Verdan Zones | Mallet Finger | Boutonnière | Elson's Test
- Verdan Zones: Odd = Joints (I=DIP, III=PIP, V=MCP, VII=Wrist). Even = Bones
- Mallet (Zone I): Stack splint DIPJ extension 6-8 weeks. Bony mallet with greater than 1/3 articular = surgery
- Boutonnière (Zone III): Central slip rupture → lateral bands migrate volar → PIPJ flexion, DIPJ hyperextension
- Elson's Test: Flex PIPJ 90°, extend against resistance. Intact = floppy DIP. Torn = rigid DIP (lateral bands tighten)
- Sagittal Band (Zone V): 'Boxer's knuckle' - tendon subluxates ulnarly between knuckles
- “Active DIP flexion exercises MANDATORY in Boutonnière splinting (pulls lateral bands dorsal)
- “Juncturae tendinum can mask proximal lacerations - test each finger independently
- “Zone V lacerations often penetrate joint capsule - requires washout
- “Relative Motion Splinting (Yoke) now gold standard for Zone V-VI repairs
Extensor Tendon Injuries
Central Slip Integrity. Flex PIP 90°. Ask to extend. Rigid DIP = Torn Central Slip. Floppy DIP = Intact.
Odd = Joints. I=DIP, III=PIP, V=MCP. Even = Bones.
Continuous Extension. 6-8 weeks 24/7. Even 1 second of flexion resets the clock.
F-RElson's Test Interpretation
Hook:Floppy = Fine (central slip intact); Rigid = Ruptured. The torn central slip throws extension onto the lateral bands, stiffening the DIP.
Overview & Epidemiology
Extensor tendon injuries are among the most frequently encountered hand tendon injuries. In a 10-year US population-based study, acute traumatic hand/wrist tendon injuries occurred at 33.2 per 100,000 person-years, with extensor injuries more common than flexor injuries, peaking at age 20-29 with a male predominance (de Jong 2014).
- Most common closed tendon injury: mallet finger (Zone I), typically from a forced flexion (ball-sport "jamming") of the extended DIPJ.
- Most common extensor injury site overall: Zone III of the index finger.
- ~25% are work-related (construction, food preparation, transport) — relevant for return-to-work counselling.
- Mechanisms: lacerations (glass, knives) dominate open dorsal injuries; closed avulsions cause mallet and Boutonnière; direct blows cause sagittal band rupture.
Pathophysiology & Functional Anatomy
The extensor mechanism is a thin, broad, low-excursion system — unlike the round, gliding flexors. Key points that drive management:
- Extrinsic extensors (EDC, EIP, EDM, EPL, ECRL/B, ECU) arise in the forearm; intrinsic muscles (lumbricals, interossei) contribute the lateral bands.
- Over the proximal phalanx the EDC splits into a central slip (inserts on the base of the middle phalanx, extends the PIPJ) and two lateral bands (join the intrinsics to form the conjoined lateral bands → terminal tendon at the distal phalanx, extends the DIPJ).
- Sagittal bands at the MCPJ tether the EDC centrally over the joint — rupture allows ulnar subluxation ("boxer's knuckle").
- Triangular ligament (dorsal, distal) keeps the lateral bands dorsal; transverse retinacular ligament (volar) restrains them. Central slip loss tips this balance so the lateral bands fall volar to the PIP axis → Boutonnière.
- Juncturae tendinum interconnect the EDC tendons over the dorsum of the hand; an adjacent intact tendon can extend a finger with a proximal (zone V-VI) laceration, masking the injury.
- Extensor tendons have little excursion and tolerate little gapping — even 1-2 mm of repair-site lengthening produces clinically significant extensor lag.
