Femoral Nerve Anatomy
The nerve is vulnerable in anterior-approach THA (retractor over the anterior acetabular rim), acetabular/pelvic fracture surgery, inguinal and pelvic procedures, and from excessive leg lengthening. Cadaveric work shows it lies closest to the anterior rim at the 90° position.
Iliacus or retroperitoneal haematoma (anticoagulation, haemophilia) compresses the nerve in the iliopsoas groove; lithotomy positioning and prolonged hip hyperflexion can also stretch it. These are classic, examinable non-operative causes.
Overview
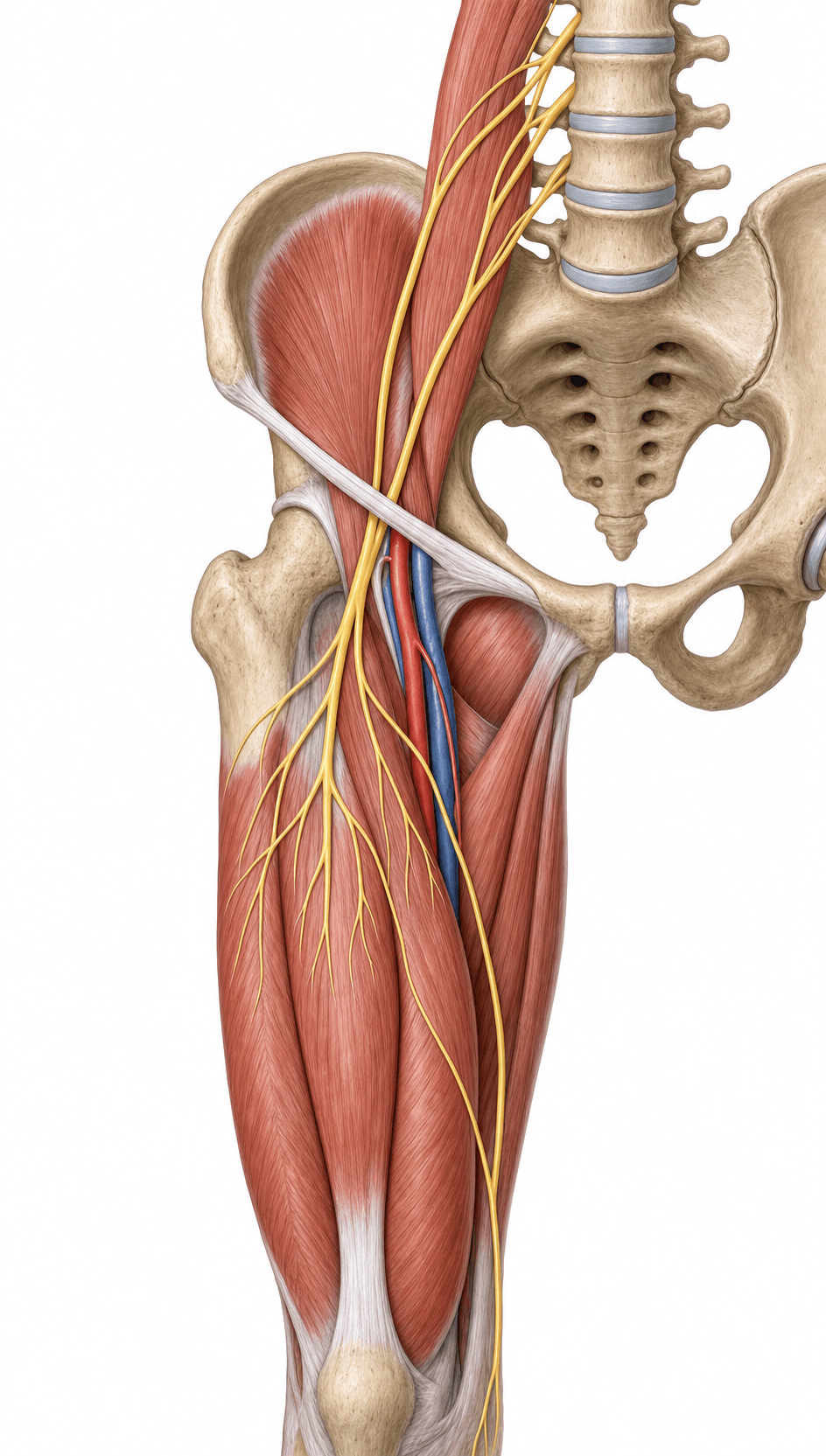
The femoral nerve is the largest branch of the lumbar plexus and the nerve a hip and knee surgeon thinks about most outside the sciatic. Its job is conceptually simple — extend the knee (and assist hip flexion) and carry sensation from the anterior thigh and medial leg — but its exam value comes from where it runs: in the iliopsoas groove (where a haematoma compresses it) and under the inguinal ligament, lateral to the artery and outside the sheath (where the direct anterior approach and groin surgery threaten it). Frame the topic as three linked ideas: the course and NAVEL relations, the deficit (quadriceps weakness, absent knee jerk, saphenous sensory loss), and the clinical hooks (anterior-approach THA, iliacus haematoma, the saphenous nerve at the knee, and femoral/adductor-canal blocks).
