Tendon Transfers | Grafts | Chronic Deficiency
- Full passive ROM is mandatory before any reconstruction attempt.
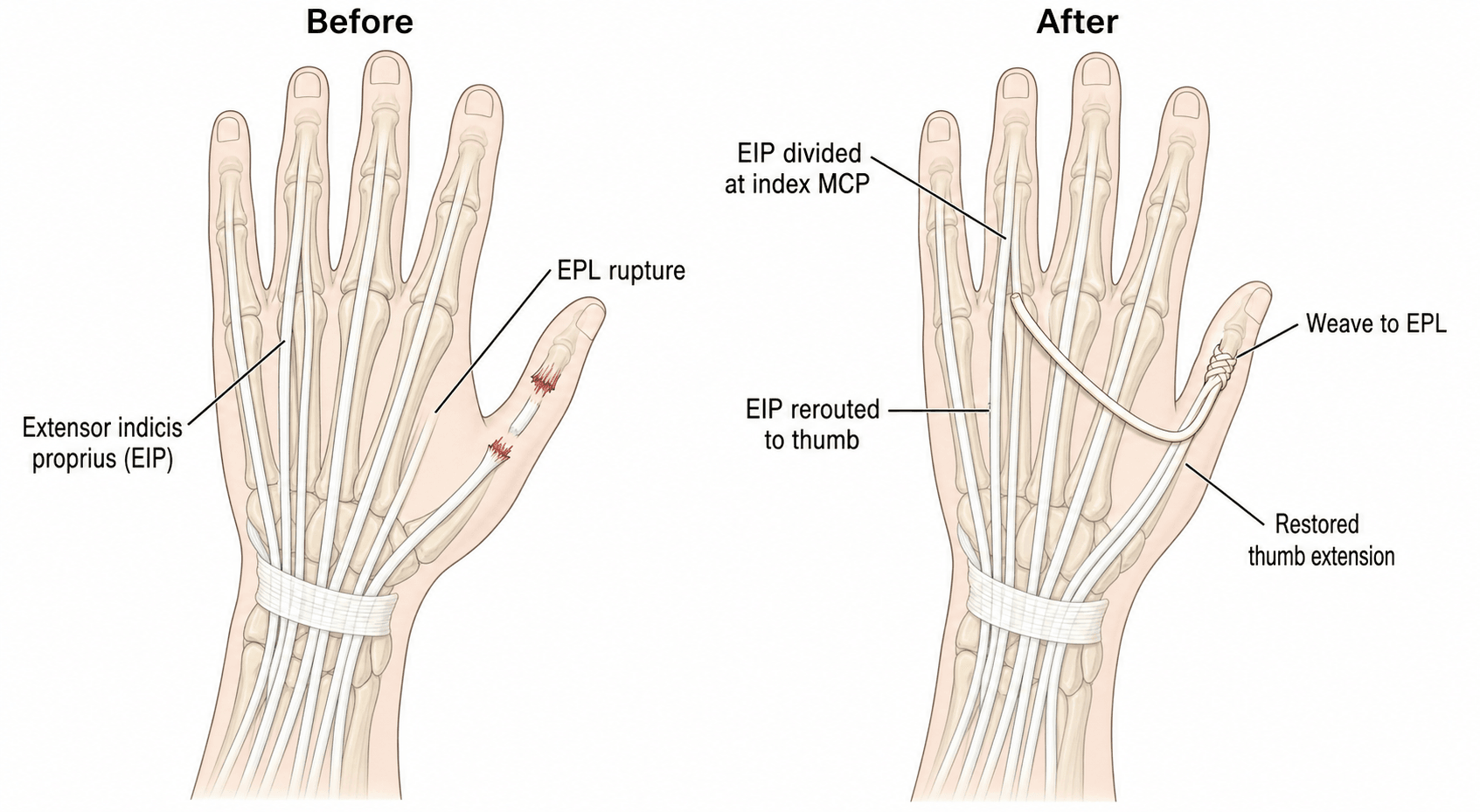
- EIP to EPL transfer is the gold standard for isolated EPL rupture.
- Timing: 3-6 months post-injury for scar maturation before reconstruction.
- Palmaris longus is the first-choice donor for free tendon grafts.
- Pulvertaft weave (3-4 weaves) is the standard tendon attachment technique.
- Vaughan-Jackson syndrome: Sequential ulnar-to-radial extensor ruptures in rheumatoid arthritis.
- “Always assess passive ROM before planning reconstruction
- “Two-stage reconstruction for severe scarring/adhesions
- “Rheumatoid cases require DRUJ synovectomy to prevent recurrence
- “Set tension with wrist neutral, MCP 45 degrees flexion
Reconstruction fails if joints are stiff. Must achieve full passive ROM at all joints before attempting any extensor reconstruction. Release contractures first, reconstruct tendons second.
Gold standard for EPL rupture. EIP is expendable (EDC maintains index extension), has similar excursion to EPL, and provides 90-95% success rate for thumb extension restoration.
Palmaris longus first choice. Present in 85%, provides 12-15cm length, minimal donor morbidity. Alternatives: plantaris (30cm), toe extensors, or ECRL slip.
For severe scarring. Stage 1: Silicone rod creates pseudosheath (3 months). Stage 2: Replace rod with tendon graft. Success rate 70-80% in difficult cases.
Overview and Epidemiology
Extensor tendon reconstruction addresses chronic extensor deficiency through tendon transfers (rerouting expendable donors) or tendon grafts (bridging gaps with free tissue). Success depends on preserved passive joint mobility, appropriate donor selection, proper surgical technique, and intensive hand therapy.
Epidemiology
- Failed primary repairs: 10-15% of acute extensor repairs develop chronic lag
- Delayed presentations: 20-30% of extensor injuries present beyond acute repair window
- Rheumatoid ruptures: Affect 10-15% of RA patients with wrist synovitis
- EPL ruptures post-Colles: 0.5-3% incidence, typically 4-12 weeks post-fracture
- Age distribution: Bimodal - young adults (traumatic), older adults (rheumatoid/atraumatic)
- Gender: Males greater than females for traumatic (3:1), females greater than males for rheumatoid (3:1)
- Occupation: Manual laborers, machinery operators at higher risk for trauma
- Typical Presentation
- Loss of thumb IP extension 4-12 weeks post-fracture
- Preferred Technique
- EIP to EPL transfer
- Typical Presentation
- Progressive loss of finger extension (ulnar to radial)
- Preferred Technique
- Side-to-side transfers, ECRB to EDC
- Typical Presentation
- Chronic extensor lag after laceration repair
- Preferred Technique
- Free tendon graft or two-stage
- Typical Presentation
- Trauma with tissue loss
- Preferred Technique
- Free tendon graft (palmaris longus)
- Typical Presentation
- Adherent extensors, MCP hyperextension
- Preferred Technique
- Tenolysis vs two-stage reconstruction
Natural History Without Reconstruction
- Thumb EPL loss: Inability to extend IP joint, weak pinch, difficulty with precision tasks
- Finger EDC loss: Extensor lag at MCP, compensatory hyperextension at IP joints
- Wrist extensor loss: Wrist drop, severe functional impairment
- Adjacent tendon hypertrophy: Partial compensation from neighboring extensors
- Intrinsic muscle compensation: Limited MCP extension via intrinsics (inadequate)
- Functional adaptation: Activity modification, assistive devices
Pathophysiology and Surgical Anatomy
Cannot reconstruct active extension if passive range is limited. Stiff joints from arthritis, contracture, or adhesions must be addressed first through contracture release, joint mobilization, or arthrodesis. No tendon reconstruction will overcome fixed joint stiffness.
