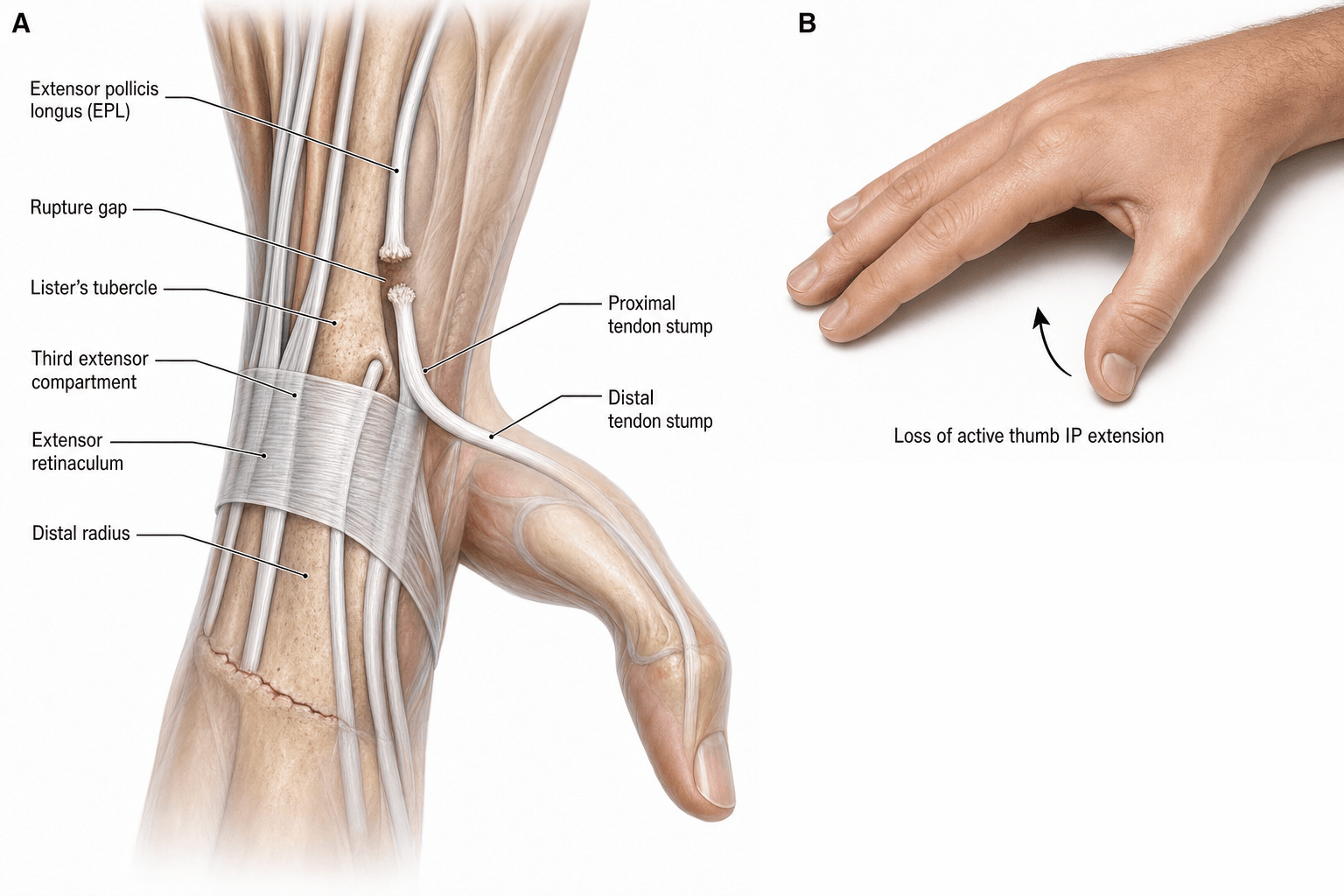
Attritional Rupture | Third Compartment | EIP-to-EPL Transfer
- EPL is the sole tendon in the 3rd dorsal compartment, angling sharply around the Lister tubercle pulley
- Most common cause of 'spontaneous' EPL rupture is an apparently minor (often non-displaced) distal radius fracture
- Direct primary repair is almost never possible - tendon ends are frayed, retracted and within an ischaemic 3rd compartment
- EIP-to-EPL tendon transfer is the gold-standard reconstruction; results are reliable and donor deficit is minimal
- Examination hallmark: positive retropulsion (drum) sign - patient cannot lift the thumb off a flat surface palm-down
- “EPL extends IP, MCP and retropulses CMCJ of the thumb (the only retropulsor)
- “After DRF, EPL ruptures weeks to months later even in a cast - mechanism is ischaemic + mechanical at the Lister tubercle
- “Loss of thumb retropulsion with intact EPB strongly suggests EPL rupture rather than PIN palsy
- “EIP is the donor of choice: it is expendable (two tendons to the index), synergistic, and of appropriate length
EPL sits alone in the 3rd dorsal compartment with EPB. It makes a sharp angular turn around the Lister tubercle, which acts as a fixed pulley. The tendon inserts on the dorsal base of the distal phalanx and is the only retropulsor of the thumb (extends IP, MCP and CMCJ in one line).