Classification: Verdan Zones
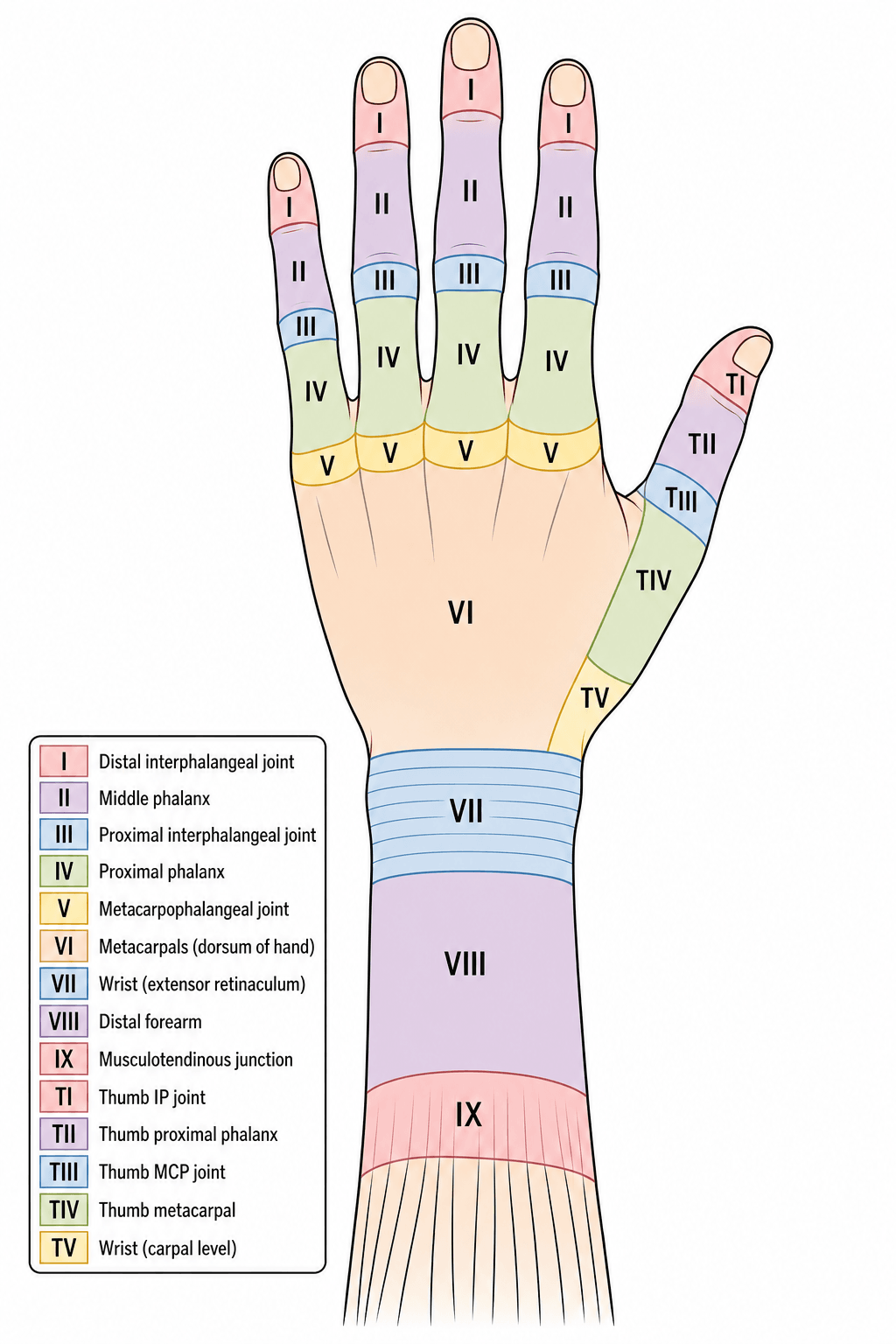
Odd numbers are joints; even numbers are bones. Treatment and prognosis vary by zone — odd-numbered (joint-level) zones have thin tendons, little surrounding tissue, and the highest adhesion risk.
- Zone I: DIP joint — terminal tendon (Mallet finger).
