Post-Traumatic Embolic Phenomenon | Gurd Criteria | Preventable with Early Fixation
- Fat emboli from marrow enter venous circulation after long-bone or pelvic fractures
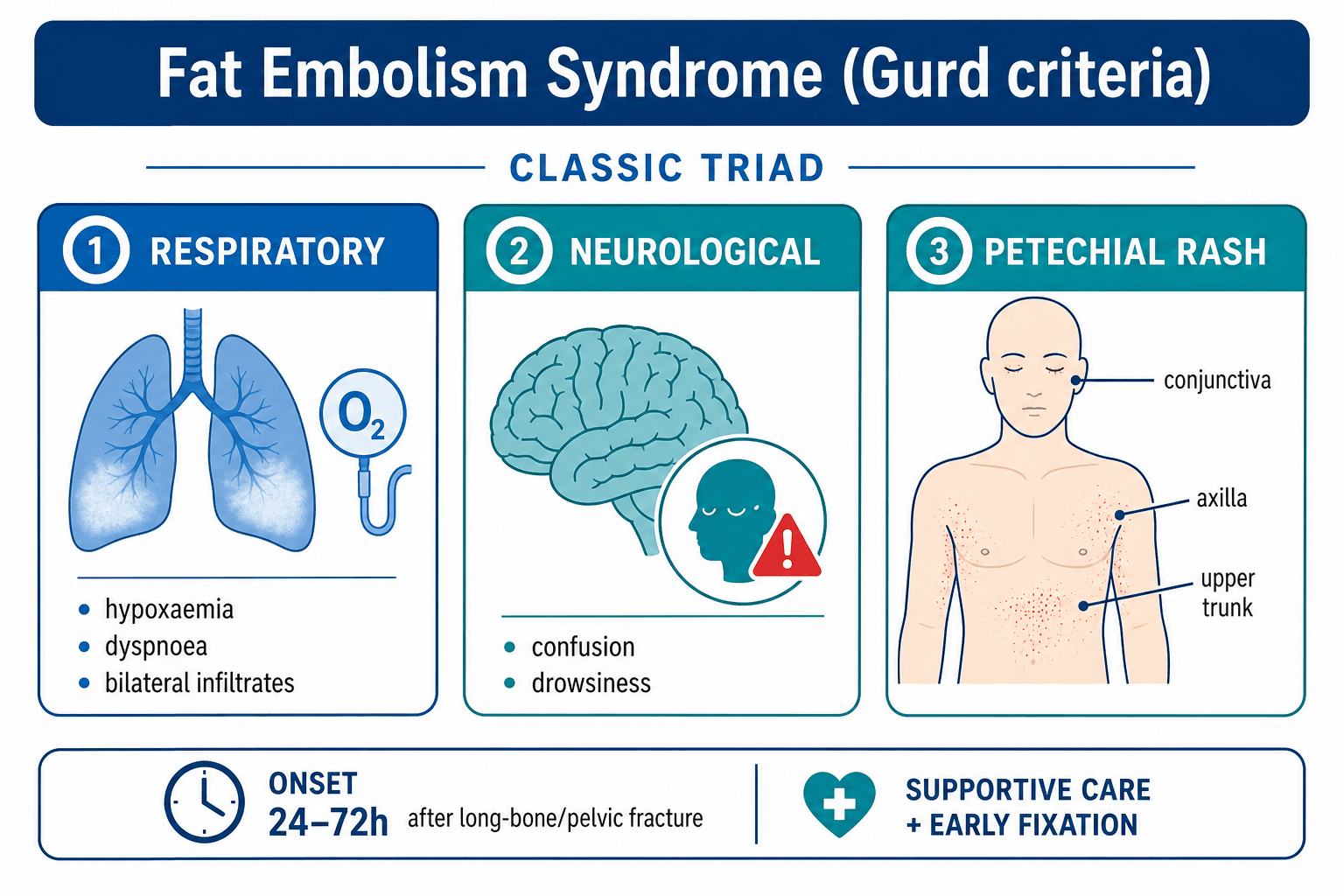
- Classic triad: hypoxia, petechiae, altered mental status appearing 24-72 hours post-injury
- Gurd criteria require one major + four minor features for clinical diagnosis
- Early definitive fixation of fractures within 24 hours reduces incidence
- Management is entirely supportive; no specific pharmacological therapy alters course
- “Petechial rash in axillae or conjunctivae is virtually diagnostic when present
- “Differential includes pulmonary embolism, pneumonia, fat vs thrombus embolus
- “Prophylactic steroids or heparin have no proven benefit in prevention
- “Monitor for ARDS progression and right heart strain in severe cases
Latency 24-72 hours post-injury. Earliest signs may appear at 12 hours but classic presentation is day 2-3. Always reassess multiply-injured patients on day 2-3 for new hypoxia or confusion.