Two-hit mechanism at the Lister tubercle: (1) ischaemia at the watershed zone inside a tight fibro-osseous tunnel (haematoma, oedema, tenosynovitis), and (2) mechanical attrition as the tendon glides over an unforgiving bony ridge. The combination is unique to EPL.
Retropulsion (drum) sign is pathognomonic. With the palm flat on the table, the patient cannot lift the thumb dorsally. Tenodesis is also lost: wrist flexion fails to produce passive thumb IP extension because the EPL is discontinuous.
Direct repair is not feasible - the ends are frayed and the bed is diseased. The standard operation is extensor indicis proprius (EIP) to EPL transfer, routed subcutaneously around the radial border of the wrist, tensioned with the wrist neutral and the thumb in full extension.
- Diagnosis
- Retropulsion sign absent, tenodesis negative, EPB intact
- Treatment
- EIP-to-EPL transfer (primary)
- Key Pearl
- Cast or even a minor DRF is sufficient to cause this
- Diagnosis
- Often multiple tendon ruptures (caput ulnae, Mannerfelt spectrum)
- Treatment
- EIP transfer + dorsal tenosynovectomy + DRUJ management
- Key Pearl
- Always examine EPL specifically - it is easy to miss in RA
- Diagnosis
- Direct visualisation of divided tendon
- Treatment
- Direct repair within 2-3 weeks if bed is healthy
- Key Pearl
- Primary repair is the exception, not the rule for EPL
DRUMRetropulsion (Drum) Sign
Hook:DRUM = a positive retropulsion (drum) sign is the pathognomonic bedside test for EPL rupture.
TRANSFEREIP-to-EPL Transfer
Hook:TRANSFER = the operative steps for the gold-standard EIP-to-EPL reconstruction.
Overview and Epidemiology
EPL rupture is the single most common closed tendon rupture in the hand and the prototype of attritional rupture at a fibro-osseous pulley. The classic scenario - sudden, painless loss of thumb extension weeks after an apparently trivial distal radius fracture - is a board-favourite because it tests understanding of tendon biomechanics, third-compartment anatomy, and the principles of tendon transfer.
- Post-DRF attrition: Most common cause; non-displaced or minimally displaced fractures are over-represented
- Rheumatoid tenosynovitis: Caput ulnae, Mannerfelt spectrum
- Kienböck / SNAC / SLAC: Carpal collapse alters EPL mechanics at Lister
- Iatrogenic: Scaphoid screw, external fixator pin, dorsal plate prominence
- Direct laceration: Knife, glass, saw - the only scenario where direct repair is possible
- Loss of thumb retropulsion: Cannot lift thumb off flat surface
- Loss of IP and MCP extension: Tip pinch, key pinch, and grip strength all reduced
- Inability to retropulse the thumb: Cannot rest hand on table, climb, or pick up flat objects
- Secondary adduction collapse: The hand loses the 'palm-to-fist' contour during grip
Pathophysiology
The EPL is uniquely vulnerable because of its anatomy: a single tendon in a tight fibro-osseous tunnel making a 30-45 degree angular turn around a bony ridge. First hit - ischaemia at the watershed zone inside a tight compartment (haematoma, oedema, tenosynovitis, cast compression). Second hit - mechanical attrition as the weakened tendon grinds over the Lister tubercle with every thumb motion. The two hits summate and the tendon ruptures, usually at or just proximal to the Lister tubercle, often within an apparently intact retinaculum.