Origin & Course
Origin
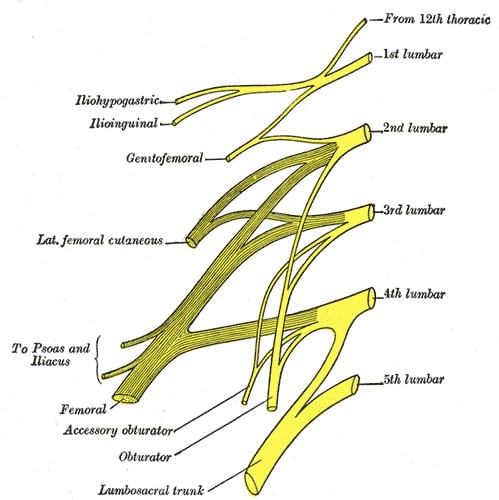
- The femoral nerve forms from the posterior divisions of the anterior rami of L2, L3 and L4.
- It is the largest branch of the lumbar plexus.
- It forms within the substance of psoas major and emerges from its lateral border.
Innervation: Motor & Sensory Supply
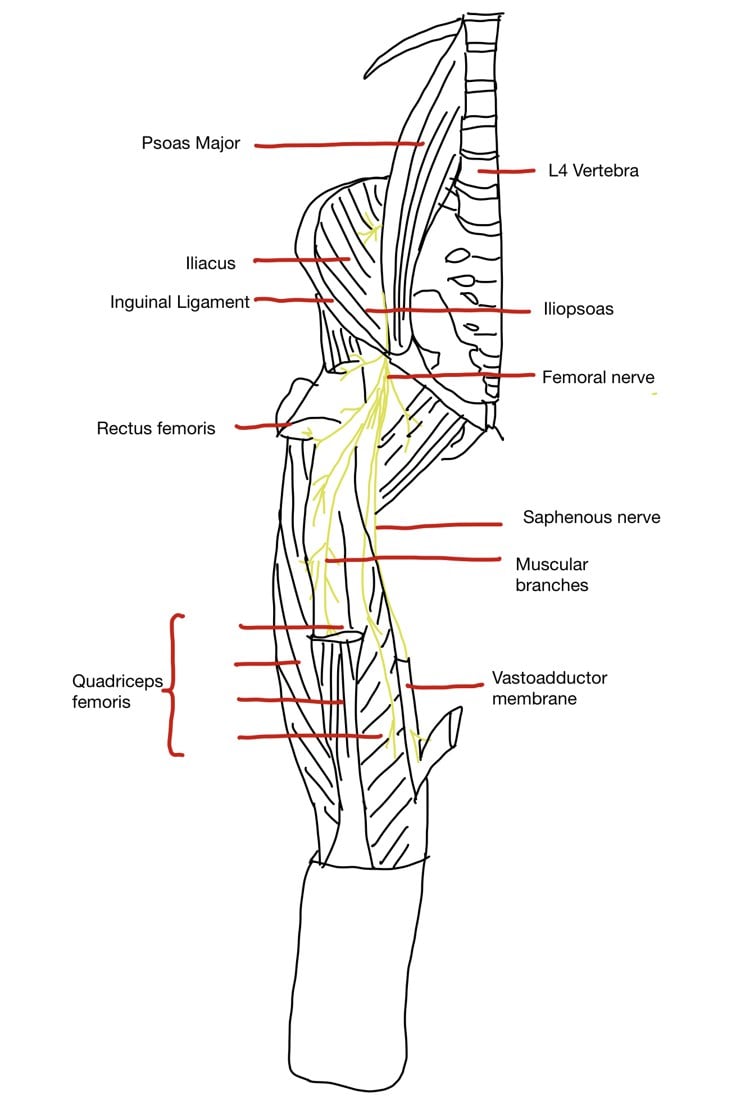
The femoral nerve supplies the muscles that extend the knee and assist hip flexion: iliacus, pectineus, sartorius, and the quadriceps femoris (rectus femoris, vastus lateralis, medialis and intermedius).