Extensor Anatomy
-
EPL (Extensor Pollicis Longus): Extends thumb IP and MCP joints, radial deviates wrist
- Origin: Ulna mid-shaft, interosseous membrane
- Course: Third dorsal compartment around Lister's tubercle
- Insertion: Distal phalanx base (dorsal)
- Excursion: 5-7cm
-
EPB (Extensor Pollicis Brevis): Extends thumb MCP joint
- First dorsal compartment with APL
- Insertion: Proximal phalanx base
-
APL (Abductor Pollicis Longus): Abducts and extends CMC joint
- First dorsal compartment
- Multiple insertions common
-
EDC (Extensor Digitorum Communis): Common extensor to all four fingers
- Fourth dorsal compartment
- Interconnections via juncturae tendinum
- Independent MCP extension capability
-
EIP (Extensor Indicis Proprius): Independent index extensor
- Fifth dorsal compartment (with EDM)
- Lies ulnar to EDC index at MCP level
- Expendable donor - EDC provides adequate index extension
-
EDM (Extensor Digiti Minimi): Independent small finger extensor
- Fifth dorsal compartment
- Often duplicated
- Partially expendable
- Central slip inserts on middle phalanx base (PIP extension)
- Lateral bands join terminal tendon at DIP (DIP extension)
- Sagittal bands stabilize extensor at MCP (prevent subluxation)
- Intrinsics contribute via lateral bands
Expendable Donor Tendons
- Function Lost
- Independent index extension
- Compensation
- EDC extends index adequately
- Limitations
- None - ideal donor
- Function Lost
- Weak wrist flexion
- Compensation
- FCR/FCU maintain flexion
- Limitations
- Absent in 15%
- Function Lost
- Independent small extension
- Compensation
- EDC extends small finger
- Limitations
- Weakens small finger extension
- Function Lost
- Slight wrist extension loss
- Compensation
- ECRB/ECU maintain extension
- Limitations
- Limited length
- Function Lost
- Trivial plantar flexion loss
- Compensation
- Gastrocnemius/soleus maintain function
- Limitations
- Requires foot incision

Pathophysiology of Extensor Failure
Traumatic Extensor Loss
- Laceration injuries: Clean division allowing primary repair
- Crush/avulsion: Segmental loss requiring grafting
- Degloving: Extensive soft tissue damage, compromised healing
- Closed rupture: Forceful flexion against resistance (Zone V-VII)
- Gap formation: Inadequate repair strength, excessive tension
- Adhesion formation: Insufficient early mobilization, excessive scarring
- Re-rupture: Premature rehabilitation, weak repair construct
- Tendon necrosis: Vascular compromise, infection
- Retraction: Proximal tendon retracts to muscle-tendon junction
- Muscle contracture: Myostatic contracture after 3-6 months
- Distal stump fibrosis: Scar tissue replaces distal tendon
- Joint stiffness: Secondary contractures from prolonged immobility
This pathophysiology necessitates reconstruction rather than delayed primary repair.
Biomechanical Principles
- Finger extensors (EDC): 5-6cm excursion for full MCP-IP motion
- Thumb extensors (EPL): 5-7cm excursion for full MCP-IP motion
- Wrist extensors: 3-4cm excursion for wrist motion
- Match excursion requirements (EIP and EPL both 5-7cm - perfect match)
- Match direction of pull (straight line reduces friction)
- Match muscle strength (adequate motor power)
- Wrist position: Neutral (0 degrees flexion-extension)
- MCP position: 45 degrees flexion for fingers, extended for thumb
- Test intraoperatively: Passive wrist motion should produce reciprocal finger motion (tenodesis effect)
- Avoid over-tensioning: Causes swan-neck deformity, joint stiffness
- Avoid under-tensioning: Results in extensor lag
Classification Systems
Extensor reconstruction is organised by anatomical zone (Kleinert-Verdan, eight zones from DIP to forearm) and by reconstruction strategy. The success-rate ranges below are series-level estimates; the head-to-head Level I comparison of the two commonest strategies (EIP transfer vs free graft for EPL) found equivalent good/very-good outcomes of ~82% and ~88% respectively (According to PubMed, Keating et al, ANZ J Surg 2026, PMID 41797307).
Reconstruction Type Classification
- Technique
- Reroute expendable donor to deficient extensor
- Indications
- Isolated loss, good vascularity, supple joints
- Success Rate
- 85-95%
- Technique
- Bridge gap with palmaris/plantaris
- Indications
- Segmental loss, clean wound
- Success Rate
- 75-85%
- Technique
- Connect adjacent EDC slips
- Indications
- Single EDC rupture with intact neighbors
- Success Rate
- 85-90%
- Technique
- Stage 1: rod; Stage 2: graft
- Indications
- Severe scarring, adhesions, failed prior surgery
- Success Rate
- 70-80%
Boyes Preoperative Grading (Candidacy for Staged Reconstruction)
The two-stage evidence selects "Boyes grade 2-5" digits (PMID 12877856), but the grading itself is never explained. Boyes' classification is the classic preoperative prognostic grading for the digit being considered for tendon-graft / staged reconstruction. It grades the quality of the tissues the graft must heal into and glide through, and so directly predicts outcome and drives the one-stage-versus-two-stage decision and patient counselling.
- State of the digit
- Minimal scar, supple mobile joints, healthy supple skin, well-vascularised bed
- Implication for reconstruction
- Most favourable - single-stage free graft reasonable; best prognosis
- State of the digit
- Heavy skin scarring / multiple prior incisions, scarred tendon bed
- Implication for reconstruction
- Hostile gliding bed - favour two-stage (rod-induced pseudosheath) over single-stage graft
- State of the digit
- Reduced passive joint motion / contracture
- Implication for reconstruction
- Restore full passive ROM first; reconstruction will fail over a stiff joint; guarded prognosis
- State of the digit
- Associated digital nerve injury / insensate digit
- Implication for reconstruction
- Poorer functional return; address sensation and counsel realistically
- State of the digit
- Several digits involved
- Implication for reconstruction
- Greater complexity and worse overall prognosis; stage and prioritise
Boyes' grading was devised for flexor reconstruction candidacy, but the same prognostic logic governs extensor staged reconstruction: the worse the grade (especially scar [2] and joint damage [3]), the stronger the case for a two-stage approach and the more guarded the counselling. This is exactly why the established two-stage series enrolled the poor-prognosis grade 2-5 digits - the favourable grade-1 digit usually does not need a rod.
Before offering a free graft, grade the digit (Boyes): a clean grade-1 bed tolerates a single-stage graft, whereas heavy scar (grade 2) or a stiff joint (grade 3) predicts failure - restore passive ROM first and favour a two-stage rod-then-graft reconstruction. Nerve injury (4) and multiple-digit involvement (5) further worsen prognosis and demand realistic counselling.