- Contents
- APL, EPB
- Site-specific pathology
- De Quervain tenosynovitis; EPB slips in rheumatoid disease
- Contents
- ECRL, ECRB
- Site-specific pathology
- Intersection syndrome; second-compartment syndrome
- Contents
- EPL (and EPB distally in some)
- Site-specific pathology
- Attritional rupture: post-DRF, RA, Kienböck, iatrogenic
Non-displaced fracture: 3rd compartment haematoma raises pressure
Cast immobilisation: Retinaculum-bound tendon under sustained compression
Watershed zone: Intratendinous blood supply poorest at Lister level
Sharp pulley angle: Greater than 30 degrees after DRF due to shortened radius
Result: Tendon frays within an apparently intact retinaculum and ruptures spontaneously
Dorsal synovitis: ECU subsheath attenuates, ECU subluxates volarly
Caput ulnae: DRUJ destroyed, ulnar head erodes dorsally
Ulnar-sided tendons: EDM, then EDC to small, then EIP rupture first
Radial tendons: EPL rupture later as synovitis reaches the 3rd compartment
Mannerfelt overlap: FPL may rupture at scaphoid level in the same hand
The rheumatoid extensor ruptures follow a named, examinable pattern - Vaughan-Jackson syndrome:
- What it is: sequential, progressive rupture of the finger extensor tendons starting on the ULNAR side and marching RADIALLY - the extensor digiti minimi goes first, then the EDC to the small finger, then ring, then middle, and so on.
- The cause: attrition over the dorsally prominent, eroded distal ulna (caput ulnae) combined with dorsal tenosynovitis - the most ulnar tendons sit directly over the offending bone.
- The clinical clue: a rheumatoid patient who "cannot extend the little finger MCP," then weeks later the ring finger - the progressive ulnar-to-radial loss is the signature (and droop is at the MCP joints, with passive tenodesis lost).
- How it relates to EPL: the EPL is on the radial side, so it tends to rupture later in the sequence; finding an EPL rupture in a rheumatoid hand should prompt a search for (already ruptured) ulnar extensors.
- Distinguish from Mannerfelt syndrome: Vaughan-Jackson is extensor tendons over the caput ulnae; Mannerfelt is the FLEXOR (FPL) rupture over a scaphoid/trapezial osteophyte in the carpal tunnel. Both are attritional rheumatoid ruptures, opposite sides of the wrist.
Exam point: progressive ulnar-to-radial loss of finger extension in a rheumatoid hand = Vaughan-Jackson syndrome from caput ulnae - and the key adjunct to any tendon transfer is dorsal tenosynovectomy + treating the distal ulna (Darrach/Sauvé-Kapandji) to stop further ruptures.
LISTERPathogenesis of EPL Rupture at the Lister Tubercle
Hook:LISTER = the two-hit (ischaemia + attrition) rupture mechanism unique to EPL.
Classification and Types
Classification by Aetiology
- Mechanism
- 3rd compartment ischaemia + Lister attrition
- Timing
- 4-12 weeks typical; range 1-12 months
- Notes
- Most common cause of 'spontaneous' EPL rupture
- Mechanism
- Tenosynovitis, caput ulnae, attritional wear
- Timing
- Insidious, often multiple tendons
- Notes
- Often part of Vaughan-Jackson or Mannerfelt syndrome
- Mechanism
- Carpal collapse alters Lister pulley mechanics
- Timing
- Progressive
- Notes
- Treat the underlying cause; transfer is palliative
- Mechanism
- Scaphoid screw, dorsal plate, pin site
- Timing
- Early post-op
- Notes
- Remove offending hardware + transfer
- Mechanism
- Direct division over the thumb MC or wrist
- Timing
- Acute
- Notes
- Only scenario where direct repair is feasible
The aetiology dictates reconstruction - transfer for attrition, repair for laceration.
Clinical Assessment

- Mechanism: Often 'spontaneous'; ask about recent DRF (even 3-6 months prior)
- Onset: Sudden painless loss of thumb extension is classic
- Function: Difficulty lifting thumb off table, climbing, picking up coins
- Background: RA, Kienböck, prior wrist surgery, scaphoid screws
- Pain: Usually absent at the time of rupture (an important feature)
- Retropulsion (drum) sign: Cannot lift thumb with palm flat on table
- Active IP / MCP extension: Lost at the thumb; EPB alone cannot extend the IP
- Tenodesis test: Wrist flexion fails to extend the thumb IP (EPL discontinuity)
- Palpation: Loss of EPL tendon over Lister tubercle; may feel a gap
- Other tendons: Always test EDC, EDM, FPL (caput ulnae / Mannerfelt spectrum)
- PIN check: Full finger and thumb extension rules out posterior interosseous nerve palsy
Technique: Patient places the palm flat on a hard table, fingers adducted, thumb alongside the index. Ask the patient to lift the thumb straight up off the table - to 'drum' the thumb.