Respiratory distress, petechial rash, neurological abnormality. One major criterion plus four minor criteria establishes clinical diagnosis. Petechiae are pathognomonic when present in the axillary distribution.
Early fracture stabilisation within 24 hours. Delayed fixation allows ongoing fat embolisation from mobile fracture sites. Damage-control orthopaedics followed by early definitive fixation is the evidence-based strategy.
Oxygenation, fluid balance, early ventilation if needed. No specific antidote exists. Avoid over-resuscitation that worsens pulmonary oedema. Monitor for progression to fulminant ARDS.
- Diagnosis
- Gurd criteria positive, petechiae present
- Treatment
- High-flow oxygen, ICU monitoring
- Key Pearl
- Early fixation prevents most cases
- Diagnosis
- Exclude head injury, positive Gurd
- Treatment
- Ventilatory support, supportive care
- Key Pearl
- Deterioration can be rapid to ARDS
- Diagnosis
- High risk if fixation postponed
- Treatment
- Urgent stabilisation, supportive
- Key Pearl
- Timing of surgery is modifiable risk
FRACTURERisk Factors for FES
Hook:FRACTURE reminds you which injury patterns and management decisions drive fat embolism risk!
Overview and Epidemiology
Fat embolism syndrome remains a leading cause of preventable morbidity and mortality in young trauma patients with long-bone fractures. Although rare in absolute terms, the condition is almost entirely preventable by timely fracture stabilisation. Recognition within the 24-72 hour window allows supportive measures to be instituted before progression to fulminant respiratory failure or irreversible neurological injury.
- Long-bone fractures: Femur, tibia, humerus most common
- Pelvic and acetabular fractures: Large marrow volume exposed
- Intramedullary nailing: Reaming and instrumentation force fat into veins
- Closed fractures: Higher intramedullary pressure than open injuries