Clinical Presentation
History
- Inability to extend specific digit(s) or thumb
- Extensor lag: Incomplete extension despite effort
- Triggering/catching: Suggests adhesions rather than rupture
- Progressive weakness: Rheumatoid pattern
- Acute onset: Laceration, closed rupture (recent trauma)
- Subacute (weeks): Post-Colles EPL rupture (4-12 weeks)
- Progressive (months): Rheumatoid sequential ruptures
- Chronic (greater than 6 months): Failed repairs, late presentation
- Thumb EPL loss: Difficulty with precision pinch, turning keys, opening jars
- Finger EDC loss: Inability to release objects, weak grip, compensatory IP hyperextension
- Multiple digit involvement: Severe hand dysfunction, inability to work
- Prior surgery: Number of procedures, types, outcomes
- Splinting history: Response to dynamic extension splints
- Therapy compliance: Intensive therapy required for success
Physical Examination
- Resting posture: Affected digit(s) in relative flexion
- Surgical scars: Indicate prior attempts, scar quality
- Skin quality: Thin, scarred skin suggests difficult reconstruction
- Muscle wasting: Thenar atrophy (EPL loss), forearm atrophy (long-standing)
- Tendon continuity: Palpate extensor mass during attempted extension
- Present: Thickened cord suggests intact but adherent tendon
- Absent: Gap or no palpable structure confirms rupture
- Distal DRUJ: Dorsal prominence, synovitis (rheumatoid)
- Muscle contraction: Palpable forearm muscle contraction despite no distal motion confirms rupture
Critical Assessment - PASSIVE ROM FIRST:
- PIPJ passive flexion-extension: Must be full (0-100 degrees)
- DIPJ passive flexion-extension: Must be full (0-80 degrees)
- MCP passive flexion-extension: Must be full (0-90 degrees)
- Thumb IP/MCP passive motion: Must be full
- Wrist passive motion: Should be functional (30-60 degrees flexion-extension)
If passive ROM limited - STOP. Address joint stiffness before any tendon work.
- Isolated tendon testing:
- EPL: Extend thumb IP with hand flat on table (positive test = cannot lift thumb)
- EIP: Extend index finger with others flexed and held
- EDC: Extend each finger independently
- Extensor lag measurement: Degrees from full passive extension to active extension
- Compensatory patterns: IP hyperextension, intrinsic recruitment
- Hand flat on table, palm down
- Patient attempts to lift thumb off table
- Positive: Thumb remains flat (EPL ruptured)
- Negative: Thumb lifts easily (EPL intact)
- Immobilize middle, ring fingers in flexion
- Attempt index or small finger extension independently
- Limited extension: Dependent on juncturae (true independent extensor lost)
- Passively extend MCP joint, attempt PIP flexion
- Limited PIP flexion with MCP extended: Intrinsic tightness present
- Differentiate from extensor tightness (limits PIP flexion with MCP flexed)
Differential Diagnosis
The cardinal presentation is loss of active digital extension. The reconstruction plan changes completely depending on which of the following is responsible, so this differential must be worked through systematically before any tendon surgery is offered.
- Key Distinguishing Feature
- Forearm muscle contracts but no distal extension; gap on palpation; tenodesis effect lost
- Pattern of Loss
- Specific tendon(s) - EPL after distal radius fracture, ulnar-to-radial in rheumatoid
- Implication for Reconstruction
- Transfer or graft if passive ROM full
- Key Distinguishing Feature
- Affects ALL digit/thumb extensors plus EDM; radial wrist extension (ECRL) spared so wrist extends in radial deviation; no sensory loss
- Pattern of Loss
- Multiple digits, no palpable gap, passive tenodesis intact
- Implication for Reconstruction
- Treat the nerve first; tendon transfer (e.g. for radial nerve palsy) only if no recovery
- Key Distinguishing Feature
- Extensor slips ulnarly into the valley with MCP flexion; can hold extension if passively centralised; usually middle finger, radial band
- Pattern of Loss
- Single MCP, dynamic
- Implication for Reconstruction
- Sagittal band repair/reconstruction, not tendon transfer
- Key Distinguishing Feature
- Fixed volar subluxation, pain and crepitus, radiographic joint changes
- Pattern of Loss
- MCP-level, often multiple
- Implication for Reconstruction
- Address joint (synovectomy/arthroplasty); tendon rebalancing secondary
- Key Distinguishing Feature
- Passive ROM exceeds active ROM; triggering or thickened cord palpable
- Pattern of Loss
- Tendon present but not gliding
- Implication for Reconstruction
- Tenolysis rather than reconstruction
- Key Distinguishing Feature
- Passive extension itself limited (not just active)
- Pattern of Loss
- Joint-level, fixed
- Implication for Reconstruction
- Release/arthrodesis before any tendon work - reconstruction will fail
According to PubMed, the sagittal band cause is well characterised: Hong et al found that direct sagittal-band repair restored full ROM and normalised DASH scores in chronic MCP extensor subluxation, confirming it is a distinct entity that should not be treated as a tendon rupture (J Hand Surg / Orthopade 2017, PMID 28721447).
Investigations
Imaging
Radiographs (AP, Lateral, Oblique):
Indications: All chronic extensor deficiency cases
Findings to assess:
- Bony prominences: Distal ulna (Vaughan-Jackson), Lister's tubercle (EPL rupture site)
- Malunion: Distal radius dorsal angulation causing tendon attrition
- Hardware: Prominent screws/plates causing mechanical attrition
- Arthritis: DRUJ, wrist, finger joints affecting reconstruction candidacy
- Fracture healing: Confirm union before reconstruction (Colles cases)
Ultrasound:
Indications:
- Confirm rupture vs adhesions
- Locate retracted tendon ends
- Assess tendon quality
Technique: High-frequency linear probe (greater than 10 MHz), dynamic assessment
Findings:
- Complete rupture: Tendon discontinuity, retracted stumps, gap
- Partial rupture: Thinned tendon, partial continuity
- Adhesions: Intact tendon with limited excursion
- Synovitis: Hypoechoic fluid around tendons (rheumatoid)
Advantages: Real-time, dynamic assessment, low cost, no radiation
MRI (T1, T2, STIR sequences):
Indications:
- Uncertain diagnosis
- Pre-operative planning for complex cases
- Assessment of muscle quality (atrophy, fatty infiltration)
- Evaluation of joint pathology
Findings:
- Tendon rupture: Signal discontinuity, tendon retraction, fluid in sheath
- Tendon quality: Thickened (chronic inflammation), thinned (attrition)
- Muscle atrophy: Reduced muscle bulk, T1 hyperintensity (fatty infiltration)
- Synovitis: T2/STIR hyperintensity around DRUJ, wrist
- Scar tissue: T1/T2 hypointensity in tendon bed
Limitations: Expensive, time-consuming, claustrophobia
Electrodiagnostic Studies (EMG/NCS):
Indications: Suspected nerve injury (PIN palsy) masquerading as tendon rupture
Findings:
- PIN palsy: Denervation in all finger/thumb extensors, wrist extensors (ECRB) spared
- Tendon rupture: Normal motor units, voluntary recruitment present
Useful to differentiate neurologic from tendon pathology.