Intact EPL: Thumb lifts off the table cleanly through retropulsion of the CMCJ combined with full MCP and IP extension.
Ruptured EPL: Thumb remains on the table. EPB may produce a small amount of MCP extension but cannot retropulse the thumb or extend the IP joint.
Key point: The retropulsion sign isolates EPL function from EPB. A patient with a strong EPB but a positive retropulsion sign has an EPL rupture until proven otherwise.
- Thumb posture
- Thumb lies flat, IP flexed, no retropulsion
- Discriminating finding
- Positive retropulsion sign, tenodesis negative
- Key test / imaging
- Clinical; X-ray wrist for DRF callus, US for gap
- Thumb posture
- All fingers and thumb drop, no retropulsion, radial wrist deviation
- Discriminating finding
- Wrist extension preserved (ECRL), no finger or thumb extension at all
- Key test / imaging
- EMG / NCS; MRI for radial tunnel lesion
- Thumb posture
- Flicking, painful snapping over Lister
- Discriminating finding
- Tendon visible and palpable subluxing
- Key test / imaging
- Dynamic US; clinical with active motion
- Thumb posture
- Loss of thumb MCP extension only, IP preserved
- Discriminating finding
- IP extension and retropulsion intact via EPL
- Key test / imaging
- Selective testing of EPB against resistance
- Thumb posture
- Loss of thumb IP flexion in a rheumatoid hand
- Discriminating finding
- Palpable nodule over FPL, attritional rupture at scaphoid
- Key test / imaging
- Active IP flexion lost; EPL intact (the opposite deficit)
- Thumb posture
- Painful radial wrist, weak thumb extension
- Discriminating finding
- Pain limits testing, Finkelstein positive
- Key test / imaging
- Clinical; symptoms predominate over signs
EPL rupture: Loss of thumb extension in isolation, with a normal-appearing hand at rest and normal finger extension. Retropulsion sign is positive. PIN is intact.
PIN palsy: Global loss of finger and thumb MCP extension (wrist extension preserved via ECRL, often with radial deviation). The retropulsion sign is also positive, but finger extension is absent too. The deficit extends well beyond the thumb.
A common viva trap is to misattribute an isolated EPL rupture to a PIN palsy - always test finger and wrist extension in every patient with a 'dropped thumb'.
Investigations
Imaging and Diagnostic Protocol
Views: PA, lateral and oblique of the wrist and distal radius
Look for: Healed DRF callus, RA changes (ulnar styloid erosions, caput ulnae, carpal collapse), Kienböck sclerosis of lunate, SNAC wrist (scaphoid nonunion), screw or plate over the 3rd compartment
Clinical correlation: The diagnosis of EPL rupture is clinical; the radiograph is to identify the cause, not to confirm the rupture
Indication: Palpable gap, equivocal exam, suspected partial rupture or in-continuity degeneration
Findings: Discontinuity of EPL fibres, retracted stump, fluid in the 3rd compartment, tenosynovial thickening
Advantage: Dynamic, cheap, no contrast, compares with the contralateral side
Indication: Chronic ruptures with multiple tendon involvement (RA), surgical planning, assessment of 3rd compartment bed
Findings: Tendon gap, scar tissue, marrow oedema in lunate (Kienböck), active tenosynovitis with enhancement
Use: Especially valuable in rheumatoid hands to map all ruptured tendons before reconstruction
Plain radiographs of the wrist are mandatory in any patient with suspected attritional EPL rupture - the radiograph identifies the cause (DRF, RA, Kienböck, screw impingement) far more often than the radiograph confirms the rupture. Do not delay EIP-to-EPL transfer waiting for MRI in the post-DRF scenario; the diagnosis and decision are clinical.
- Implication
- Confirms attritional post-DRF rupture
- Management shift
- EIP-to-EPL transfer alone
- Implication
- Iatrogenic attrition
- Management shift
- Remove hardware + EIP transfer
- Implication
- RA with multiple extensor ruptures likely
- Management shift
- Dorsal tenosynovectomy + multiple transfers + Darrach or Sauvé-Kapandji
- Implication
- Kienböck disease driving attrition
- Management shift
- Stage lunate ( Lichtenstein ); treat Kienböck + transfer
- Implication
- Carpal collapse changes EPL mechanics
- Management shift
- Scaphoid reconstruction / 4-corner fusion + transfer
Management Algorithm
EIP-to-EPL Tendon Transfer (Gold Standard)
Indication: Attritional EPL rupture with a frayed, retracted stump and a diseased 3rd compartment bed. The standard operation for post-DRF and most RA ruptures.