- Zone III: PIP joint — central slip (Boutonnière).
- Zone V: MCP joint — sagittal bands (boxer's knuckle).
- Zone VII: Carpus — extensor retinaculum (high adhesion/tethering risk).
ODD = JOINTSVerdan Zones
Hook:Just remember the odd numbers (I, III, V, VII) sit over joints — the even numbers fall over the bones in between.
Clinical Presentation
Extensor tendon injuries are classified by Verdan zones (I-IX)—odd numbers are joints, even numbers are bones. Zone I (DIP/Mallet finger) is the most common closed tendon injury: treat with Stack splint in extension for 6-8 weeks. Zone III (PIP/Boutonnière) involves central slip rupture causing lateral band volar migration; requires extension splinting for 6 weeks with active DIP flexion exercises to prevent deformity. Elson's test diagnoses central slip injury: with PIP flexed 90°, if the central slip is torn, the DIP becomes rigid (lateral bands tighten). Zone V (MCP) sagittal band rupture ("Boxer's knuckle") causes extensor subluxation into the valley between knuckles. Unlike flexors, extensors are flat with less excursion and prone to gapping.
Investigations
Extensor injuries are largely a clinical diagnosis, but targeted investigations refine management:
- Plain radiographs (AP + true lateral): mandatory for any suspected mallet — quantify fragment size (% articular surface) and look for volar subluxation of the distal phalanx (the key surgical trigger). Also excludes associated fracture/dislocation and radiopaque glass foreign bodies in lacerations.
- Wound exploration is the definitive "investigation" for open dorsal injuries — examine through the full range of motion, as a tendon divided in flexion retracts out of the wound when the finger is extended.
- Bedside tests: Elson's test (central slip integrity, Zone III) and assessment of active extension against gravity/resistance at each zone. Test each digit independently to defeat juncturae masking.
- Ultrasound / MRI: reserved for chronic, occult, or zone VII-VIII injuries where the level of disruption or adhesion is unclear; not routine in the acute setting.
Examining the Extensor Mechanism at the Bedside
The topic invokes several bedside tests (Elson's, "Boyes' test", independent-digit testing, distinguishing EDC from EIP) — here they are together.
- Elson's test (central slip / Zone III). With the PIP flexed 90° over a table edge, ask for PIP extension against resistance: a rigid (fixed-extension) DIP means the central slip is torn (extensor force diverted to the lateral bands); a floppy DIP means it is intact. This is the reference early test.
- Boyes' test (central slip, late sign). With the PIP held in passive extension, ask the patient to flex the DIP actively: inability to flex the DIP suggests central-slip injury with tight/contracted lateral bands. It turns positive later than Elson's, which is why Elson's is preferred acutely.
- Distinguishing EDC from EIP (and EDM). Ask the patient to extend the index (or little) finger while the other fingers are held in a fist — only the independent extensors (EIP to the index, EDM to the little finger) can extend in that position, because EDC is slack when the other MCPs are flexed. This confirms an intact independent extensor (and identifies EIP as available for transfer).
- Defeating the juncturae. Test each digit independently: through the juncturae tendinum, an intact adjacent EDC can extend a finger with a proximal (Zone VI) laceration and mask the injury — so a finger that extends does not prove its own tendon is intact.
- Sagittal band (Zone V). The patient cannot initiate MCP extension from a flexed position but can hold it once passively placed; watch for the tendon snapping ulnar-ward into the intermetacarpal valley.
Acutely, use Elson's test for the central slip (rigid DIP on resisted PIP extension = torn); Boyes' test (loss of active DIP flexion with the PIP held extended) is the same injury's late sign. To find an intact independent extensor (e.g. before an EIP transfer), extend one finger with the others fisted — only EIP/EDM can. And always test each finger separately, because juncturae tendinum can mask a proximal laceration.
Differential Diagnosis of Loss of Active Finger Extension
The cardinal sign of an extensor injury — inability to actively extend a digit — has several mimics. Distinguishing them changes management entirely.