- Hip flexion is assisted (iliacus, pectineus, sartorius, rectus femoris) - but psoas major also contributes via direct lumbar plexus branches, so hip flexion is only partly affected by a femoral lesion below the inguinal ligament.
- Knee extension depends on the quadriceps - the key deficit in femoral nerve palsy (knee gives way).
- Sensory: anterior thigh via the medial and intermediate cutaneous nerves of the thigh; and the saphenous nerve (the terminal sensory branch of the posterior division) supplies the medial leg, ankle and medial foot.
IPed So QuietlyMuscles supplied by the femoral nerve
Hook:I-Ped-So-Quietly: Iliacus, Pectineus, Sartorius, Quadriceps. The quadriceps is the headline — its loss (knee buckling, absent knee jerk) defines femoral nerve palsy.
Surgical & Regional Anatomy: Saphenous Nerve, Knee Surgery and Nerve Blocks
Two practical extensions of femoral nerve anatomy are heavily examined.
The saphenous nerve and its infrapatellar branch
The saphenous nerve is the long, purely sensory terminal branch of the posterior division. It travels with the femoral artery into the adductor (subsartorial / Hunter's) canal, then pierces the fascia between sartorius and gracilis to become subcutaneous near the knee and supply the medial leg, ankle and medial foot (down to the medial malleolus — it does NOT reach the great toe, which is deep peroneal). Two surgical points follow:
- The infrapatellar branch of the saphenous nerve crosses the medial knee and is the nerve most commonly injured by medial knee incisions, arthroscopy portals, medial meniscus surgery, ACL graft harvest and total knee arthroplasty — producing numbness over the lateral aspect of the knee/proximal leg or a painful neuroma.
- Saphenous nerve entrapment can occur where it exits the adductor canal, causing medial knee/leg pain that mimics other pathology.
Distinct from the infrapatellar branch at the knee, the saphenous nerve's distal trunk descends the medial leg immediately alongside the great (long) saphenous vein and passes ANTERIOR to the medial malleolus with it — a constant, examinable relationship. The consequences:
- Long/great saphenous vein harvest (for coronary or peripheral bypass) and saphenous vein cutdown at the ankle (the time-honoured emergency venous access just anterior to the medial malleolus) classically injure the saphenous nerve, leaving numbness or a painful neuroma along the medial foot/ankle — the vein and nerve are taken together if the surgeon is not careful.
- The anteromedial portal of ankle arthroscopy and medial-side ankle/hindfoot incisions put the same nerve at risk; some surgeons "vein-light" or transilluminate to find and protect it.
- It explains medial-ankle sensory loss after these procedures and is why the saphenous nerve is the lower-limb counterpart of "nerve travels with the named vein."
Note the territory limit already given: the saphenous nerve reaches the medial malleolus and medial foot but not the great toe (deep peroneal) — useful when mapping a sensory deficit to the saphenous rather than a peroneal branch.
Femoral and adductor-canal nerve blocks
- A femoral nerve block (below the inguinal ligament, lateral to the artery) gives excellent analgesia for hip and knee surgery and femoral shaft fractures, but it weakens the quadriceps — a fall risk.
- The adductor canal block targets the saphenous nerve (and sensory fibres) more distally in the thigh: it provides knee analgesia while largely sparing quadriceps strength, so it is increasingly preferred for knee arthroplasty to allow earlier safe mobilisation. The trade-off (motor-sparing analgesia vs density of block) is a classic discussion point.
