraisal errors in vivas come from mixing up paired concepts that sound similar but answer different questions. Knowing the distinction is high yield.
- What It Actually Means
- A p value tests compatibility with chance; clinical importance tests whether the effect exceeds a meaningful threshold.
- Why It Matters
- A large trial can make a trivial difference significant; a small trial can miss an important one.
- What It Actually Means
- Relative risk or odds ratio is a ratio; absolute risk reduction is the actual event-rate difference.
- Why It Matters
- A halving of risk (relative) may be a fraction of a percent (absolute) when baseline risk is low.
- What It Actually Means
- Concealment hides the upcoming assignment before enrolment; blinding hides the received treatment afterwards.
- Why It Matters
- Concealment protects randomisation integrity; blinding protects performance and detection.
- What It Actually Means
- A confidence interval shows the range of effects compatible with the data; the p value gives a single threshold answer.
- Why It Matters
- A non-significant result with a wide interval is uncertainty, not proof of no effect.
- What It Actually Means
- Intention-to-treat keeps patients in their randomised group; per-protocol analyses only compliant patients.
- Why It Matters
- Per-protocol can reintroduce selection bias and exaggerate surgical benefit.
- What It Actually Means
- Efficacy is performance under ideal trial conditions; effectiveness is performance in routine practice.
- Why It Matters
- A result from an expert centre may not transfer to a general unit (the efficacy-effectiveness gap).
Type I and Type II Error, and Statistical Power
Behind every p value and every "underpowered" comment sit two error types examiners expect you to define precisely.
- Definition
- False positive - concluding a difference exists when it does not
- Governed by
- The significance level (conventionally 0.05)
- Orthopaedic consequence
- Adopting an implant or technique that is in truth no better
- Definition
- False negative - missing a real difference
- Governed by
- Sample size and effect size (beta conventionally 0.10 to 0.20)
- Orthopaedic consequence
- Discarding a genuinely better treatment because the trial was too small
- Power equals one minus beta - the probability of detecting a true effect of a given size. Trials are usually designed for 80 to 90 percent power.
- The sample-size (power) calculation is set a priori from the expected effect size (often the MCID), the baseline event rate or variance, alpha and the desired power. A small expected effect or a rare event demands a large sample - the central reason so many surgical RCTs end up underpowered.
- Absence of evidence is not evidence of absence: a non-significant result in an underpowered study does not prove equivalence. Check whether the study had the power to detect a clinically important difference, and read the confidence interval.
Q: A surgical RCT reports 'no significant difference' (p = 0.3) between two implants. Does this prove they are equivalent? A: No. This is most often a Type II error in an underpowered study. Check the a priori power calculation and the confidence interval - if the interval still includes a clinically important difference, the trial simply could not exclude one. Proving equivalence requires a purpose-designed equivalence or non-inferiority trial, not a failed superiority trial.
Guidelines, Registries and Global Practice
Critical appraisal is the engine behind every guideline and registry, so candidates from any system should know how the major bodies build and grade recommendations and how their orthopaedic registries are used as evidence.
How major bodies grade evidence
- Approach
- Clinical practice guidelines using a structured strength-of-recommendation system from systematic reviews.
- What To Note
- Recommendation strength reflects evidence quality plus consistency; many orthopaedic topics rest on limited or moderate evidence.
- Approach
- NICE uses GRADE-based methods; BOAST standards translate evidence into auditable care standards.
- What To Note
- BOAST documents convert evidence into concise, measurable practice points.
- Approach
- Education and consensus around fracture management with evidence summaries.
- What To Note
- Strong on technique and classification; consensus may outpace high-level trial data.
- Approach
- Consensus statements and instructional reviews across Europe.
- What To Note
- Useful where regional practice and implant availability differ.
- Approach
- Systematic reviews with explicit GRADE certainty ratings.
- What To Note
- Often rate orthopaedic surgical evidence as low or moderate certainty.
Registries as evidence
National joint replacement registries are a defining global source of orthopaedic effectiveness and safety data. They capture rare revision events and long-term survivorship that trials cannot.
- AOANJRR (Australia), NJR (England, Wales, NI and Isle of Man), AJRR (US), SHAR (Sweden), NARA (Nordic) and NZJR (New Zealand) provide implant survivorship, revision rates and bearing or fixation comparisons across hundreds of thousands of procedures.
- Strengths: large numbers, real-world populations, early detection of poorly performing implants (the metal-on-metal hip signal is the classic example).