Why Can't This Finger Extend?
Management
Pathology: rupture of the terminal extensor tendon at its insertion, with or without a bony avulsion (bony mallet).
- Closed (soft-tissue): Stack/extension splint, DIPJ in full extension ONLY (PIPJ free), worn continuously for 6-8 weeks, then nights for 2-4 weeks. Any episode of DIP flexion resets healing.
- Bony mallet WITHOUT subluxation: splinting is appropriate even for large fragments — outcomes match surgery at lower cost/complication (Gumussuyu 2020).
- Bony mallet WITH volar subluxation / joint instability: extension-block pinning (Ishiguro) or ORIF.
- Chronic: tenodermodesis, or central slip tenotomy (Fowler) for secondary swan-neck.
To test Central Slip (Zone III): Flex PIPJ 90° over table edge. Ask patient to extend against resistance. If Central Slip INTACT: Strong extension, DIPJ remains floppy. If Central Slip TORN: Weak extension, DIPJ becomes rigid (Lateral bands tighten).
Clinical Context: Crucial to diagnose acute Zone III injury before Boutonnière develops.
Epidemiology of Hand & Wrist Tendon Injuries
- 10-year US population-based cohort: acute traumatic tendon injury incidence 33.2 per 100,000 person-years
- Extensor tendon injuries occurred MORE frequently than flexor tendon injuries
- Most common extensor injury site: zone III of the index finger; peak incidence at age 20-29; male predominance
- Work-related injuries accounted for 24.9%, most often in construction/extraction occupations
Splinting for Mallet Finger (Cochrane Review)
- Four randomised/quasi-randomised trials, 278 participants with 283 mallet injuries
- Insufficient evidence to show any custom-made or off-the-shelf finger splint is superior to a standard Stack splint
- No significant difference between Kirschner-wire fixation and splinting (Pryor & Howard) for the single comparative trial
- Patient adherence to continuous splint use and splint durability identified as central to success
Elson's Test for Central Slip Rupture (Original Description)
- Closed central slip rupture is easily missed until a late buttonhole (Boutonnière) deformity appears
- From a PIP flexed 90° over a table edge, the patient extends against resistance
- Absent PIP extension force WITH fixed (rigid) extension at the DIP indicates complete central slip rupture
- Detects injury earlier than Boyes' test, which only becomes positive late
Pin-Block vs Extension Orthosis for Bony Mallet
- 39 closed mallet fractures with greater than 1/3 articular involvement WITHOUT subluxation (Wehbe-Schneider IB/IC); 21 pin-block vs 18 extension orthosis
- No significant difference in clinical outcome, extension lag, DIPJ flexion, pain or aesthetic scores at mean 18-month follow-up
- Conservative group had a more frequent dorsal bump but fewer complications (no pin-tract infection/nail dystrophy)
- Direct, indirect and total costs were significantly higher in the surgical group
Extension Block Pinning (Ishiguro) vs Single K-Wire for Bony Mallet
- 98 surgically treated mallet fractures comparing the Ishiguro extension-block technique with a single-wire 'umbrella' technique, assessed at 1 year by the Crawford method
- Both percutaneous techniques achieved good results overall
- Better outcomes in younger patients and those treated early, regardless of technique
- Technique selection should be guided by fragment size/displacement (Wehbe-Schneider type) and time from injury
ICAM / Relative-Motion Yoke Orthosis for Zone IV-VII Repairs
- Describes the Wyndell Merritt immediate controlled active motion (ICAM) relative-motion yoke orthosis for zone IV-VII extensor repairs
- The yoke holds the repaired digit in relative MCP extension, offloading the repair while permitting immediate active hand use
- Case experience showed early restoration of composite motion and grip strength comparable to the uninjured hand by ~10 weeks
- Offers a low-profile alternative to bulky dynamic/static forearm-based splinting, without wrist immobilisation
Relative Motion Flexion Orthosis for Boutonnière
- 23 patients managed with a relative-motion flexion (RMF) orthosis: 8 acute Boutonnière (6 weeks) and chronic cases after serial casting (3 months)
- Greater MCP flexion increases dorsal EDC pull on the lateral bands, drawing them dorsally and relaxing the volar lumbrical pull
- All patients met Strickland-Steichen 'excellent' criteria, with a mean 35° increase in range of motion
- Both acute and selected chronic Boutonnière improved, supporting a trial of non-operative RMF before surgery
Complications
Complications of Extensor Injury
Guidelines, Registries & Global Practice
Global Epidemiology
- Acute traumatic hand/wrist tendon injuries occur at ~33 per 100,000 person-years (10-year US population study); extensor injuries are more common than flexor, peaking at age 20-29 with male predominance (de Jong 2014).