Laboratory Studies
Rheumatoid Cases:
- Inflammatory markers: ESR, CRP (assess disease activity)
- Rheumatoid factor: Confirm RA diagnosis
- Anti-CCP antibodies: More specific for RA
Infection workup (if concerned):
- CBC: Leukocytosis suggests infection
- Blood cultures: If systemic signs
- Wound cultures: If draining sinus
Preoperative Assessment
- Critical: Measure and document passive ROM all joints
- Photography: Consider photos documenting passive motion
- Consent discussion: If passive ROM limited, discuss joint surgery first
- Palmaris longus test: Oppose thumb to small finger, flex wrist - look for central cord
- Present: 85% of population
- Absent: Consider plantaris or ECRL
- EIP presence: Should be present in all patients (very rare congenital absence)
- Skin quality: Thin/scarred skin may require flap coverage
- Previous incisions: Plan incisions to avoid skin necrosis
- Infection history: Delay reconstruction if recent infection
- Occupation: Return to work expectations, timeline
- Hand dominance: Dominant hand may justify more aggressive reconstruction
- Therapy access: Access to certified hand therapist essential
- Compliance: Realistic assessment of ability to follow complex protocol
Management
Do NOT reconstruct before 3 months post-injury - scar tissue must mature. Do NOT delay beyond 6-12 months - muscle contracture and joint stiffness worsen outcomes. Optimal window: 3-6 months.
Non-Operative Management
- Minimal functional deficit (patient acceptance)
- Severe medical comorbidities prohibiting surgery
- Inadequate passive ROM with refusal of joint surgery
- Very elderly/low-demand patients
- Relative indication: Recent rupture (less than 3 months), partial ruptures
- Mechanism: Outrigger provides passive extension force
- Duration: 6-12 weeks continuous wear
- Success: Low for complete ruptures (less than 20%), better for adhesions
- Adaptive equipment (built-up handles, key turners)
- Occupational therapy for compensatory strategies
- Acceptable for low-demand patients
Outcomes: Persistent functional deficit, progressive joint contracture, patient dissatisfaction common
Surgical Reconstruction
Patient Selection Criteria
- Supple joints - Full passive ROM at all involved joints
- Mature scar - Minimum 3 months since injury/prior surgery
- Adequate soft tissue - Healthy skin coverage, no active infection
- Realistic expectations - Understanding of limitations, therapy commitment
- Therapy access - Access to certified hand therapist
- Absolute: Active infection, inadequate passive ROM, unrealistic expectations
- Relative: Severe medical comorbidities, poor soft tissue, smoking (cessation 4 weeks pre-op)
Reconstruction Techniques
EIP to EPL Transfer Technique
Gold Standard for EPL Rupture
- Chronic EPL rupture (post-Colles, rheumatoid, idiopathic)
- Failed EPL primary repair
- EPL loss from trauma
- EIP expendable (EDC provides adequate index extension)
- Similar excursion to EPL (5-7cm)
- Direct line of pull after rerouting
- Excellent success rate (90-95%)
- Supine, arm on hand table
- Tourniquet on upper arm (250 mmHg)
- Hand pronated
- Identify EIP tendon (ulnar to EDC at MCP level)
- Typically both tendons visible to index - EIP is ulnar
- Tag EIP with marking suture
- Divide EIP as distally as possible (at extensor hood)
- Retrieve EIP proximally with traction
- Center over Lister's tubercle
- Extend 4cm proximally over EPL muscle belly
- Identify third dorsal compartment (EPL)
- Open compartment - find EPL distal stump (may be attenuated)
- Trace EPL muscle belly proximally - excise degenerated tendon
- Create subcutaneous tunnel from wrist incision to thumb (radial side)
- Longitudinal over IP joint dorsum
- Identify EPL insertion on distal phalanx base
- Prepare EPL stump by freshening if adequate tissue
- If no distal stump: create bone tunnel in distal phalanx
- Retrieve EIP from index incision into wrist incision
- Pass EIP subcutaneously around radial wrist (mimic EPL course)
- Thread EIP through subcutaneous tunnel to thumb incision
- Weave EIP to EPL stump using Pulvertaft weave:
- Create 4-6mm longitudinal slit in EPL stump
- Pass EIP through slit
- Create second slit 5mm distal, pass EIP through again
- Repeat for 3-4 total weaves
- Suture each weave with 4-0 Ethibond/FiberWire
- Set tension: Wrist neutral, thumb MCP/IP joints extended (can passively flex to neutral)
- Intraoperative test: Passive wrist flexion extends thumb; wrist extension allows thumb flexion
- Trim excess EIP tendon
- Drill 2mm bone tunnel from dorsal to volar distal phalanx base
- Pass EIP through tunnel
- Suture to periosteum or button over volar pulp
- Skin only (5-0 nylon or subcuticular)
- Avoid deep sutures (restrict glide)
- Thumb spica splint
- Wrist 30 degrees extension
- Thumb CMC, MCP, IP extended
- Duration: 4 weeks
This technique provides excellent thumb extension restoration with minimal donor morbidity.
Addressing Underlying Pathology
- DRUJ synovectomy: Remove inflammatory synovium
- Darrach procedure: Distal ulna excision (most common)
- Sauve-Kapandji: DRUJ fusion with proximal pseudarthrosis (preserves stability)
- Failure to address DRUJ: High re-rupture rate (up to 30%)
- Remove prominent hardware: Screws, plates causing mechanical attrition
- Correct malunion: Osteotomy if severe dorsal angulation causing attrition
- Release scar/adhesions: Tenolysis of surrounding structures
- Z-plasties: Lengthen contracted skin
- Skin grafts: Provide adequate soft tissue coverage
- Flap coverage: If deep structures exposed
Free Graft Biology and Why Transfers Beat Grafts
The topic repeatedly states that free grafts do worse than transfers "due to avascularity of graft requiring healing" and that grafts "stretch 10-15% over 3 months," and it justifies the two-stage rod on bed quality - but the underlying graft biology that explains all of this is never developed.
A free tendon graft is transplanted avascular and must be incorporated by the recipient. It heals in a sequence: an early ischaemic phase with partial central necrosis and loss of tenocytes, then revascularisation and cellular repopulation from the surrounding bed (extrinsic) and from synovial-fluid diffusion (intrinsic) over roughly the first 4-6 weeks, followed by remodelling of collagen over months. The graft is weakest during the avascular and early-revascularisation phase, which is why grafts are protected longer and progress more slowly than a transfer.
- A transfer keeps its own blood supply and intact musculotendinous unit - it only has to heal at its juncture(s), so it is stronger earlier and does not depend on revascularisation. This is the biological reason EIP-to-EPL transfer (~90-95%) outperforms free grafting and is the default for irreparable EPL rupture.
- A free graft depends entirely on the recipient bed for revascularisation and gliding. A healthy vascular bed supports incorporation; a densely scarred, avascular bed both starves the graft and binds it in adhesions, which is why single-stage grafting fails in scarred fields.
the silicone rod provokes a smooth, vascularised pseudosheath over ~3 months, so the stage-2 graft is delivered into a gliding, perfusable channel rather than dense scar - converting a hostile (Boyes grade 2) bed into one a graft can survive and glide in.
- Graft stretch / creep (~10-15%) during remodelling - so set tension slightly tighter than desired and expect possible late extensor lag.
- Adhesions are the price of extrinsic (bed-dependent) healing - hence early protected motion to balance graft protection against adhesion formation.
A tendon transfer keeps its blood supply and heals only at the juncture, so it is stronger early and more reliable; a free graft is avascular and must revascularise from the recipient bed over 4-6 weeks, making it weaker early and utterly dependent on bed quality. That single fact explains transfer-over-graft preference, why a scarred bed needs a two-stage rod-induced pseudosheath, the graft's 10-15% stretch, and its higher adhesion/lag rate.