- Respiratory failure: Progression to ARDS in severe cases
- Neurological sequelae: Cognitive impairment, focal deficits, coma
- Mortality: Up to 10-20 percent in fulminant cases
- Preventable: Early fixation reduces incidence by over 50 percent
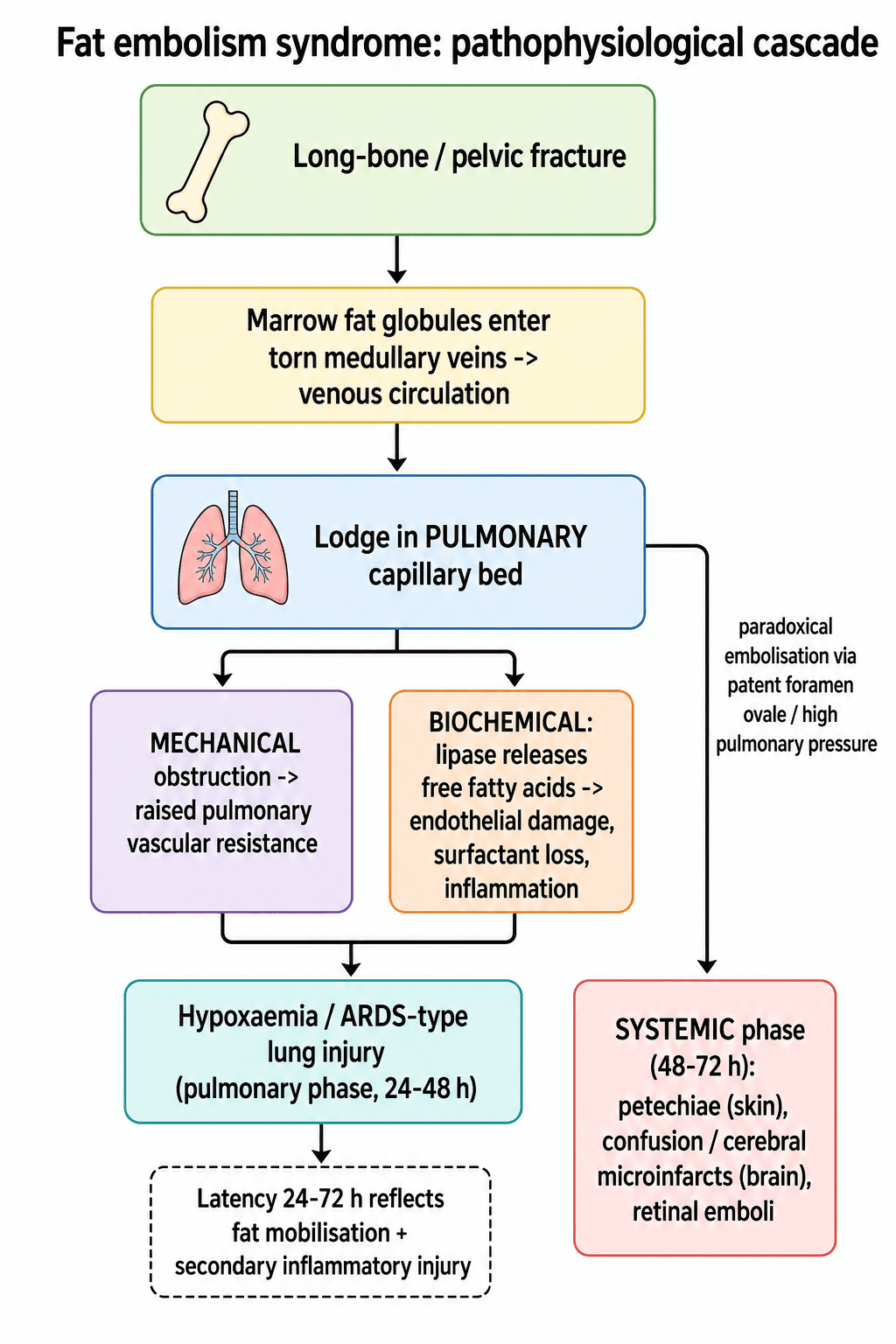
Pathophysiology
Fat globules from bone marrow enter the venous circulation through torn medullary veins at the fracture site. These emboli travel to the pulmonary capillary bed causing mechanical obstruction, chemical pneumonitis from free fatty acids, and activation of inflammatory cascades. In patients with patent foramen ovale or high pulmonary pressures, paradoxical embolisation to systemic circulation produces the characteristic petechiae and cerebral manifestations. The 24-72 hour latency reflects the time required for fat mobilisation, embolisation, and secondary inflammatory lung injury.
- Events
- Fat globules enter venous system
- Clinical Manifestation
- Often subclinical initially
- Time Course
- Immediate to hours
- Events
- Mechanical block plus chemical injury
- Clinical Manifestation
- Hypoxia, tachypnoea, infiltrates
- Time Course
- 24-48 hours
- Events
- Paradoxical emboli, inflammation
- Clinical Manifestation
- Petechiae, confusion, petechial rash
- Time Course
- 48-72 hours
Mechanical obstruction of pulmonary capillaries raises pulmonary vascular resistance. Free fatty acids released by lipase cause direct endothelial damage and surfactant inactivation. Inflammatory cascade produces capillary leak and ARDS picture. V/Q mismatch leads to refractory hypoxia.
Petechial rash results from dermal capillary occlusion and thrombocytopenia. Cerebral emboli produce microinfarcts visible on MRI as diffuse white-matter lesions. Retinal emboli may be seen on fundoscopy (Purtscher retinopathy). Right heart strain occurs with massive pulmonary embolus load.