- Limitations: confounding by indication, limited patient-reported outcomes, variable capture of function and pain, and dependence on accurate data entry.
High-resource versus limited-resource practice
- Higher-resource setting
- Subscription journals, guideline databases and registries.
- Limited-resource setting
- Reliance on open-access sources, WHO guidance and society summaries.
- Higher-resource setting
- Populations often match trial cohorts.
- Limited-resource setting
- Implant availability, follow-up capacity and case mix may differ from trial settings.
- Higher-resource setting
- Revision, patient-reported outcomes and survivorship.
- Limited-resource setting
- Limb salvage, infection control and return to function may dominate.
A guideline or registry finding from any one country is evidence contributing to a global picture; the appraisal question is always whether the population, implant and system match the patient in front of you, not which country produced the data.
Controversies and Areas of Uncertainty
Critical appraisal is itself debated. Examiners reward candidates who can discuss the limits of the evidence hierarchy rather than reciting it.
The classical pyramid places randomised trials above observational data, yet large registries and target-trial-emulation methods can answer questions (rare implant failure, long-term survivorship) that no feasible trial can. Many surgical questions cannot be ethically or practically randomised.
Blinding the surgeon is impossible, learning curves bias early results, equipoise is often lacking, and expertise-based designs are uncommon. A poorly conducted surgical trial may be weaker than a well-designed cohort study.
Selective outcome reporting, spin in abstracts, underpowered studies and unregistered protocols remain common in the orthopaedic literature. Trial registration and core outcome sets are partial but incomplete remedies.
The minimum clinically important difference varies by population, anchor method and baseline severity, so the same point change can be "important" in one study and not another. Treat any single MCID value with caution.
Say explicitly that the evidence hierarchy ranks designs on average but that a specific study must be judged on its own conduct, and that for many surgical questions high-quality observational and registry data are the best obtainable evidence.
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“You are shown a randomised trial comparing two fixation methods. The conclusion says one implant is statistically superior with p = 0.04.”
“A meta-analysis reports that a surgical technique reduces revision risk. The forest plot looks convincing, but the included studies are heterogeneous observational cohorts.”
“A paper reports that a new clinical test for a meniscal tear has a sensitivity of 90 percent and a specificity of 60 percent, validated against arthroscopy in a specialist sports clinic.”
Start
- State the PICO
- Identify study design
- Ask if design matches question
- Find primary outcome
- Check follow-up duration
Believe
- Selection bias
- Allocation concealment
- Blinding/outcome assessment
- Missing data
- Confounding and reporting bias
Use
- Absolute and relative effect
- Confidence interval
- Clinical importance
- Benefits versus harms
- Applicability to patient and setting
“Define the question, test the validity, quantify the effect and decide whether it applies.”
Evidence Base
Evidence-based medicine definition
- Evidence-based medicine integrates best evidence with clinical expertise and patient values.
- It is not cookbook medicine.
- External evidence can inform but not replace clinical judgement.
GRADE approach
- GRADE separates certainty of evidence from strength of recommendation.
- Evidence can be downgraded for risk of bias, inconsistency, indirectness, imprecision and publication bias.
- Recommendations also depend on values, harms and resource use.
Reporting guidelines
- Different study types require different reporting checklists.
- Transparent reporting helps readers judge bias and applicability.
- Poor reporting does not always mean poor methods, but it prevents confident appraisal.
AMSTAR 2
- AMSTAR 2 provides a structured method for appraising systematic reviews of healthcare interventions.
- It distinguishes critical from non-critical weaknesses.
- A meta-analysis can be misleading if the review question, search, bias assessment or synthesis is weak.
Levels of evidence in orthopaedics
- Major orthopaedic journals adopted a five-level hierarchy (Level I randomised trials through Level V expert opinion) applied separately to therapeutic, prognostic, diagnostic and economic questions.
- The level assigned depends on both study design and methodological quality, so a flawed randomised trial can drop below Level I.
- The grading was introduced to help readers rapidly gauge the strength of orthopaedic evidence.
Large orthopaedic RCT as appraisal exemplar (SPRINT)
- A multicentre randomised trial enrolling 1200 skeletally mature patients across 29 sites in Canada, the United States and the Netherlands compared reamed with non-reamed intramedullary nailing of tibial shaft fractures.
- Patients, outcome assessors and data analysts were blinded, and a blinded committee adjudicated the composite reoperation primary outcome.
- An a priori subgroup analysis separated open from closed fractures, illustrating prespecified rather than data-driven subgrouping.