- Zone III of the index finger is the most common extensor injury site; mallet finger (Zone I) is the most common closed tendon injury and a frequent ball-sport (cricket, basketball, baseball) and occupational injury worldwide.
- ~25% of hand tendon injuries are work-related, concentrated in construction/extraction, food preparation, and transport occupations — relevant for return-to-work planning in any health system.
Side-by-Side Guidance
- Position on extensor injuries
- Continuous DIP-extension splinting for soft-tissue mallet; surgery reserved for subluxation/large unstable fragments; early controlled motion regimens for zone IV-VII repairs
- Position on extensor injuries
- Zone-based management; splinting first-line for mallet and acute closed Boutonnière; primary repair with epitendinous augmentation for open lacerations
- Position on extensor injuries
- Endorses relative-motion (ICAM/yoke) and early-active-motion protocols for dorsal hand repairs to reduce adhesions
- Position on extensor injuries
- Harmonises Verdan zone terminology and outcome reporting across regions
There is broad international agreement: closed soft-tissue mallet and acute Boutonnière are splinted; open lacerations are repaired; relative-motion rehabilitation is favoured for zone IV-VII. Differences are mainly in operative thresholds for bony mallet and in availability of certified hand therapy.
Registry & Outcome Notes
- Unlike arthroplasty, extensor tendon injuries are not tracked in implant registries; evidence rests on cohort series and the single Cochrane review (Handoll 2004), which highlights the lack of high-level trial data — a recognised research gap.
- Outcome reporting uses Strickland-Steichen / Miller criteria, extensor lag, and total active motion (TAM); standardised PROMs (e.g. MHQ) increasingly supplement these.
High- vs Limited-Resource Practice
- Well-resourced settings: certified hand therapists, custom thermoplastic and relative-motion orthoses, early-active-motion protocols, and ready microsurgical repair.
- Limited-resource settings: reliance on prefabricated/improvised extension splints (aluminium-foam, Stack), static immobilisation when therapy is scarce, and longer travel for specialist repair — making adherence-friendly, low-cost splinting and clear patient education disproportionately important.
- Universal first principles: tetanus status, wound irrigation and prophylactic antibiotics for contaminated/bite wounds, and a low threshold to exclude joint penetration in dorsal lacerations.