Classification and Types
Gurd Diagnostic Criteria (Clinical Diagnosis)
- Feature
- Respiratory distress
- Diagnostic Weight
- One major required
- Clinical Note
- Hypoxia less than 60 mmHg on room air
- Feature
- Petechial rash
- Diagnostic Weight
- One major required
- Clinical Note
- Axilla, chest, conjunctiva classic
- Feature
- Neurological change
- Diagnostic Weight
- One major required
- Clinical Note
- Confusion most common, focal signs possible
- Feature
- Tachycardia greater than 110
- Diagnostic Weight
- Four minor needed
- Clinical Note
- Nonspecific but supportive
- Feature
- Pyrexia greater than 38.5 C
- Diagnostic Weight
- Four minor needed
- Clinical Note
- Common in trauma, low specificity
- Feature
- Thrombocytopenia
- Diagnostic Weight
- Four minor needed
- Clinical Note
- Platelets less than 150 times 10 to the 9
- Feature
- Fat macroglobulinaemia
- Diagnostic Weight
- Four minor needed
- Clinical Note
- Urine or sputum fat globules
- Feature
- Renal involvement
- Diagnostic Weight
- Four minor needed
- Clinical Note
- Oliguria, fat in urine
- Feature
- Jaundice
- Diagnostic Weight
- Four minor needed
- Clinical Note
- Hepatic involvement
- Feature
- Retinal emboli
- Diagnostic Weight
- Four minor needed
- Clinical Note
- Purtscher retinopathy on fundoscopy
Diagnosis requires one major criterion plus four minor criteria. Petechiae are the most specific finding.
Clinical Assessment
- Injury pattern: Long-bone, pelvic, or multiple fractures
- Timing: Exact time of injury and any surgical intervention
- Symptoms onset: Precise timing of hypoxia, confusion, rash
- Risk modifiers: Age, closed vs open fracture, reaming performed
- Respiratory: Tachypnoea, hypoxia, bilateral crackles
- Skin: Diligent search for axillary or conjunctival petechiae
- Neurological: GCS, focal deficits, confusion level
- Fracture sites: Stability, swelling, any ongoing manipulation
Technique: Examine axillae, upper chest, and conjunctivae under good light. The rash appears as fine petechiae 1-2 mm in diameter, often in crops, and may be transient.
Interpretation: When present with hypoxia and neurological change after long-bone fracture, the diagnosis of fat embolism syndrome is virtually certain. Absence does not exclude the diagnosis.
Key point: The rash is caused by dermal capillary occlusion and associated thrombocytopenia; it typically resolves within 5-7 days.
- Distinguishing Features
- 24-72 h latency, petechiae, long-bone fracture
- Key Discriminator
- Axillary petechiae + Gurd criteria
- Investigation
- Clinical diagnosis, CT chest, echo
- Distinguishing Features
- Earlier onset possible, risk factors for VTE
- Key Discriminator
- No petechiae, D-dimer, CT pulmonary angiogram
- Investigation
- CTPA
- Distinguishing Features
- Focal signs, fever pattern, aspiration history
- Key Discriminator
- Unilateral findings, sputum culture
- Investigation
- Chest X-ray, sputum
- Distinguishing Features
- Immediate onset, focal neurology, external signs
- Key Discriminator
- No latency, CT head positive
- Investigation
- CT brain
- Distinguishing Features
- Within 6 hours of transfusion
- Key Discriminator
- Transfusion history, no fracture relation
- Investigation
- Clinical timing
The petechial rash is often missed because it is transient and requires deliberate inspection of the axillae and conjunctivae. In any patient with long-bone fracture who develops hypoxia or confusion on day 2 or 3, perform a targeted skin and eye examination before attributing symptoms to atelectasis or head injury.
Alternative Diagnostic Criteria
The Gurd (and Gurd and Wilson) criteria are the most widely used, but they are not the only system, and examiners often ask what else exists. All are clinical, all overlap, and none has been validated as superior; they are best understood as different ways of weighting the same features.