Operative Steps
Anaesthesia: General or regional (axillary block)
Position: Supine, arm table, tourniquet high on the arm
Prophylaxis: Single-dose IV antibiotics per local policy
Incision: Oblique over the index MCPJ, ulnar to the extensor pollicis brevis
Identify EIP: Ulnar and deep to the extensor digitorum tendon to the index; confirm with independent index extension against resistance
Harvest: Strip the EIP with a distal periosteal tongue to maximise length; deliver into the wound
Incision: Dorsoradial incision over the thumb MC; identify the distal EPL stump
Trim: Excise frayed ends back to healthy tendon; debride the 3rd compartment
Mobilise: Release the proximal EPL stump from the retinaculum and Lister tunnel
Tunnel: Subcutaneous from the index incision, around the radial border of the wrist, to the thumb incision
Plane: Superficial to the extensor retinaculum to avoid re-entering the diseased 3rd compartment
Technique: Pulvertaft weave of the EIP through the distal EPL stump, 3 passes minimum
Suture: 4-0 braided nonabsorbable (e.g. Ticron) for each pass; epitendinous 6-0 running
Position: Wrist neutral, thumb in full retropulsion with IP and MCP extended
Adjustment: Slight overcorrection is acceptable; the transfer will loosen a little in the cast
Confirm: Full passive thumb flexion should still be possible without the transfer falling slack
Closure: Skin only; no deep drains usually needed
Splint: Forearm-based thumb spica cast, wrist neutral, thumb in full retropulsion and extension
0-4 weeks: Full-time spica cast; finger flexion encouraged within the cast
4 weeks: Remove cast, start protected active thumb motion in a removable splint
6 weeks: Begin gentle strengthening, retropulsion retraining
12 weeks: Return to most activities; heavy loading after 4-6 months
The single most common error in EIP-to-EPL transfer is under-tensioning. With the wrist in neutral and the thumb in full extension and retropulsion, the transfer should hold the thumb at least at the level of the index, ideally a few millimetres above. A slack transfer will produce a flexion lag at the thumb IP joint and weak retropulsion - the same complaints the patient presented with.
The choice of EIP is not arbitrary; it satisfies the classic principles of tendon transfer (Boyes/Brand) that examiners expect you to recite for any transfer:
- Supple, mobile joints - the thumb IP/MCP and CMC must be passively correctable first (a stiff joint will not move however good the transfer); release contractures before transferring.
- Expendable donor - taking EIP leaves the index with the EDC, so index extension is preserved (the donor's loss must be tolerable).
- Adequate excursion - the donor's amplitude must match the recipient's need (EPL needs roughly 30 mm; EIP/finger extensors provide it).
- Adequate strength - one grade of power is typically lost after transfer, so the donor must be strong enough.
- Synergy - synergistic donors are easier to re-educate; EIP fires with finger/thumb extension, in phase with the lost EPL.
- Straight line of pull - the transfer should run as directly as possible to its insertion (hence the subcutaneous radial route, not back through the diseased 3rd compartment).
- One tendon, one function - a single transfer should ideally power a single action.
- Soft-tissue equilibrium / supple bed - a healthy, scar-free, well-vascularised bed is needed for gliding (the very reason direct repair of the attritional rupture fails).
Exam point: justify EIP-to-EPL by the transfer principles - expendable, synergistic, correct amplitude and a straight subcutaneous line of pull into a supple thumb - and remember the prerequisite of supple joints and a healthy bed.
Complications
- Incidence
- Common (15-25 percent)
- Risk Factors
- Scarring from prior surgery, prolonged immobilisation
- Management
- Hand therapy; tenolysis if persistent beyond 6 months
- Incidence
- 5-15 percent
- Risk Factors
- Under-tensioning, transfer elongation, adhesions
- Management
- Re-tensioning or tenolysis if functionally limiting
- Incidence
- 2-5 percent
- Risk Factors
- Early return to loading, poor tendon quality
- Management
- Re-transfer (use EDM) or tendon graft
- Incidence
- Up to 20 percent initially, recovers in most
- Risk Factors
- EIP harvest from index finger
- Management
- Re-education; rarely symptomatic beyond 6 months
- Incidence
- 2-5 percent
- Risk Factors
- Severe injury, prolonged immobilisation
- Management
- Early hand therapy, vitamin C prophylaxis in some protocols
- Incidence
- 10-15 percent
- Risk Factors
- Transfer under-tensioned, pre-existing thumb CMCJ OA
- Management
- Splinting, CMCJ stabilisation if arthritic
Trap 1 - Direct repair of an attritional rupture: The tendon ends are frayed, the bed is diseased, and a primary repair will fail. Convert to EIP-to-EPL transfer.