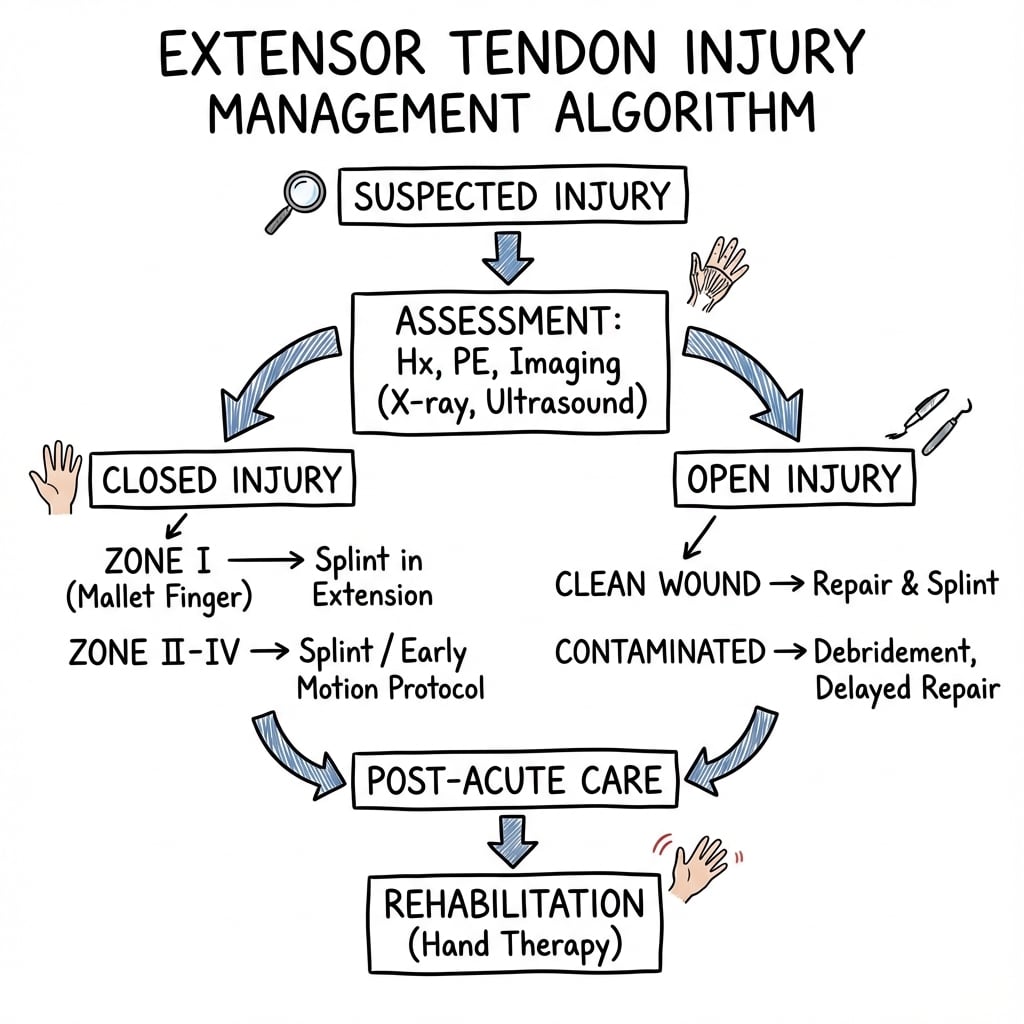
Decision Pathway Diagram
The Extensor Mechanism as a Balanced System (Why the Deformities Interconvert)
The topic describes mallet, Boutonnière and swan-neck as separate deformities and notes that a chronic mallet can cause a swan-neck — here is the single balance that links them.
- A delicate central-slip vs lateral-band balance. PIP extension is driven by the central slip (dorsal); DIP extension by the conjoined lateral bands and terminal tendon. The triangular ligament holds the lateral bands dorsal at the PIP, while the transverse retinacular ligament and the oblique retinacular ligament (ORL, of Landsmeer) restrain them volar-ward and mechanically couple PIP and DIP motion (the ORL runs volar to the PIP axis and dorsal to the DIP axis, so PIP extension tightens it and assists DIP extension).
- Boutonnière = the central slip fails. Loss of the central slip lets the lateral bands slip volar to the PIP axis: they now flex the PIP and, being tight, hyperextend the DIP — PIP flexion plus DIP hyperextension.
- Swan-neck = the opposite imbalance. When the balance tips the other way — a chronic mallet (terminal tendon lost, so extensor force is thrown proximally onto the central slip), volar plate laxity, or intrinsic tightness — the PIP hyperextends and the DIP flexes. This is why an untreated mallet can evolve into a secondary swan-neck.