- Basis
- Major (respiratory distress, petechiae, cerebral signs) plus minor (tachycardia, pyrexia, thrombocytopenia, fat macroglobulinaemia, retinal/renal/jaundice changes)
- Threshold / key point
- One major plus four minor features; the most cited system
- Basis
- Respiratory parameters alone in a long-bone-fracture patient
- Threshold / key point
- Sustained PaO2 under 60 mmHg, PaCO2 over 55 mmHg or pH under 7.3, respiratory rate over 35 despite sedation, and increased work of breathing - argues FES can be diagnosed on respiratory deterioration alone
- Basis
- Weighted point score of clinical features
- Threshold / key point
- Petechiae 5, diffuse infiltrates 4, hypoxaemia 3, then confusion, fever, tachycardia and tachypnoea 1 each; a cumulative score of 5 or more suggests FES
If asked for an alternative to the Gurd criteria, the Lindeque criteria are the most useful answer: they make the point that a sustained, unexplained respiratory deterioration after a long-bone fracture can itself be sufficient to diagnose fat embolism syndrome, even before petechiae or confusion appear.
RPNGurd Major Criteria
Hook:Remember the three pillars of fat embolism diagnosis: Respiratory failure, Petechial rash, Neurological change!
Investigations
Investigation Sequence
Indication: Any suspicion of hypoxia or tachypnoea Findings: PaO2 less than 60 mmHg on room air, widened A-a gradient, respiratory alkalosis initially Action: Quantifies severity and guides oxygen therapy
Views: PA or AP erect Look for: Bilateral diffuse infiltrates, "snowstorm" appearance classic but uncommon Clinical correlation: May be normal early; changes lag behind clinical hypoxia
Tests: Full blood count (thrombocytopenia), coagulation, renal and liver function, lipase if available Findings: Platelets often less than 150 times 10 to the 9, fat globules in urine or sputum (low sensitivity) Action: Supports minor Gurd criteria
Indication: To exclude thromboembolic PE or assess right heart strain Findings: Fat emboli not visible on CTPA; RV dilation suggests massive load Action: Guides ICU escalation and rules out treatable differentials
Indication: Focal signs or persistent coma after exclusion of head injury Findings: Diffuse white-matter hyperintensities on T2 MRI consistent with microemboli Action: Supports diagnosis and prognostication
Chest X-ray and CT are supportive but never diagnostic in isolation. The diagnosis of fat embolism syndrome is clinical using Gurd criteria. Do not delay supportive care while awaiting advanced imaging. Early fixation decisions are based on fracture pattern and physiological stability, not on imaging confirmation of emboli.
Cerebral Fat Embolism
A subset of patients present with neurological features predominating, sometimes with little or no respiratory compromise - cerebral fat embolism. It is easily mistaken for traumatic brain injury, sedation, hyponatraemia or sepsis, so it must be actively considered in a long-bone-fracture patient who becomes confused or drowsy on day 2 to 3.
- Finding
- Fluctuating consciousness, confusion, drowsiness, seizures or focal deficits, occasionally coma; may precede or occur without the pulmonary phase
- Significance
- Neurological-predominant FES is under-recognised because the chest can look well
- Finding
- Numerous small foci of restricted diffusion on DWI scattered through the white matter - the 'starfield' pattern - with T2/FLAIR white-matter hyperintensities
- Significance
- More specific than the T2 changes alone and helps separate it from diffuse axonal injury
- Finding
- Paradoxical embolisation through a patent foramen ovale or across the pulmonary bed at high pressure
- Significance
- Explains systemic (cerebral and cutaneous) involvement
- Finding
- Often good neurological recovery with supportive care despite a dramatic presentation
- Significance
- Supports aggressive supportive management rather than nihilism
On diffusion-weighted MRI, cerebral fat embolism produces multiple tiny scattered foci of restricted diffusion throughout the white matter - the 'starfield' appearance - reflecting microembolic infarcts. Recognising this pattern in a confused long-bone-fracture patient supports the diagnosis and, importantly, predicts that good recovery is still likely with supportive care.