Complications and Salvage
- Incidence
- 15-25%
- Prevention
- Early passive motion, minimize trauma
- Management
- Intensive therapy, tenolysis at 6+ months
- Incidence
- 5-10%
- Prevention
- Adequate immobilization, proper tension
- Management
- Revision reconstruction vs salvage
- Incidence
- 10-20%
- Prevention
- Proper tension setting, compliant therapy
- Management
- Dynamic splinting, revision if greater than 30 degrees
- Incidence
- 15-25%
- Prevention
- Early passive IP motion
- Management
- Aggressive therapy, manipulation, possible release
- Incidence
- 5%
- Prevention
- Avoid over-tensioning
- Management
- PIP extension splinting, release if severe
- Incidence
- Less than 5%
- Prevention
- Careful harvest technique
- Management
- Usually resolves spontaneously
- Incidence
- 2-3%
- Prevention
- Sterile technique, prophylactic antibiotics
- Management
- Antibiotics, possible debridement
- Incidence
- Rare
- Prevention
- Proper tension setting, avoid over-lengthening
- Management
- Revision to adjust length
Tendon Adhesions
Most common complication (15-25% incidence)
- Limited active extension with full passive extension
- Discrepancy between active and passive ROM (greater than 20 degrees)
- Palpable thickening/triggering along tendon course
- Plateau in ROM improvement despite therapy
-
Conservative (first-line):
- Intensive hand therapy (work-hardening protocol)
- Dynamic extension splinting (low-load prolonged stress)
- Tendon gliding exercises, massage, ultrasound therapy
- Duration: 3-6 months trial
-
Surgical Tenolysis:
- Timing: Minimum 6 months post-reconstruction (allow scar maturation)
- Technique: Release adhesions circumferentially around tendon, preserve juncture
- Post-op: Immediate active motion (regional anesthesia catheter for pain control)
- Outcomes: 60-75% improvement in ROM (some recurrent adhesion expected)
Postoperative Management and Rehabilitation
Extensor Reconstruction Rehabilitation Protocol
Splint Type: Dorsal blocking splint or thumb spica (EPL cases)
Position:
- Wrist 30 degrees extension
- MCP 0 degrees extension (fingers) or thumb extended (EPL)
- IP joints free (allow gentle passive motion)
Activity:
- No active extension (protected healing)
- Passive IP/DIP flexion allowed (prevents stiffness)
- Edema control: Elevation, Coban wrapping
Purpose: Protect juncture healing (Pulvertaft weave or bone insertion).
Remove splint for exercises, reapply between sessions
Exercises:
- Place-and-hold: Passively extend digit, actively hold position (10 sec x 10 reps)
- Active extension: Gentle active extension within comfortable range
- Blocking exercises: Isolate MCP extension (hold PIP/DIP in slight flexion)
- Tendon gliding: Hook fist → straight fist → full extension sequence
Activity:
- Light ADLs (eating, grooming)
- NO gripping, NO lifting greater than 500g
Therapist supervision: Essential - prevent over-aggressive motion, monitor for complications.
Discontinue splint (except nighttime if extensor lag present)
Exercises:
- Progressive strengthening: Putty (soft → medium → firm progression)
- Resistance bands: Gentle resistance to extension
- Grip strengthening: Begin gentle grip exercises
- Functional activities: Light work simulation
Activity:
- Return to light work (sedentary jobs)
- Avoid heavy lifting (still less than 5kg)
Monitor: Extensor lag (if increasing, decrease activity intensity).
Unrestricted activity by 10-12 weeks
Goals:
- Full ROM restoration (0-90 degrees MCP, 0-100 degrees PIP)
- Strength 80-90% of contralateral
- No extensor lag (or less than 10 degrees acceptable)
Activity:
- Return to full work duties
- Return to sport (contact sports week 12)
- Heavy lifting permitted
Long-term: Continue strengthening if weakness persists; dynamic splinting if extensor lag greater than 20 degrees.
Protocol Modifications by Reconstruction Type
- Thumb spica splint (wrist, thumb extended)
- Emphasize IP joint motion early (prevent stiffness)
- Begin pinch strengthening week 6
- More conservative progression (graft weaker than transfer initially)
- Extend immobilization to 5 weeks if concerned about healing
- Slower strengthening progression
- Same as free graft protocol
- Higher vigilance for adhesions (aggressive therapy if motion plateaus)
- Consider early tenolysis (6 months) if severe adhesions
- Can be slightly more aggressive (less tension on repair)
- Buddy tape affected and donor digits weeks 4-8
- Independent finger exercises less critical (coupled motion expected)
Monitoring for Complications
- Acceptable: Less than 10 degrees (functional outcome)
- Concerning: 10-20 degrees (may improve with therapy)
- Unacceptable: Greater than 20 degrees (consider revision if persists beyond 3 months)
- Clinical sign: Passive ROM greater than active ROM (discrepancy greater than 20 degrees)
- Management: Intensive hand therapy, dynamic splinting
- Surgical: Tenolysis at 6 months if failed conservative management
- Cause: Over-tensioned reconstruction → MCP hyperextension, PIP flexion
- Prevention: Proper tension setting intraoperatively
- Management: PIP extension splinting; if severe, may need reconstruction release
- Prevention: Early passive IP motion during immobilization phase
- Management: Aggressive therapy, dynamic splinting, manipulation under anesthesia if refractory
Guidelines, Registries & Global Practice
Extensor reconstruction is a technique-driven field without large randomised trials or dedicated joint-registry data; the global standard rests on systematic reviews, case series and biomechanical work. The picture below summarises the worldwide evidence and where regional practice genuinely differs.
Global Epidemiology
- Figure
- ~3.5% in one matched cohort ('hook'-shaped Lister tubercle a risk factor)
- Source
- According to PubMed, Ogata et al, J Hand Surg Asian Pac Vol 2022 (PMID 36178420)
- Figure
- 0% to 12.5% across studies; EPL most commonly affected
- Source
- According to PubMed, Kunes et al, Hand (N Y) 2022 (PMID 35168382)
- Figure
- ~25% bilateral absence in the overall series; unilateral absence commoner on the non-dominant hand
- Source
- According to PubMed, Eric et al, Surg Radiol Anat 2010 (PMID 21107568)
- Figure
- Attritional extensor rupture from DRUJ arthritis/inflammation; persistent functional deficit after surgery despite high satisfaction
- Source
- According to PubMed, McIntyre et al, J Wrist Surg 2024 (PMID 39027023)
Manual occupations (construction, agriculture, machinery) drive traumatic injury worldwide, while inflammatory arthropathy drives atraumatic and attritional rupture. Rheumatoid arthritis prevalence is broadly 0.5-1% globally, so rheumatoid extensor rupture is a comparable problem across health systems.
Guidance and Standard of Care, Side by Side
No society publishes a dedicated extensor-reconstruction guideline; recommendations are extrapolated from hand-surgery consensus and distal-radius-fracture guidance.