- The therapeutic corollary. This coupling explains the treatments used elsewhere in this topic: active DIP flexion during Boutonnière splinting draws the lateral bands back dorsally; a Fowler central-slip tenotomy deliberately weakens PIP extension to rebalance a mallet-driven swan-neck; and over-correcting a Boutonnière risks tipping the finger into a swan-neck. (Each established deformity is developed in its own topic.)
Mallet, Boutonnière and swan-neck are all failures of the same central-slip / lateral-band / ORL balance. Lose the central slip and the lateral bands fall volar → Boutonnière (PIP flexed, DIP hyperextended). Lose the terminal tendon (mallet) or gain PIP volar-plate laxity and the force shifts dorsally → swan-neck (PIP hyperextended, DIP flexed). This is why an untreated mallet can become a swan-neck, and why DIP-flexion exercises and the Fowler tenotomy work.
M-B-SFinger Deformities by Zone
Hook:Boutonnière and swan-neck are mirror-image PIP/DIP postures: Boutonnière flexes the PIP, swan-neck hyperextends it.
Controversies & Areas of Uncertainty
- Surgery vs splinting for bony mallet — the long-held "greater than 1/3 articular surface" rule is increasingly questioned. In fractures without volar subluxation, comparative data show splinting matches surgery for outcome at lower cost and complication (Gumussuyu 2020). The strongest surgical indication is now DIPJ subluxation/instability, not fragment size alone.
- Optimal mallet splint and duration — the Cochrane review (Handoll 2004) found no splint type superior; 6-8 weeks continuous is convention rather than high-level evidence, and the trade-off between rigid adherence and skin maceration is unresolved.
- Relative-motion (yoke/ICAM) vs traditional dynamic/static splinting for zone IV-VII repairs — relative-motion protocols allow immediate hand use and appear to reduce adhesions, but most evidence is Level IV; high-quality randomised comparison data are still limited.
- Acute primary repair of central slip vs splinting for closed zone III injuries — closed acute injuries are generally splinted, but the threshold for operative repair (e.g. with displaced bony avulsion or open injury) varies between units.
- Extent of capsular exploration in zone V lacerations — whether every dorsal MCP laceration mandates formal joint exploration, or only those with a "fight-bite" mechanism or visible capsular breach, remains a point of judgement; the cost of a missed septic joint drives a low threshold.
MCQ Practice Points
Q: What are the extensor tendon zones and why are they important?
A: 8 zones (odd numbers over joints, even over bones): Zone 1 (DIP), Zone 2 (middle phalanx), Zone 3 (PIP), Zone 4 (proximal phalanx), Zone 5 (MCP), Zone 6 (metacarpals), Zone 7 (wrist), Zone 8 (forearm). Importance: Treatment varies by zone - Zone 1-2 often splinted, Zone 3+ usually repaired. Zones over joints have thinner tendons and less surrounding tissue, making repair more challenging and prone to adhesions.
Q: What is a mallet finger and how is it treated?
A: Mallet finger: Zone 1 injury with disruption of terminal extensor tendon, causing DIP flexion deformity (15-45°). Types: Tendinous (closed injury, forced flexion); Bony (avulsion fracture of distal phalanx dorsum). Treatment: Closed/small bony mallet: Splinting in DIP extension (Stack splint) for 6-8 weeks continuous, followed by 4 weeks night splinting. Bony mallet with greater than 30% articular surface or subluxation: Consider K-wire or ORIF.
Q: What is a boutonniere deformity and what causes it?
A: Boutonniere deformity: PIP flexion + DIP hyperextension, caused by Zone 3 injury (central slip disruption). Mechanism: Central slip disruption causes lateral bands to migrate volar to PIP axis, becoming flexors at PIP and increasing extension at DIP. Acute treatment: Splint PIP in extension (DIP free) for 6 weeks. Chronic boutonniere: Surgical reconstruction (lateral band mobilization, extensor tenolysis, central slip reconstruction) with variable results.
Q: What is the Elson test and what does it assess?