Management Algorithm
Prevention Through Early Fixation
Goal: Reduce incidence by stabilising fracture sites before ongoing fat embolisation occurs
Prevention Protocol
Splint fractures: Reduces motion and further embolisation Avoid excessive manipulation: Log-roll carefully, limit reductions Plan surgery early: Book theatre within 24 hours if physiologically stable
External fixation or traction: For unstable patients (damage-control orthopaedics) Physiological optimisation: Correct acidosis, hypothermia, coagulopathy Monitor closely: Serial observations for early signs of FES
Early total care: Convert to intramedullary nail or plate when safe Reaming considerations: Use unreamed nails or ream gently in high-risk patients Post-op monitoring: Continue vigilance for 72 hours
Multiple studies demonstrate that definitive fixation within 24 hours of injury significantly reduces the incidence of fat embolism syndrome compared with delayed fixation. In polytrauma patients too unstable for early total care, damage-control external fixation followed by conversion within 5-7 days still lowers risk compared with prolonged traction.
SUPPORTManagement Priorities
Hook:SUPPORT captures the entirely supportive, multidisciplinary approach required in fat embolism syndrome!
Complications
- Incidence
- Up to 30 percent of moderate-severe cases
- Risk Factors
- Delayed fixation, large marrow volume, young age
- Management
- Mechanical ventilation, prone positioning if refractory
- Incidence
- 10-20 percent of those with CNS involvement
- Risk Factors
- Severe or prolonged hypoxaemia, large embolus load
- Management
- Neurorehabilitation, supportive care
- Incidence
- Rare but life-threatening
- Risk Factors
- Massive pulmonary embolus load, pre-existing pulmonary hypertension
- Management
- Inotropes, pulmonary vasodilators, ECMO in extreme cases
- Incidence
- Common minor criterion
- Risk Factors
- Consumptive process from emboli
- Management
- Supportive, avoid unnecessary transfusions
- Incidence
- 5-20 percent depending on severity
- Risk Factors
- Fulminant presentation, delayed recognition, comorbidities
- Management
- Prevention is the only effective strategy
The single most effective intervention to reduce complications from fat embolism syndrome is early definitive fracture fixation within 24 hours whenever the patient's physiological state permits. Once the syndrome is established, management is supportive only and mortality rises sharply with progression to fulminant ARDS or coma.
Outcomes and Prognosis
- Intervention
- Definitive stabilisation promptly
- Expected Outcome
- FES incidence reduced by greater than 50 percent
- Long-term Impact
- Minimal long-term sequelae in most
- Intervention
- Oxygen, monitoring, fracture fixation
- Expected Outcome
- Full recovery in 70-80 percent
- Long-term Impact
- Possible mild cognitive or respiratory limitation
- Intervention
- Ventilation, advanced therapies
- Expected Outcome
- Mortality 10-20 percent, survivors may have deficits
- Long-term Impact
- Neurorehabilitation often required
Best prognosis: Early recognition, prompt supportive care, fracture stabilisation achieved, young patient without comorbidities. Poor prognosis: Delayed diagnosis beyond 72 hours, progression to refractory ARDS, pre-existing lung disease, massive head injury coexisting. Key modifiable factor: Timing of fracture fixation remains the only evidence-based intervention that meaningfully alters incidence and therefore outcome.
Guidelines, Registries & Global Practice
- Long-bone fractures account for the majority of FES cases worldwide, with femur fractures carrying the highest risk
- Incidence ranges from 1-3 percent after isolated femur fracture to 5-10 percent in polytrauma with multiple long bones
- Young adults (15-40 years) predominate because of higher marrow fat content and greater exposure to high-energy trauma
- Resource-limited settings see higher rates when early fixation is delayed by operating theatre access or transfer logistics
- High-resource centres: 24-hour trauma theatres, damage-control protocols, immediate ICU availability, routine early total care
- Limited-resource environments: Prolonged traction or external fixation common, delayed definitive nailing, higher FES incidence
- Universal principle: The earlier fracture stability is achieved, the lower the embolus load, regardless of implant type
- Registry data: No dedicated FES registry exists; incidence inferred from trauma databases and orthopaedic registries
- Diagnosis emphasis
- Clinical Gurd criteria; imaging supportive only
- Prevention priority
- Early definitive fixation within 24 hours when safe
- Supportive care
- Oxygenation, ventilation, fluid balance; no specific drugs
- Diagnosis emphasis
- High index of suspicion in long-bone fractures on day 2-3
- Prevention priority
- Damage-control orthopaedics followed by early conversion
- Supportive care
- ICU-led supportive care; avoid over-resuscitation
- Diagnosis emphasis
- Gurd criteria remain diagnostic standard
- Prevention priority
- Early stabilisation reduces pulmonary complications
- Supportive care
- Mechanical ventilation per ARDSNet protocol if required
- Diagnosis emphasis
- Clinical diagnosis; petechiae highly specific
- Prevention priority
- Timing of surgery is the key modifiable risk factor
- Supportive care
- Multidisciplinary trauma-ICU-ortho collaboration essential
No international registry specifically tracks fat embolism syndrome. Incidence and outcomes are derived from large trauma databases (e.g., NTDB, TARN) and orthopaedic registries (NJR, AJRR) that capture fracture fixation timing and pulmonary complications. Evidence consistently shows that early fracture stabilisation is the only intervention with a measurable preventive effect.