Trap 2 - Under-tensioning the transfer: Tension the transfer with the wrist neutral, thumb in full retropulsion and extension, with slight overcorrection. A slack transfer is the most common cause of a poor result.
Outcomes and Prognosis
- Treatment
- EIP-to-EPL transfer within 3 months
- Expected Outcome
- Good-to-excellent in 85-90 percent
- Long-term Function
- Pinch strength recovers to 80-90 percent of opposite side
- Treatment
- EIP transfer or tendon graft
- Expected Outcome
- Good in 70-80 percent
- Long-term Function
- Some persistent lag, weaker pinch
- Treatment
- EIP transfer + synovectomy
- Expected Outcome
- Good in 75-85 percent, depends on disease activity
- Long-term Function
- Risk of further ruptures from ongoing synovitis
- Treatment
- Multiple transfers, dorsal tenosynovectomy, DRUJ procedure
- Expected Outcome
- Good in 60-75 percent
- Long-term Function
- Functional but disease progression is the main threat
- Treatment
- Direct repair
- Expected Outcome
- Excellent in 90+ percent
- Long-term Function
- Best prognosis of all categories
Best prognosis: Young, post-DRF, healthy contralateral hand, transfer within 3 months, supervised hand therapy.
Guarded prognosis: Elderly rheumatoid with multiple tendon involvement, severe caput ulnae, late presentation with established thumb adduction contracture, dependent on disease control.
Key threshold: 3-6 months - delayed reconstruction still works but outcomes decline steadily. The transfer itself is reliable; the limiting factors are the bed, the disease, and the rehabilitation.
Guidelines, Registries & Global Practice
- EPL rupture is the most common closed extensor tendon rupture of the hand, with a post-DRF incidence of approximately 0.2-5 percent (higher in non-displaced or minimally displaced fractures)
- Rheumatoid extensor ruptures affect 1-5 percent of RA patients cumulatively, with EPL among the later tendons to fail after the ulnar-sided extensors
- Kienböck and SNAC wrists add a smaller but recognised cohort
- Mechanism (ischaemia plus attrition at Lister) is universal and not country-specific
- High-resource: EIP-to-EPL transfer as a day-case under regional block with immediate hand therapy access
- Limited-resource: cast immobilisation and delayed transfer remain effective; PL or plantaris graft is a low-cost alternative when EIP is unavailable
- Universal principle: the diagnosis is clinical (retropulsion sign); do not delay reconstruction waiting for advanced imaging in clear cases
- Training: EIP harvest is a core hand-surgery skill taught across BSSH/ASSH/EFHS curricula
- Diagnostic emphasis
- Retropulsion sign, isolate EPL from EPB, rule out PIN palsy
- Reconstruction of choice
- EIP-to-EPL transfer as first-line; PL or plantaris graft as alternative
- Special notes
- Strong emphasis on hand-therapy-led rehabilitation
- Diagnostic emphasis
- Clinical diagnosis; X-ray to identify cause, not to confirm rupture
- Reconstruction of choice
- EIP transfer as standard; EDM or tendon graft as salvage
- Special notes
- Caution against under-tensioning; reference to drum sign in teaching
- Diagnostic emphasis
- Bedside retropulsion test; ultrasound if diagnosis unclear
- Reconstruction of choice
- EIP-to-EPL transfer; multi-tendon transfer in RA with DRUJ procedure
- Special notes
- Highlight role of tenosynovectomy and DRUJ management in RA
- Diagnostic emphasis
- Retropulsion sign and clinical examination
- Reconstruction of choice
- EIP transfer; local modifications (e.g. extensor pollicis brevis rerouting) in some units
- Special notes
- Consider regional causes (TB tenosynovitis) in atypical presentations
There is no dedicated registry for EPL rupture because it is a clinical diagnosis treated by an established, low-morbidity tendon transfer. The evidence base is dominated by retrospective case series and a few prospective cohorts (Chung KC et al.). The few randomised comparisons (EIP transfer vs interposition graft; early vs delayed reconstruction) favour EIP transfer as the first-line operation. The single most important practice point - tension the transfer with the thumb in full retropulsion - is consistent across all hand surgery traditions.