- Relevant position
- Recognises EPL rupture as a complication of both non-operative and operative treatment; supports surgical reconstruction (commonly EIP transfer)
- Evidence basis
- Consensus / limited evidence
- Relevant position
- Tendon transfer or graft for irreparable extensor loss with supple joints; certified hand-therapy access central to outcome
- Evidence basis
- Expert consensus
- Relevant position
- EIP transfer and free graft give equivalent functional return for EPL rupture (good/very good in ~82% vs ~88%)
- Evidence basis
- Level I (PMID 41797307)
- Relevant position
- Side-to-side coaptation is at least as strong/stiff as the Pulvertaft weave, supporting earlier active motion
- Evidence basis
- Level V cadaveric (PMID 20223604, 33279324)
Points of genuine agreement: full passive ROM is a mandatory prerequisite; EIP-to-EPL transfer is the default for irreparable EPL rupture; severe scarring is managed in two stages; rheumatoid cases must address the DRUJ to prevent re-rupture.
Registry Evidence
There is no implant or joint registry for soft-tissue extensor reconstruction (no prosthesis is implanted), so registry-level survival data do not exist. The best comparative evidence is the Level I systematic review above plus pooled case series, not registry output - a key honesty point for the exam.
Global Practice Variation
- High- vs limited-resource settings: outcome depends heavily on access to a certified hand therapist; where structured therapy is unavailable, surgeons favour simpler, more robust constructs and may accept earlier arthrodesis for salvage.
- Graft vs transfer preference: equivalent outcomes mean choice is driven by local training and donor availability (palmaris longus absent in roughly a quarter of patients) rather than by superiority of one technique.
- Inflammatory disease: peri-operative immunosuppression is managed with the treating rheumatologist following the prevailing national perioperative guidance (e.g. ACR/EULAR-aligned recommendations), individualised to infection and flare risk; dedicated drug names and hold intervals vary by region and are deliberately not prescribed here.
Across all health systems, the strongest outcomes follow early referral to specialist hand-surgery services and coordinated multidisciplinary care — hand surgeon, certified hand therapist, and rheumatology where relevant.
Surgical Pearls and Pitfalls
Technical Pearls
- Three weaves minimum: Standard secure juncture
- Four weaves typical: Added strength at the cost of more bulk - optimise balance of security vs gliding resistance
- Suture technique: Horizontal mattress preferred over simple sutures (better purchase)
- Taper final end: Smooth transition reduces catching sensation
- Critical determinant of outcome: Over-tension (swan-neck), under-tension (lag)
- Standard position: Wrist neutral, MCP 45 degrees flexion
- Intraoperative test: Passive wrist flexion should extend fingers reciprocally
- Allowance for stretch: Set slightly tighter than desired (grafts stretch 10-15% over 3 months)
- Palmaris identification: Resist thumb opposition against resistance - central cord most prominent
- Tendon stripper use: Requires experience - can transect tendon if improper technique
- Tag orientation: Mark proximal vs distal end (maintain correct orientation during weaving)
- Avoid perpendicular scars: Zigzag or S-incisions prevent contracture
- Respect previous scars: Incorporate when possible, maintain blood supply
- Minimize skin trauma: Careful handling prevents wound complications
Common Pitfalls and Avoidance
- Error: Proceeding despite limited passive ROM
- Consequence: Reconstruction fails, wasted surgery
- Avoidance: Mandatory passive ROM documentation pre-op; release contractures first
- Error: Reconstruction less than 3 months post-injury
- Consequence: Excessive adhesions, poor glide, re-rupture
- Avoidance: Wait 3-6 months unless soft tissues pristine
- Over-tensioning:
- Consequence: Swan-neck deformity, joint stiffness, pain
- Avoidance: Set with MCP 45 degrees flexion, allow passive finger flexion intraoperatively
- Under-tensioning:
- Consequence: Persistent extensor lag, weak extension
- Avoidance: Set tension slightly tighter than desired (accounts for stretch)
- Error: Only 1-2 weaves, or inadequate suturing
- Consequence: Juncture failure, gap formation, rupture
- Avoidance: Minimum 3 weaves, horizontal mattress sutures each weave
- Error: Single-stage graft in severely scarred bed
- Consequence: Massive adhesions, non-functional result
- Avoidance: Two-stage for severe scarring; transfer over graft when possible
- Error: Reconstructing tendons without addressing DRUJ synovitis
- Consequence: Re-rupture rate up to 30%
- Avoidance: ALWAYS perform DRUJ synovectomy + Darrach/S-K in rheumatoid cases
- Error: Too many weaves, bunching of sutures
- Consequence: Adhesions, catching sensation, limited ROM
- Avoidance: Taper final end, trim excess, smooth juncture
Troubleshooting Intraoperative Issues
- Use infant feeding tube as guide
- Create new subcutaneous tunnel if old bed too scarred
- Consider two-stage approach
- Use plantaris (longer than palmaris)
- Use two palmaris grafts end-to-end
- Consider ECRL slip as augmentation
- Rare but possible (congenital absence)
- Use EDC slip to index finger as alternative
- Consider ECRB to EPL if no alternatives
- Anchor graft directly to bone (drill tunnel)
- Use bone anchor or suture anchor
- Button technique over volar pulp
MCQ Practice Points
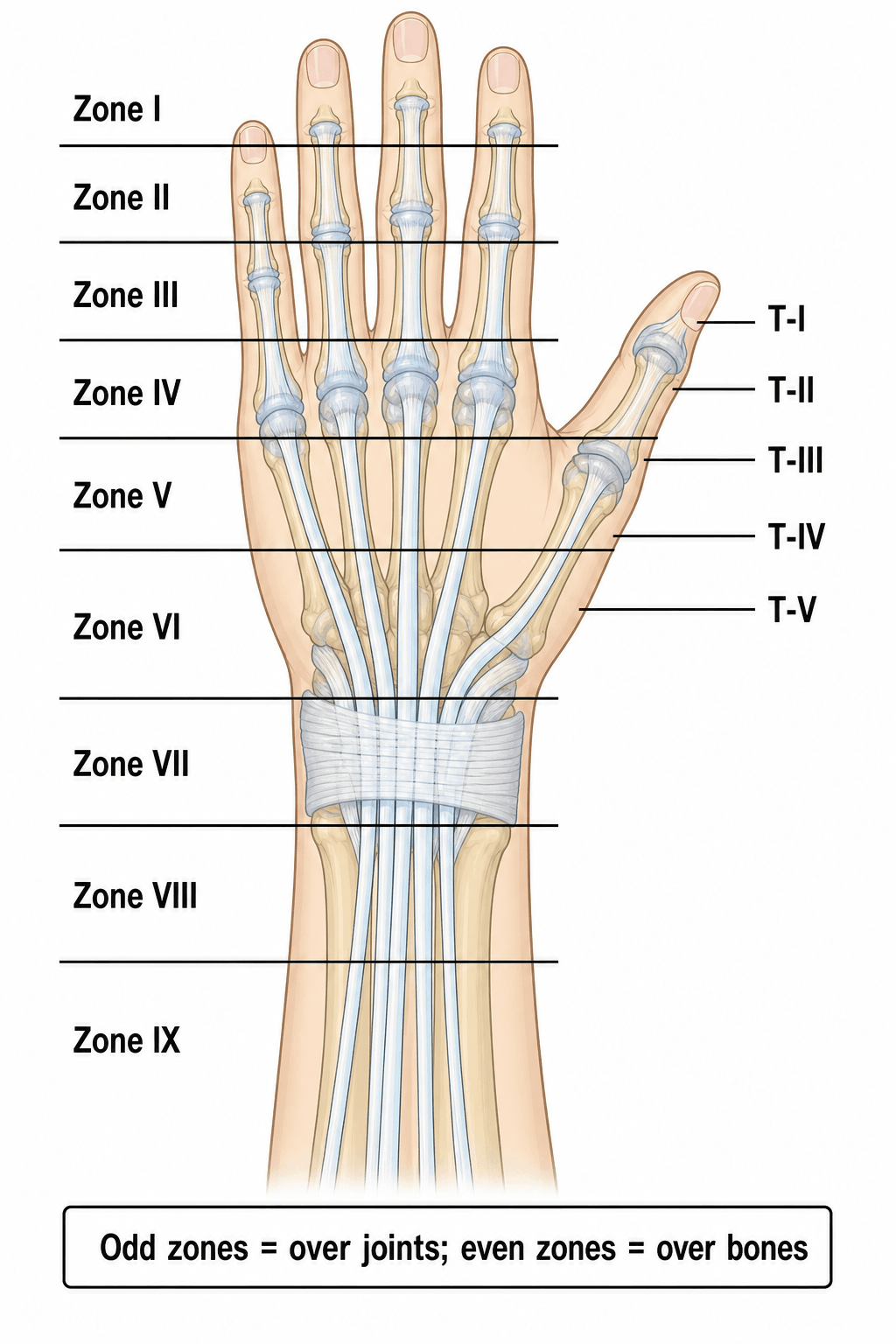
Q: What are the zones of extensor tendon injury in the hand and their significance?