Record in every long-bone fracture patient:
- Time of injury and time of definitive fixation
- Daily respiratory observations and oxygen requirements on days 1-3
- Presence or absence of axillary or conjunctival petechiae
- Neurological status on day 2-3
- Gurd criteria checklist if any suspicion arises
Missed or delayed diagnosis of fat embolism syndrome in a young trauma patient is a recurring source of morbidity and occasional mortality worldwide. Early fixation and vigilant monitoring on days 2-3 are the global standard of care.
Controversies & Areas of Uncertainty
Reaming increases intramedullary pressure and produces a transient shower of emboli. However, large trials show no significant difference in clinically important fat embolism syndrome rates between reamed and unreamed nails when fixation occurs early. Choice is dictated by fracture pattern and surgeon preference rather than FES prevention.
Older trials suggested high-dose methylprednisolone might reduce inflammatory response, but modern systematic reviews find no improvement in clinical outcomes or mortality. Current guidelines do not recommend routine prophylactic steroids for FES prevention.
The precise threshold at which a borderline polytrauma patient should undergo conversion from damage-control external fixation to definitive nailing remains debated. Physiological parameters (lactate clearance, base deficit, temperature, coagulation) guide individualised decisions rather than a fixed time cut-off.
Routine preoperative echocardiography to detect patent foramen ovale is not justified. In established fulminant FES with right heart strain, echocardiography guides haemodynamic management but does not alter the supportive treatment paradigm.
MCQ Practice Points
Q: What is the primary route by which fat enters the circulation in long-bone fractures? A: Torn medullary veins at the fracture site allow marrow fat to enter the venous system under elevated intramedullary pressure. Reaming and instrumentation further increase this pressure and embolus load.
Q: What are the three major Gurd criteria required for clinical diagnosis of fat embolism syndrome? A: Respiratory distress (hypoxia, tachypnoea, bilateral infiltrates), petechial rash (typically axillary or conjunctival), and neurological abnormality (confusion, drowsiness, focal deficit). One major plus four minor criteria establish the diagnosis.
Q: What is the typical latency period between injury and onset of fat embolism syndrome? A: 24-72 hours after injury. Earliest manifestations may appear at 12 hours, but the classic presentation occurs on the second or third day. Onset after 96 hours is unusual unless fracture sites remain unstable.
Q: What is the single most effective intervention to reduce the incidence of fat embolism syndrome? A: Early definitive fracture fixation within 24 hours of injury whenever the patient's physiological condition permits. Damage-control external fixation followed by conversion within days is an acceptable alternative in unstable polytrauma patients.
Q: What is the mainstay of treatment once fat embolism syndrome is diagnosed? A: Entirely supportive care: oxygen or mechanical ventilation to maintain oxygenation, careful fluid management, fracture stabilisation, and prevention of secondary organ injury. No pharmacological agent has proven benefit.
Q: What is the approximate mortality rate in fulminant fat embolism syndrome progressing to ARDS? A: 10-20 percent. Survivors of severe cases may have residual cognitive or respiratory impairment requiring rehabilitation. Prevention through early fixation remains far more effective than treatment.