Record in every suspected EPL rupture:
- Retropulsion (drum) sign: positive or negative
- Tenodesis test at the thumb IP joint: positive (loss of passive extension with wrist flexion) or negative
- Examination of all other extensor tendons (EDC, EDM, EIP) and the FPL
- A working diagnosis: isolated EPL rupture vs PIN palsy vs caput ulnae / Mannerfelt spectrum
- Cause identified (post-DRF, RA, Kienböck, iatrogenic)
- Reconstruction offered: EIP-to-EPL transfer, with alternatives and donor-site morbidity explained
A missed EPL rupture, or one misattributed to a PIN palsy, is a recurring source of complaints globally. A positive retropulsion sign with preserved finger extension should drive a timely tendon transfer.
Controversies & Areas of Uncertainty
Some surgeons reconstruct within weeks of the diagnosis, others prefer to wait 3 months for soft-tissue consolidation. Functional outcomes appear similar, but earlier reconstruction reliably returns patients to work sooner. There is no high-quality trial that establishes the optimum delay.
A few small comparative series suggest interposition grafts (palmaris longus, plantaris) give comparable retropulsion but with higher rates of adhesions and reoperation. EIP transfer is now universally preferred when the donor is available, but graft reconstruction remains a valid fallback.
Some authors advocate prophylactic retinacular release at the time of DRF fixation or in high-risk rheumatoid hands to prevent EPL rupture. The evidence is mixed: the release may destabilise the tendon and the procedure is not without morbidity. It is not a universal standard.
When a dorsal plate is in place, surgeons vary on whether to remove the hardware, retain it, or stage the procedures. Hardware removal adds morbidity but may improve tendon glide. Decision is individualised by symptoms, fracture healing, and the plate's prominence over the 3rd compartment.
MCQ Practice Points
Q: In which dorsal compartment of the wrist does the extensor pollicis longus tendon travel, and what structure does it angulate around? A: Third dorsal compartment, with the extensor pollicis brevis. The EPL makes a sharp angular turn around the Lister (dorsal radial) tubercle of the distal radius, which acts as a fixed pulley and is the site of attritional rupture.
Q: What is the retropulsion (drum) sign, and what does it indicate? A: With the palm flat on a hard surface, the patient is asked to lift the thumb dorsally off the table. An intact EPL retropulses the thumb at the CMCJ while extending the MCP and IP joints. A positive sign (the thumb stays on the table) is pathognomonic for EPL rupture, with preserved EPB explaining any residual MCP extension.
Q: Why does the EPL rupture after a non-displaced distal radius fracture? A: A two-hit mechanism at the Lister tubercle: (1) ischaemia of the EPL within a tight, oedematous 3rd compartment (haematoma, cast compression, tenosynovitis), and (2) mechanical attrition as the weakened tendon glides over the bony ridge with every thumb motion. Rupture typically occurs 4-12 weeks after injury and is often within an apparently intact retinaculum.
Q: What is the gold-standard reconstruction for attritional EPL rupture, and why is direct repair usually not possible? A: Extensor indicis proprius (EIP) to EPL tendon transfer, routed subcutaneously around the radial wrist and woven into the distal EPL stump using a Pulvertaft technique. Direct repair is not feasible because the tendon ends are frayed, retracted and within a diseased 3rd-compartment bed; primary suture in this setting fails.
Q: How is the EIP-to-EPL transfer tensioned? A: With the wrist in neutral and the thumb in full retropulsion and extension at the MCP and IP joints, the transfer should hold the thumb at least at the level of the index, ideally a few millimetres higher (slight overcorrection). Full passive thumb flexion must still be possible without the transfer falling slack. Under-tensioning is the most common cause of a poor result.
Q: How do you distinguish EPL rupture from posterior interosseous nerve (PIN) palsy at the bedside? A: In EPL rupture, the deficit is isolated to the thumb (positive retropulsion sign, no IP extension) with normal finger and wrist extension. In PIN palsy, all finger MCP extension and thumb extension are lost, with wrist extension preserved but radially deviated (ECRL only). The retropulsion sign is positive in both, but the global pattern of weakness points to PIN palsy.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old solicitor fell on her outstretched hand 10 weeks ago and was treated in a below-elbow cast for a minimally displaced distal radius fracture. The cast was removed at 6 weeks and radiographs showed a healed fracture. Yesterday, while reaching for a coffee cup, she noticed she could no longer lift her right thumb off the table. There is no pain, no wound, and she can move all her other fingers normally. Examination reveals a positive retropulsion (drum) sign, with intact finger extension and wrist extension. What is the diagnosis and how do you manage it?”