A: Odd zones over joints, even zones between: Zone I (DIP) - mallet finger, Zone III (PIP) - boutonnière, Zone V (MCP) - fight bite location, Zone VII (wrist) - under retinaculum. Zone III injuries risk boutonnière deformity if central slip disrupted. Zone V requires thorough washout for human bite injuries.
Q: What is the EIP to EPL transfer used for?
A: Extensor indicis proprius (EIP) transfer reconstructs extensor pollicis longus (EPL) rupture. Common indication: EPL rupture after distal radius fracture (Lister's tubercle attrition). EIP expendable as EDC provides index extension. Transfer rerouted subcutaneously to EPL insertion. Alternative: palmaris longus graft.
Q: What tendon grafts are available for extensor tendon reconstruction?
A: Palmaris longus (absent in 15%): Ideal length, easy harvest. Plantaris: Longer, useful for multi-digit reconstruction. Toe extensors: EDL to lesser toes. Fascia lata: For larger defects. Graft length should be 10% longer than defect to allow tensioning. Two-stage reconstruction if significant scarring.
Q: What is the mechanism and treatment of sagittal band injury?
A: Sagittal band rupture (usually radial side of middle finger) causes extensor tendon subluxation ulnarly with MCP flexion. Acute injuries: Splinting MCP in extension 4-6 weeks. Chronic injuries: Surgical repair or reconstruction using extensor slip, juncturae tendinum, or capsular flap. Often seen in rheumatoid arthritis.
Q: What is a two-stage tendon reconstruction and when is it indicated?
A: Stage 1: Insert silicone rod to create pseudosheath in scarred bed, allow soft tissue equilibration (2-3 months). Stage 2: Replace rod with tendon graft through formed sheath. Indicated when severe scarring, absent sheath, or poor soft tissue bed precludes primary reconstruction. Maintains gliding channel.
At a Glance
Extensor tendon reconstruction addresses chronic deficiency after failed primary repair or delayed presentation, with full passive ROM as an absolute prerequisite - stiff joints guarantee failure. EIP to EPL transfer is the gold standard for isolated EPL rupture (90-95% success rate), while palmaris longus is the first-choice free graft donor (present in 85%, 12-15cm length). Timing is 3-6 months post-injury for scar maturation. For severe scarring, two-stage reconstruction using a silicone rod to create a pseudosheath yields 70-80% success. In rheumatoid cases (Vaughan-Jackson syndrome), DRUJ synovectomy is mandatory to prevent recurrent ruptures.
DIP-MID-PIP-PROX-MCP-META-WRIST-FOREARMExtensor Zones of the Hand
Hook:Start at the fingertip (DIP) and work proximally to remember extensor zones!
EIP BESTTendon Transfer Donors
Hook:EIP BEST = the best expendable donors for extensor reconstruction!
SMARTReconstruction Prerequisites
Hook:Be SMART before reconstruction - assess all prerequisites carefully!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old woman presents 8 weeks after successful closed reduction and casting of a displaced distal radius fracture. She has sudden onset inability to extend her thumb IP joint that occurred 2 days ago without trauma. Fracture is healed on x-ray. Examination shows inability to actively extend thumb IP joint, but full passive motion. She can palpate EPL muscle contraction in forearm. What is your diagnosis and management?”
“A 58-year-old woman with long-standing rheumatoid arthritis presents with progressive inability to extend her small and ring fingers at the MCP joints over the past 2 months. She has prominent distal ulna dorsally and synovial thickening at the wrist. Examination shows inability to actively extend small and ring finger MCPs, but passive extension is full. Middle finger extension is weak. What is your diagnosis and surgical management?”
“A 35-year-old carpenter had EDC lacerations to index and middle fingers repaired primarily 8 months ago. Despite intensive hand therapy, he has 50 degrees extensor lag at both MCPs. The dorsum has thick, adherent scarring from multiple prior tenolysis procedures. Passive ROM at all joints is full (confirmed 0-90 degrees MCP, 0-100 degrees PIP). He is highly motivated to regain function. What is your management?”