A: Elson test assesses central slip integrity (Zone 3). Technique: PIP flexed 90° over table edge, patient attempts to extend against resistance. Positive test: Weak PIP extension with rigid DIP (due to lateral bands substituting via intact lateral bands). Negative test: Strong PIP extension with floppy DIP. A positive Elson test in acute injury indicates central slip rupture requiring splinting to prevent boutonniere deformity.
Q: What is a sagittal band rupture and how does it present?
A: Sagittal band stabilizes extensor tendon over MCP joint (Zone 5). Rupture causes extensor subluxation (tendon subluxates ulnarly, usually over middle finger). Presentation: Painful snapping over MCP with finger extension; May be unable to initiate extension from flexed position. Causes: Trauma (punch), inflammatory arthritis. Treatment: Acute (less than 3 weeks) - splinting MCP in extension; Chronic - surgical repair/reconstruction of sagittal band.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old woman cut the back of her hand on glass. She has a 2cm laceration over the 3rd MCP joint. She cannot extend the middle finger at the MCPJ. X-ray is normal. How do you manage this?”
“A 28-year-old basketball player presents 2 days after jamming his right ring finger. He has a flexion deformity at the DIP joint and cannot actively extend it. X-rays show an avulsion fracture involving approximately 40% of the articular surface of the distal phalanx with 2mm of volar subluxation of the distal phalanx. What is your assessment and management approach?”
“A 45-year-old presents with a longstanding deformity of his left index finger that occurred after a basketball injury 18 months ago. He was told it was just a 'jammed finger' and it was not treated initially. Examination shows fixed PIP joint flexion contracture of 40 degrees and DIP joint hyperextension of 30 degrees. He cannot actively extend the PIP joint beyond 40 degrees of flexion and passive correction is limited to 20 degrees. X-rays show no arthritis. He requests treatment as the deformity affects his hand function and appearance. What would you discuss?”
Zones
- I: DIP (Mallet)
- III: PIP (Central Slip/Boutonnière)
- V: MCP (Sagittal Band)
- Odd = Joints
Tests
- Elson's Test: For Zone III (Central slip)
- Bouvier Test: For Ulnar Claw (Intrinsics)
Treatments
- Mallet: Splint DIP only 6-8w
- Boutonnière: Splint PIP extension 6w (Active DIP flexion)
- Open V/VI: Repair + Early Motion
References
- Elson RA. Rupture of the central slip of the extensor hood of the finger. A test for early diagnosis. J Bone Joint Surg Br. 1986;68(2):229-31. PMID 3958008.
- Handoll HHG, Vaghela MV. Interventions for treating mallet finger injuries. Cochrane Database Syst Rev. 2004;(3):CD004574. PMID 15266538.
- de Jong JP, Nguyen JT, Sonnema AJM, et al. The incidence of acute traumatic tendon injuries in the hand and wrist: a 10-year population-based study. Clin Orthop Surg. 2014;6(2):196-202. PMID 24900902.
- Gumussuyu G, Asoglu MM, Guler O, et al. Extension pin block technique versus extension orthosis for acute bony mallet finger; a retrospective comparison. Orthop Traumatol Surg Res. 2020;107(5):102764. PMID 33333280.
- Burns MC, Derby B, Neumeister MW. Wyndell Merritt immediate controlled active motion (ICAM) protocol following extensor tendon repairs in zone IV-VII. Hand (N Y). 2013;8(1):17-22. PMID 24426888.
- Merritt WH. The relative motion concept in acute and chronic boutonniere deformity: invited commentary. J Hand Ther. 2023;36(2):258-268. PMID 37045641.
- Rocchi L, Fulchignoni C, De Vitis R, et al. Extension block pinning vs single Kirschner wiring to treat bony mallet finger. Acta Biomed. 2022;92(S3):e2021535. PMID 35604272.
- Doyle JR. Extensor tendons: acute injuries. In: Green's Operative Hand Surgery.