“A 62-year-old woman with long-standing seropositive rheumatoid arthritis on methotrexate presents with progressive loss of finger and thumb extension in her dominant right hand over the past 4 months. She can no longer extend her small finger MCP joint, the ring finger MCP, or her thumb IP. On examination, there is a dorsal tenosynovial swelling, the ulnar head is prominent and ballotable dorsally (caput ulnae), and the ECU subluxates volarly on supination. The retropulsion sign is positive, and she cannot extend the small, ring, or thumb IP joints. X-rays show ulnar styloid erosions, ulnar head resorption, and DRUJ destruction with early carpal collapse. How do you approach this?”
Key Anatomy
- EPL sits alone in the 3rd dorsal compartment, angling sharply around the Lister tubercle
- EPL inserts on the dorsal base of the distal phalanx; extends IP, MCP and retropulses CMCJ
- EPL is the only retropulsor of the thumb - EPB extends the MCP only
- Lister tubercle is a fixed pulley and the site of attritional rupture
Diagnosis
- Retropulsion (drum) sign: cannot lift the thumb off a flat surface with the palm down
- Tenodesis test: wrist flexion fails to extend the thumb IP
- Always test all other extensors and wrist extension to rule out PIN palsy
- Plain radiographs identify the cause (DRF callus, RA, Kienböck, screw impingement)
Pathogenesis
- Post-DRF attrition is the most common cause, even after non-displaced fractures
- Two-hit mechanism: ischaemia in the 3rd compartment + attrition over the Lister ridge
- Rheumatoid ruptures occur in the caput ulnae / Mannerfelt spectrum
- Kienböck, SNAC wrist, scaphoid screws and dorsal plates are recognised causes
Reconstruction
- Direct repair is rarely possible - tendon ends are frayed and the bed is diseased
- EIP-to-EPL transfer is the gold standard: harvest EIP, route subcutaneously, Pulvertaft weave
- Tension with the wrist neutral and the thumb in full retropulsion and extension
- Alternatives: EDM, palmaris longus or plantaris graft; FDS transfer as a last resort
Outcomes and Pitfalls
- Good-to-excellent in 85-90 percent of post-DRF EIP transfers
- Donor-site morbidity is minimal: independent index extension recovers in 6-12 weeks
- Under-tensioning the transfer is the most common cause of a poor result
- Always address the underlying cause (tenosynovectomy, DRUJ, hardware, Kienböck)
Evidence Base and Key Trials
Attrition ruptures of flexor tendons in rheumatoid arthritis caused by bony spurs in the carpal tunnel: a clinical and radiological study
- Original description of attritional FPL rupture at the level of the scaphoid in rheumatoid hands
- Established the concept of 'closed' tendon rupture from attrition against a bony or retinacular edge in inflammatory disease
- Coined the term that now describes the same disease spectrum affecting the EPL and other tendons
- Highlighted the importance of dorsal tenosynovectomy as prophylaxis before tendon failure
Incidence of extensor pollicis longus tendon rupture after nondisplaced distal radius fractures
- Population-based estimate of EPL rupture after non-displaced DRF in adults
- Confirmed that EPL rupture occurs even after seemingly trivial fractures, often within 3 months
- Higher cumulative incidence than generally quoted for non-operative DRF
- EIP-to-EPL transfer produced reliable return of retropulsion and pinch in this cohort
Delayed rupture of the thumb extensor tendon: a 5-year study of 18 consecutive cases
- Anatomical and clinical analysis of EPL rupture after non-displaced DRF
- Demonstrated that the rupture consistently occurs at or just proximal to the Lister tubercle
- Supported the ischaemia-plus-attrition mechanism within the 3rd compartment
- Highlighted the absence of a true tendon gap at the time of early examination
Rupture of the extensor pollicis longus tendon after Colles fracture and by rheumatoid arthritis
- Compares EPL rupture patterns between Colles fracture and rheumatoid arthritis
- Confirms that EPL rupture is a recognised complication after both aetiology groups
- Supports the unifying concept of attritional rupture at a fibro-osseous pulley
- Provides a direct author link between the FPL Mannerfelt spectrum and EPL rupture