Extensor Zones (Kleinert-Verdan)
- Zone I: DIP joint (mallet)
- Zone II: Middle phalanx
- Zone III: PIP joint (boutonniere)
- Zone IV: Proximal phalanx
- Zone V: MCP joint
- Zone VI: Metacarpal
- Zone VII: Wrist/retinaculum (EPL rupture site)
- Zone VIII: Distal forearm
Reconstruction Prerequisites (SMART)
- Supple joints - full passive ROM mandatory
- Mature scar - wait 3-6 months post-injury
- Adequate soft tissue coverage
- Realistic patient expectations
- Therapy access and commitment
Reconstruction Options
- Tendon transfer: EIP to EPL (90-95% success)
- Free graft: Palmaris longus (75-85%)
- Side-to-side: Adjacent EDC (85-90%)
- Two-stage: Rod then graft for scarring (70-80%)
EIP to EPL Transfer
- Gold standard for EPL rupture
- EIP expendable (EDC extends index)
- Three incisions: index MCP, wrist, thumb IP
- Reroute EIP around radial wrist to EPL
- Pulvertaft weave 3-4 passes
- Tension: wrist neutral, thumb extended
- Splint 4 weeks, success 90-95%
Tendon Graft Donors
- Palmaris longus: 1st choice (12-15cm, 85% present)
- Plantaris: 2nd choice (25-30cm from foot)
- Toe extensors: 3rd choice (8-12cm)
- ECRL slip: Alternative (8-10cm)
Pulvertaft Weave
- Gold standard tendon attachment
- 3 weaves = secure minimum
- 4 weaves = added strength, more bulk
- Horizontal mattress sutures each weave
- Taper final end (reduce bulk)
EPL Rupture Post-Colles
- Incidence: 0.5-3% of distal radius fractures
- Timing: 4-12 weeks post-fracture (delayed)
- Mechanism: Ischemic necrosis at Lister's tubercle
- Presentation: Cannot extend thumb IP, no trauma
- Treatment: EIP to EPL transfer
- Success: 90-95%
Vaughan-Jackson Syndrome
- Sequential extensor ruptures in rheumatoid arthritis
- Sequence: EDM → ring → middle → index → EPL
- Mechanism: Attrition over distal ulna prominence
- Reconstruction: Side-to-side, EIP/EDM transfers, ECRB to EDC
- MUST do DRUJ synovectomy + Darrach/Sauve-Kapandji
- Success: 60-80% (disease progression affects outcome)
Two-Stage Reconstruction
- Indication: Severe scarring/adhesions
- Stage 1: Silicone rod creates pseudosheath
- Wait 3 months minimum (pseudosheath formation)
- Stage 2: Replace rod with tendon graft
- Success: 70-80% (vs 40% single-stage in scar)
Tension Setting
- Most critical technical factor
- Wrist neutral position
- MCP 45 degrees flexion (fingers)
- Thumb extended (EPL reconstruction)
- Test: Passive wrist flexion → finger extension
- Over-tension: Swan-neck deformity
- Under-tension: Extensor lag
Rehabilitation Protocol
- Weeks 0-4: Immobilization (splint)
- Weeks 4-6: Protected active motion
- Weeks 6-8: Strengthening
- Weeks 8-12: Full activity
- Early passive IP motion (prevent stiffness)
Complications
- Adhesions: 15-25% (most common)
- Rupture: 5-10% (revision vs salvage)
- Extensor lag: 10-20% (revise if greater than 30 degrees)
- Swan-neck: 5% (over-tensioning)
- Joint stiffness: 15-25% (aggressive therapy)
Exam High-Yield Facts
- Passive ROM is mandatory prerequisite
- EIP to EPL for isolated EPL rupture
- Palmaris longus first choice graft (85% present)
- Two-stage for severe scarring
- Rheumatoid: Address DRUJ pathology
- Pulvertaft weave: 3-4 passes standard
Outcomes and Evidence Base
Expected Outcomes by Reconstruction Type
- Success Rate
- 90-95%
- Return to Function
- 3-4 months
- Complication Rate
- Less than 10%
- Success Rate
- 75-85%
- Return to Function
- 4-6 months
- Complication Rate
- 15-20%
- Success Rate
- 70-80%
- Return to Function
- 6-9 months
- Complication Rate
- 20-30%
- Success Rate
- 85-90%
- Return to Function
- 3-4 months
- Complication Rate
- 10-15%
- Success Rate
- 60-80%
- Return to Function
- 4-6 months
- Complication Rate
- 20-30%
Prognostic Factors
- Full passive ROM pre-operatively (most critical)
- Clean, well-vascularized soft tissues (traumatic greater than rheumatoid)
- Single tendon reconstruction (multiple tendons worse)
- Transfer over graft (vascularized tissue heals better)
- Patient compliance with therapy (essential)
- Non-smoker (smoking impairs tendon healing)
- Younger age (better healing potential)
- Limited passive ROM pre-op (poor outcomes despite surgery)
- Multiple prior surgeries (scarring, adhesions)
- Rheumatoid arthritis (disease progression)
- Smoking (nicotine impairs healing)
- Diabetes (impaired healing)
- Poor compliance (inadequate therapy)
- Pooled analysis of 9 studies comparing extensor indicis transfer versus free tendon graft for EPL ruptures not amenable to primary repair
- Good or very good Geldmacher scores in 81.8% after extensor indicis transfer
- Good or very good Geldmacher scores in 87.5% after free tendon grafting
- The two techniques gave a practically equivalent return to postoperative function
- Extensor indicis favoured as the more reliable option on theoretical and clinical grounds (no graft donor-bed dependence)
- Seven patients followed long-term after extensor indicis proprius to EPL tendon transfer for fracture-related EPL rupture
- Isolated active index MCP extension preserved in 7/7 (100%) - confirms EIP is expendable
- 6/7 (86%) could extend index MCP and thumb IP against resistance
- Mean thumb IP extension lag only -5 degrees; mean index MCP extension 1 degree
- Mean QuickDASH 16, indicating good patient-reported function
- Twelve cases of Vaughan-Jackson syndrome treated with distal ulna excision (Darrach) plus extensor tendon transfer
- Attritional extensor rupture from distal radioulnar joint arthritis/inflammation - underlying DRUJ pathology addressed in every case
- At mean 53 months: mean PRWHE 34.5, mean QuickDASH 28.2
- Ten of 12 patients satisfied; Net Promoter Score 42 despite residual functional deficit
- Only 2 patients required further surgery (total wrist arthrodesis)
- Two-stage reconstruction in 20 patients (22 digits) with poor-prognosis (Boyes grade 2-5) injuries
- Stage 1 silicone (Hunter) rod creates a gliding pseudosheath; stage 2 passes the graft through that pseudosheath
- Good/excellent results in 82% (Buck-Gramcko) and 73% (modified Strickland) at mean 50-month follow-up
- Results compared favourably with classic Hunter two-stage free-graft reconstruction
- Low rates of post-reconstruction rupture and tenolysis
- Cadaveric comparison of side-to-side cross-stitch repair versus a Pulvertaft (3-incision) weave
- Load at first failure, ultimate load and stiffness were all significantly higher for the side-to-side repair
- Pulvertaft repairs failed by suture knot slipping/pull-through then donor pulling through recipient
- Side-to-side repairs failed by intrasubstance fibre shearing of the donor tendon
- Stronger, stiffer junctures may permit earlier active mobilisation and fewer adhesions
Long-Term Outcomes
- EIP to EPL: 95% maintain functional thumb extension
- Free grafts: 80% maintain functional extension (some stretch/lag)
- Rheumatoid: 70% maintain function (disease progression affects outcome)
- High (greater than 85%) for traumatic cases with successful reconstruction
- Moderate (60-70%) for rheumatoid cases (expectation management critical)
- Low (less than 50%) for failed reconstructions
- Sedentary work: 3-4 months typical
- Manual labor: 4-6 months, may need job modification
- High demand athletes: 6-9 months, some permanent limitation
Evidence Base
Key Evidence for Extensor Tendon Reconstruction
- 100 cadaveric tendons used to compare Pulvertaft weave versus single-pass side-to-side coaptation
- Side-to-side constructs had significantly higher peak load and stiffness than Pulvertaft weave constructs
- Coaptation bulk did not differ between Pulvertaft and side-to-side constructs
- Side-to-side coaptations showed higher peak gliding resistance through tissue planes
- Mesh versus braided suture made no difference to strength, bulk or gliding within a construct group
- Ninety studies reviewed on extensor tendon injury after volar locking plate fixation of distal radius fractures
- Incidence of extensor tendon rupture ranged from 0% to 12.5%
- The extensor pollicis longus is the most commonly ruptured extensor tendon
- Dorsal screw prominence and dorsal fracture fragments are key, partly preventable risk factors
- Hardware removal plus tendon transfer or reconstruction may be required to restore extension
- Bilateral EPL ruptures occurring at the time of bilateral displaced distal radius fractures
- Both fractures fixed via volar Henry approach with bilateral volar plating
- Both EPL ruptures reconstructed with extensor indicis proprius tendon transfer
- Satisfactory thumb extension restored with no reported complications
- Demonstrates EPL rupture can occur acutely at injury, not only as the classic delayed (4-12 week) attritional rupture