NAVELFemoral Nerve at the Groin
Hook:Lateral to medial: NAVEL - the femoral Nerve is most lateral, outside the sheath that holds only artery, vein and canal.
Clinical Correlations
Deficit
- Weak knee extension (quadriceps) - the patient describes the knee buckling/giving way, especially on stairs.
- Reduced or absent patellar (knee-jerk) reflex.
- Sensory loss over the anterior thigh and the medial leg (saphenous territory).
- Hip flexion is relatively preserved (psoas spared if the lesion is distal).
The classic straight-leg-raise (Lasègue) tensions the sciatic nerve and L4-S1 roots and is negative in upper-lumbar disease. To stress the femoral nerve and its L2, L3, L4 roots you need the femoral nerve stretch test (the "reverse straight-leg raise"): with the patient prone (or in the lateral position) the knee is flexed and the hip extended, stretching the femoral nerve over the front of the hip and reproducing anterior-thigh pain in a high lumbar (L2-3 or L3-4) disc herniation / upper-lumbar radiculopathy. (The same manoeuvre done as a quadriceps stretch is Ely's / the prone knee-bend test.) This is the bedside counterpart to "distinguish a femoral palsy from an L3/L4 radiculopathy": a distal femoral lesion gives quadriceps weakness with a negative femoral stretch test, whereas a proximal root/plexus lesion is positive — and an upper-lumbar disc characteristically causes anterior-thigh/quadriceps symptoms with a preserved knee jerk only early before the L3/L4 reflex arc fails. It is examinable as an OSCE manoeuvre and a viva discriminator between root, plexus and peripheral femoral pathology.
Guidelines, Registries & Global Practice
Global Practice Picture
Femoral nerve anatomy underpins safe anterior-based hip exposure worldwide. With the international growth of the direct anterior approach, awareness of femoral nerve palsy (incidence around 1% in reported series) and the anatomical "danger zone" at the anterior acetabular rim has become standard teaching, alongside recognition of iliacus haematoma as a non-operative cause.
Side-by-Side Synthesis
- Detail
- L2-L4 posterior divisions (largest lumbar plexus branch)
- Detail
- Psoas-iliacus groove → under inguinal ligament, lateral to artery
- Detail
- NAVEL (nerve most lateral, outside sheath)
- Detail
- Iliacus, pectineus, sartorius, quadriceps (knee extension)
- Detail
- Anterior thigh + saphenous (medial leg/foot)
- Detail
- Weak knee extension, absent patellar reflex, anteromedial sensory loss
- Detail
- Anterior THA retractor / lengthening; iliacus haematoma; lithotomy
Evidence Base
Both papers below were checked against their PubMed records and address the same modern concern — femoral nerve palsy in the direct anterior approach. Yoshino's cadaveric study gives the anatomical rule (the nerve is closest to the anterior acetabular rim at the 90° position, so avoid a retractor there), and Hoshino's clinical series gives the incidence and outcome (about 1 percent, linked to retractor position and over-lengthening, usually fully recovering). Together they justify the single most practical exam point: place anterior retractors carefully and watch limb length. Neither addresses the saphenous/block anatomy, which rests on cadaveric and regional-anaesthesia literature.
Anatomical Implications Regarding Femoral Nerve Palsy During a Direct Anterior Approach to Total Hip Arthroplasty: A Cadaveric Study
- Cadaveric study of 84 hips mapping the femoral nerve's distance from the anterior acetabular rim
- Minimum distance ranged 16.6-33.2 mm; the nerve was closest to the rim at the 90 degree (anterior, 'three o'clock') position
- Iliopsoas thickness and femoral length correlated with the distance at 90 degrees
- Recommends avoiding retractor placement at 90 degrees to the anterior rim to reduce femoral nerve injury
Femoral nerve palsy following primary total hip arthroplasty with the direct anterior approach
- Retrospective review of 273 primary direct-anterior-approach THAs; femoral nerve palsy incidence 1.1%
- Suspected causes: improper anterior acetabular retractor positioning and excessive leg lengthening
- All three palsies recovered completely within a year
- No significant relationship between palsy and the surgeon's direct-anterior experience