Clinical Imaging
Imaging Findings in Fat Embolism Syndrome
Chest radiographs typically show bilateral diffuse infiltrates resembling ARDS or pulmonary oedema. High-resolution CT may demonstrate ground-glass opacities and centrilobular nodules. MRI brain can reveal diffuse white-matter hyperintensities on T2-weighted sequences consistent with embolic microinfarcts. Echocardiography may show right ventricular strain or patent foramen ovale facilitating paradoxical emboli. Imaging supports clinical diagnosis but is never pathognomonic; the diagnosis remains clinical.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old motorcyclist sustains an isolated closed midshaft femur fracture. He undergoes intramedullary nailing 18 hours after injury. On the second postoperative day he develops tachypnoea, hypoxia requiring 6 L oxygen, and mild confusion. Axillary petechiae are noted on examination. What is your diagnosis and immediate management?”
“A 32-year-old with bilateral femur fractures and an unstable pelvic ring injury undergoes damage-control external fixation on day 1 because of hypotension and acidosis. On day 3 he is still in the ICU, now with refractory hypoxia on 100 percent oxygen, bilateral infiltrates, petechial rash, and GCS 10. The orthopaedic team asks whether to proceed with conversion to definitive fixation. What is your recommendation?”
Key Pathophysiology
- Fat from marrow enters venous circulation via torn medullary veins after long-bone or pelvic fracture
- Latency 24-72 hours reflects embolisation plus secondary chemical pneumonitis from free fatty acids
- Pulmonary capillary obstruction plus inflammation produces ARDS-like picture
- Paradoxical emboli through PFO or high pulmonary pressure cause systemic petechiae and cerebral effects
Gurd Diagnostic Criteria
- Major (one required): respiratory distress, petechial rash, neurological change
- Minor (four required): tachycardia, pyrexia, thrombocytopenia, fat globules, renal involvement, jaundice, retinal emboli
- Petechiae in axillae or conjunctivae are the most specific physical finding
- Diagnosis is clinical; imaging and labs support but do not confirm
Prevention Strategy
- Early definitive fixation within 24 hours reduces incidence by greater than 50 percent
- Damage-control external fixation in unstable patients followed by conversion within days
- Avoid excessive fracture manipulation and prolonged traction
- No pharmacological prophylaxis (steroids, heparin) has proven benefit
Supportive Management
- Oxygen or mechanical ventilation targeting SpO2 greater than 92 percent
- Low-tidal-volume ventilation (6 mL/kg) if ARDS develops
- Careful fluid balance to avoid worsening pulmonary oedema
- Fracture stabilisation once physiologically optimised
Prognosis and Key Thresholds
- Mortality 10-20 percent in fulminant cases progressing to ARDS or coma
- Most moderate cases recover fully with supportive care
- Early fixation is the only evidence-based intervention that alters incidence
- Residual cognitive or respiratory impairment possible in severe survivors
Evidence Base and Key Trials
Fat embolism: an aid to diagnosis
- Original description of clinical diagnostic criteria still used today
- Major criteria (respiratory, neurological, petechial) plus minor laboratory and clinical features
- Emphasised the 24-72 hour latency and association with long-bone fractures
- Highlighted that petechiae are the most specific physical sign
Early versus delayed stabilization of femoral fractures. A prospective randomized study.
- Prospective randomised study of 178 patients comparing early versus delayed femoral-fracture stabilisation
- In multiply-injured patients, DELAYED fixation gave a higher incidence of pulmonary complications (ARDS, fat embolism, pneumonia), longer hospital stay and more ICU days
- Hospital cost was significantly higher with delayed treatment for all patients
- Established the principle that early fracture stabilisation improves pulmonary outcomes in polytrauma
Fat embolism in patients with multiple injuries
- Early surgical stabilisation in polytrauma patients markedly reduced fat embolism incidence
- Benefit of prompt fixation demonstrated in patients with multiple long-bone injuries
Post-traumatic fat embolism syndrome
- Clinical presentation and management of post-traumatic FES in a modern case series
- Supports Gurd criteria and supportive care approach in resource-variable settings